
Abstract
Background The prevalence and prognosis of post-acute stage SARS-CoV-2 infection fatigue symptoms remain largely unknown.
Aims We performed a systematic review to evaluate the prevalence of fatigue in post-recovery from SARS-CoV-2 infection.
Method Medline, Embase, PsycINFO, CINAHL, Web of Science, Scopus, trial registries, Cochrane Central Register of Controlled Trials and Google Scholar were searched for studies on fatigue in samples that recovered from PCR diagnosed COVID-19. Meta-analyses were conducted separately for each recruitment setting.
Results We identified 39 studies with 8825 patients that recovered from COVID-19. Post-COVID-19 patients self-report of fatigue was higher compared to healthy controls (RR = 3.688, 95%CI [2.502, 5.436], p < 0.001). Over 50% of patients discharged from inpatient care reported symptoms of fatigue during the first (ER = 0.517, 95%CI [0.278, 0.749]) and second month following recovery (ER = 0.527, 95%CI [0.337, 0.709]). 10% of the community patients reported fatigue in the first month post-recovery. Patient setting moderated the association between COVID-19 recovery and fatigue symptoms (R2 = 0.12, p < 0.001). Female gender was associated with greater self-report of fatigue (OR =1.782, 95%CI [1.531, 2.870]). Patients recruited through social media had fatigue above 90% across multiple time points. Fatigue was highest in studies from Europe.
Conclusion Fatigue is a symptom associated with functional challenges which could have economic and social impacts. Developing long-term planning for fatigue management amongst patients beyond acute stages of SARS-CoV-2 infection is essential to optimizing patient care and public health outcomes.
The first cases of SARS-CoV-2 (later named COVID-19) were reported in November 2019[1]. By March 2020, the World Health Organization gave it a pandemic status [2]. Even during the early period of the spread, several studies reported acute mental health effects[3] ranging from stress[4] to depression[5] and anxiety[6]. A high level of post-traumatic stress and depressive symptoms were reported in a systematic review of these studies[7].
Several factors can influence mental health and wellbeing in pandemics. General factors may be related to fear of acquiring the infection[8 ,9], challenges posed by the pandemic restrictions[10 ,11], and the economic impacts of the pandemic itself[12 ,13]. The specific factors influencing mental health due to COVID-19 can be the direct biological mechanisms by which the virus affects individuals[14]. For example, an autoinflammatory response affecting multiple systems has been noted in early research of patients infected with SAR-Cov-2[15 ,16].
The virus can directly affect the brain[17 ,18] and produce symptoms such as encephalopathy[19], dysgeusia[20], anosmia[21], confusion[22 ,23], dizziness[24], headache[25], Ischemic Stroke[26 ,27], and behavioural changes[28]. At a symptom level, acute mental health effects of the virus include depression[29], anxiety[30], and fatigue[31]. However, viral infections are known to have effects beyond the acute infection[32 ,33]. They can impact mental health even when the virus is not active in the body[34]. Post recovery from the infection, patients may suffer symptoms such as fatigue[35] and low mood[36]. Chronic fatigue has been associated with previous infections with cytomegalovirus (CMV)[37], Epstein-Barr Virus (EBV)[38], Herpesvirus-6[39], Ross River virus[40], Dengue virus[41], MERS[42], and SARS[34]. The causes of post-viral symptoms during recovery stages are largely unknown. Longer-term changes in the immune system[41 ,43] or dysregulation of peripheral and autonomic nervous system functioning[44 ,45] have been implicated.
Several patterns of persistent symptoms are emerging post recovery from COVID-19. The symptoms may be present continually[46 ,47] or in a cyclical manner[48], at times triggered by stress[49 ,50] and physical effort[51 ,52]. Fatigue and low mood have been noted repeatedly even after the acute SARS-Cov-2 infection has subsided[53-55]. The terms ‘long Covid’, ‘long haul Covid’, and ‘Covid long hauler’ are frequently used in the media and scientific literature to capture the challenges of individuals suffering from such post-Covid syndromes[56-58]. These syndromes can fall into more than one pattern[54 ,59], and the underlying causal mechanisms may be many. For instance, in certain individuals, cardiac function changes have been described in patients with symptoms of fatigue after contracting and recovering from acute SAR-Cov-2 infection[60 ,61]. Patients admitted in the ICU may also have more extensive lung damage[62] with fatigue as a symptom[63].
In some countries, such as the UK, services to address the long-term effects of COVID-19 have been proposed[64 ,65] and are being established[66 ,67]. In this context, fatigue is an important symptom because it is associated with disability[68 ,69] and economic consequences[70 ,71]. Fatigue symptoms may also affect the morale of the sufferers and push them to develop other psychiatric conditions such as depression[72 ,73]. Various professional bodies have published initial guidelines for the management of such symptoms[74]. It has been argued that patients with even milder attacks of COVID-19 who do not receive inpatient care may suffer long-term symptoms[75].
The current literature is unclear about the incidence and prevalence of such symptoms in individuals with a past diagnosis of SARS-Cov-2 and how long they persist. As the number of patients recovering from COVID-19 continues to rise, addressing long-term consequences, such as fatigue, are critical for optimizing the health outcomes of survivors.
This systematic review aims to address essential questions specific to post-Covid fatigue to inform and guide the evaluation and management of COVID-19 recovery. First, the study will provide a quantitative evaluation of post-Covid fatigue prevalence across different time points from cross-sectional and longitudinal studies. Where possible, the review will also examine associations with factors such as the severity of illness, type of patient population (e.g., inpatient vs outpatient), effect of gender, comorbidities and different definitions of recovery.
Methods
This systematic review was conducted in accordance with the PRISMA [76] and MOOSE guidelines. The study protocol and MEDLINE search strategy were pre-registered in the Open Science Framework (i.e., osf.io/zu25b) on the 14th of September, 2020 and underwent full registration in the International Prospective Register of Systematic Reviews on the 18th of September, 2020 (i.e., [CRD42020209411]).
Search strategy
We searched Medline, Embase, PsycINFO, CINAHL, Web of Science, Scopus, trial registries (i.e., NIH clinical trials registry, Cochrane Central Register of Controlled Trials and ISRCTN registry) and google scholar. Pre-print servers (MedRxiv and Psycharxiv) were also included in our search. The database search was undertaken on the 16th of September, 2020, the 1st of October, 2020 the 8th of November, 2020, and the 14th of February, 2021. The study selection process was applied to these new searches.
A combined set of MeSH and keywords associated with COVID-19 and fatigue were used to identify publications on fatigue in individuals recovered from acute COVID-19 infection, diagnosed with appropriate testing. No restrictions relating to study design, location, or language were imposed. The search strategy was synthesized by one of the authors (TB) and reviewed by a medical librarian. The strategy for each database is provided in Supplementary Material S-2. Only publications from 2019 onwards were considered. References from opinion publications relating to post-COVID fatigue were hand searched and screened. Study authors were contacted when PCR reports were ambiguous or for further data on the course of fatigue. Rayyan (QCRI) software was used for screening and managing the abstracts. Title, abstract, and full-text screening were conducted by two independent reviewers (TB and SG), and a senior author (SR) resolved any screening discordance. Study selection criteria were applied to the retrieved full text articles independently by two reviewers (TB and SG). Any disagreements were resolved through a discussion between the reviewers and a senior author (SR).
Selection Criteria
The eligibility criteria were: a) COVID-19 was diagnosed by Rapid Testing polymerase chain reaction test (RT-PCR) or Viral Antigen Test; b) Recovery was defined by a negative finding in one of these tests and/or clinical judgement; c) Fatigue was assessed on follow-up either through self-report, clinical interview or a fatigue specific scale.
The exclusion criteria were: a) COVID-19 status was screened through antibody testing (i.e., IgG and IgM) only; b) absence of a post-infection follow-up; c) presence of medical or neurological complications (which could explain fatigue symptoms); d) the sample was comprised of participants below the age of 18; e) publication was in a language other than English, French or Spanish; or f) utilizing non-human methodology (i.e., lab simulation, in vitro or animal models).
As post-viral effects related to COVID-19 is an evolving challenge, several study designs were considered for evaluation: cluster or non-cluster randomized controlled trials, controlled trials, and uncontrolled trials, cross-sectional, case-control and cohort studies.
Data Extraction
Data extraction was initiated on the 20th of December, 2020, and completed on the 20th of February, 2021. Data extraction was conducted by reviewers (TB and SG) in consultation with a senior author (SR). Study authors were contacted if required data were missing from a publication. Descriptive data extracted in this systematic review included the author, year of publication, study location, COVID-19 diagnostics, participants’ mean age, study setting (i.e., clinical setting, general population), fatigue symptom report, study sample size, attrition, length of time between recovery and follow-up assessments of fatigue. For each report of post-viral fatigue, continuous data (i.e., mean and standard deviation) and categorical data (i.e., frequency data) relating to post-viral fatigue were extracted for meta-analysis.
Assessment of Bias and Quality
Study quality assessments were completed by two reviewers (TB and SG). A third reviewer (SR) resolved any discrepancies. Risk of bias was assessed using several instruments, matching the appropriate scale to the study design. For non-randomized studies, the National Institute of Health Study Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies was selected. For randomized studies, Cochrane’s ROB 2 was identified. The Joanna Briggs level of evidence scale for prognosis[77] was used for the overall strength of evidence.
Data analysis
Comprehensive Meta-Analysis software (version 3) was used to conduct a meta-analysis of the data from the selected studies. Analyses were initiated on the 21st of February, 2021. A random-effects model was used for all statistical analyses. The primary outcome was the presence of fatigue. We calculated pooled prevalence and two-tailed 95% confidence intervals in studies reporting post-viral fatigue on follow-up. Prevalence analyses were pooled by recruitment setting: inpatient, outpatient, mixed, registries, and social media or COVID-19 app-based settings. For each recruitment setting, meta-analyses were performed for studies that applied uniform measurements of fatigue (i.e., self-report and validated measurement tools) and in which follow-up was conducted within the same month post-recovery. We used Risk Ratio (RR) as an effect size metric in studies that compared patients who recovered from COVID-19 with a control group. Odds Ratios (OR) were also used where COVID-19 recovered patients were divided into groups based on the severity of the acute infection or type of hospital care received. ORs were calculated to compare patients with PCR test negative and those retested positive after recovery. ORs were also used for examining gender differences and estimating the effect of biomarkers. Meta-regressions were conducted on studies rated as fair or good quality. We first examined the moderating effect of self-reported fatigue compared to the use of fatigue rating scales. The majority of the studies assessed fatigue through self-reports. Data from these were used to examine the effect of time since recovery, PCR negative test confirmed recovery, recruitment setting, average sample age, proportion of females, Diabetes Mellitus, COPD and hypertension.
Heterogeneity was tested using the Q statistic and reported in the form of a percentage of variation across studies (I2). A visual inspection of publication bias was conducted using a funnel plot and Egger’s linear regression modelling to statistically determine the presence of symmetry.
Results
Study Selection
The initial search of the literature identified 4384 abstracts. 496 abstracts were selected. Full-text articles of these abstracts were obtained, and study criteria were applied. Thirty-one published studies[53-55 ,78-105] and eight medRxiv preprints[46 ,75 ,106-111], met the inclusion criteria for this systematic review (Figure 1). The sample sizes ranged from 18[102] to 1655[79], with mean age across studies ranging from 32.3 (SD = 8.5)[54] to 67.1 (SD =11.6)[87]. The studies represented 18 countries with a total sample of 8825 individuals recovered from COVID-19 (Table 1). Diagnosis of COVID-19 was confirmed through Polymerase Chain Reaction (PCR) testing. PCR negative status was used to confirm recovery in 16 studies (5190 cases). 25 studies (3635 cases) defined recovery hospital discharge or a specified number of days since the last positive PCR results. 25 studies were from inpatient settings and five were from outpatient settings, while four studies recruited through a mix of different clinical settings. Two studies recruited through patient registries, and one utilized a combination of two epidemiological datasets. Two studies reported recruitment through other methods such as social media (k = 1) or a COVID-19 symptom app (k = 1). 30 studies measured fatigue through symptom self-report and 9 studies utilized validated fatigue scales to evaluate fatigue rates within their samples.

Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram.
Characteristics of included studies
Four studies compared patients discharged from ICUs and hospital wards[84 ,89 ,92 ,105]. Five studies compared recovery from severe and non-severe experiences of SARS-CoV-2 infection[55 ,79 ,81 ,94 ,101]. Three studies compared COVID-19 recovered patients and healthy controls[46 ,81 ,102]. Eight studies compared residual fatigue in female and male survivors[75 ,79 ,81 ,82 ,88 ,89 ,92 ,105], and two compared patients who retested positive for SARS-Cov-2 on PCR test with those who retrained PCR negative status[83 ,106]. Finally, two studies evaluated the association between biomarkers and post-COVID fatigue[80 ,92].
Data were extracted from thirty-nine studies and organized primarily according to the study setting and time intervals over which fatigue was assessed. Thirty (i.e., 30/39) studies used self-report of fatigue and ten used fatigue rating scales.
The study setting groups were: primarily inpatients, primarily outpatients, mixed inpatients/outpatients, population studies, recruitment through apps and social media. The time intervals or temporal groups were: 0-30 days (1 month), 31-60 days (1-2 months), 61-90 days (2-3 months), 91-120 days (3-4 months), 121-150 days (4-5 months), and 151-180 days (5-6 months).
Studies differed in the way recovery from COVID-19 was defined. Therefore, for each study, we chose one of the following approaches: PCR negative test, number of days after discharge from the hospital, and number of days since onset of the symptoms or PCR positive test. Fifteen studies defined their follow-up time as the number of days since symptom onset or PCR positive test results. In these studies, to account for the acute phase of COVID-19, day-0 of recovery was defined as fourteen days after follow-up initiation as this represents the recommended length of self-quarantine for patients with COVID-19[112 ,113]
Eight had repeated measure designs[46 ,55 ,75 ,86 ,95 ,96 ,98 ,104]. Where there were multiple assessments of fatigue within a temporal group, we calculated the mean of the fatigue scores or mean of the proportion of patients reporting fatigue.
Quality assessment and Publication bias
Risk of bias assessment was conducted using the NIH Quality Assessment Tool for observational studies. Most studies were of fair quality (see S-6). The interrater reliability of the assessments was high (k = 0.8921, %agreement = 94.65%), and discrepancies were resolved through consensus. However, most studies were exploratory in nature rather than hypothesis-driven. Publication bias was assessed through funnel plots and Egger’s regression. A low level of Publication bias was observed when all studies were considered (see S-5; Egger’s bias = -2.742, 95%CI [-6.019, 0.534), t = 1.69, p = 0.099). No significant publication bias was found in studies with self-reported fatigue (Egger’s bias = -2.458, 95%CI [-6.649, 1.734), t = 1.196, p = 0.241). However, studies using fatigue scales showed significant publication bias (Egger’s bias = -3.797, 95%CI [-7.534, -0.059), t = 2.34, p = 0.047).
1. Fatigue in COVID-19 recovered patients from inpatient settings
In the twenty-five studies with inpatient settings, the duration of follow-up was from 1-6 months. The majority of these studies assessed fatigue through self-reports (k = 20). 10 studies used PCR negative test as a proxy for recovery.
In Group 1 (<1 month), 3 out 5 studies used self-report of fatigue. There was a trend towards lower pooled prevalence of fatigue with the use of validated scales at 32% (k = 2, ER = 0.320, 95%CI [0.126, 0.607], I2 = 88.14%) compared to self-reports at 51.7% (k = 3, ER = 0.517, 95%CI [0.278, 0.749], I2 = 92.81%). However, the heterogeneity associated with these studies was found to be high. No meaningful comparison could be made between methods of defining recovery as 4 out of 5 studies used PCR negative test to confirm recovery.
With 12 studies, Group 2 (1-2 months) had the largest sample size and all studies used self-reports of fatigue. The pooled prevalence of fatigue was 52.7% (k = 7, ER = 0.527, 95%CI [0.337, 0.709], I2 = 96.07%; see figure 2a) in studies that did not use PCR negative test to confirm recovery compared to 49.3% (k = 7, ER = 0.493, 95%CI [0.204, 0.787], I2 = 98.36%; see figure 2b) in studies that used PCR negative test. This difference was nonsignificant (Q = 0.037, df = 1, p > 0.05) and there was considerable heterogeneity between studies.

Prevalence of self-reported fatigue within the second month following inpatient recovery defined by clinical assessment rather than PCR negative testing.
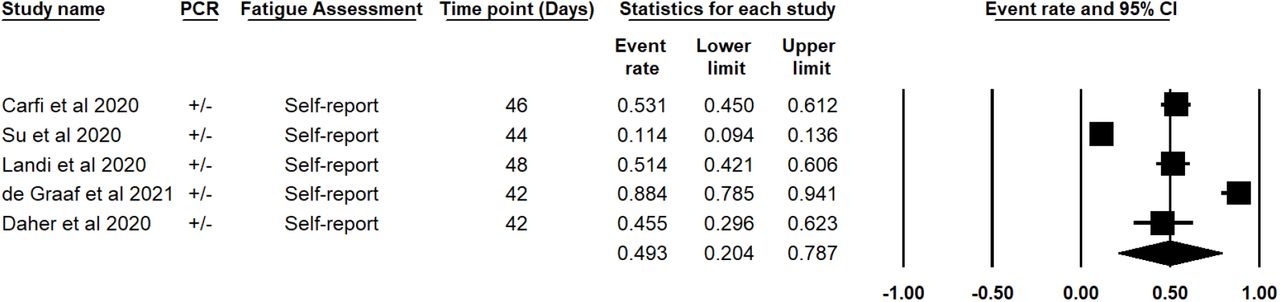
Prevalence of self-reported fatigue within the first month following inpatient recovery defined by PCR negative testing.
In Group 3 (2-3 months), 11 studies assessed fatigue. 7 of these studies used self-reports of fatigue and 4 used fatigue scales. Self-reported fatigue was higher in studies that did not use PCR negative test to define recovery (k=5, ER = 0.590, 95%CI [0.189, 0.684], I2 = 58.83%; see figure 2c) compared to those that did not (k=2, ER = 0.352, 95%CI [0.071, 0.795], I2 = 95.34%; see figure 2d) but this did not reach significance (p > 0.05). Pooled prevalence of fatigue measured with scales was 47.8% (k = 4, ER = 0.478, 95%CI [0.399, 0.558], I2 = 56.29%; see figure 2e) with moderate heterogeneity between studies. No meaningful comparison could be made between methods of defining recovery within these studies as only 1 study used PCR negative test to confirm recovery. The pooled prevalence of fatigue measured through scales was lower than the analysis of self-reported fatigue, this difference was nonsignificant (Q = 0.424, df = 1, p > 0.05).
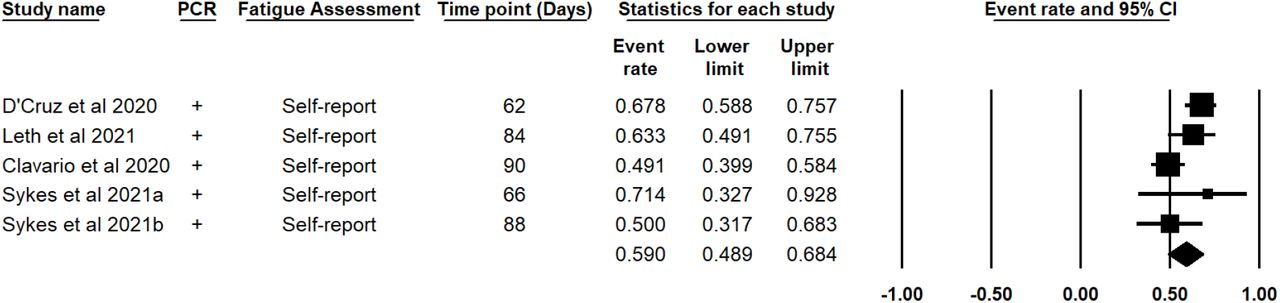
Prevalence of self-reported fatigue within the third month following inpatient recovery defined by clinical assessment rather than PCR negative testing.

Prevalence of self-reported fatigue within the third month following inpatient recovery defined by PCR negative testing.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Prevalence of fatigue within the third following inpatient recovery, in which fatigue was measured using validated fatigue scales.
In the 3-4 month period (Group 4), there were 3 studies that elicited self-report of fatigue. Only 1 study used the PCR negative test result to identify recovery and had a fatigue prevalence of 28.3% (n = 538, 95%CI [ 0.246, 322]). The two smaller studies that did not use PCR negative test status for recovery, had a wide difference in fatigue prevalence with a 19.3% pooled prevalence of fatigue (k = 2, ER = 0.193, 95%CI [0.049, 0.523], I2 = 90.04%).
Group 5 (4-5 months) had only one study[105] which assessed self-reported fatigue. The prevalence of fatigue within their sample was found to be 39.1% (k = 1, ER = 0.391, 95%CI [0.218, 0.598]). Notably, this study did not use PCR to define recovery.
Two studies followed up recovered patients beyond 6 months (Group 6). Huang and colleagues measured fatigue through self-report and defined recovery through PCR negative test. Within their sample, 1038 (62.7%) reported fatigue out of a total of 1655 participants (95%CI [0.604, 0.650]). In contrast, Latronico et al. also evaluated fatigue 180 days following discharge and assessed fatigue using the Fatigue Severity Scale rather than dichotomous self-reports. This single point estimate found a 35.6% (95%CI [0.231, 0.504]) prevalence of residual fatigue in COVID-19 recovered cases; this assessment did not use the PCR test to confirm recovery from COVID-19. However, the study conducted by Latronico et al. had a lower precision of estimate, likely due to a small sample size of 55 participants.
2. Fatigue in COVID-19 recovered patients from outpatient settings
Five studies measured fatigue outcomes in COVID-19 in the first, second, and third month following recovery.
In Group 1 (<1 month) the larger study by Cellai et al. did not use PCR negative test for recovery, and reported fatigue in only 3.4% (n = 496, 95%CI [0.021, 0.054]) of patients. However, this may have been a result of the study design. Only a small number of the total sample were assessed for symptoms after 3 weeks. The Knight et al. study established recovery through PCR test negative findings. 34.7% (n = 101, 95%CI [0.260, 0.444]) and 28.4% (n = 95, 95%CI [0.203, 0.383]) reported fatigue during follow-ups conducted 36 days and 81 days following recovery status.
The only study of fatigue between 1-2 months (Group 2) was Townsend et al. This study evaluated the presence of post-COVID fatigue. The prevalence of fatigue within their sample was 52.3% (n = 128, 95%CI [0.437, 0.608]). Fatigue was measured using the Chalder Fatigue Scale, but recovery was not defined using PCR testing.
Two studies assessed fatigue using a validated scale within 2-3 months (Group 3). Woo et al. had a smaller sample size of 18 and a very wide time interval over which patients were assessed for symptoms. The prevalence of fatigue was 16.7% over 20-105 days. In contrast, Townsend et al. (2021) reported fatigue in 47.7% of their cohort (n = 153, 95%CI [0.399, 0.556]). Neither study used PCR negative testing to confirm recovery, and the data from these studies were not pooled due to significant differences in the duration of follow-up.
3. Fatigue in COVID-19 recovered patients from mixed settings
Four studies evaluated fatigue in patients that recovered from COVID-19 in mixed settings. Two studies examined self-reported fatigue during the first month (Group 1) following recovery and consisted of patients that recovered from in-and outpatient care, and non-hospitalized cases. Data from these studies were not pooled due to significant differences in their follow-up design. First, 72.8% (n = 287, 95%CI [0.674, 0.777]) of the cohort in a study conducted by Kamal et al. reported experiencing fatigue. This study used PCR to define recovery from COVID-19. Another study conducted within this timeframe by Tenforde et al. found a prevalence of 71% when considering only respondents to telephone follow-up; however, this prevalence dropped to 35.4% when considering the full sample in which non-respondents are included.
One study was found to report fatigue during the second month of recovery within a mixed sample (i.e., hospital and non-hospital care). Within their sample, the prevalence of fatigue was found to be 29.5% (n = 61, 95%CI [0.194, 0.421]).
Peterson et al. used the Fatigue Impact Scale during an average follow-up of 111 days; however, this was accomplished using a wide range of 45-215 days. The fatigue reported within their cohort was lower than other studies as the prevalence was found to be 8.3% (n = 180, 95%CI [0.051, 0.134]); this difference is most likely affected by the study methodology.
4. Fatigue in COVID-19 recovered subjects recruited from general registry and secondary data
Three studies were found to analyze self-report data from non-hospitalized patient registries (k = 2) and non-selective databases (k = 1). None defined recovery by PCR, and all measured fatigue using symptom self-report. Pooling two data points within the first month (Group 1) of recovery resulted in a prevalence of 9.7% (k = 2, ER = 0.097, 95%CI [0.031, 0.262], I2 = 91.10%; see S-4).
One study by Cirulli and colleagues assessed fatigue during the second month of recovery. Within their sample, 6.6% (n = 152, 95%CI [0.036, 0.118]) reported the presence of fatigue symptoms 46 days following recovery.
All three studies evaluated fatigue symptoms during the third month of recovery, in which pooling point estimates resulted in an 8.2% (k = 3, ER = 0.082, 95%CI [0.034, 0.188], I2 = 80.75%; see S-4) prevalence of fatigue. Figures from all different time points in this study are substantially lower than post-COVID fatigue in the hospital population.
5. Fatigue in COVID-19 recovered subjects recruited using social media or tech-based apps
Two heterogeneous studies recruited individuals that recovered from COVID-19 using social media (k = 1) and a COVID-19 related app (k = 1) during the first and second months following recovery.
A repeated measures study conducted by Sudre et al. used a mobile symptom tracking COVID-19 app. Within their sample, fatigue was reported by 97.7% of 558 recovered cases (ER = 0.977, 95%CI [0.960, 0.986]) during follow-up participation 28 days post-positive PCR test results. Furthermore, when assessing fatigue in 189 individuals that recovered from COVID-19 56 days following PCR diagnosis of COVID-19, the prevalence was found to be 96.8% (k = 1, ER = 0.968, 95%CI [0.931, 0.986]). The study aimed to identify symptoms associated with long-COVID; fatigue was found to be the most prevalent symptom within individuals reporting persistent symptoms following COVID-19 recovery. Fatigue during the first week of diagnosis was found to be the strongest predictor of fatigue reports during a follow-up 28 days post-diagnosis fatigue (k = 1, OR=2.83 95%CI [2.09;3.83]). This study remains ongoing and is now assessing over 4182 incident cases of COVID-19.
Klein et al. recruited their sample using social media 5 to 6 months (Group 5) post recovery and employed a snowball recruitment method. The prevalence of self-reported fatigue was found to be 21.90% (K = 1, ER = 0.977, 95%CI [0.960, 0.986]) 180 days post-PCR diagnosis.
6. Comparing fatigue in COVID-19 recovered patients with healthy controls
Three studies compared individuals recovered from COVID-19 with healthy controls. The studies collected participants from inpatients[81], outpatients[102] and an epidemiological database[46]. Pooled analysis of fatigue data was conducted for the period between 76-97 days, and fatigue assessment for all studies was in the form of self-report. COVID-19 patients were found to have a 3.688 increase in relative risk of fatigue outcomes compared to non-COVID-19 exposed groups (k = 3, RR = 3.688, 95%CI [2.502, 5.436], z = 6.592, p < 0.001; I2 = 0%; see S-4). The heterogeneity within these studies was low.
One study[46] assessed fatigue over 3-time points in which the COVID-19 recovered group had an increased relative risk of fatigue across time points when compared to healthy controls. These follow-ups were conducted 16 days (n = 4021, RR = 4.451, 95%CI [2.341, 8.464], p < 0.001), 46 days (n = 3221, RR = 4.696, 95%CI [2.406, 9.163], p < 0.001) and 76 days (n = 2821, RR = 5.530, 95%CI [2.746, 11.136], p < 0.001) following recovery. However, this is likely explained by higher attrition in the post-COVID-19 group compared to the control group. Notably, there were not enough data points to conduct a meta-analysis.
7. Fatigue in Covid-19 PCR negative vs PCR positive patients
Two studies had data from discharged inpatients comparing those who retested PCR positive to those who were persistently PCR negative. No significant difference was found between patients identified as recovered from COVID-19 and patients retested positive for COVID-19 (k = 2, RR = 0.806, 95%CI [0.476, 1.363], p = 0.420, I2 = 53.02%; see S-4).
8. Gender and fatigue reports amongst COVID-19 recovered patients
Eight studies had data comparing males with females in COVID-19 recovered patients from both inpatient[79 ,81 ,82 ,88 ,89 ,105] and outpatient[92] settings and epidemiological datasets[75]. Females were more likely to self-report fatigue between 84-180 days of follow-up (Group 3-6) in pooled data from 4 studies (k = 4, OR =1.782, 95%CI [1.531, 2.870], z = 3.366, p = 0.001, I2 = 52.51%; see S-4). Sensitivity analysis in which only studies from Groups 2 to 3 were included further replicated the observed gender effects (k = 3, OR = 2.096, 95%CI [1.531, 2.870], z = 4.620, p < 0.001, I2 = 0%), and heterogeneity for this analysis was low. However, this difference disappeared when fatigue was assessed using rating scales (see S-4) in two studies across two time points of 12-48 days (k = 2, OR = 1.254, 95%CI [0.0.273, 5.756], p = 0.771, I2 = 89.92%), and 72 to 81 days post-COVID-19 recovery (k = 2, OR = 1.503, 95%CI [0.456, 4.951], p = 0.503, I2 = 90.63%).
9. Fatigue in Severe vs. Non-Severe SARS-CoV-2 patients
Two studies similar in design and duration of follow-ups, compared recovered individuals with severe COVID-19 and non-severe COVID-19 related illnesses. When examining outcomes 54 to 97 days following recovery, individuals recovering from severe cases of COVID-19 did not significantly differ from one another with respect to fatigue (OR = 1.344, 95%CI [0.958, 1.886], z = 1.711, p = 0.087, I2 = 0%; see S-4) and other chronic symptoms[81 ,94]. Data from 2 other studies, which could not be pooled due to differences in study design, had similar findings; in which no difference was observed during the first month following PCR negative findings (OR = 1.181, 95%CI [0.262, 5.326], p = 0.829), and 75 days following discharge in which fatigue was assessed using the Chalder Fatigue Scale (OR = 0.711, 95%CI [0.397, 1.274], p = 0.252). Similarly, no significant difference was detected when evaluating evidence comparing patients discharged from the ICU and hospital during a follow-up within the second and third month of recovery (k = 2, OR = 0.991, 95%CI [0.332, 2.960], z = -0.017, p = 0.987, I2 = 60.23%; see S-4) in which fatigue was assessed using validated scales, and second and fourth month in which fatigue was self-reported (k = 2, OR = 1.001, 95%CI [0.363, 2.762], z = 0.002, p > 0.999, I2 = 27.18%; see S-4).
In contrast, Huang et al. found within a sample of 1733 COVID-19 recovered cases that had previously received care in the form of a high-flow nasal cannula for oxygen therapy, non-invasive ventilation or invasive mechanical ventilation were 2.73 times (OR = 2.725, 95%CI [1.694, 4.381]) more likely to experience post-COVID fatigue when compared to patients that had previously received no supplementary oxygen. Perhaps the divergent findings may be linked to the different ways in which severity is defined. A more objective measure of severity was utilized in the study, which showed a difference between the severe and non-severe groups.
10. Biomarkers and Post-COVID fatigue
Two studies examined immunological markers and their association with fatigue in patients that recovered from COVID-19. These studies were not pooled due to design differences in fatigue assessments. With regard to the two-point estimates, Liang et al. found no significant effect on fatigue outcomes when examining the role of CD3 (p > 0.05), CD4 (p > 0.05), CD8 (p > 0.05) lymphocytes. Furthermore, both pro-inflammatory IL-6 (p > 0.05), and CRP (p > 0.05) were nonsignificant predictors of fatigue 90 days following PCR negative testing. This finding was mirrored by Townsend et al. in which lymphocytes (p > 0.05), IL-6 (p > 0.05) and CRP (p > 0.05) were nonsignificant predictors of fatigue 72 days post-hospital discharge. However, patients recovered from COVID-19 within the Liang et al.’s sample were found to be 94.76 times more likely to experience fatigue for each unit increase in serum troponin-I (95%CI [24.935, 360.149], p < 0.001), suggesting cardiovascular implications. However, the current review did not have the necessary data points to evaluate this meta-analytically.
11. Country of origin and fatigue
Extracted studies provided sufficient data points for comparison of self-reported fatigue in Asia, North-America, and Europe within the first six months of recovery from COVID-19. Self-reported fatigue was dependent on the continent of origin when comparing data points from Europe, North-America, and Asia (Q = 0.424, df = 2, p = 0.016). Europe had the highest levels of self-reported fatigue post-recovery from COVID-19 (K = 14, ER = 0.546, 95%CI [0.389, 0.695], I2 = 91.37%), followed by North-America (K = 7, ER =0.300, 95%CI [0.149, 0.510], I2 = 97.58%) and Asia (K = 9, ER = 0.225,95%CI [0.116, 0.392], I2 = 98.83%). Heterogeneity was high within the continental data points. However, multivariate meta-regression determined that the significant variance explained by continental differences was robust as it remained significant (k = 30, Q = 11.44, df = 2, p = 0.0033) when holding recruitment setting constant.
12. Moderator analysis
Meta-regression was employed to examine the explained variance between point estimates and only included studies assessed to be of fair or good quality. Studies with repeated measures were excluded from the moderation analysis. When considering the first six months following COVID-19 recovery, the comparison between self-reported fatigue and fatigue assessed using validated scales did not significantly differ regarding COVID-19 prevalence (k = 27, Q = 0.07, df = 1, p = 0.7931).
All further moderation analyses were carried out using self-reported fatigue. The association between COVID-19 recovery and fatigue was not found to be dependent on the use of PCR negative testing to define recovery (k = 20, Q = 0.76, df = 1, p = 0.3819), average sample age (k = 18, z = 0.379, p = 0.379), sample gender proportions (k = 20, z = -1.78, p = 0.076), proportions of Diabetes Mellitus (k = 20, z = 1.51, p = 0.131) or the sample prevalence of COPD (k = 12, z = 0.85, p = 0.394). However, the association between COVID-19 recovery and fatigue was found to be dependent on recruitment setting (k = 20, R2 = 0.12, Q = 17, df = 3, p = 0.0007), and hypertension (k = 20, R2 = 0.01, β = 2.81, z = 2.01, p = 0.044). Overall, when considering 6 months following COVID-19 recovery, the length since recovery was not a significant mechanism of change for the association between COVID-19 exposure and post-recovery fatigue outcomes (K = 20, z = 0.28, p = 0.778), even when holding patient setting constant (k = 20, z = -0.23, p = 0.814).
Discussion
This systematic review shows that self-reported fatigue after recovery from COVID-19 infection can last up to 6 months based on the longest duration studies. Patients in the post-acute stage of COVID-19 were 3.7 times more at risk for onset of fatigue compared to healthy controls. Between 30% to 60% of inpatient and outpatient treated patients reported fatigue. However, at the population level, the proportion of COVID-19 recovered patients suffering fatigue may be lower (i.e., < 10%). The highest proportion of fatigue (i.e., up to 90%) was amongst those persons who were recruited through social media and COVID-19 apps. This could be the effect of self-selection as those with persistent symptoms are more likely to use these channels to report on their health. PCR negative to confirm recovery did not influence fatigue. Even when the PCR test is negative, non-viral shedding may continue to occur[114], which may explain this finding.
There were insufficient number of studies comparing self-report to the assessment of fatigue through rating scales. However, in females, fatigue was higher compared to males but only on self-report and not on assessments using rating scales. The severity of COVID-19 did not appear to moderate the expression of fatigue. This maybe a result of how disease severity is defined (e.g., based on admission to general wards or to ICU), which could be dependent on multiple factors, including local admission protocols. A more precise definition of severity used in at least one study did show an increase in self-reported fatigue in those deemed more unwell.
Surprisingly, age did not have an effect on self-report or rating scale scores of fatigue. Since mortality is higher in older adults, the survivors may have fewer symptoms overall. Similarly, our analysis could not assess the influence of chronic disease comorbidity. The data on comorbidities reported in publications does not allow accurate quantification of the chronic disease burden. This would require access to individual patient data.
There is an effect of continent of origin (see S-7), but it is possible that this may be due to reliance on self-report rather than the use of more objective fatigue measurement instruments. Reinfection measured through PCR positive seroconversion did not appear to influence the proportion of people reporting fatigue. There are initial findings of links with biomarkers; however, this will require additional studies to confirm persistent associations.
Limitations and Strengths
To the best of our knowledge, this is the first systematic review examining fatigue post-recovery from COVID-19 across a wide range of individuals and settings spanning several countries. However, the findings were affected by significant heterogeneity in study design, duration, population, method of assessment of fatigue, and more. In addition, our search was restricted to articles in English, French, and Spanish. Based on JBI methodology, the evidence for prognosis was level 3.a, and there was a wide range of study designs restricting definitive conclusions on quantifying fatigue post-recovery from COVID-19. The study highlights that clinical populations are at risk for persistent fatigue. This could inform how advice is given to those who have been treated for SARS-Cov-2 infection in the hospital or outpatient settings. We did not have information to analyse the effect of different waves of the infection.
Future research and application to clinical practice
Health policy and healthcare leadership must prepare for a longer-term management plan for COVID-19 as there are significant needs beyond recovery from the acute infection. Fatigue, along with other symptoms, may also affect the ability to function and work. This may have a significant economic impact as well as an impact on the lives of significant others in the patients’ lives. Fatigue and its economic impact has been studied[71]. Future research should focus on more objective assessments of fatigue and standardized follow-up of post-COVID-19 patients. In the interest of public health, it should be possible to share anonymized individual data of persistent post-COVID-19 symptoms. New variants of coronavirus may have a different profile of fatigue and this warrants further research. Finally, more research is needed into the pathogenesis of what may be a range of long-term syndromes.
Data Availability
Please contact Dr. Sanjay Rao (sra4{at}uottawa.ca) for availability of data
Conflict of Interest
The authors declare that they have no conflict of interest.
Funding Statement
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Author contributions
S.R., T.T., S.K., S.J., and T.B. contributed to the design and conception of the study. S.R., S.G., and T.B. were involved in screening the texts for inclusion in the review. S.G. and T.B. extracted the data. T.B. and S.R. led the analysis and interpretation of data. S.R. and T.B. led the manuscript’s write-up, and T.T. contributed to the manuscript write-up. S.R. and T.B. contributed to the analysis and interpretation of the synthesis. All other authors provided a critical review of the manuscript and assisted with revising the manuscript. T.B., coordinated and S.R., supervised the systematic review. All authors approved the final manuscript for submission.
Footnotes
Corresponding Author Contact information Updated
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.
- 91.
- 92.↵
- 93.
- 94.↵
- 95.↵
- 96.↵
- 97.
- 98.↵
- 99.
- 100.
- 101.↵
- 102.↵
- 103.
- 104.↵
- 105.↵
- 106.↵
- 107.
- 108.
- 109.
- 110.
- 111.↵
- 112.↵
- 113.↵
- 114.↵



