
Summary
Background Real-world evidence on the effectiveness of oral antivirals in mild-to-moderate COVID-19 patients is urgently needed. This retrospective cohort study aims to evaluate the clinical and virologic outcomes associated with molnupiravir and nirmatrelvir/ritonavir use in COVID-19 patients during a pandemic wave dominated by the Omicron BA.2 variant.
Methods We analyzed data from a territory-wide retrospective cohort of hospitalized patients with confirmed diagnosis of SARS-CoV-2 infection from 26th February 2022 to 26th April 2022 in Hong Kong. Oral antiviral users were matched with controls using propensity-score matching in a ratio of 1:4. Study outcomes were a composite outcome of disease progression (all-cause mortality, initiation of invasive mechanical ventilation [IMV], or intensive care unit admission) and their individual outcomes, and lower viral load of cycle threshold (Ct) value ≥30 cycles. Hazard ratios (HR) of event outcomes were estimated using Cox regression models.
Results Among 40,776 hospitalized patients with SARS-CoV-2 infection over a mean follow-up of 41.3 days with 925,713 person-days, 2,359 and 1,000 patients not initially requiring oxygen therapy were initiated with molnupiravir and nirmatrelvir/ritonavir, respectively. The crude incidence rates of all-cause mortality and IMV were 22.24 and 1.06 events per 10,000 person-days among molnupiravir users, 11.04 and 1.75 events per 10,000 person-days among nirmatrelvir/ritonavir users. Oral antiviral use was associated with a significantly lower risk of the composite outcome of disease progression (molnupiravir: HR=0.53, 95%CI=0.46-0.62, p<0.001; nirmatrelvir/ritonavir: HR=0.33, 95%CI=0.24-0.46, p<0.001) than non-use, which was consistently observed for all-cause mortality (molnupiravir: HR=0.55, 95%CI=0.47-0.63, p<0.001; nirmatrelvir/ritonavir: HR=0.32, 95%CI=0.23-0.45, p<0.001). Molnupiravir users had lower risks of IMV (HR=0.31, 95%CI=0.16-0.61, p<0.001). Time to achieving lower viral load was significantly shorter among oral antiviral users than matched controls (molnupiravir: HR=1.21, 95%CI=1.07-1.37, p=0.002; nirmatrelvir/ritonavir: HR=1.25, 95%CI=1.04-1.50, p=0.015). Amongst survivors, nirmatrelvir/ritonavir had shorter length of hospital stay (−0.70 days, 95%CI=-1.37 to -0.04, p=0.039) than matched controls. Head-to-head comparison of molnupiravir and nirmatrelvir/ritonavir reported higher risk of mortality (HR=1.53 95%CI=1.01-2.31, p=0.047) and longer length of hospital stay (0.83 days, 95%CI=0.07-1.58, p=0.032) for molnupiravir users.
Conclusions Against Omicron BA.2, initiation of novel oral antiviral treatment in hospitalized patients not requiring any oxygen therapy was associated with lower risks of disease progression and all-cause mortality, in addition to achieving low viral load faster.
Funding Health and Medical Research Fund, Food and Health Bureau
Evidence before this study The medical and research community are actively exploring the use of oral antivirals in COVID-19 patients to lower their risks of hospitalization and death, and to reduce the burden on healthcare systems. We searched Scopus and PubMed for studies until 13 May 2022 using the search terms “SARS-CoV-2 OR COVID-19” AND “molnupiravir OR Lagevrio OR EIDD-2801” OR “nirmatrelvir OR Paxlovid OR PF-07321332”. Major studies examining the safety and efficacy of molnupiravir include MOVe-IN and MOVe-OUT trials conducted in hospitalized and non-hospitalized COVID-19 patients, respectively. Clinical evidence for the use of ritonavir-boosted nirmatrelvir came from the EPIC-HR trial conducted among non-hospitalized adults with COVID-19. While no clinical benefits have been observed with molnupiravir use in the inpatient setting among patients with moderate-to-severe COVID-19, early initiation of molnupiravir or nirmatrelvir/ritonavir within 5 days of symptom onset in non-hospitalized patients with mild-to-moderate COVID-19 and risk factors for progression to severe disease has been associated with relative risk reduction of hospitalization or death by 30% and 88%, respectively. Notably, these clinical trials were conducted prior to the prevalence of Omicron variant, and the efficacy of oral antivirals against this current variant of concern can only be inferred from experimental evidence to date. Real-world evidence of oral antiviral use in patients with SARS-CoV-2 infection of Omicron variant is lacking.
Added value of this study To the best of our knowledge, this is the first real-world study exploring the clinical use of oral antivirals during a pandemic wave dominated by SARS-CoV-2 Omicron variant. We conducted a territory-wide, retrospective cohort study to examine the effectiveness of molnupiravir and nirmatrelvir/ritonavir in COVID-19 patients who did not require supplemental oxygen on admission in Hong Kong. Early initiation of oral antivirals within 2 days of admission was associated with significantly lower risks of disease progression and all-cause mortality, in addition to achieving low viral load faster than their respective matched controls. Molnupiravir use was also associated with a significantly lower risk of requiring invasive mechanical ventilation than non-use. Furthermore, our head-to-head comparison suggested a relatively larger reduction in mortality risk with nirmatrelvir/ritonavir than molnupiravir use.
Implications of all the available evidence Current guidelines are now prioritizing the distribution of oral antivirals to those who do not require supplemental oxygen, but who are at the highest risk of disease progression. Our study cohort reflected such prescription pattern in real-world clinical practice. The antiviral effect and mortality benefit observed in this patient cohort support the use of oral antivirals in COVID-19 patients who do not require supplemental oxygen on admission during a pandemic wave of Omicron variant. Our findings also support the prioritization of nirmatrelvir/ritonavir over molnupiravir use in COVID-19 patients whenever accessible and clinically appropriate, in view of the former’s substantial mortality benefit. Ongoing research will inform the safety and effectiveness of oral antivirals in specific patient populations (by vaccination status and viral variants), drug combinations, and different healthcare settings.
Introduction
In the midst of the coronavirus disease 2019 (COVID-19) pandemic, various drugs have been repurposed or developed for treating patients with SARS-CoV-2 infection. In December 2021, molnupiravir (Lagevrio) and ritonavir-boosted nirmatrelvir (Paxlovid) are two oral antivirals that have been granted Emergency Use Authorization (EUA) by the U.S. Food and Drug Administration (FDA) for the treatment of non-hospitalized patients with mild-to-moderate COVID-19, who are at risk of progression to severe disease, so as to reduce the burden on healthcare systems by lowering their risk of hospitalization or death 1,2.
While both molnupiravir and nirmatrelvir/ritonavir are indicated for non-hospitalized patients with mild-to-moderate COVID-19 within 5 days of symptom onset should they be at risk of progression to severe disease, current guidelines give priority to nirmatrelvir/ritonavir and another antiviral remdesivir (relative risk reduction by 87%) that have demonstrated higher efficacy than molnupiravir in reducing hospitalization or death among COVID-19 patients not requiring hospitalization or supplemental oxygen 1-4. Notably, several concerns and research gaps remain in the use of the two oral antivirals, for instance, if initiation in asymptomatic COVID-19 patients is appropriate, the lack of clinical data in treating patients infected with specific VOC, and their safety and efficacy in vaccinated individuals with breakthrough infections 5-7. Furthermore, efficacy of molnupiravir as illustrated in the
MOVe-OUT trial has been questioned in light of its premature termination, imbalances in risk factors and COVID-19 severity of patients at baseline, results with borderline statistical significance and of uncertain clinical significance, and discrepancies between interim and full analyses that could not be fully explained by differences in patient characteristics 8-10.
Real-world evidence on the effectiveness of molnupiravir and nirmatrelvir/ritonavir in COVID-19 patients is urgently needed 11, as well as head-to-head comparison between the two oral antivirals. This retrospective cohort study aims to evaluate the clinical and virologic outcomes associated with molnupiravir and nirmatrelvir/ritonavir use in COVID-19 patients during a community epidemic dominated by the Omicron BA.2 variant.
Methods
Study Design
A territory-wide, retrospective cohort study was used to examine the effectiveness of oral antivirals (molnupiravir or nirmatrelvir/ritonavir) in hospitalized adult patients with COVID-19 without oxygen therapy in the Hong Kong Special Administrative Region, China, during the observation period from 26th February 2022 to 5th May 2022.
Data Source and Study Population
Electronic health records of patients with COVID-19 were retrieved from the Hospital Authority (HA), a statutory provider of public inpatient services and primary public outpatient services in Hong Kong. Electronic health records included demographics, date of registered death, hospital admission, emergency department visits, diagnoses, prescription and drug dispensing records, procedures, and laboratory tests. The HA linked the health records and anonymized population-based vaccination records of individuals provided by the Department of Health using unique identification numbers (Hong Kong Identity Card or foreign passport number). The database has been widely used for high-quality studies to evaluate the safety and effectiveness of drug treatments for COVID-19 at a population level 12. Our cohort comprised patients with positive results of reverse transcription-polymerase chain reaction (RT-PCR) or rapid antigen test who were admitted to local public hospitals from 26th February 2022 to 26th April 2022. Patients were eligible for inclusion if they had been admitted within 3 days of their COVID-19 diagnosis date, or if COVID-19 diagnosis was confirmed within 3 days of their admission date, so as to account for any potential time lag in the confirmation of cases during an upsurge of patients with SARS-CoV-2 infection. The index date was defined as the date of hospital admission (day 0). Patients who were admitted to hospital with COVID-19 before 26th February 2022 (the date of first molnupiravir prescription) or after 26th April 2022 (less than 1 week of follow-up), aged <18 years, or with oxygen support or mechanical ventilation on the index date, were excluded.
This study was approved by the institutional review board of the University of Hong Kong / Hospital Authority Hong Kong West Cluster (reference no. UW 20-493). Given the extraordinary nature of the COVID-19 pandemic, individual patient-informed consent was not required for this retrospective cohort study using anonymized data.
Treatment Exposure and Follow-up Period
Hospitalized patients with COVID-19 without oxygen therapy and receiving early (i) molnupiravir and (ii) nirmatrelvir/ritonavir treatment at public hospitals during the observation period were defined as (i) molnupiravir users and (ii) nirmatrelvir/ritonavir users. We defined treatment exposure period at 2 days within admission to mitigate potential immortal time bias between treatment initiation and admission13-15. Controls were selected from the cohort of hospitalized patients with COVID-19 without oxygen therapy who did not receive oral antivirals (molnupiravir and/or Paxlovid) during the observation period, using the propensity-score in a ratio of 1:4. Patients were observed from the index date until registered death, the occurrence of outcome events, crossover of oral antiviral treatment, or the end of the observation period (5th May 2022), whichever came first.
Outcomes
Study outcomes were a composite outcome of disease progression (all-cause mortality, initiation of invasive mechanical ventilation [IMV], or intensive care unit [ICU] admission) and their individual outcomes, and lower viral load of cycle threshold (Ct) value ≥30 cycles. Hospital length of stay (LOS) was also determined for discharged survivors. In response to an upsurge of COVID-19 cases during the study period and the limited number of hospital beds, the HA had revised their discharge criteria on 26th February 2022 to allow patients hospitalized with COVID-19 to be discharged as early as they were deemed clinically stable by their attending physicians, and provided that their residential premises were suitable for isolation or they would be accepted by community isolation facilities, where they would continue their isolation until negative test results were obtained (on days 6 and 7 for fully vaccinated individuals [with at least two doses]; and day 14 for those not fully vaccinated [unvaccinated or vaccinated with only one dose]) 16.
Over the follow-up period, changes in the proportion of patients in respective clinical status (namely in-hospital death, on supplemental oxygen or mechanical ventilation, without oxygen therapy, and discharged) were compared between molnupiravir and control groups.
Baseline Covariates
Baseline covariates of patients included age, sex, symptomatic presentation, Charlson Comorbidity Index (CCI), concomitant treatments initiated on the index date (antibiotics, dexamethasone and other systemic steroids, interferon-β-1b, baricitinib, tocilizumab, and paracetamol), COVID-19 vaccination status (fully vaccinated [with at least two doses of Comirnaty or 3 doses of CoronaVac), and laboratory parameters at admission (Ct value, lactate dehydrogenase, C-reactive protein, and lymphocyte count).
Statistical Analyses
Propensity-score models conditional on the aforementioned baseline covariates in a logistic regression model was performed, and the propensity of receiving each oral antiviral was estimated. Missing laboratory parameters (Supplementary Table 1) for oral antiviral users were imputed 20 times using other parameters in the propensity-score model 17. We applied Rubin’s rules to pool the treatment effects estimated from the 20 independent imputed datasets 18. We used the standardized mean difference (SMD) to assess the balance of each baseline covariate between the groups before and after propensity-score matching, with SMD greater than 0.1 indicating covariate imbalance 19.
Hazard ratios (HR) with 95% confidence intervals (CI) of each outcome between oral antiviral users and non-users were estimated using Cox regression models. Further analysis on the head-to-head comparison of molnupiravir and nirmatrelvir/ritonavir on each outcome was performed after re-matching baseline covariates of two oral antiviral groups.
All statistical analyses were performed using Stata version 17 (StataCorp LP, College Station, TX). All significance tests were 2-tailed, where P-value <0.05 was considered statistically significant.
Results
In this territory-wide, retrospective cohort study, a total of 40,776 hospitalized patients with confirmed diagnosis of SARS-CoV-2 infection over a mean follow-up of 41.3 days with 925,713 person-days were identified from 26th February 2022 to 26th April 2022, where 2,359 and 1,000 were prescribed molnupiravir and nirmatrelvir/ritonavir during admission on or before 26th April 2022, respectively (Figure 1). Baseline characteristics of oral antiviral and control groups before matching are presented in Supplementary Table 2. After 1:4 propensity-score matching, this analysis included 2,116 molnupiravir users (with 8,396 matched control) and 991 nirmatrelvir/ritonavir (with 3,952 matched control) with COVID-19 not initially requiring any oxygen therapy at baseline. After matching, propensity score distribution of oral antiviral and matched control groups were highly overlapping (Supplementary Figure 1) while baseline characteristics of patients were balanced between oral antiviral and matched control groups with all SMDs <0.1 (Table 1). The median duration from symptom onset to molnupiravir initiation was 2 (interquartile range[IQR]: 1-3) days, and that from symptom onset to nirmatrelvir/ritonavir initiation was 2 (IQR: 1-3) days. The proportion of molnupiravir who received molnupiravir 800mg twice daily for 5 days was 96.2% while the proportion of nirmatrelvir/ritonavir users who completed the 5-days regimen (nirmatrelvir 300mg with ritonavir 100mg twice daily for 5 days) was 98.5%.
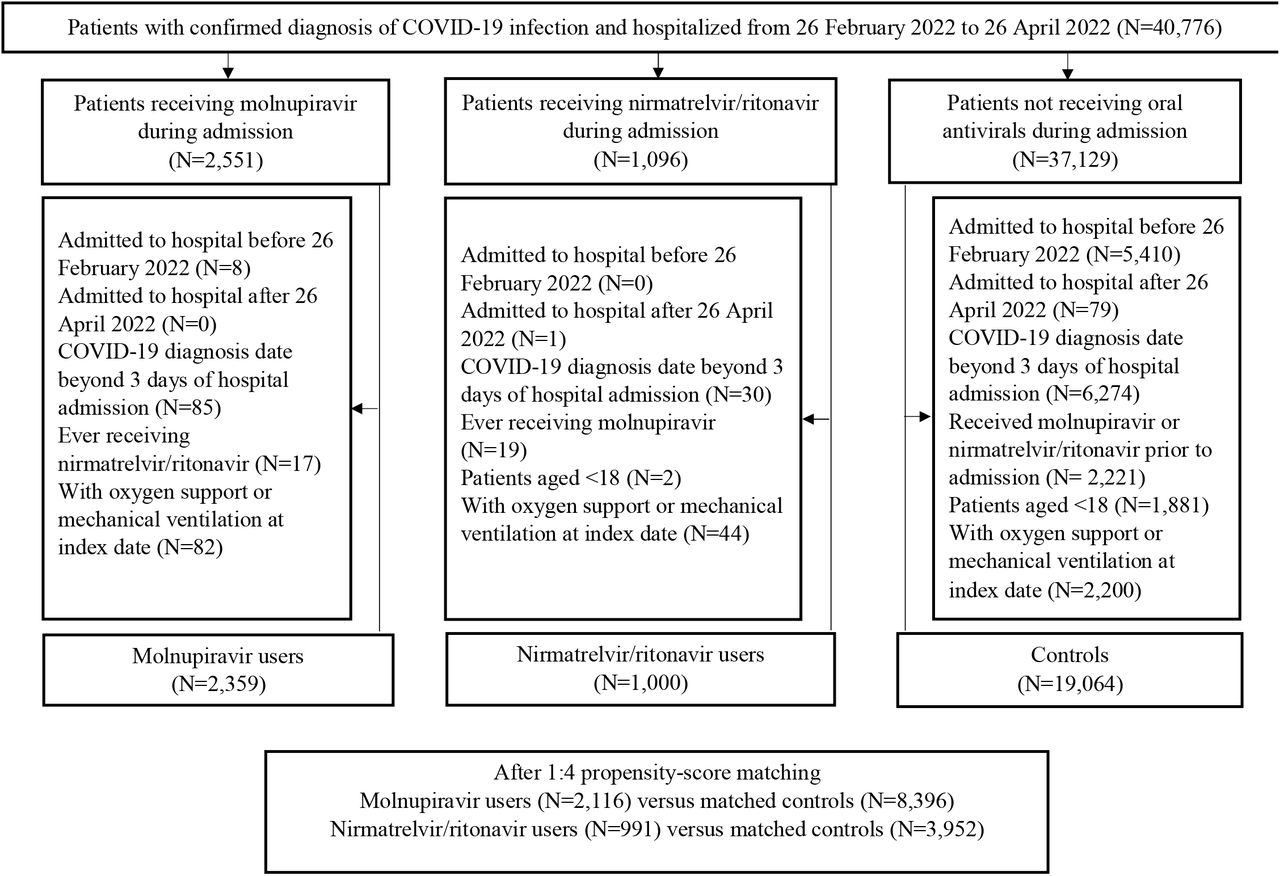
Identification of molnupiravir users, nirmatrelvir/ritonavir users, and their matched controls among patients hospitalized with COVID-19 not requiring oxygen therapy from 26 February 2022 to 26 April 2022 in Hong Kong
Baseline characteristics of inpatients with COVID-19 in (a) molnupiravir and respective matched control groups, and (b) nirmatrelvir-ritonavir and respective matched control groups after 1:4 propensity score matching
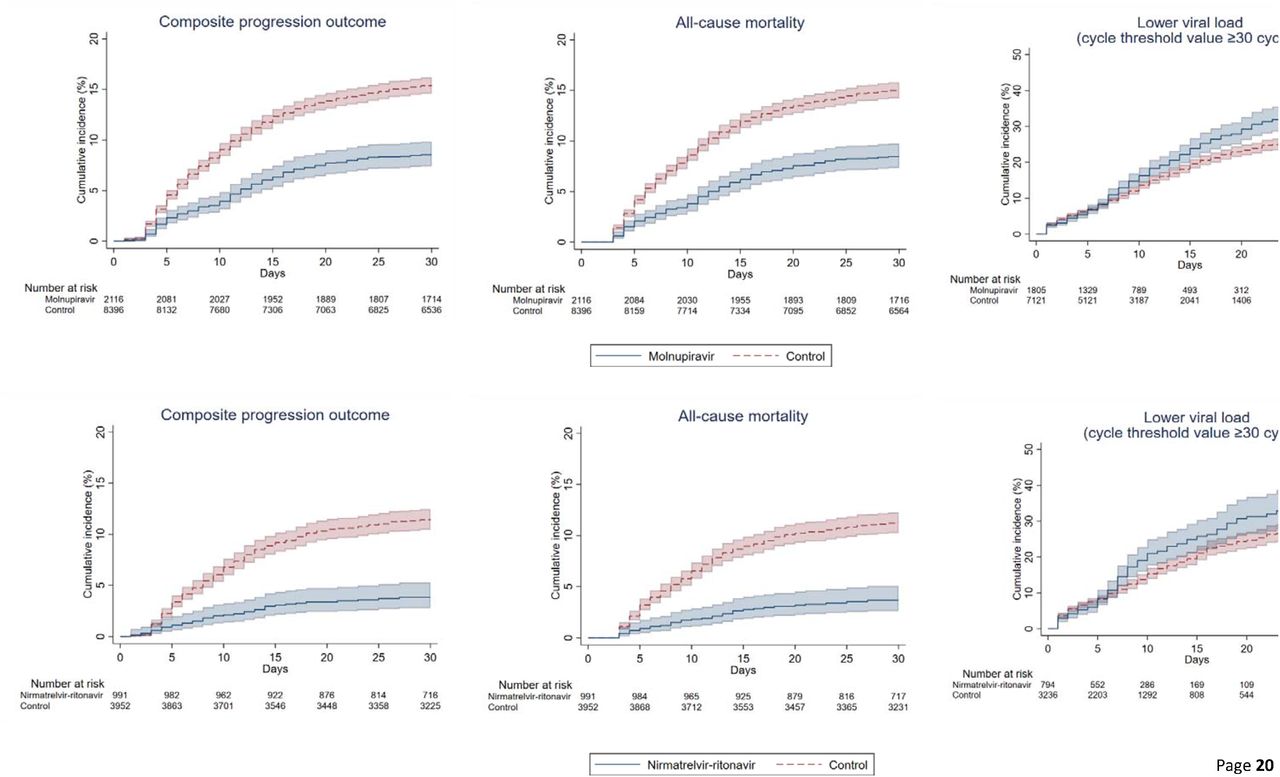
The crude incidence rates of all-cause mortality and IMV were 22.24 and 1.06 events per 10,000 person-days among molnupiravir users, 11.04 and 1.75 events per 10,000 person-days among nirmatrelvir/ritonavir users (Table 2). Oral antiviral use was associated with a significantly lower risk of the composite outcome of disease progression (molnupiravir: HR=0.53, 95%CI=0.46-0.62, p<0.001; nirmatrelvir/ritonavir: HR=0.33, 95%CI=0.24-0.46, p<0.001) than non-use, which was consistently observed for all-cause mortality (molnupiravir: HR=0.55, 95%CI=0.47-0.63, p<0.001; nirmatrelvir/ritonavir: HR=0.32, 95%CI=0.23-0.45, p<0.001) (Table 2 and Figure 2). Molnupiravir users had lower risks of IMV (HR=0.31, 95%CI=0.16-0.61, p<0.001). Time to achieving lower viral load was significantly shorter among oral antiviral users than matched controls (molnupiravir: HR=1.21, 95%CI=1.07-1.37, p=0.002; nirmatrelvir/ritonavir: HR=1.25, 95%CI=1.04-1.50, p=0.015) (Table 2 and Figure 2). Amongst survivors, nirmatrelvir/ritonavir had shorter length of hospital stay (−0.70 days, 95%CI=-1.37 to -0.04, p=0.039) than matched controls.
Hazard ratios of clinical and virologic outcomes for a) molnupiravir users versus their matched controls, and b) nirmatrelvir/ritonavir users versus their match controls, and differences in hospital length of stay between the groups amongst discharged survivors

Cumulative incidence plots of (a) composite progression outcome, (b) all-cause mortality, and (c) lower viral load for molnupiravir users versus t matched controls, and (a) composite progression outcome, (b) all-cause mortality, and (c) lower viral load for nirmatrelvir/ritonavir users versus their match controls
Since day-3 from baseline, the proportion of patients with in-hospital death was noticeably higher in the control group than oral antiviral users (Molnupiravir: 1.4% vs 0.6%; nirmatrelvir/ritonavir: 1.1% vs 0.4%), which persisted until day-28 of follow-up (Molnupiravir: 14.8% vs 8.3%; nirmatrelvir/ritonavir: 10.3% vs 3.2%) (Figure 3). The proportion of patients discharged was generally comparable between oral antiviral and matched control groups throughout the observation period.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comparison of disease status at days 3, 7, 14, 21, and 28 after the index date (hospital admission) a) between molnupiravir users and their matched controls, and b) between nirmatrelvir/ritonavir users and their matched controls
Table 3 demonstrates a head-to-head comparison of molnupiravir and nirmatrelvir/ritonavir after one-to-one propensity score matching, and reports higher risk of mortality (HR=1.53 95%CI=1.01-2.31, p=0.047) and longer length of hospital stay (0.83 days, 95%CI=0.07-1.58, p=0.032) for molnupiravir users.
Hazard ratios of clinical and virologic outcomes for molnupiravir users versus nirmatrelvir-ritonavir users, and differences in hospital length of stay between the groups amongst discharged survivors
Discussion
In this retrospective cohort of COVID-19 patients not requiring any supplemental oxygen on admission, initiation of molnupiravir or nirmatrelvir/ritonavir was associated with significantly lower risks of disease progression and all-cause mortality, in addition to achieving low viral load faster than their respective matched controls. Molnupiravir use was also associated with a significantly lower risk of IMV initiation; while nirmatrelvir/ritonavir users had a shorter length of hospital stay than their control counterparts. Furthermore, our head-to-head comparison suggested a relatively larger reduction in mortality risk with nirmatrelvir/ritonavir than molnupiravir use. To our knowledge, this is the first real-world study exploring the clinical use of oral antivirals during a pandemic wave dominated by the SARS-CoV-2 Omicron BA.2 variant.
Based on the very limited studies on the safety and efficacy of oral antivirals in COVID-19 patients, current guidelines and the medical community are now prioritizing their distribution to those who do not require supplemental oxygen, but who are at the highest risk of disease progression, i.e. who will likely benefit the most from antivirals 4,11,20,21. Our study cohort reflected such prescription pattern in real-world clinical practice; and provided real-world evidence supporting their use in those at risk of progression to severe disease, namely the elderly with multiple pre-existing comorbidities and who had not been fully vaccinated, during a pandemic wave dominated by the Omicron variant. The significant risk reduction in disease progression associated with both molnupiravir and nirmatrelvir/ritonavir was mainly driven by a substantial reduction in mortality risk, which has been illustrated in respective major clinical trials 22,23. Despite an inpatient setting of the current study, our patient population who did not require any supplemental oxygen at baseline was likely different from that of the MOVe-IN trial, where the majority presented with moderate-to-severe COVID-19 and approximately half of the patients were on oxygen therapy 24. Meanwhile, our molnupiravir users probably resembled those of the MOVe-OUT trial, where the antiviral was initiated early to patients with mild-to-moderate COVID-19 and risk factors for severe disease 23. Molnupiravir users were also more likely than the placebo group to achieve improved clinical outcomes and greater viral load reduction during follow-up 23.
Correspondingly, our results were in line with the latter establishing a significant mortality benefit and reduced disease progression (of increasing oxygen needs) among molnupiravir users, whilst these were not evident in the MOVe-IN trial when it was initiated at a later and more severe stage of COVID-19 23,24.
In terms of viral load reduction, our patients managed to achieve low viral load faster with molnupiravir or nirmatrelvir/ritonavir use upon SARS-CoV-2 infection of the Omicron variant, which added clinical support to the efficacy of oral antivirals demonstrated in experimental studies 25-29. In recent studies based on previous VOC (including Delta), early initiation of molnupiravir has been shown to promote clinical improvement and symptom resolution in patients with mild-to-moderate COVID-19, in addition to accelerating viral load reduction, SARS-CoV-2 RNA clearance, and elimination of infectious virus 23,30-32. The EPIC-HR trial was also conducted prior to the prevalence of Omicron variant, where nirmatrelvir/ritonavir use was associated with significant viral load reduction of Delta variant in patients with mild-to-moderate COVID-19 compared to placebo 20,22. To the best of our knowledge, this is the first clinical study offering real-world evidence of oral antiviral use among COVID-19 patients during a pandemic wave of Omicron variant.
Our head-to-head comparison between the two oral antivirals offers preliminary evidence confirming the prioritization of nirmatrelvir/ritonavir over molnupiravir in COVID-19 patients who do not require supplemental oxygen, whenever accessible and clinically appropriate 3,4,21. A relatively larger reduction in all-cause mortality risk was observed with nirmatrelvir/ritonavir use in this study, in addition to its greater efficacy in preventing COVID-19-related hospitalization than molnupiravir in previous trials, and without the risk of host mutational activity 11. Recently, an experimental study hypothesized that the efficacy of different antivirals may be influenced by their drug concentrations in the lungs of COVID-19 patients 33. For instance, both remdesivir and EIDD-1931 (active metabolite of molnupiravir) have been identified as substrates of equilibrative nucleoside transporters (ENT) 1 and 2, while nirmatrelvir is not 33,34. During acute lung injury and tissue hypoxia induced by SARS-CoV-2 infection, ENT repression may contribute to lower pulmonary concentrations of remdesivir and EIDD-1931 compared to that of nirmatrelvir, hence the latter may demonstrate higher effectiveness in COVID-19 patients than remdesivir and molnupiravir with controversial findings 8,33. Nonetheless, further in vivo studies are needed to confirm such postulation, explore other potential mechanisms and their application to specific COVID-19 patient populations. While molnupiravir is recommended only when neither nirmatrelvir/ritonavir nor remdesivir are accessible or clinically appropriate, molnupiravir still has its own merit considering its ease of administration via the oral route (compared to parenteral administration for remdesivir), no apparent drug-drug interactions (which are significant for nirmatrelvir/ritonavir), and no dosage adjustment needed based on hepatic or renal impairment (which is necessary for nirmatrelvir/ritonavir) 1,3,4,20.
This territory-wide, retrospective cohort study of COVID-19 patients who did not initially require supplemental oxygen suggested that initiating oral antivirals within 2 days of admission was associated with significant risk reduction in disease progression and all-cause mortality, and achieving low viral load faster compared to non-use. Referring to the medical records of hospitalized cases who were closely monitored, clinical outcomes and procedures were systematically documented and analyzed. Medication adherence could also be guaranteed in an inpatient setting compared to oral antiviral users in the community.
Nevertheless, several limitations of our study should be acknowledged. Firstly, we cannot exclude the possibility of selection bias or confounding by indication in this observational study, despite our population-based cohort was fully representative of the local COVID-19 patient population who did not require supplemental oxygen on admission. Besides, the clinical profile of our patients who would be deemed at risk of progression to severe COVID-19 might be different from those in the major trials of molnupiravir and nirmatrelvir/ritonavir, for instance, their dominant risk factor was overweight or obesity 22,23, whilst ours was old age. Secondly, since the Ct value was no longer adopted as one of the discharge criteria during our study period, patients might have already been deemed clinically stable for discharge before reaching the specific cutoff. Accordingly, further studies are needed to confirm our findings on viral load reduction and length of hospital stay associated with oral antiviral use. Results from ongoing trials (namely PANORAMIC and RECOVERY) and observational studies are awaiting 35-39, and further research is needed to explore the safety and effectiveness of oral antivirals in different patient populations (especially by COVID-19 vaccination status and VOC), drug combinations, and other healthcare settings such as nursing homes or residential care facilities.
As proposed by the medical and research community, logistics and distribution issues should be adequately addressed by governments and the healthcare sector to meet ethical standards and promote optimal and equitable access in the face of limited supplies, such as developing an evidence-based scoring system or risk prediction tools to help physicians prioritizing the distribution of oral antivirals to COVID-19 patients who would most likely benefit from them, based on predicted efficacy and risk assessments 11,20,21. Notably, some unknown long-term risks associated with molnupiravir use include possible carcinogenicity and teratogenicity, as mutations have been observed in mammalian cells in vitro; and the risk of emergence of more infectious and vaccine-resistant viral variants attributed to the genetic mutations induced 7-9,40-42. Moreover, concerns about the development of drug resistance to molnupiravir and nirmatrelvir/ritonavir have been raised, especially considering the high mutation rates of SARS-CoV-2 and potential selective pressure induced by an extensive use of antiviral monotherapy 21,43. Active pharmacovigilance programs and sequencing of viral mutations are essential to monitoring their long-term safety and effectiveness in different patient populations and waves of COVID-19 pandemic 21.
In conclusion, this retrospective cohort study of COVID-19 patients who did not initially require supplemental oxygen suggested that early initiation of oral antivirals was associated with significant risk reduction in disease progression and all-cause mortality, as well as achieving low viral load faster than non-use. Furthermore, a relatively larger reduction in mortality risk could be observed with nirmatrelvir/ritonavir use compared to molnupiravir during a pandemic wave of the SARS-CoV-2 Omicron BA.2 variant. Ongoing research will inform the safety and effectiveness of oral antivirals in specific patient populations, drug combinations, and healthcare settings.
Data Availability
The clinical outcome data were extracted from the Hospital Authority database in Hong Kong and vaccination records were extracted from the eSARS data provided by the Centre for Health Protection. Restrictions apply to the availability of these data, which were used under license for this study.
Contributors
The study was designed by CKHW, GML and BJC. The underlying data was verified by CKHW, ICHA and EHYL, and data analyses were done by CKHW and ICHA. CKHW and KTKL wrote the first draft of the manuscript which was revised by GML and BJC. All authors interpreted data, provided critical review and revision of the text and approved the final version of the manuscript.
Data Sharing
The clinical outcome data were extracted from the Hospital Authority database in Hong Kong and vaccination records were extracted from the eSARS data provided by the Centre for Health Protection. Restrictions apply to the availability of these data, which were used under license for this study.
Declaration of interest
BJC reports honoraria from AstraZeneca, Fosun Pharma, GlaxoSmithKline, Moderna, Pfizer, Roche and Sanofi Pasteur. The authors report no other potential conflicts of interest.
Footnotes
↵* Full professors
References



