
Abstract
Importance/Background Despite the global healthcare’s exhaustive efforts to treat COVID-19, we still do not have an effective cure for it. Repurposing Ivermectin, a known antiparasitic agent, for treating COVID-19 has demonstrated positive results in several studies. We aim to evaluate the benefit and risk of Ivermectin in COVID-19.
Methods We conducted a systematic search for full-text manuscripts published from February 1, 2020 to March 27, 2021 that focused on efficacy and safety of Ivermectin therapy against COVID-19. The primary outcomes were overall mortality, need for intensive care unit (ICU) admission; secondary outcomes were - adverse effects, need for mechanical ventilation. Random-effects models were used for all analysis.
Results We included a total of 38 studies (n=15,002) in the qualitative analysis (Mortality N=28, ICU admission= 8, Mechanical Ventilation= 10, Adverse events=28) and out of these, 30 studies (n=11,291) were included in the quantitative analysis (Mortality N=22, ICU admission= 5, Mechanical Ventilation= 9, Adverse events=17). In the mortality meta-analysis, odds of death were lower in the Ivermectin-arm compared to the non-Ivermectin arm. (OR 0.39, 95% CI 0.22-0.70; I2=81%). Subgroup analysis of 12 randomized controlled trials with severity-based data showed mortality benefit overall (OR 0.33, 95% CI 0.15-0.72; I2=53%) and in the mild/moderate sub-group (OR 0.10, 95% CI 0.03-0.33; I2=0%). Benefit of Ivermectin in decreasing; the need for ICU admission (OR 0.48, 95% CI 0.17-1.37; I2=59%) and mechanical ventilation (OR 0.64, 95% CI 0.40-1.04; I2=17%) was not significant. The quantitative analysis of adverse effects with Ivermectin use was inconclusive (OR 0.92, 95% CI 0.64-1.33; I2=14%).
Conclusion Our meta-analysis suggests that Ivermectin could be an effective adjuvant therapy in reducing mortality, particularly in patients with mild-moderate clinical presentation of COVID-19. Trends of decreased need for ICU admissions and mechanical ventilation were observed but were not significant. The analysis for adverse effects was inconclusive.
What We Already Know about This Topic
COVID-19 is an ongoing global pandemic, for which Ivermectin has been tried on a therapeutic and prophylactic basis.
Results from several clinical trials and observational studies suggest that Ivermectin may improve survival and clinical outcomes with a good safety profile when compared with other treatments; however, the current evidence is limited.
What This Article Tells Us That Is New
This systematic review and meta-analysis provide a summary of the latest literature on the efficacy and safety of Ivermectin use for COVID-19.
Based on our quantitative and qualitative analysis, we found that Ivermectin may be a potentially useful adjuvant therapy in reducing mortality, the need for ICU admissions and mechanical ventilation in COVID-19 patients.
Introduction
On March 11, 2020, the World Health Organization (WHO) declared COVID-19 disease a global pandemic1. Today, on April 29,2021, there are about >149 million confirmed cases worldwide and >3 million deaths due to COVID-192. Patients infected with SARS-COV-2, the causative Coronavirus, exhibit a spectrum of clinical presentations ranging from asymptomatic to severely critical and multiple risk factors are involved in the prognosis of the disease3-8. To guide decision-making for this multi-system disease8-17, a variety of treatment modalities have been proposed and evaluated18-23. However, the evidence for the risk-benefit ratio of most of these treatments remains unclear.
Ivermectin has held an excellent safety record in humans as an antiparasitic agent for over three decades24. Apart from its established activity against several parasites, Ivermectin has demonstrated antiviral activity against many RNA and DNA viruses in vivo and against a few in vitro by targeting specific proteins25. One such plausible mechanism against RNA viruses is the inhibition of importin (IMP) α/β Integrase, thus blocking viral entry into the nucleus and the ensuing suppression of the cell’s anti-viral response25-28. Moreover, it exhibited anti-bacterial, anti-inflammatory, and anti-cancer effects24,29,30. An Australian study demonstrated the effectiveness of Ivermectin in inhibiting SARS-COV2 in-vitro31. Subsequently, several Ivermectin-based clinical trials and observational studies conducted globally showed mostly positive results32-35. Some countries have incorporated this therapy in their COVID-19 guidelines36-39. Only a month after this authorization, Peru witnessed a record drop of 25% in COVID-19 related mortality40.
Dr. Satoshi Ōmura, who was among the scientists that won the Nobel prize for the discovery of Ivermectin, highlighted the need to develop a drug that arrests the early stage of viral replication in COVID-1941. Repurposing Ivermectin, a low-cost drug may help bypass the time and funds needed to develop and test novel therapies. The lack of robust evidence has been a major hindrance in the large-scale approval of Ivermectin. The available studies are methodologically diverse and mostly under-powered while few report conflicting results. Therefore, we intend to systematically review the latest literature and plan to perform a meta-analysis to overcome some of the individual study biases.
Methods
Search Method and strategy
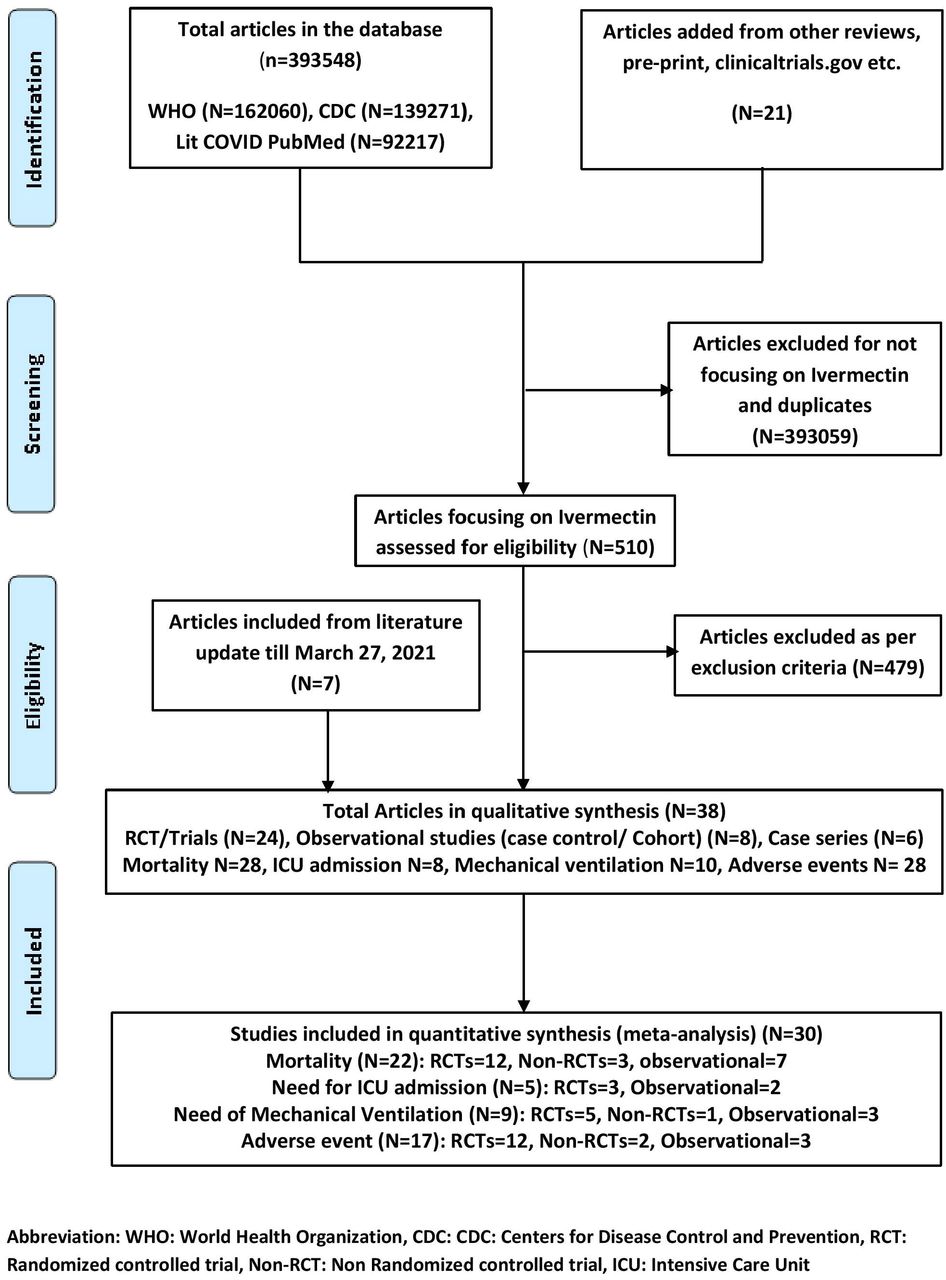
We conducted a comprehensive literature search for studies mentioning the use of Ivermectin in COVID-19 from February 1, 2020 till March 27, 2021 (Figure 1). We screened all titles and abstracts identified by preliminary search for eligible studies and manually searched references of included articles for additional studies. Then we analyzed full-text manuscripts of included studies according to the protocol of Systematic Review and Meta-Analysis (PRISMA) guidelines.

Eligibility Criteria
We included studies reporting outcomes of mortality, ICU admission, mechanical ventilation, and adverse-effects with Ivermectin treatment against COVID-19. We excluded studies focusing on pregnant females, in-vitro studies, meta-analyses, case reports and case series <5 patients.
Study selection and data extraction
The extracted data was tabularized in Microsoft Excel with following parameters: author, country of study, study design, number of patients, Ivermectin regimen, concomitant treatment, efficacy outcomes and adverse effects. The included data was checked for accuracy by all authors and disagreements were resolved through consensus and after input from a third reviewer. IRB approval was exempted because data was extracted from publicly available studies. We also analyzed raw data files of studies by Cadegiani42 and Lima-Morales et al43 for cases receiving Ivermectin; and Niaee et al44 for clinical severity data. In Cadegiani et al’s study42, we considered ‘CG1’ as control group because only this sample was demographically comparable to the treatment group. Bernigaud et al.’s study45 was excluded because the methodology and outcomes were poorly described. Additionally, we compiled all ongoing clinical trials on Ivermectin from clinicaltrials.gov (e-table 8).
Outcomes
The primary outcome was defined as mortality benefit with Ivermectin therapy in COVID-19 and need for ICU admission. The secondary outcomes were need for mechanical ventilation and adverse effects of Ivermectin.
Statistical analysis
Primary and Secondary outcomes were quantitatively analyzed by Review Manager (RevMan) Version 5.4 for windows46 and Comprehensive Meta-Analysis software package (Biostat, Englewood, NJ, USA)47 was used for qualitative-analysis. Random-effects model was used for both48. Raw data for outcomes and non-events from each study were used to calculate crude odds ratio (OR) with 95% confidence intervals (CI) for each study. The Cochrane Q and I2 statistics were calculated to assess heterogeneity between studies48. I2 <25% were interpreted as low-level heterogeneity48. We performed subgroup analysis by study design to decrease inherent selection bias in observational studies48. Probability of publication bias was assessed with funnel plot using Egger’s tests48 (e-figure 14-19). If there was statistical heterogeneity in results, further sensitivity analysis was conducted to determine the source of heterogeneity by excluding each study. After significant heterogeneity was excluded, random-effects model was used for meta-analysis. P-value <0.05 (2-sided) was considered statistically significant48.
Risk of Bias and Quality assessment
Clinical trials were evaluated using Cochrane risk of bias tool49 (e-table 2) and correlation of quality measures with estimates of treatment effects in meta-analyses of randomized controlled trials tool50 (e-table 3) was used for quality assessment. We used NIH quality assessment Tool for case series51 (e-table 4), case-control (e-table 5), or cohort studies (e-table 6). NIH quality assessment tools were based on quality assessment methods, concepts, and other tools developed by researchers in the Agency for Healthcare Research and Quality (AHRQ), Cochrane Collaboration, USPSTF, Scottish Intercollegiate Guidelines Network, and National Health Service Centre for Reviews and Dissemination, consulting epidemiologists and evidence-based medicine experts, with adaptations by methodologists and NHLBI staff. We assessed the certainty of evidence by using GRADE pro profiler52 (GRADE working group, McMaster University and Evidence Prime Inc) at the outcome level (e-table 7).
Results
Study Characteristics
A total of 15002 patients from 38 articles32-35,42-44,53-83 (Ivermectin n=6669, No Ivermectin n=8333) were included in qualitative analysis, 11291 patients from 30 studies (Ivermectin n=2996, No Ivermectin n=8295) were included in quantitative synthesis (e-table 1, Figure 1). Out of 24 trials, 19 were true RCTs (e-table 1, Figure 1). The remaining 14 studies were observational and included 6 case-series (e-table 1, Figure 1). Out of 38, 16 articles were available as preprints and clinicaltrials.gov was used for data extraction for 2 trials76,84 (e-table 1, Figure 1). We only included the patients treated therapeutically in the study by Elgazzar et al64. Due to absence of informed consent, blinding and randomization, we considered Veerapaneni et al’s83 study as case control study.
Primary Outcomes
Mortality
Meta-analysis
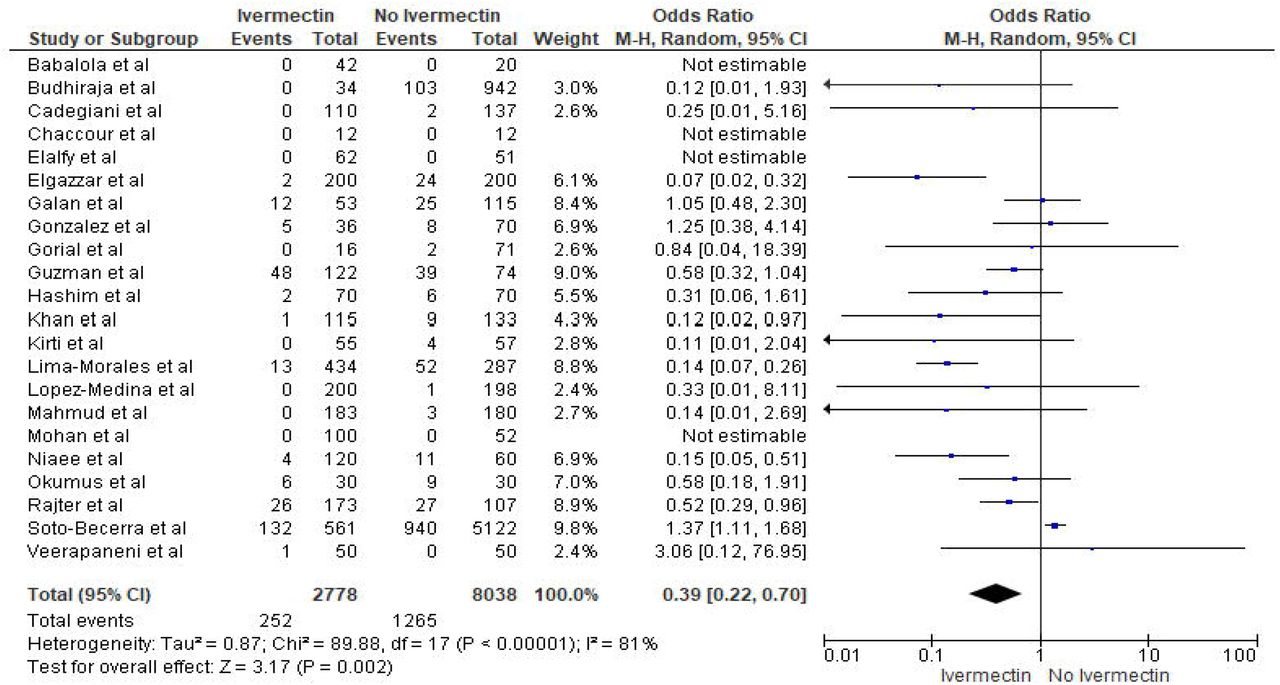
Overall
Total 22 studies reported mortality rate in patients receiving Ivermectin (252/2778) vs no-Ivermectin therapy (1265/8038). The odds of mortality in the Ivermectin group were significantly lower compared to control group (OR 0.39, 95% CI 0.22-0.70, p=0.002; I2=81%) (Figure 2A) but evidence was graded very low. In sensitivity analysis, we observed similar mortality benefit with moderate heterogeneity after excluding study by Soto-Becerra et al82 (OR 0.36, 95% CI 0.22-0.58, p<0.001; I2=56%) (Figure 2B).

Subgroup analysis by study design
Subgroup: Clinical trials
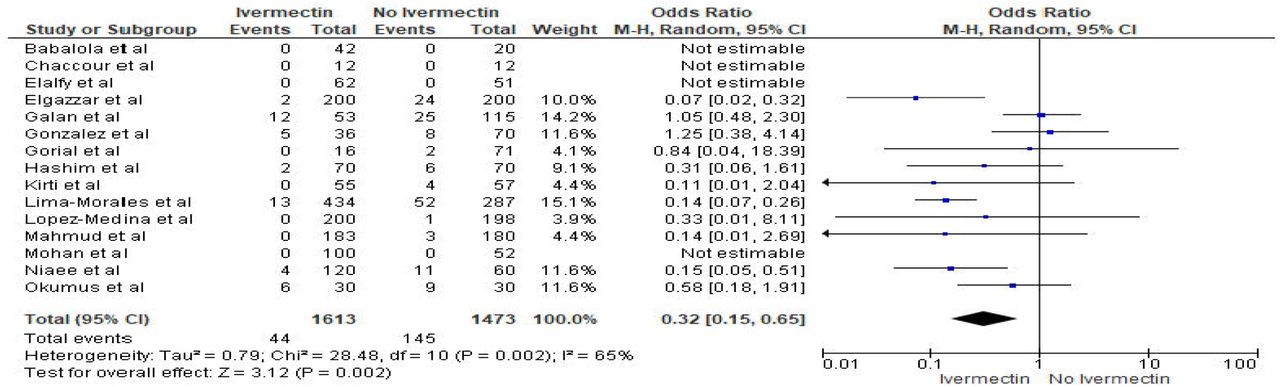
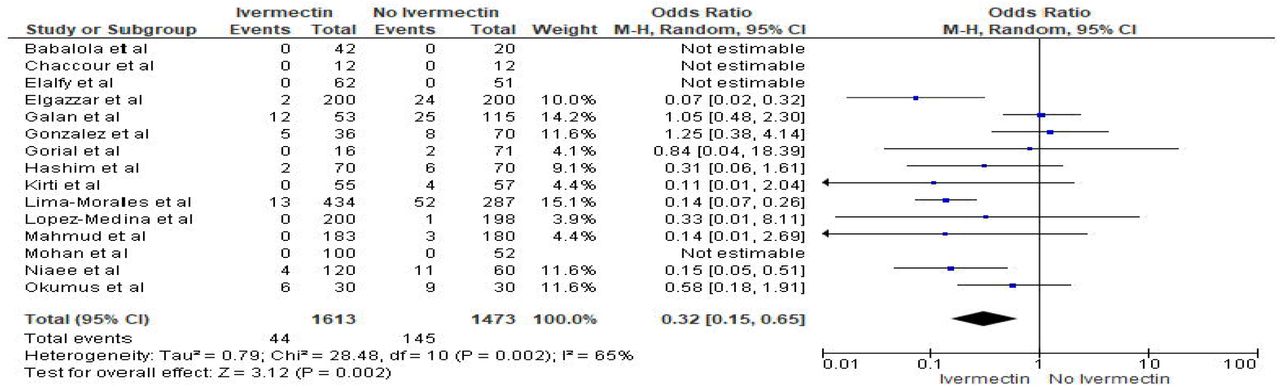
We performed subgroup analysis of 15 clinical trials (RCTs N=12, Non-RCTs N=3) and observed similar mortality benefit (OR 0.32, 95% CI 0.15-0.65, p=0.002; I2=65%) (Figure 3A) but evidence was graded very low. On excluding Galan et al66 for sensitivity analysis, benefit observed was more solid with moderate heterogeneity (OR 0.26, 95% CI 0.13-0.50, p<0.001; I2=46%) (e-figure 1)
Subgroup: RCTs
We analyzed clinical severity-based data in 12 RCTs. The odds of mortality were lowered with Ivermectin in the overall group, with moderate heterogeneity (OR 0.33, 95% CI 0.15-0.72, p=0.005; I2=53%) Similar benefit was observed in the mild/moderate subgroup (OR 0.10, 95% CI 0.03-0.33, p=0.002; I2=0%). However, mortality benefit was not statistically significant in the severe/critical subgroup (OR 0.53, 95% CI 0.23-1.23, p=0.14; I2=57% (Figure 3B). Certainty of evidence was moderate overall; however, it was high in mild/moderate and moderate in severe/critical subgroup. Therefore, in mild/moderate COVID-19 patients, Ivermectin could be used for reducing mortality.
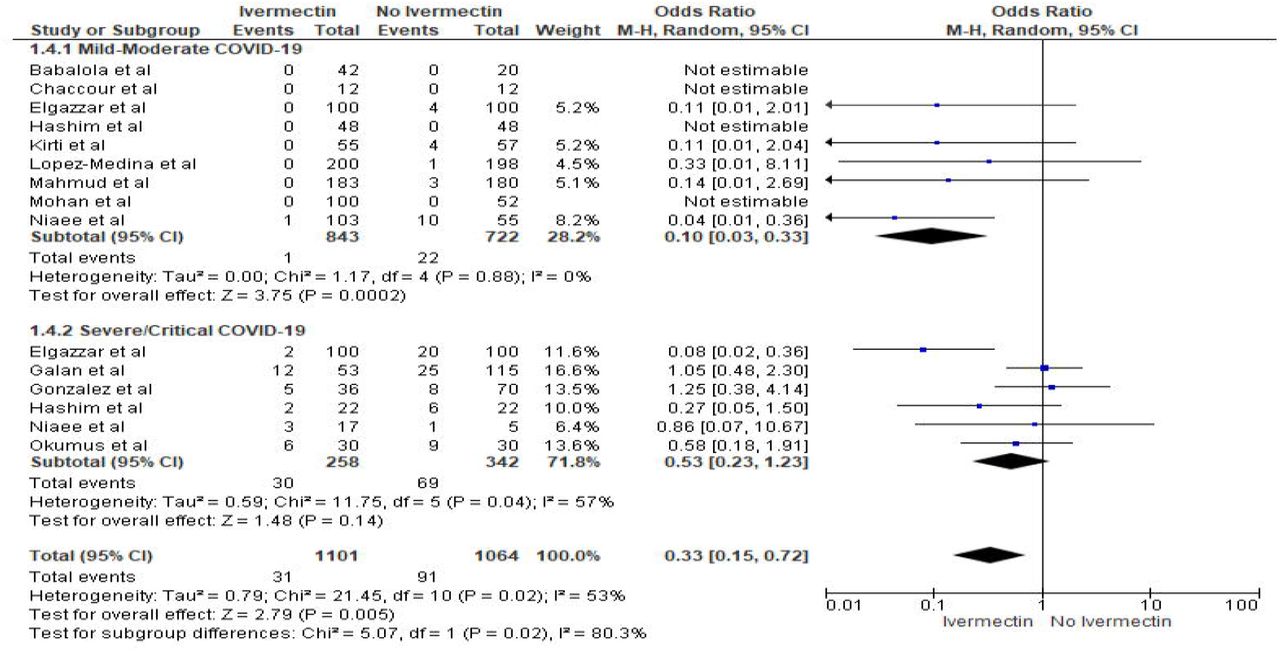
In sensitivity analysis, after excluding Elgazzar et al64 from the severe/critical subgroup, odds of mortality increased in the total group, with moderate heterogeneity (OR 0.43, 95% CI 0.21-0.90, p=0.02; I2=39%). The odds increased in the severe/critical subgroup, with no heterogeneity (OR 0.84, 95% CI 0.49-1.43, p=0.53; I2=0%), but remained statistically insignificant (e-figure 2).
Observational studies
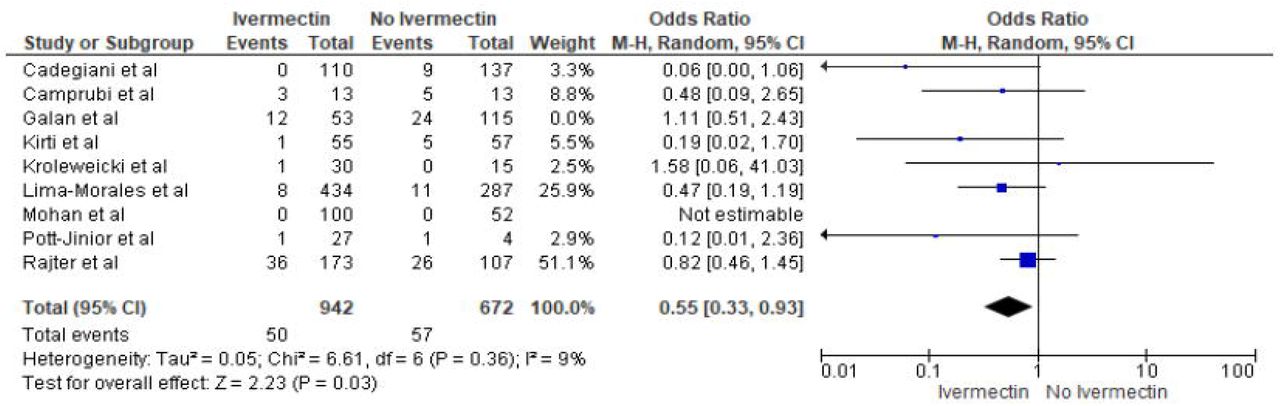
Mortality benefit was not statistically significant in subgroup of 7 observational studies (OR 0.61, 95% CI 0.30-1.22, p=0.16; I2=74%) (Figure 3C) and evidence was graded very low. On excluding Soto-Becerra et al82 in sensitivity analysis, we observed statistically significant mortality benefit (OR 0.51, 95% CI 0.34-0.77, p=0.001; I2=0%) (e-figure 3).

Subgroup analysis for hospitalized patients
Overall
Subgroup analysis for hospitalized patients (studies N=15) showed mortality benefit with high heterogeneity (OR 0.48, 95% CI 0.28-0.83, p=0.009; I2=75%) (e-figure 4). After excluding Soto-Becerra et al82 in sensitivity analysis, we observed similar benefit with acceptable heterogeneity (OR 0.43, 95% CI 0.26-0.71, p=<0.01; I2=48%) (e-figure 5).
Subgroup: Inpatient RCTs
Analysis of RCTs (N=8) with only hospitalized patients showed similar mortality benefit (OR 0.36, 95% CI 0.15-0.87, p=0.02; I2=67%) (e-figure 6). Evidence was graded moderate. After excluding Galan et al66 in sensitivity analysis, mortality benefit with moderate heterogeneity was seen (OR 0.28, 95% CI 0.11-0.73, p=0.009; I2= 59%) (e-figure 7).
Subgroup: Inpatient Observational studies
Mortality benefit was also seen in 6 observational studies with only hospitalized patients, with high heterogeneity (OR 0.63, 95% CI 0.31-1.29, p=0.21; I2=77%) (e-figure 8). Evidence was graded very low. In sensitivity analysis, after excluding Soto-Becerra et al82 significant mortality benefit was seen with low heterogeneity (OR 0.51, 95% CI 0.32-0.81, p=0.005; I2=10%) (e-figure 9).
Qualitative Analysis for mortality
Pooled analysis of 28 studies out of 38 studies, yielded a rate of 3.5%, 95% CI 1.8-6.6; I2=95.1% (e-figure 10).
Need for ICU admission
Meta-analysis
In 5 studies (out of 30), 27/263 in the Ivermectin arm, 52/322 in the control arm needed ICU admission. Benefit with Ivermectin was not statistically significant (OR 0.48, 95% CI 0.17-1.37, p=0.17; I2=59%) (Figure 4A). Evidence was graded very low. In sensitivity analysis, after excluding Galan et al66 we observed statistically significant benefit (OR 0.32, 95% CI 0.11-0.92, p=0.03; I2=27%) (Figure 4B). Based on low grading of evidence and observed low-moderate heterogeneity in analysis, Ivermectin may be helpful in decreasing need for ICU admission. Further validation with well-designed pragmatic platform trials is needed.


Qualitative Analysis
Pooled ICU admission rate obtained from 8 studies (out of 38) was 5.4%, 95% CI 1.9-14.7; I2=91.9% (e-figure 11).
Secondary Outcomes
Need for Mechanical Ventilation
Meta-analysis
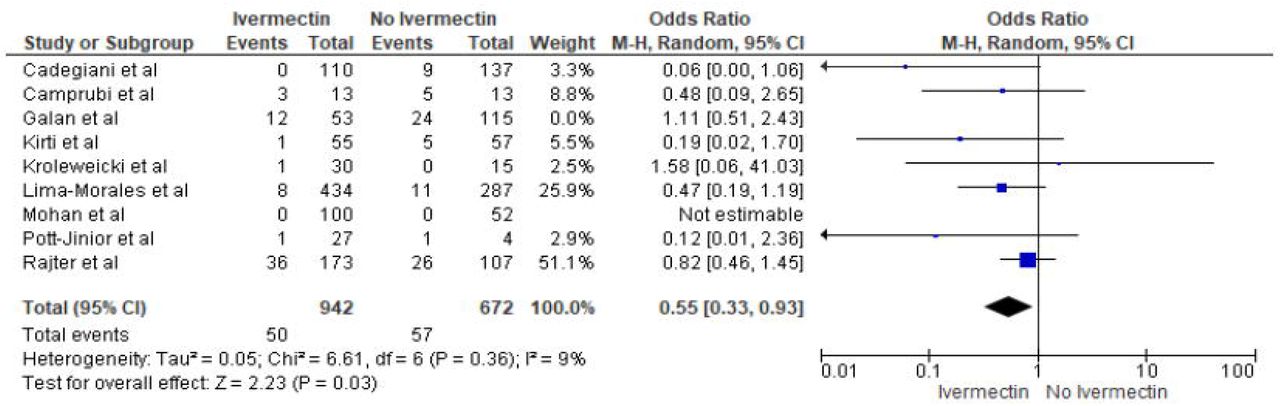
Overall, 9 studies documented the need for mechanical ventilation. 62/995 patients receiving Ivermectin and 81/787 patients in the control arm required mechanical ventilation. The benefit of Ivermectin was statistically insignificant (OR=0.64, 95%CI 0.40-1.04, p=0.07; I2=17%) (Figure 4C). Evidence was graded very low. On excluding Galan et al66 in sensitivity analysis, benefit observed was statistically significant with low heterogeneity (OR 0.55, 95% CI 0.33-0.93, p=0.03; I2=9%) (Figure 4D). Although the evidence was low, Ivermectin may confer significant protection against the need for mechanical ventilation. Hence, we would suggest considering Ivermectin with bedside clinician’s judgement.

Qualitative Analysis
The rate of need for mechanical ventilation based on 10 studies (out of 38) was 4.4%, 95% CI 1.6-11.1; I2=88.8% (e-figure 12).
Adverse events
Meta-analysis
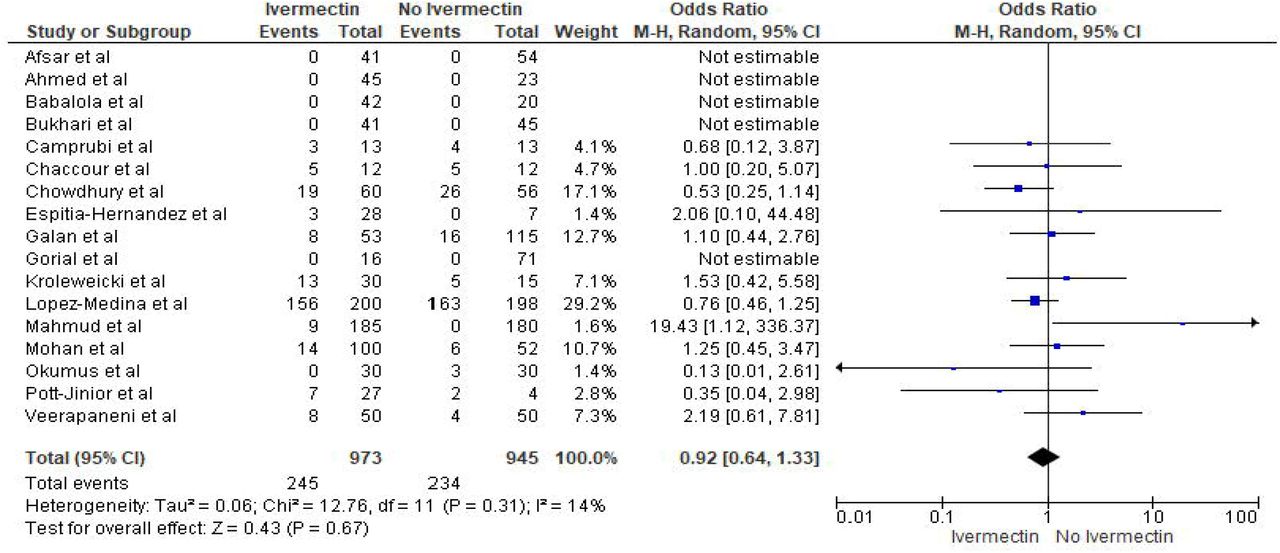
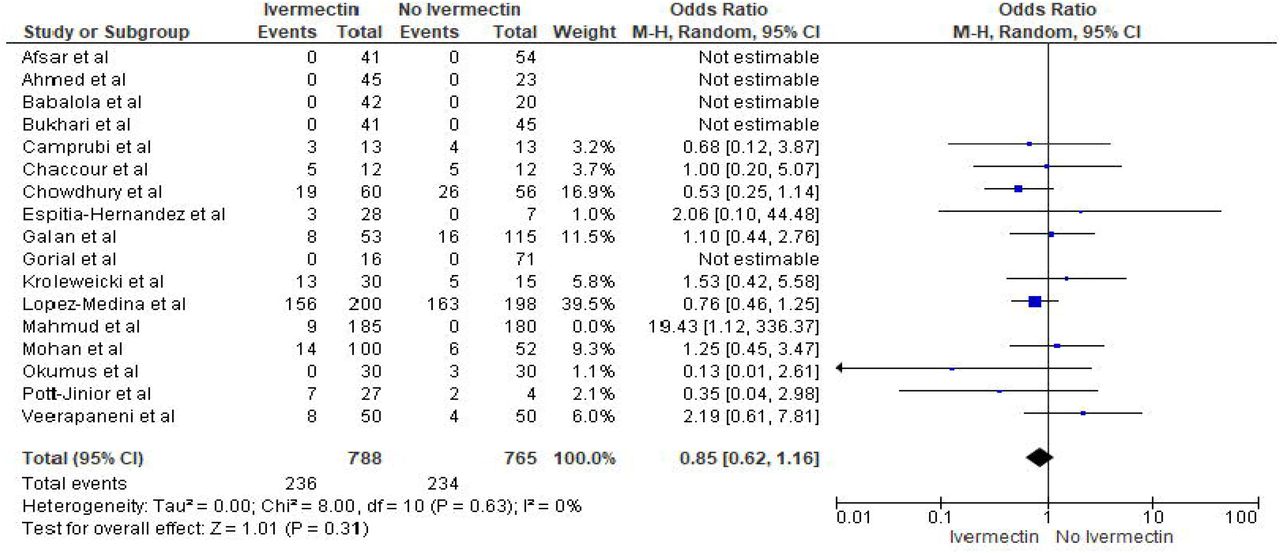
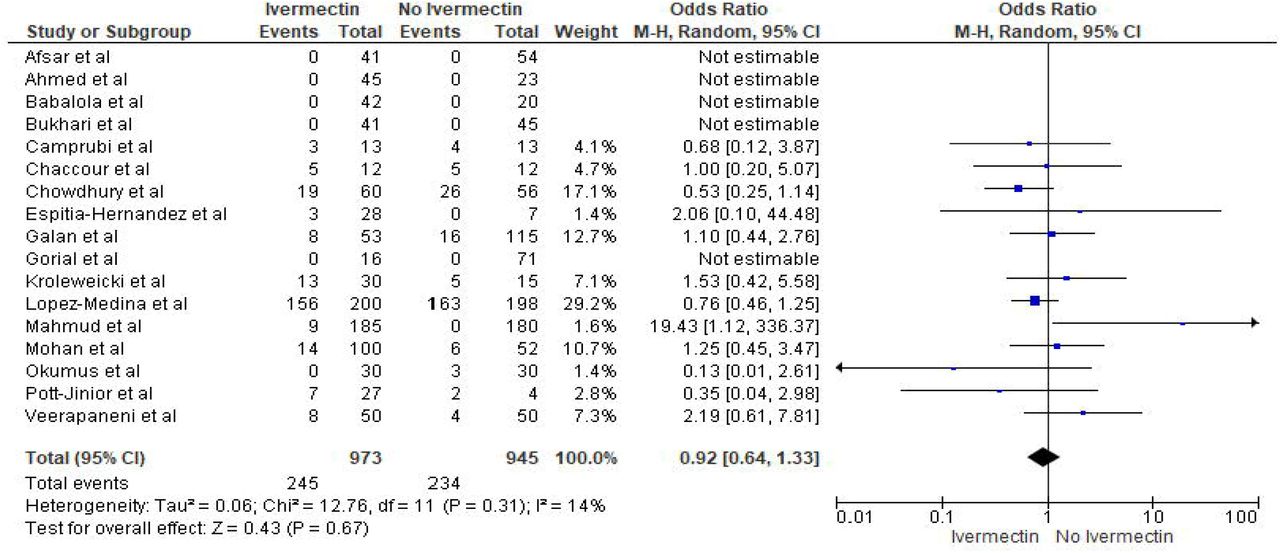
A total of 17 studies reported data for rate of adverse-events in the Ivermectin-arm (245/973) vs control group (234/945). We did not find an association between Ivermectin and rate of adverse events as compared to controls (OR 0.92, 95% CI 0.64-1.33, p=0.67; I2=14%). (Figure 5A) but evidence was graded very low. In sensitivity Analysis, after excluding Mahmud et al76 incidence of adverse effects with Ivermectin was similar to that of the control group but was not conclusive (OR 0.85, 95% CI 0.62-1.16, p=0.31; I2=0%) (Figure 5B).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Qualitative Analysis
A total of 28 studies (out of 38) yielded a pooled rate of 8.1%, 95% CI 4.2-14.8; I2=93.5% (e-figure 13).
Discussion
Our meta-analysis suggests that Ivermectin may improve survival in COVID-19 patients and reduce the need for admission to the ICU and mechanical ventilation. However, its relation to the incidence of adverse effects is inconclusive. Further, our qualitative analysis indicates that Ivermectin treatment is linked to lower death rate and better clinical outcomes with a low incidence of adverse effects. The inherent methodological limitations and risk of bias conferred variable evidence grading in the findings in various patient outcomes.
Mortality
Our findings are corroborated by other meta-analyses done by Padhy85 (studies N=3), Hill86 (studies N=6), Lawrie87 (studies N=5), Nardelli88 (studies N=7), Kow89 (studies N=6), Bryant et al90 (studies N=13) and the BIRD group91 (studies N=13) which found Ivermectin to be conclusively linked to lower mortality when compared to usual treatment. A network meta-analysis92 (studies N=2) reported that Ivermectin was linked to lower mortality with a very close statistical significance. Casteneda-Sabogal et al’s meta-analysis93 (studies N=6) found no conclusive association of Ivermectin with reduced mortality. Of note, the above two studies reported low or very low certainty of evidence92,93. Our sample size exceeds (studies N=22) that of all the aforementioned studies.
Our pooled analysis resulting in a low mortality rate of 3.5% with use of Ivermectin reiterates its positive impact in lowering mortality in COVID-19 patients. For a valid comparison, it is important to factor in the time window during which the individual studies were conducted. Most studies recorded their data in the II&III quarter of 2020 when mortality rates with various treatments were often higher in respective countries94.
Need for ICU admission and Mechanical Ventilation
Due to the small number of studies and their small individual sample size, benefit with Ivermectin in reducing ICU admissions or mechanical ventilation cannot be concluded with confidence. In our pooled analysis, we observed significantly lower rates for ICU admission (5.43%) and mechanical ventilation (4.36%) in Ivermectin-treated patients when compared to other treatments95-97. It must be noted that our pooled analysis mostly included mild/moderate patients, which may skew the results in favor of Ivermectin.
Adverse events
Our analysis for adverse events was inconclusive. We noticed that most adverse events were non-serious: nausea, vomiting, abdominal pain, diarrhea, pruritus, lethargy, vertigo, tingling, numbness, anxiety, mild hyperglycemia etc. Yet, very few patients reported serious events like organizing pneumonia, hyponatremia, erosive esophagitis, infections/infestations. Erosive esophagitis was attributed to concomitant use of Doxycycline76; hyponatremia74 was likely from SIADH-a rare COVID-19 complication98. Only Lopez-Medina et al75, that used a high Ivermectin dose of 1500ug/Kg over 5 days, reported drug discontinuation due to adverse-reactions. Given the non-serious nature of most adverse-reactions, and a low pooled rate of 8.1% in comparison to other available treatments23,99,100, we suggest that Ivermectin was generally well tolerated.
Strengths
To our knowledge, this is the largest patient sample size for a systematic review and meta-analysis on the use of Ivermectin for COVID-19. This study integrates data of approximately 15,000 patients from 38 studies conducted globally. Additionally, we obtained robust evidence by conducting various subgroup analyses. For a stronger empirical evidence of Ivermectin’s efficacy, we excluded studies which did not meet the rigor of true RCTs in the ‘RCTs’ subgroup for a ‘high’ rated level of evidence as per the GRADEpro tool52. The GRADE framework is known to be the most widely used assessment to rate quality of evidence52. Sensitivity analyses were performed when results were statistically weak. Moreover, we performed qualitative analyses to incorporate data from uncontrolled studies.
Limitations
Our results are to be interpreted carefully bearing in mind that we included several non-peer-reviewed articles to obtain the latest data. We cannot preclude the possibility of unreported biases and confounders that could have been recognized by a peer-review process. Furthermore, there was significant heterogeneity in treatment protocols used for dosage, duration, route of administration in interventional and control group. Our analyses may not have accounted for confounding by concomitant therapy. Patient demographics and outcome measures varied among different studies. Few studies documented the inclusion of patients <18 years of age. However, the mean/median, dispersion values consistently suggested a predominantly adult population. The clinical classification for severity was inconsistent across the included studies. Most studies were conducted on patients with mild /moderate presentation, which limits the generalizability of our results. There was insufficient data regarding the time of treatment in the course of the disease, hence inferences could not be made in that regard. We could not confirm adequate control-matching in some observational studies. We advise discretion in interpretation of our results for adverse-event rate since most of the reported adverse-effects could not be measured objectively by investigators. Because most of the studies were conducted in developing nations, not everyone underwent RT-PCR testing owing to limited resources; clinical diagnosis was used instead. Even though RT-PCR is the gold standard for diagnosis, it is subject to its limitations. By virtue of its design, we postulate that this meta-analysis formulated with a random-effects model may have addressed some of the heterogeneity stemming from the above factors. Lastly, we must acknowledge the subjective nature of the GRADE tool used to evaluate the level of evidence52.
Current status of Ivermectin
In February 2021, the NIH withdrew its recommendation against using Ivermectin for COVID-19101. Around the same time, WHO shared that they will thoroughly evaluate the available and upcoming evidence on Ivermectin before announcing any change in guidelines102. As of March 5,2021, the FDA has warned people against using Ivermectin for COVID-19103, specifically against self-medicating with veterinary Ivermectin formulations103,104. They are yet to review the evidence but have initiated a preliminary research. Recently, the EMA (European Medicines Agency) stated that Ivermectin cannot be recommended for the prevention or treatment of COVID-19 outside clinical trials105.
Conclusion
In summary, Ivermectin may have a role as an adjuvant treatment in decreasing mortality in mildly/moderately ill COVID-19 patients. Also, lower odds of ICU admissions and use of mechanical ventilation with Ivermectin use were noted but with very low evidence. The association with adverse events was inconclusive. Using well-designed larger observational studies106,107 and clinical trials, we need to investigate Ivermectin’s ideal dosage and timing in the disease course, drug interactions and possible synergistic drug combinations to achieve maximum benefit. We propose pragmatic practice embedded platform trials108 to test this and other re-purposed and novel therapies specifically in severe COVID-19 patients and other critically ill patients.
Data Availability
The data is available on our site.
Figure Legends
Figure 1: Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow— study inclusion. ICU: Intensive Care Unit, CDC: Centers for Disease Control and Prevention, RCT: Randomized controlled trial, WHO: World Health Organization
Figure 2: Meta-analysis for Ivermectin use and overall Mortality
Figure 3: Subgroup analysis by study design for Ivermectin use and mortality
Figure 4: Meta-analysis for Ivermectin use and need for ICU admission and mechanical ventilation
Figure 5: Meta-analysis for Ivermectin use and Adverse effects
e-figure 1: Sensitivity analysis Mortality- clinical trials (excluded Galan et al)
e-figure 2: Sensitivity analysis Mortality- RCTs (excluded Elgazzar et al)
e-figure 3: Sensitivity analysis Mortality- Observational (excluded Soto-Becerra et al)
e-figure 4: Subgroup Analysis- Inpatient overall
e-figure 5: Sensitivity Analysis- Inpatient overall (excluded Soto-Becerra et al)
e-figure 6: Subgroup Analysis- Inpatient by Study Design -RCTs
e-figure 7: Sensitivity Analysis- Inpatient RCTs (excluded Galan et al)
e-figure 8: Subgroup Analysis- Inpatient by Study Design -Observational
e-figure 9: Sensitivity Analysis- Inpatient Observational (excluded Soto-Becerra et al)
e-figure 10: Pooled Mortality overall
e-figure 11: Pooled Need for ICU admission
e-figure 12: Pooled Need for Mechanical Ventilation e-figure 13: Pooled adverse event overall
e-figure 14: Funnel Plot overall mortality
e-figure 15: Funnel Plot Mortality RCTs-Mild/Moderate COVID-19
e-figure 16: Funnel Plot Mortality RCTs-Severe COVID-19
e-figure 17: Funnel Plot Need for ICU Admission
e-figure 18: Funnel Plot Need for Mechanical Ventilation
e-figure 19: Funnel Plot Adverse event
e-table 1. Study characteristic table for all included studies
e-table 2. Cochrane Risk of bias assessment of the trials those were included in the study
e-table 3. Correlation of quality measures with estimates of treatment effects assessment of the trials those were included in the study
e-table 4. NIH quality assessment Tool for case series those were included in the study
e-table 5. NIH Quality Assessment of Case-Control Studies
e-table 6. NIH Quality Assessment of Observational Cohort and Cross-Sectional Studies
e-table 7. Certainty of the evidence (GRADE) Profile at Outcome Level
e-table 8. Ongoing clinical trials
Acknowledgment
We acknowledge Dr. Anant Mohan, Dr. Asma Asghar, Dr. José Morgenstern, Dr. Flavio Cadegiani, Dr. Morteza Niaee, Dr. Nasir Afsar, Dr. Nurullah Okumus, Dr. Pablo Méndez-Hernández and Dr. Ravi Kirti for their correspondence and contribution.
Footnotes
Conflicts of Interest: None of the authors have reported any conflicts of interest.
Financial Support: There is no financial disclosure related to this study.
List of abbreviations
- CDC
- Centers for Disease Control and Prevention
- COVID-19
- Coronavirus Disease 2019
- DNA
- Deoxyribonucleic Acid
- FDA
- Food and Drug Administration
- FLCCC
- Front line COVID-19 Critical Care
- ICU
- Intensive Care Unit
- IRB
- Institutional Review Board
- NIH
- National Institutes of Health
- RCT
- Randomized controlled trial
- RNA
- Ribonucleic Acid
- RT-PCR
- Reverse Transcription Polymerase Chain Reaction
- IMP
- Importin
- SARS-CoV-2
- Severe Acute Respiratory Syndrome Coronavirus 2
- WHO
- World Health Organization
References
- 1.↵
- 2.↵
- 3.↵
- 4.
- 5.
- 6.
- 7.
- 8.↵
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.↵
- 18.↵
- 19.
- 20.
- 21.
- 22.
- 23.↵
- 24.↵
- 25.↵
- 26.
- 27.
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.
- 34.
- 35.↵
- 36.↵
- 37.
- 38.
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.
- 55.
- 56.
- 57.
- 58.
- 59.
- 60.
- 61.
- 62.
- 63.
- 64.↵
- 65.
- 66.↵
- 67.
- 68.
- 69.
- 70.
- 71.
- 72.
- 73.
- 74.↵
- 75.↵
- 76.↵
- 77.
- 78.
- 79.
- 80.
- 81.
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.↵
- 106.↵
- 107.↵
- 108.↵




