
Abstract
Importance Aside from supportive management, there remains no specific treatment for Coronavirus Disease 2019 (COVID-19).
Objective Determine whether ozonated autohemotherapy is associated with a shorter time to clinical improvement in patients with severe COVID-19 pneumonia.
Design Single-center proof-of-concept prospective cohort study.
Setting Internal Medicine ward at Policlinica Ibiza Hospital, Spain.
Participants Eighteen consecutive patients with laboratory confirmed COVID-19 infection and severe pneumonia who were admitted to hospital between 20th March and 19th April 2020.
Exposures Patients in the ozonated autohemotherapy arm received hemotherapy twice daily starting on the day of admission for a median of 4 days. Each treatment involved administration of 200 mL autologous whole blood enriched with 200 mL of oxygen-ozone mixture with a 40 μg/mL ozone concentration. Patients in the control arm received supportive care. Assignment to hemotherapy versus usual care was determined based on the admitting physician on the day of admission, with only one of the three possible physicians prescribing ozonated autohemotherapy
Main Outcomes The primary outcome was time from hospital admission to clinical improvement, which was defined as either hospital discharge or a two-point improvement in clinical status measured on a six-point ordinal scale. Secondary outcomes were clinical improvement measured on the 7th, 14th and 28th day after admission, as well as time to a 2-fold reduction in concentrations of C-protein reactive, ferritin, D-dimer and lactate dehydrogenase.
Results The mean age of the cohort was 68 y and 72% (n=13) were male. Nine patients (50%) received ozonated autohemotherapy beginning on the day of admission. In unadjusted comparisons, ozonated autohemotherapy was associated with significantly shorter time to clinical improvement (median [IQR]), 7 days [6-10] vs 28 days [8-31], p=0.04) and significantly higher proportion of patients achieving 14-day clinical improvement (88.8% vs 33.3%, p=0.01). In risk-adjusted analyses, ozonated autohemotherapy was associated with a shorter mean time to clinical improvement (−11.3 days, p=0.04, 95% CI −22.25 to −0.42).
Conclusions and Relevance Ozonated autohemotherapy was associated with a significantly shorter time to clinical improvement in this prospective cohort study. Given the small sample size and singlecenter study design, these observations require evaluation in larger randomized controlled trials.
Introduction
The ongoing pandemic of Coronavirus Disease 2019 (COVID-19) infections has led to more than 5.2 million cases and 341.000 deaths globally as of May 24th, 2020 (Johns Hopkins University and Medicine; COVID-19 map Johns Hopkins Coronavirus Resource Centre; https://coronavirus.jhu.edu/map.html; accessed May 24th, 2020). About 15% of infected adults develop severe pneumonia requiring supplemental oxygen, and an additional 5% progress to acute respiratory distress syndrome requiring mechanical ventilation (often for several weeks). 1,2
At present, there remains no proven and efficacious treatment for this new disease. Consequently, there is a growing tendency to use novel methods. Ozone therapy is the administration of a mixture of ozone (molecule consisting of three oxygen atoms) and oxygen. Ozone therapy can be administered systemically by adding it to a sample of a patient’s own blood sample and then reinfusing it, in what is termed ‘ozonated autohemotherapy’. While ozone therapy is currently not available in the United States, several other countries – including Spain, Italy, Greece, Cuba, Russia, Portugal and Turkey – have incorporated ozone therapy in medical practice.
The pathogenesis of the virus is not fully understood, but it is well-known that the pathological picture varies, mainly involving the lungs where diffuse alveolar damage predominates with involvement of the microcirculation leading to marked hypoxia. 3 A dysregulation of the immune response is present in these patients and lymphocytopenia is a hallmark in the vast majority of these patients.4 Innate immunity and coagulation pathways are intricately linked. 5 COVID-19–associated macrophage activation, hyperferritinemia, cytokine storm, release of pathogen-associated molecular patterns and damage-associated molecular proteins can result in release of tissue factor and activation of coagulation factors that create a predisposition to hypercoagulability. 5
The potential benefits of ozonated autohemotherapy include reduced tissue hypoxia, decreased hypercoagulability, renal protection, modulated immune function, improved phagocytic function, and impaired viral replication. 6
There remain no published data on the efficacy and safety of ozonated autohemotherapy in patients with severe COVID-19 pneumonia, although an online report of the Scientific Society of Oxygen-Ozone Therapy (SIOOT) describes a case series of 73 patients, of whom 32.8% were intubated and 67.1% were non-intubated. 7 Of all the intubated-patients, 62.5% were extubated after 5 sessions with ozone autohemotherapy. Of all the non-intubated patients, only 6% required intubation. Whereas, the group of patients with only usual care without ozone auothemotherapy, had only a 20% rate of recovery among the intubated patients. We therefore conducted a proof-of-concept prospective cohort study to determine if ozonated autohemotherapy was associated with a shorter time to clinical improvement in patients with severe COVID-19 pneumonia.
Methods
Study Design
This prospective cohort study was performed at the Policlinica Ibiza Hospital in Spain. It was conducted in compliance with the Declaration of Helsinki and approved by a multidisciplinary human research ethics committee at the institution. Each participant gave written informed consent for administration of any interventions, collection of relevant clinical data and ascertainment of outcomes. The study cohort consisted of all consecutive adults (18 y or older) who were admitted to the hospital with a diagnosis of severe COVID-19 pneumonia between 20th March to 19th April 2020. All included patients met the following criteria: confirmed COVID-19 infection (diagnosed by nasopharyngeal swab performed on admission); severe pneumonia with baseline chest X-ray abnormalities; PaO2/FiO2 ratio < 300 or oxygen saturation <94% on room air, and tachypnea with respiratory rate exceeding 30 per minute.
Allocation to Study Arms
Patients admitted to the hospital during the study period were assigned to one of three possible general internal medicine physicians based on clinical convenience (i.e., new patient admission was assigned to the most immediately available physician). Each physician was responsible for the clinical care of the individual admitted patient for the duration of their hospitalization. One of the three admitting physicians prescribed ozonated autohemotherapy to all inpatients with severe COVID-19 pneumonia, while the other two physicians did not. Based on the responsible admitting physician, patients were assigned to the ozonated autohemotherapy arm or usual clinical care arm.
Standard Clinical Care
All patients received usual clinical care for COVID-19 pneumonia, which included supplemental oxygen therapy, hydroxychloroquine, lopinavir, ritonavir, corticosteroids, and antibiotics (including azithromycin) at the discretion of the individual patient’s attending physician. Decisions on endotracheal intubation, mechanical ventilation and critical care unit admission were also made at the discretion of the individual patient’s attending physician.
Ozonated Autohemotherapy Intervention
Ozonated autohemotherapy involved intravenous infusion of ozonated autologous whole blood. Initially, 200 mL of autologous whole blood was drawn from the patient’s antecubital vein into a standard plastic disposable blood collection bag (certified SANO3 bag) containing 35 mL of anticoagulant citrate dextrose solution (ACD-A). The blood was then enriched with 200 mL of gas mixture oxygen-ozone with an ozone concentration at 40 μg/mL obtained by Ozonobaric P Sedecal, an ozone generator with CE0120 certificate type IIb. The ozonized blood was then slowly re-infused into the same vein over approximately 10 minutes.
Outcomes
The primary clinical outcome was time to clinical improvement during hospital admission. This time was measured relative to the date of hospital admission. Clinical improvement was defined as a two-point reduction (relative to the patient’s status on hospital admission) on a six-point ordinal scale, or discharge alive from the hospital, whichever came first. The six-point scale was as follows: death (6 points); extracorporeal membrane oxygenation or mechanical ventilation (5 points); noninvasive ventilation or high-flow oxygen therapy (4 points); oxygen therapy without need for high-flow oxygen or non-invasive ventilation (3 points); hospital admission without need for oxygen therapy (2 points); and discharged from hospital or reached discharge criteria (1 point). Discharge criteria were as evidence of clinical recovery (normalization of pyrexia, respiratory rate < 24 per minute, oxygen saturation > 94% on room air, and absence of cough) for at least 72 hours.
This six-point scale and definition of clinical improvement (i.e., two-point improvement in scale) has been used in prior research on intervention for relating to COVID-19 infection. 8 Personnel ascertaining outcomes were not blinded to whether patients received usual care versus ozonated autohemotherapy.
Secondary outcomes were clinical improvement as measured at the 7th, 14th and 28th days after hospital admission. Time to a two-fold decrease in concentrations of C-protein reactive, ferritin, D-dimer and lactate dehydrogenase were also daily measured. Patients also underwent repeat COVID-19 PCR testing at 5 and 15 days after hospital admission – provided that there was co-existing evidence of clinical improvement. Follow-up ceased at the point of hospital discharge, patient death, or 31st day after hospital admission (which ever came first).
Statistical Analysis
All analyses were performed using STATA version 13.0 (StataCorp. 2013. Stata Statistical Software: Release 13. College Station, TX: StataCorp LP). Statistical significance was defined by a 2-sided P-value less than 0.05. The Shapiro-Wilk test was used to determine whether variables were normally distributed. Unadjusted differences between treatment and control arms were then calculated using the two-sample t-test (normally distributed continuous variables), Mann-Whitney U-test (continuous variables with evidence of non-normal distributions) and Fisher’s exact test (categorical variables). Unadjusted times to clinical improvement were compared between the two study arms using Kaplan-Meier survival curves and the log-rank test. Patients were censored at the point of hospital discharge, death or 31st day after hospital admission (whichever came first). The adjusted association between ozonated autohemotherapy and mean time to clinical improvement was estimated using a multivariable linear regression model that adjusted for age, sex, and baseline quick SOFA score. These covariates were pre-specified on the basis of their clinical significance. Patients who had not achieved clinical improvement within the follow-up period were assigned a time value of 31 days. There was no pre-specified sample size calculation for this proof-of-concept study. Instead, all consecutive patients admitted to the study site within a pragmatic one-month period were included in the study cohort.
Results
The cohort included 18 consecutive patients. The mean age was 68 years (SD 15) years and 72.2% (n=13) were male. The baseline characteristics of these patients are presented in Table 1. In total, 9 patients (50%) received ozonated autohemotherapy.
Baseline characteristics
There were no statistically significant baseline differences between the study arms, but these comparisons were limited by small sample size of the present study (Table 1). Nonetheless, the baseline characteristics of the two study arms were qualitatively similar, aside from age (mean age was higher in the usual care arm), weight (mean weight was higher in the usual care arm), and body mass index (mean value was higher in the usual care arm).
Primary outcome: Time to clinical improvement
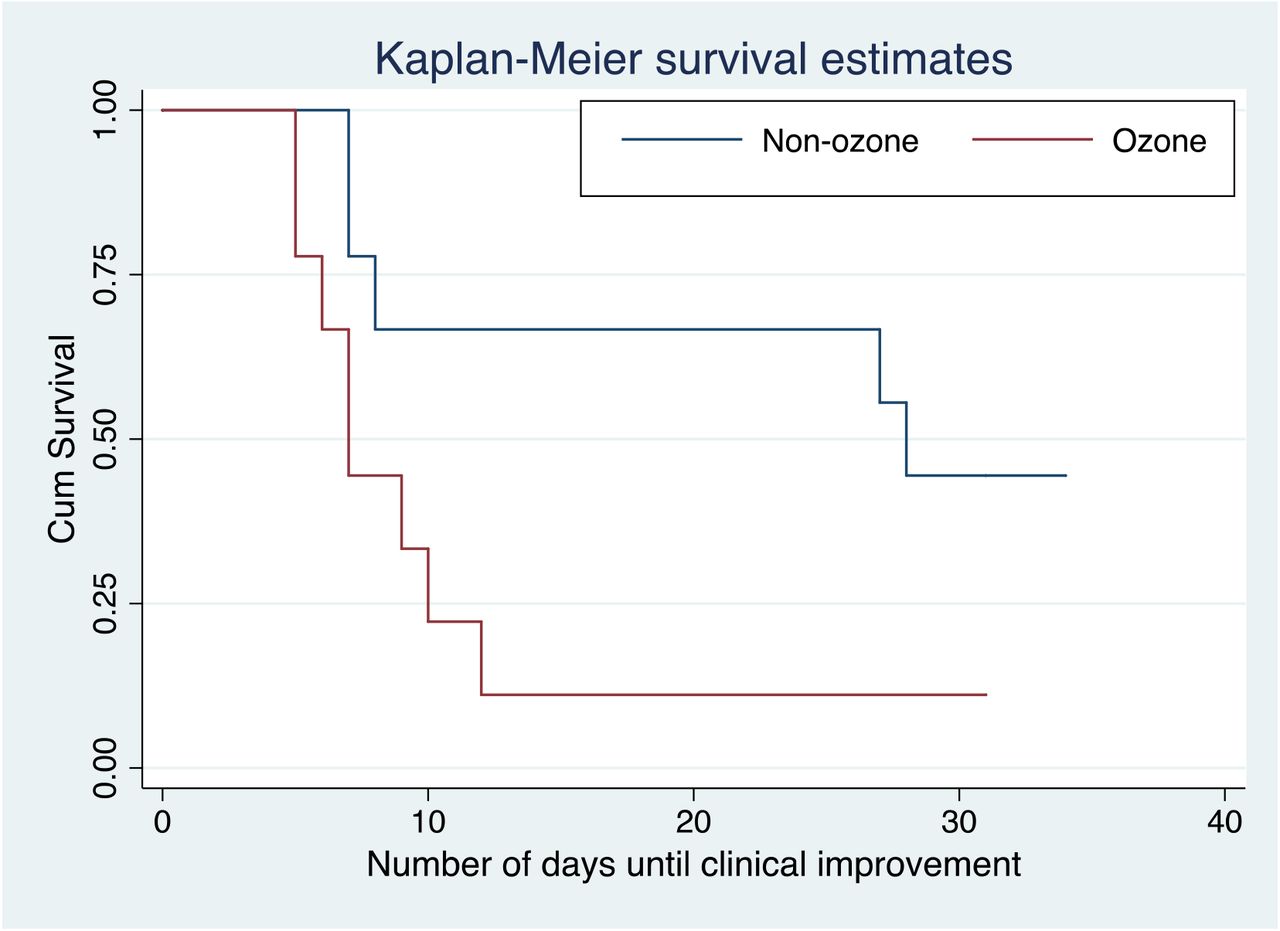
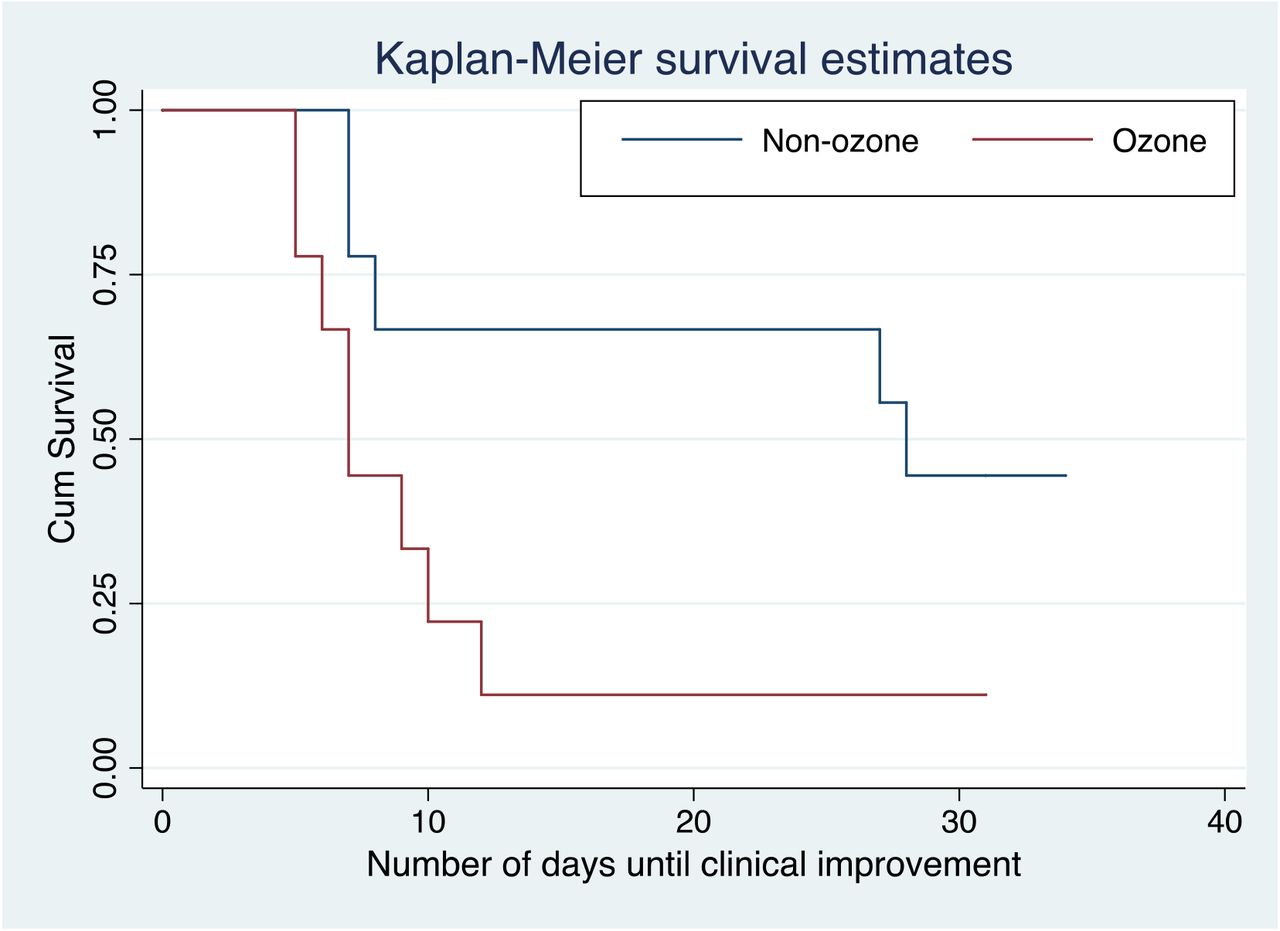
Ozonated autohemotherapy was associated with a statistically and clinically significant lower time to clinical improvement (median [IQR]), 7 days [6-10] vs 28 days [8-31], p=0.04) (Figure 1 and Table 2). In unadjusted linear regression analyses, the mean time to clinical improvement was 12.4 days shorter in the ozonated autohemotherapy arm (−12.4 days; p=0.01; 95% CI −22.49 to −2.39). In adjusted linear regression analyses, the mean time to clinical improvement in the ozonated autohemotherapy arm was 11.3 days shorter (−11.3 days, p=0.04, 95% CI −22.25 to −0.42). We also conducted a post-hoc sensitivity analysis that adjusted for age, quick SOFA and weight – all of which were baseline characteristics with qualitative differences between study arms. The adjusted difference in time to clinical improvement (−11.6 days, p=0.05, 95% CI −23.3 to 0.41) was qualitatively similar in this sensitivity analysis. Unadjusted times to clinical improvement using Kaplan-Meier survival curves and the log-rank test showed a significant difference between groups (Log Rank (Mantel-Cox) Chi-square 4,182. p=0,041) (Fig 1).
{kind=link}
Kaplan-Meier survival curves
Outcomes
Secondary Outcomes
Ozonated autohemotherapy was associated with a significant higher probability of clinical improvement at day 14 (88.8% vs 33.3%, p=0.01). Ozonated autohemotherapy was also associated with a shorter time to a 2-fold decrease of C-reactive reactive (3.5 days [3-28] vs 13 days [8-25], p=0.008), ferritin (8 days [5-10] vs 15 days [10-25], p=0.016), D-dimer (4 days [1-10] vs 19.5 days [10-28], p=0.009) and Lactate Dehydrogenase (9 days [7-9] vs 25 days [12-26], p=0.01). There was a trend towards a lower mean time to negative PCR COVID-19 testing results [13.1 (SD 5.7) vs 21.4 (SD 7.4 days), p=0.05). No differences with respect to ventilator-free days at day 28 (median [IQR]), 28 days [28-28] vs 28 days [0-28], p=0.14), in-hospital or 28-days mortality (11.1% vs 22.2%; p=1), were observed.
Discussion
In this proof-of-concept prospective cohort study of 18 consecutive hospitalized patients with confirmed COVID-19 severe pneumonia, twice-daily ozonated autohemotherapy was associated with a clinically and statistically significant reduction in the time to clinical improvement. Risk-adjusted analyses confirmed the results of the unadjusted analyses. This cohort study provides novel new data pointing to the potential role of ozonated autohemotherapy for treatment of severe COVID-19 pneumonia.
Our findings are consistent with recent reviews describing the potential biologically plausible benefits associated with ozonated autohemotherapy for COVID-19 infection. 9-11 As previously described, there are no prior published data, except for an online report of the Scientific Society of Oxygen-Ozone Therapy (SIOOT). 7
Ozone is a gas found in the stratosphere where it absorbs various ultraviolet radiation. It is considered a toxic gas, but its toxicity effect is dependent on concentration and duration of exposure. Ozone is composed of three oxygen atoms and has a molecular weight of 48 g/mol with a solubility in water about ten-fold higher than oxygen (49 mL in 100 mL, 0.02 M, at 0° C). Consequently, the great solubility of ozone in water allows its immediate reaction with any soluble compounds and biomolecules present in biological fluids.
Ozone is generated by medical devices for medical purposes. Medical ozone generators produce the gas from pure oxygen by passing it through a high voltage gradient (5-13 KV). This yields a gas mixture consisting of at least 95% oxygen and no more than 5% ozone. Thermodynamically is unstable and spontaneously reverts back into oxygen. A medical ozone generator produces concentrations ranging from 1 to 100 μg/ml for safety, but 10-70 μg/ml are commonly used for medical purposes. There are multiples routes for medical ozone administration. Ozone inhalation may be toxic to the pulmonary system and other organs. However, ozonated autohemotherapy has been shown to be safe in multiple randomized clinical trials, observational studies and meta-analyses. 12 The incidence of adverse affects of ozone therapy is very low (estimated at 0.0007%), and typically manifests itself as euphoria, nausea, headaches and fatigue. 13 In general, it is a very safe therapy when administered correctly, with the recommended dose. Complications like air embolism are caused by incorrect administration practices and by using non-certified equipment.
There is a potential role for ozonated autohemotherapy for treatment of patients with severe COVID-19 pneumonia, with several plausible mechanisms of action. When human blood is expose to a gas mixture composed of medical oxygen and ozone, oxygen equilibrates with the extracellular and intraerythrocytic water before becoming bound to hemoglobin until it is fully oxygenated, on the contrary, ozone, more soluble than oxygen, readily dissolves in water and reacts instantaneously with several biomolecules such as, ascorbic acid, urate, free cysteine, GSH molecules and albumin thiol groups, and disappears. The compounds generated during the reactions [reactive oxygen species (ROS) and lipid ozonation products (LOPs)] represent the “ozone messengers” and are responsible for its biological and therapeutic effects. 14
Ozone might improve blood circulation and oxygen delivery to ischemic tissue 15-18 as a result of the concerted effect of nitric oxide, 19 increase intra-erythrocytic 2,3-DPG level, 20 and increase of some prostacyclins such as PGI2. 21 These effects can help to decrease the hypercoagulation that has been observed in COVID patients. 22 Another important role played by ozone in COVID-19 is its immunomodulatory effects. The inflammatory response is a hallmark of severe infection and cytokine modulation is key to avoid patient deterioration. Ozone has potent anti-inflammatory properties through the modulation of the NLRP3 inflammasome which is recognized to play a crucial role in the initiation and continuance of inflammation in various diseases. 23 Ozone may modulate the accumulation of neutrophils locally, the expression of IL-6, TNF-α, and albumin modified by ischemia in the kidneys, as well as increase local antioxidant capacity. 24 Consequently, ozone may also have a role in renal protection, which should be explore in further research.
Regarding to the specific potential action of the ozone against coronavirus, the effectiveness of ozone against pathogens is well known. The ozone appears to be the best agent available for sterilizing water 25, although the in-vivo virucidal activity of ozone in the dosage used in this present study is unknown. It has been suggested that ozone could act a signal molecule in the organism, being generated by human neutrophils and being necessary for antibody-catalyzed formation 26 which play a role in the natural humoral response to infection. 27 Ozone also is capable of inducing the release and modulation of interferons and related cytokine, such as interleukin-2, IFN-γ, tumor-necrosis factor and colony stimulating factors, 28,29 and is also able to modulate and stimulate phagocytic function 30,31 which may have a very positive effect in COVID-19 infection.
Finally, ozone may impair viral replication, as suggested in its effects on SARS and MERS 32 Angiotensin-converting enzyme type 2 (ACE2) cell receptors has been identified as receptor for SARS-CoV-2 33, which could be blocked with specific monoclonal antibodies but also through the control of the nuclear factor erythroid 2–related factor 2 (Nrf2) that regulates and blocks the activity of this receptor. 34 Because ozone is able to cause a rapid Nrf2 activation, 35 it seems very likely that this may be an important physiological mechanism to block endogenous COVID-19 reduplication by preventing contact with this receptor. Furthermore, spike proteins (S) is responsible for receptor binding and membrane fusion. 36 It contains a highly conserved transmembrane domain that consists of three parts: an N-terminal tryptophan-rich domain, a central domain, and a cysteine-rich C-terminal domain. Both, the cysteine-rich domain and tryptophan-rich domain, have been shown to be necessary for fusion. 37,38 Both cysteine and tryptophan, are sensitive to oxidation. It has been hypothesized that ozone metabolites could oxidize cysteine residues, making it difficult for the virus to enter the host cell and preventing viral replication. 39
Notably, our results, while promising, do not prove the benefit of ozonated autohemotherapy in severe COVID-19 pneumonia. This proof of concept study points to the need for further research, such as a well-designed, well-powered multicenter randomized clinical trial, to confirm our findings.
Our study has several limitations. First, the sample size of our cohort is small. Second, the 95% CIs for our adjusted estimates were wide, and do not exclude a 20–30% decrease in the coefficient for time (days) to clinical improvement. Third, as with most observational studies, we cannot exclude the possibility of residual unmeasured confounding. Fourth, it is a single-center study, limiting the external validity of our results. Finally, outcome assessors were not blinded to treatment arm assignment.
The strengths of this study include its pragmatic real-world COVID-19 population, use of objective primary clinical outcome and risk-adjustment using methods of regression modeling analyses.
In conclusion, ozonated autohemotherapy was associated with a significant shorter time to clinical improvement in severe COVID-19 pneumonia patients in this small single-center cohort. Given the wide 95% CI, our study points to the need for further research in this clinical setting with larger sample size across multiples centers.
Question
Is ozonated autohemotherapy associated with shorter time to clinical improvement in patients with severe COVID-19 pneumonia?
Findings
In this single-center proof-of-concept prospective cohort study of 18 patients with severe COVID-19 pneumonia, ozonated autohemotherapy was associated a 11-day reduction in mean time to clinical improvement compared to usual clinical care.
Meaning
Ozonated autohemotherapy was associated with a statistically and clinically significant lower time to clinical improvement in patients with severe COVID-19 pneumonia.
Acknowledgements
Dr. Wijeysundera is supported in part by a Merit Award from the Department of Anesthesiology and Pain Medicine at the University of Toronto, and the Endowed Chair in Translational Anesthesiology Research at St. Michael’s Hospital and University of Toronto.
References




Subject Area
Reviews and Context
0
Comment
0
TRIP Peer Reviews
0
Community Reviews
0
Automated Services
0
Blogs/Media
Author Videos