
Abstract
Background Asylum seekers and refugees (ASR) in Germany are dispersed quasi-randomly to state-provided, collective accommodation centres. We aimed to analyse contextual effects of post-migration housing environment on their mental health.
Methods We drew a balanced random sample of 54 from 1 938 accommodation centres with 70 634 ASR in Germany’s 3rd largest federal state. Individual-level data on depression (PHQ2) and anxiety (GAD2) symptoms as well as sociodemographic- and asylum-related covariates, was collected and linked to contextual geo-referenced data on housing environment (‘Small-area Housing Environment Deterioration’ index, number of residents, remoteness, urbanity and German Index of Multiple Deprivation). We fitted two-level random-intercept models to exploratively estimate adjusted contextual effects.
Results Of 411 surveyed participants, 45.53% and 44.83%, respectively, reported symptoms of depression or anxiety. 52.8% lived in centres with highest deterioration, 46.2% in centres with >=50 residents, 76.9% in urban, and 56% in deprived districts. 7.4% of centres were remote. The accommodation-level median odds ratio for GAD2 was 2.10 with contextual-level variance of 16%.
For odds of reporting GAD2 / PHQ2, the highest degree of deterioration (OR 2.22; 95% CI 0.52-9.59 / 1.99;0.55-7.18), large accommodation size (1.34;0.59-3.06. / 1.12;0.56-2.26), remoteness (2.16;0.32-14.79 / 3.79;0.62-23.18) and district urbanity (3.05;0.98-9.49 / 1.14;0.46-2.79) showed higher, but statistically not significant, point-estimates. District deprivation demonstrated higher odds for GAD2 (1.21;0.51-2.88) and, inversely, lower odds for PHQ2 (0.88;0.41-1.89).
Conclusion We found tendencies for, but no significant, contextual effects of housing environment on ASR mental health in accommodation centres. Confirmatory analyses with prior power calculations are needed to complement these exploratory estimates.
What is already known on this subject Research on mental health of asylum seekers and refugees (ASR) has focused on pre- and peri-migratory factors, and increasingly recognizes post-migratory factors and their importance in restoring, sustaining, and protecting health to enable societal integration and participation. Research on the small-area housing environment, and its potential health effects is still scarce, and often limited by high-levels of aggregation of contextual factors, crude or not-standardised measurements on housing characteristics, and risk of compositional bias due to selective migration into housing environments.
What this study adds We make use of the quasi-random allocation of ASR to state-provided, collective accommodation centres, and link individual-level data on health and socio-demographic variables with small-area measures of contextual housing environment at accommodation-level to explore potential effects while minimising the risk of compositional bias. Accommodation-level factors contribute considerably to mental health variance. A tendency towards higher odds of reporting symptoms of generalized anxiety could be observed for housing deterioration, higher numbers of residents, remoteness as well as district urbanity and deprivation. Similar tendencies were estimated for reporting symptoms of depression except for deprivation potentially functioning protectively. Confirmatory research with appropriate sample size calculations as well as mediation and structural equation analysis are needed. Results may guide policy makers in design and planning of needs-based health services and housing infrastructure.
Introduction
Undergoing disruptive situations in their home country, during flight or in arrival countries, asylum seekers and refugees (ASR) experience a high burden of disease.[1–3] This is particularly reflected in high prevalence rates of psychological distress, e. g. depression, generalized anxiety disorder or post-traumatic stress, both globally[4, 5] and in Germany.[1, 4, 6, 7]
Historically, mental health research has focused on pre- and peri-migratory risk factors when studying refugee health,[8] but focus has been slowly shifting towards post-migration stressors in the country of reception, e. g. unemployment, loneliness or factors relating to the asylum process.[6, 9–11]
In addition to these individual-level factors, several contextual determinants of mental health have been discussed. These range from housing type and condition,[9, 12] residential instability[13] or economic opportunity[9] to restrictive (non-)health migration policies.[14, 15] Their importance has been particularly aggravated by the SARS-CoV-2 pandemic where ASR have been experiencing a high cumulative incidence risk in case of an outbreak within their accommodation.[16]
Furthermore, the German asylum system assigns newly arriving ASR to a place of residence based on administrative quota in a quasi-random manner, and free movement to other residential areas is restricted until the application is closed. Such assignment to neighbourhoods is not only disempowering and limits individual autonomy,[17] but has resulted in higher numbers of vulnerable asylum seekers (i.e. minors, female, or elderly) living in districts characterised by high socioeconomic deprivation.[18] Such disadvantageous contextual conditions may exacerbate pre-existing socioeconomic inequalities, aggravate (perceived) downward social mobility, and deteriorate the already high burden of mental illness.[19]
However, research on small-area housing environment and its potential health effects is still scarce, and often limited by crude or non-standardised measurements on housing characteristics, high-levels of aggregation of contextual factors, and risk of compositional bias due to selective migration into housing environments. For example, housing measures have been criticized for being not rigorous, very diverse, and mainly based on respondent self-reports with researcher observations being the exception.[12]Others report on crude measures such as “private/shared” accommodation,[9] while more sophisticated analyses of housing environments predominantly include populations with completed asylum claims[20] and hence suffer from the risk of selective migration into residential areas.
Against these backdrops, we aimed to exploratively assess contextual effects of housing environment on mental health of ASR, while using reliable and valid data on the post-migration contextual environment at small-area level and minimising the risk of compositional bias.
Methods
Setting, sampling and recruitment
We collected data in 54 collective refugee accommodation centres, sampled from a total of 1 938 centres with 70 634 ASR across all districts of Germany’s 3rd largest federal state of Baden-Wuerttemberg (2017/2018). With 10.8 million inhabitants and 44 districts, it receives about 13% of all incoming ASR to Germany based on a quota system considering state-level tax income and population size.[21] After a stay in reception centres for up to 18 months, ASR are quasi-randomly dispersed to district-level collective accommodation centres determined by a quota based on district-level population size. The numbers of ASR assigned to each district are proportional to the size of the district population relative to the overall state population. As there are no mandatory standards for accommodation centres, location and quality of centres vary strongly within and between districts.[22]
Participants were recruited using a complex random sampling design balanced for (1) the number of resident ASR within centres and (2) their total number in the region. Detailed information on sampling and data collection have been reported previously.[2, 23]
Individual-level health and socio-demographic variables
Individual-level variables were captured part of a health monitoring survey using a paper-based questionnaire in nine languages.[2, 23] Mental health was captured by 2-item screeners for symptoms of depression (Public Health Questionnaire-2, PHQ2[24]) and generalized anxiety (Generalized Anxiety Disorder-2, GAD2[25]). Both offer a valid ultra-brief tool to identify individuals who may be suffering from either mental disorder.
We further collected data on participants’ socio-demographics (age at interview, sex, educational attainment, region of origin, the number of children), physical health (self-reported chronic illness), and factors related to the asylum process (residence status) including the number of transfers between accommodation centres as a proxy of residential instability as these have been reported to be influential for mental health.[3, 11, 13] We used these factors to adjust for potential confounding by individual-level health, socio-demographic characteristics, and aspects related to the asylum process (table 1).
Contextual variables on housing environment
We linked individual-level data of ASR with contextual characteristics of their housing environment at level of accommodation centres (via unique identifiers for each centre and participating individual). Centre data (at level of exact streets and houses) was linked to neighbourhood characteristics via Google Maps, and to district-level characteristics (nomenclature des unités territoriales statistiques (NUTS) level 3) via secondary data-sources and official statistics (table 1).
Data at level of accommodation centres comprised the accommodation size, i.e. number of residents, and the stage of decay of the built environment quantified by the Small-area Housing Environment Deterioration index (SHED). SHED was rated by the field teams and consists of six dimensions assessing (1) conditions of windows/glass and (2) walls/roof, (3) garbage accumulation and (4) graffiti inside and outside the house and (5) the condition of outside spaces including gardens, complemented by (6) a global rating of the overall living environment. SHED’s theoretical framework, its construction, piloting, and validation, including proven high intra- and interrater reliability, have been reported elsewhere in detail.[26] The composite SHED index score is calculated based on individual item’s z-transformation (to standardize item scores across different scales) and normalization (to scale all item scores in the range of 0–1). We then split the index score into four relative quartiles of distribution, ranging from Q1 (lowest) to Q4 (highest level of deterioration).
Neighbourhood characteristics for each accommodation centre included a remoteness index. Using Google Maps and each centre’s exact address, we calculated the travel distance to three locations of essential services (medical services, grocery shopping, town hall), both on foot and using public transportation, for Monday mornings at 9am. After, we dichotomized the index at >=2 locations needing > 20minutes both on food and by public transportation (if available).
Accommodations were then linked with district-level factors comprising urbanity, as assessed by the German Federal Institute for Research on Building, Urban Affairs and Spatial Developments (BBSR) defining an urban district as one with a population density over 150 inhabitants per km2,[27] as well as district deprivation, as assessed by the German Index of Multiple Deprivation, Version 2010[28] calibrated to the distribution of the GIMD score within the state of Baden-Württemberg. Centres were then classified as located in ‘high-/low- deprivation districts’ based on the median GIMD-10 score across all 44 districts.
Conceptual Model
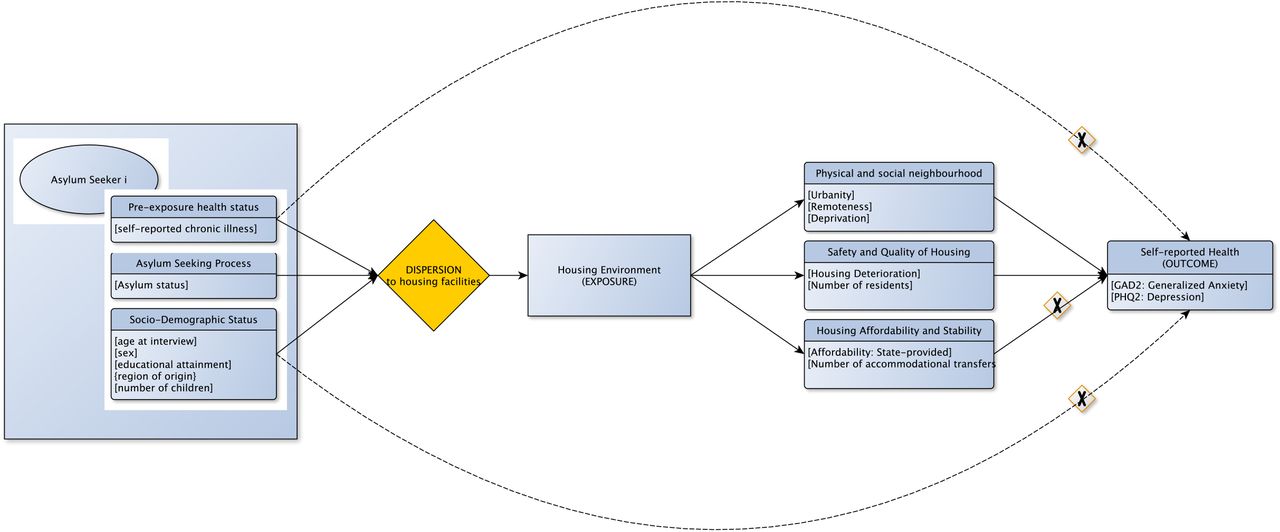
We conceptualised the relationship between exposures, outcomes, and co-variables vis à vis the dispersion process of being assigned to residential areas in a causal diagram guiding our analysis. The dispersion functions as a quasi-random allocation of asylum seekers to district-level collective accommodation centres. See figure 1.

Effects of housing on self-reported health are mediated via (1) physical and social neighbourhood, (2) safety and quality of housing and (3) housing affordability and stability. Focussing on the contextual pathways, effects through number (3) are blocked as (a) state-provided accommodations nullify questions of affordability and (b) our models are adjusted for the number of accommodational transfers conceptualized as housing stability. Other potential confounders (pre-exposure health status as well as sociodemographic factors) are adjusted for in the models.
Time flows from left to right. Variables for each domain have been put into square brackets.
Statistical analyses
We performed a descriptive analysis of absolute and relative frequencies for each contextual exposure variable at the level of accommodation centres. We further quantified the individual-level distribution of the outcome variables of interest stratified by all contextual measures and potentially confounding covariates.
Two-level random-intercept logistic regression models were fitted for each outcome variable of interest (PHQ2, GAD2) calculating odds ratios (OR) and 95% confidence intervals (95% CI) adjusting for above mentioned individual-level covariates and the clustering of participant-level observations within each accommodation centre.
For this, we utilized a stepwise approach starting with fitting a null model displaying accommodation-level variability in outcome variables (M0) and assessing statistically significant clustering in such two-level random-intercept models compared to single-level null-models. Next, we fitted a two-level model for each outcome and each exposure individually, both unadjusted, i.e. without individual-level variables (M1a-M1e), and adjusted, i.e. including individual-level variables (M2a-M2e), before fitting a multiple regression model for all post-migration contextual housing variables together (unadjusted for individual-level variables) (M3). Finally, we fitted a last model including all post-migration contextual housing variables while adjusting for all above mentioned individual-level variables as potential confounders (M4). We refrained from reporting effect estimates for covariates conceived as potential confounders in our reporting to prevent ‘table 2 fallacy’.[29, 30]
To quantify accommodation-level differences in the outcomes of interest, we calculated both the accommodation-level and total variance as well as the intraclass correlation (ICC) as their quotient. Given difficulty in interpretation of ICC in logistic regression as individual-level and contextual-level variance are not directly comparable,[31, 32] we further calculated median odds ratios (MOR) of the distribution of odds ratios calculated for each pair of participants with similar individual-level covariates across clusters to better understand differences in outcomes based on accommodation centres.
For comparing and assessing model fit, we calculated Akaike information criterion (AIC), Bayesian information criterion (BIC) and model significance based on Wald-chi2. To assess potential multicollinearity, we further computed the variance inflation factor (VIF) for each variable and reported the range of VIFs for each model.
For visualization purposes, we plotted the predicted outcomes of interest against each accommodation centre, based on the null, exposure adjusted and fully adjusted models.
For all statistical analyses, we utilized an approach based on listwise deletion of missing data, determined the level of statistical significance at a p-value of 0.05 and conducted all computation in Stata SE V16. [33]
Results
Post-migration contextual housing environment
Of all randomly selected accommodation centres, 46.29% presented with high (Q3) or highest levels (Q4) of deterioration on the SHED index (Table 2). In terms of residents, this translates to 52.8% of study participants living in such deteriorated housing. Most of the accommodation centres (79.6%) had less than 50 ASR as residents, while the average number of residents was ca. 34 (SD=34, min=4 to max=158). At the same time, the 20.4% accommodation centres with 50 or more residents accounted for 46.2% of all ASR in the sample. While most ASR (76.9%) were living in urban districts, 56% were living in districts characterised by high levels of deprivation. A total of 7.4% of accommodation centres, accounting for 3.2% of ASR, were remotely located.
Distribution of health outcomes by individual-level characteristics
Of all surveyed ASR, 45.53% reported symptoms of depression and 44.83% symptoms of generalized anxiety. The prevalence of symptoms of depression or anxiety were comparable across the strata of age, sex, self-reported longstanding illness, region of origin, educational attainment, number of children, or residence status (table 3). A large majority (more than 80%) of those with symptoms of depression or anxiety reported two or more accommodational transfers since arrival in Germany (table 3) with about 50% awaiting results of their asylum application.
Distribution of health outcomes by accommodation-level characteristics
Exploring accommodation-level characteristics, participants reporting symptoms of depression or generalized anxiety shared another similar pattern: Equal numbers of residents lived in accommodation centres with 50 or more residents (50.6% depression; 54.5% generalized anxiety) and a majority in districts classified as urban (75.9%; 80.8%) and as deprived (55.1%; 60.3%). 5.1% and 5.8% of symptom-positive participants, respectively, lived in accommodation centres assessed as remote. In terms of the SHED index, the largest group of symptom-positive participants lived in housing of the third highest level of deterioration (39.9%; 30.1%). For further details, please consult table 3.
Generalized linear models
Fitting an empty two-level random-intercepts model, we found statistically significant clustering in reporting symptoms of generalized anxiety on the level of accommodation centres (Likelihood ratio test; p-value <0.001). The model resulted in an intraclass correlation of 0.16 which translated into a MOR of 2.10 for the accommodation-level effects. No significant clustering at accommodation-level was found for symptoms of depression.
In the univariate and multivariate models, a tendency towards higher odds of reporting symptoms of generalized anxiety was observed for participants living in centres assessed as highly deteriorated (fully adjusted model M4: OR 2.22 [95% CI 0.52,9.59]), accommodating >=50 residents (1.34 [0.59,3.06]), assessed as remote (2.16 [0.32,14.79]) or situated in urban (3.05 [0.98,9.49]) or deprived (1.21 [0.51,2.88]) districts. Statistical significance was observed for none of the above.
For symptoms of depression, a similar tendency was observed: Higher odds of reporting symptoms were observed for accommodations with highest level of deterioration (1.99 [0.55,7.18]), accommodating >= 50 residents (1.12 [0.56,2.26]), assessed as remote (3.79 [0.62,23.18]) or those situated in urban districts (1.14 [0.46,2.79]). In contrast to symptoms of generalized anxiety, living in a high-deprivation district tends to be associated with lower odds of reporting symptoms of depression (0.88 [0.41,1.89]). Similar to GAD2 scores, statistical significance was not observed for any of the above.
The stepwise approach in regression modelling allowed for calculation of several criteria of model fit: Both AIC as well as BIC improved with each model and presented their lowest value in M4. There was no evidence for multicollinearity between exposures based on VIFs. Detailed regression results can be found in table 4. Predicted random-intercepts for each accommodation centre have been ranked and plotted for three models (M0, M3, M4) visualizing the reduction in accommodation-level variance in GAD2 after inclusion of contextual- and individual-level factors (figure 2) towards a MOR of 1.34 in the fully adjusted model (M4) (table 4).

{kind=link}
{kind=link}
Discussion
Using the quasi-random allocation of ASR into residential areas to examine contextual effects on housing environment on mental health, this study reports three principal findings. First, housing environments for half of the participants were characterized by high deterioration, high deprivation of districts, and for most, by urbanity. About 20% lived in large centres (>=50 residents), while 7% of centres were remote and cut-off from essential facilities (medical facilities, groceries, community town hall).
Second, about every second ASR reported symptoms of depression or anxiety, while anxiety significantly clustered at accommodation level.
Third, we observed a tendency to higher odds of reporting symptoms of generalized anxiety and/or depression when living in collective accommodation centres with highest level of deterioration, large numbers of residents, remote location and/or being situated in an urban district. Being in a district with high level of deprivation showed different point estimates for the two mental health outcomes: while deprivation came along with higher odds for reporting symptoms of generalized anxiety, the inverse pattern was found for symptoms of depression. Results should be deemed exploratory and preliminary as sampling for these analyses was underpowered and fixed effects throughout lacked statistical significance.
Strengths and limitations
Conceived as a cross-sectional study lacking base-line data on health, no causal inferences can be made, and future studies should analyse the dispersal into different contexts and potential health effects within longitudinal designs. The study was further limited by the explorative nature: point estimates of fixed effects were surrounded by large 95% CIs and lacked statistical significance, raising questions of an underpowered sampling for these analyses. Further, given the nature of the used PHQ2 and GAD2 screening instruments, all mental health symptoms were self-reported, i.e. not assessed by a mental health specialist, and may as such lack clinical relevance. While we studied the mutually adjusted effects of several contextual factors on mental health (further adjusted for individual-level factors), we did not study the interrelation or combined effects of these contextual variables on health outcomes. Given the potentially complex relationship between the explored aspects of post-migration contextual housing environment future analyses should analyse the inter-relations and potential interactions between these.
At the same time, a strength of this study lies in its high-quality and extensive data at high geographical resolution. Sampling was based on a complex design balanced for the number of ASR residing in the accommodation centre and in the respective region. The surveyed participants were representative for the overall population in the state Baden-Wuerttemberg with respect to nationality, age, and sex as reported elsewhere.[2] All instruments used are internationally established and if not were validated separately[2, 26] and, if needed, underwent a rigorous translation and pre-testing process.[34] Individual level was accurately linked to collected contextual data or to geo-referenced data at highest level of resolution, as such minimising the risk of misclassification bias. Given the resource-intense sampling procedure to reach this population, this primary data study including the linkage options offer added value to research on refugee health in the context of housing and post-migration determinants. Other studies analysing housing effects on health among ASR[20] used the IAB-BAMF-SOEP-refugee panel which has a nation-wide scope.[35] However, the majority of individuals included in the sample (> 80%) have completed asylum claims,[20] which means that selective migration into housing environments in cross-sectional designs cannot be ruled out. In contrast, our sample consists of ASR who have more recently arrived in Germany; as such, only 24% of our sample had been granted residence permit and lived in the centres because they could not find or afford private housing. As freedom of movement is restricted if the decision on the asylum claim is pending, the risk of compositional bias is substantially reduced.
Research gaps
Several research questions remain for future research studies. First, in the final exposure and confounder adjusted model M4, a median odds ratio of 1.38 remained signalling left-over accommodation-level variance to be explored. Second, given the small potentially underpowered sample for such analyses, confirmatory analyses with appropriate sample size calculations are needed. Third, to better understand the inter-relations between various post-migration contextual housing characteristics further statistical approaches, e. g. cluster analyses, principal component analyses or other structural equation modelling techniques, may be of value. Finally, studies considering timing and time variance, e. g. longitudinal studies, as well as studies ensuring randomization or utilizing natural quasi-randomization, are needed to confirm potential cause-effect relationships.
Implications for policy
Given the deteriorated condition of most collective accommodation centres and pre-existing ASR’s mental health burden, sustainable long-term monitoring of housing conditions and health of ASR is important to ensure a comprehensive epidemiological understanding enabling evidence-informed, efficient, and targeted preventative measures, health care spending and adequate housing policies.
With legal residence requirements in certain districts or collective accommodation centres and living realities shaped by disempowerment and loss of autonomy, it is a moral responsibility to prevent such structural violence in form of dispersing individuals into disadvantaged contexts. Housing standards and investments in maintenance of state-provided collective accommodation centres for ASR may be a critical component in ensuring long-term health maintenance and allowing post-migration contexts as “powerful determinant[s] of mental health”[8] to facilitate long-term improvements in health and building grounds for successful arrival, integration, and participation of ASR in their host country.
Conclusion
Higher levels of housing deterioration, larger numbers of residents and remoteness of accommodation centres as well as their district’s level of urbanity may be associated with higher odds of reporting symptoms of generalized anxiety and depression (adjusted for individual-level factors), but evidence for significant effects could not be established in this exploratory study. High deprivation at district-level may be a risk factor for generalized anxiety but potentially a protective factor for reporting symptoms of depression. Together, these factors reduced variance at accommodation level, but further unexplained variance remained for reporting symptoms of generalized anxiety. Further confirmatory studies with appropriate sample size calculations and longitudinal designs are needed.
Data Availability
All data produced in the present study are available upon reasonable request to the authors
Additional Information
Ethical considerations
Primary data has been collected as part of the RESPOND project at Heidelberg University Hospital, Germany (https://respond-study.org/) and oral informed consent was obtained from all participants after oral, written and audio-based information in nine languages deployed by a multi-lingual field team. Ethical clearance was received by the ethics committee of the Medical Faculty of Heidelberg on October 12, 2017 (S-516/2017[2]).
Role of the funding source
The primary data collection was funded by the German Federal Ministry for Education and Research (BMBF) in the scope of the project RESPOND (Grant Number: 01GY1611). The study was realised with funding of the German Science Foundation (DFG) in the scope of the NEXUS project (FOR 2928 / GZ: BO 5233/1-1). AM acknowledges financial support by the Else Kröner-Fresenius-Stiftung (2017_Promotionskolleg.08) within the Heidelberg Graduate School of Global Health. The funders had no influence on study design, analysis, or decision to publish.
Availability of data
Data are available from the authors upon reasonable request.
Authors’ contributions
AM: study conceptualisation, data collection, data analysis, writing of original draft
LB: project and study conceptualisation, project management, data collection, draft revision
KB: project and study conceptualisation, funding acquisition, project management, data collection, draft revision
Declaration of interests
The authors declare that they have no conflict of interests.
REFERENCES



