
Abstract
Protection of healthcare workforce is of paramount relevance for the care of infected and non-infected patients in the setting of a pandemic such as coronavirus disease 2019 (COVID-19). Healthcare workers are at increased risk to become infected because of contact to infected patients, infected co-workers and their community outside the hospital. The ideal organisational strategy to protect the healthcare workforce in a situation in which social distancing cannot be maintained at the workplace remains to be determined. In this study, we have mathematically modelled strategies for the employment of hospital workforce with the goal to simulate health and productivity of the workers. Therefore, deterministic models were extended to account for stochastic influences potentially occurring in rather small populations. The models were also designed to determine if desynchronization of medical teams by dichotomizing the workers may protect the workforce. Our studies model workforce productivity depending on the infection rate, the presence of reinfection and the efficiency of home office. As an application example, we apply our theory to the case of coronavirus disease 2019 (COVID-19). The results of the models reveal that a desynchronization strategy in which two medical teams work alternating for 7 days reduces the infection rate of the healthcare workforce. In case of immunity to the infectious agent this affect is mainly relevant at early stages of the pandemic. This effect is independent on infection rates and increases the overall workforce productivity under certain situations.
1. Introduction
During the spread of worldwide pandemics, protecting and supporting caregivers to maintain the workforce in hospitals is a crucial and challenging task. Under such extraordinary situations, the efficiency of healthcare workforce is threatened by several factors including: 1) infected patients, 2) infected co-workers and 3) infected persons outside the hospital. This is of high importance in the current epidemics of coronavirus disease 2019 (COVID-19) given that the virus may be transmitted by asymptomatic persons based on the long incubation period averaging at 5 days (1, 2). Unlike for most other professions, social distancing is typically not possible in medical teams where healthcare workers are required to work in close contact with patients and coworkers.
Currently, little is known about which work organizational strategies in the hospital are most suitable protect the healthcare workforce. Potential strategies may include prolonging duty hours and thereby limiting interactions between coworkers or complete desynchronization of the workforce in which teams are dichotomized and each half of the team works for one week alternatively.
In this short report, we perform computer simulations of biophysical models of coronavirus epidemics of COVID-19 in a healthcare working team, and discuss the efficiency of different work strategies during the viral outbreak.
Different types of mathematical models have been used to study epidemiology. In the classical Susceptible Infectious Recovered (SIR) model, a susceptible patient (S) can be infected (I), and the infected person can recover (R), without the risk of reinfection. Variants of this model, are the Susceptible Infectious Susceptible (SIS) and Susceptible Exposed Infectious Recovered (SEIR) models (3). The SEIR model in which the recovered patients are susceptible again, has already been used for modeling purposes during the COVID-19 outbreak (4). Also in the context of the COVID19, SEIR models have been used to model control of expansion and have been extended to include age and asymptomatic cases (5, 6). Another extension of SEIR models that have been presented in this context consists on including persons in quarantine (QSEIR model) (7, 8).
Here, we put forward SIS and SIR models by dividing the infectious persons into a latent and infected state in order to account for the potentially long asymptomatic phase of COVID-19. Next, have developed two time-dependent compartmental models with and without reinfection by adapting the SAIR model of (9-11). Next, we add a variable to account for work W and build two mathematical models for COVID-19 described by ordinary differential equations (ODE). These are denoted by Susceptible Latent Infected Work (SLIW) model and Susceptible Latent Infected Recovered Work (SLIRW) model. In our SLIW model, the workers can be healthy and susceptible to be infected, S, infected in the incubation period, L, infected presenting symptoms, I. Additionally in the SLIRW model, after recovery the patients become immune to new infections, R. Additionally, the models are adapted to account for work done, W, by the non-infected workers.
To investigate the possible workforce organizations, we use ODE describing the dynamics of the models including time-dependent parameters in which the rate change based on their location, that is, in-hospital compared with home office.
The rest of the report is organized as follows. We study and compare organizational strategies on the hospital workforce in the situation of a pandemic on productivity in the absence of reinfection and with reinfection (section 2), and present the results of simulations (section 3). Finally, our results are summarized and discussed (section 4).
2. Models
2.1. Sketch of the models
Figure 1 shows the SLIW and SLIWR models with compartmentalization that we describe in detail in Section 2.1.2 and Section 2.2.2, respectively. In our models, we consider that a group of healthcare workers are divided in two teams of equal size. At any time, one team is at the workplace whereas the other team stays at home. A dichotomous work switch is implemented as follows (Figure 1A): during the first week Team 1 stays at the workplace and Team 2 at home; during the second week Team 1 stays at home and Team 2 at the workplace; next the teams continue alternating their location at the end of each week. When at the workplace, each healthy susceptible worker can become latent at a time-dependent infection rate that is larger than when staying at home. Latent workers develop the infection at the workplace, at the same rate than at home. Infection of a susceptible by a latent worker can only occur in the workplace. We also assume that infected workers recover at the same rate at the workplace than at home, becoming again susceptible (SLIW) or fully recovered and immune (SLIRW).

Sketch of the Susceptible Latent Infected Work model (SLIW) and Susceptible Latent Infected Recovered Work model (SLIRW) models. (A) Scheme of work shifts between two teams changing their location in the workplace and at home once per week. (B) Infection dynamics at the workplace and home. See Sec. 2.2 and 2.3 for further details. Image of the doctor adapted from (12).
2.2. Models with reinfection (SILW)
2.2.1. One group of healthcare workers
Our first infection model describes the evolution in time t of the number S of healthy workers susceptible to be infected, the number, L, of infected persons in a latent state, and the number I of infected persons presenting symptoms. To study the impact on the workers’ efficiency, we introduce a function W that accounts for the amount of work done by all the available workers. The dynamics of each population are described by the following system of ODEs.
 where α is the infection rate, resulting into an infected in a latent state. f(t)is a function accounting for the number of people infected in the city, which we assume is growing in time. β is the infection rate when the person is infected by a co-worker, s is the activation rate of the sickness, in which a patient in a latent state starts presenting symptoms. r is the recovery rate, where an infected patient recovers and becomes healthy. W is a function that accounts for the work output of the workers, for simplicity we assume its growth is proportional to the number of available workers. For simplicity, we consider the death rate negligible and we do not consider recoveries coming from latent patients. In our simulations reported below, we set the initial condition to S(0)=300, L(0)=0, I(0)=0, and W(0)=0, thereby representing a large unit with 300 workers.
where α is the infection rate, resulting into an infected in a latent state. f(t)is a function accounting for the number of people infected in the city, which we assume is growing in time. β is the infection rate when the person is infected by a co-worker, s is the activation rate of the sickness, in which a patient in a latent state starts presenting symptoms. r is the recovery rate, where an infected patient recovers and becomes healthy. W is a function that accounts for the work output of the workers, for simplicity we assume its growth is proportional to the number of available workers. For simplicity, we consider the death rate negligible and we do not consider recoveries coming from latent patients. In our simulations reported below, we set the initial condition to S(0)=300, L(0)=0, I(0)=0, and W(0)=0, thereby representing a large unit with 300 workers.
2.1.1 Two groups of healthcare workers
In order to study the desynchronization strategy, in which the workers are divided in half, one group works for one week in the hospital while the other works at home, and the week after they change their functions. In doing so, we model it as two groups of healthy persons susceptible to be infected, H1 and H2, two groups of infected persons in a latent state, L1 and L2,and two groups of infected persons presenting symptoms, I1 and I2. The dynamics of each population are described by the following system of ordinary differential equations
 for the first group and
for the first group and
 for the second group. The rate of change of the work output obeys
for the second group. The rate of change of the work output obeys

For this model, we use the same parameters than in the previous model, except for αj and βj(with j=1,2). Group 1 is one week at home and one week at the hospital, and Group 2 the opposite. Therefore we simulate our model for the first seven days with β2 =0, α2 =0.1α1, because the two groups are not in contact with the co-workers, and we assume that the probability to become infected is higher when working in the hospital. For the following seven days, we introduce a switch of the group’s location, by exchanging their parameter values. This procedure is repeated every 7 days. We assume that the productivity decreases during home office, therefore we choose A(t)=1 and B(t)<A(t) during the odd weeks and B(t)=1 and A(t)<B(t) during the even weeks.
Based on the available data of COVID19, we choose s= 1/5day, because the average duration of the incubation period is 5 days, and r= 1/14day because the average recovery time is 14 days. Additionally, we chose a logistic function  with characteristic time τ= 5.
with characteristic time τ= 5.
2.2. Model without reinfection allowing for recovery (SLIRW)
2.2.1. One group
In this section we study the effect of a model in which the patients develop immunity to the disease after the infection. Therefore, we add a variable for the recovered patients, R, which cannot become infected after reaching that state, and the dynamics are described by the following system of ordinary differential equations
With S(0)=300, L(0)=0, I(0)=0, R(0)=0 and W(0)=0 as initial condition.
2.2.2 Two groups
Here the desynchronization strategy is modelled for a situation in which the workers develop immunity and cannot be reinfected. This includes two groups of healthy persons susceptible to be infected, H1 and H2, two groups of infected persons in a latent state, L1 and L2,and two groups of infected persons presenting symptoms, I1 and I2. The dynamics of each population are described by the following system of ordinary differential equations, for the first group
 whereas for the second group
whereas for the second group
The total work done by the two groups is given by

3 Results
3.1 Simulations of the SLIW model
First, we study the effect of the infection rates on the health of the workers. In figure 2 we show the simulations of our systems of ODEs with two representative sets of parameters, low infection rate (Figure 2A) and high infection rate (Figure 2B). Regardless the values, we observe that the strategy of dividing the workers in two groups decrease the number of infected workers, thus increasing the available workforce. In figure 3 A, B we show the number of workers as a function of the infection rates. We observe that with the desynchronization strategy the number of healthy workers is higher than with the normal strategy.

Representative examples of infection rates of healthcare workers with and without desynchronization (SLIW). Number of healthy workers as a function of time for two sets of parameters values. (A) Assumption: low infection rate: α=0.1, β=0.001. α1=0.1, β1=0.001during the odd weeks, and α2 =0.1, β2 =0.001during the even weeks.
(B) Assumption: high infection rate: α=0.2, β=0.002. α1=0.2, β1=0.002 during the odd weeks, and α2 =0.2, β2 =0.002 during the even weeks. All rates are in units of day-1.

Impact of infection rates on healthcare workers availability. Number of healthy workers as a function of the infection rates. (A) Normal strategy. (B) Desynchronization strategy α stands for α1 during the odd weeks and α2 during the even weeks, idem for β. The rates α and β in units of day-1.
So far, we have observed that the desynchronization strategy increases the number of healthy workers. Next, we aim to determine the economic impact of this strategy for the company. Therefore, we simulate our model for 6 weeks and we represent the value of W divided by the total number of workers as a function A(t) and B(t) during the home office week (Figure 4). We observe that if the productivity decreases by 50% during the home office week, the normal strategy performs better than the desynchronized strategy. For higher values (75% or 100%) of the home office productivity, the desynchronized strategy outperforms the normal strategy for high infection rates.
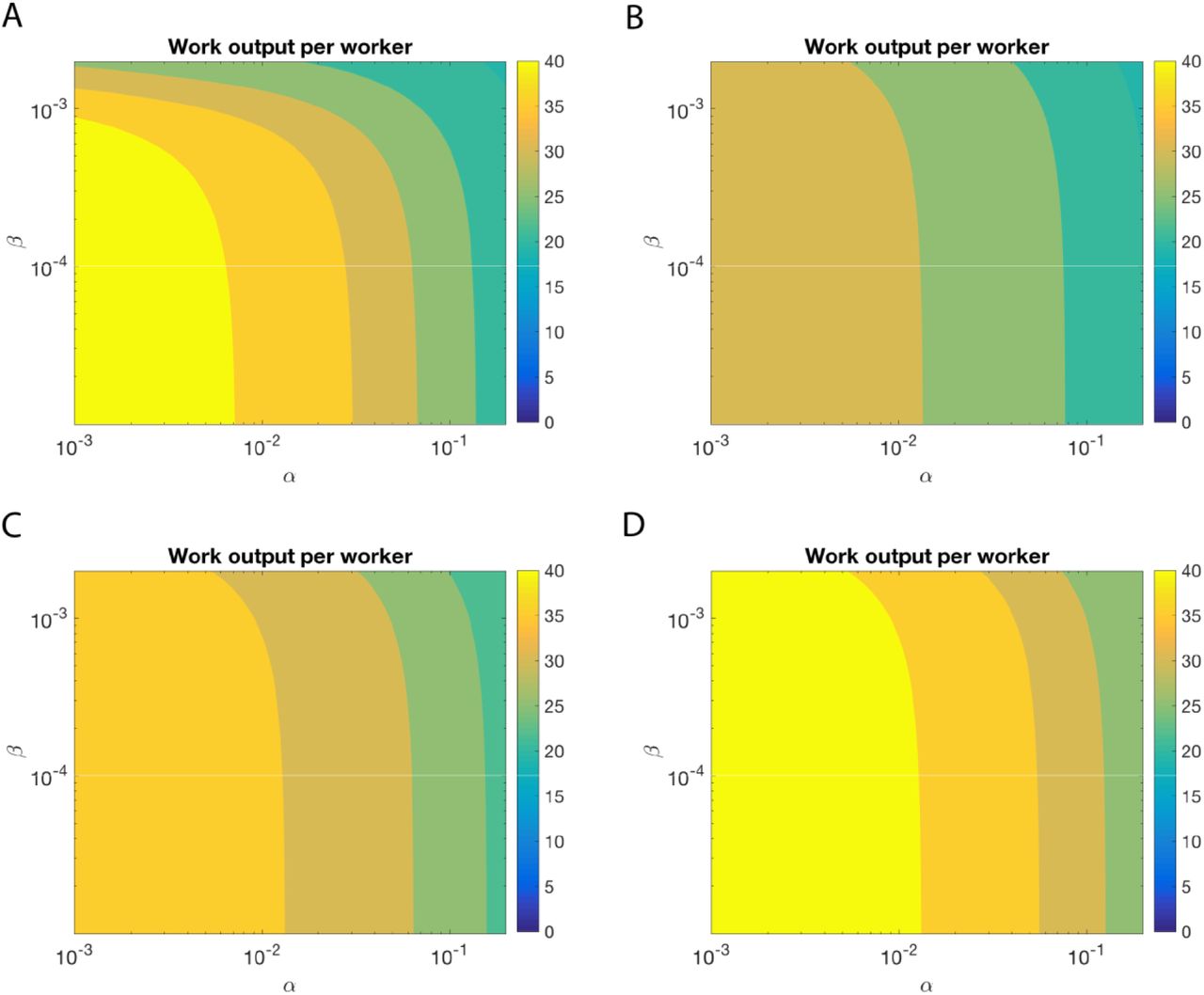
Impact of infection rates on the productivity. Value of the work output W(t) divided by the total number of workers at the end of the simulation (6 weeks) for the normal strategy (Strategy 1), and different values of the home office productivity with the desynchronized strategy (Strategy 2). (A) Strategy 1, (B) Strategy 2, with productivity at home B=0.5, (C) Strategy 2, productivity at home B=0.75, (D) Strategy 2, productivity at home B=1. The rates α and β in units of day-1.
3.2. Simulations of the SLIRW model
First, we study the effect of the infection rates. In figure 5 we show the simulations of our systems of ODEs with two representative sets of parameters. Regardless the values, we observe that the strategy of dividing the workers in two groups increase the number of healthy workers during the peak of infection. In figure 6 we show the number of minimum healthy workers as a function of the infection rates during a 6 weeks simulation.

Representative examples of infection rates of healthcare workers with and without desynchronization (SLIRW). Number of healthy workers (susceptible plus recovered) as a function of time.
(A) Assumption: low infection rate: α=0.1, β=0.001. α1=0.1, β1=0.001during the odd weeks, and α2 =0.1, β2 =0.001during the even weeks.
(B) Assumption: high infection rate: α=0.2, β=0.002. α1=0.2, β1=0.002 during the odd weeks, and α2 =0.2, β2 =0.002 during the even weeks. All rates are in units of day-1.

Impact of infection rates on healthcare workers availability during the peak infection rate. Minimum fraction of healthy workers during a simulation as a function of the infection rates. (A) Normal strategy. (B) Desynchronization strategy α stands for α1 during the odd weeks and α2 during the even weeks, idem for β. The rates α and β in units of day-1.
So far we have observed that the desynchronization strategy increases the number of healthy workers also in the situation without reinfection. To determine the economic impact, we simulate our model for 6 weeks and we represent the value of W as a function α and β, for different values of the home office efficiency (Figure 7).

Impact of infection rates on the productivity. Value of W(t) at the end of the simulation for the normal strategy (Strategy 1), and different values of the home office productivity with the desynchronized strategy. (A) Strategy 1, (B) Strategy 2, productivity at home 0.5, (C) Strategy 2, productivity at home 0.75, (D) Strategy 2, productivity at home 1. The rates α and β in units of day-1.
3.3. Comparison: SLIW vs SLIRW models
Next, we compared the SLIW and SLIRW. In doing so, we defined iR as the infection rate and we computed the value of W as a function the home office efficiency for different values of the infection rate, by choosing α=0.1iR and β=0.001iR (Figure 8). We observe that for the SLIW model requires a smaller home office efficiency than the SLIRW model.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Value of W (work done) at the end of the simulation as a function of the home office efficiency for different infection rates, where α = 0.1iR and β = 0.001iR. The dashed threshold is the productivity with the 1 group strategy. (A) SLIW model. (B) SLIRW model. (C) Value of home office efficiency B needed to be as productive as the normal strategy, as a function of infection rates, where α = 0.1iR and β = 0.001iR for SLIW and SLIWR models.
4 Discussion
Given the urgent need to protect caretakers, we present here modelling approaches that address the impact of desynchronization of healthcare workforces in a short report. We have developed two time-dependent compartmental models (SLIW/SLIRW with and without reinfection) by adapting the SAIR model of (9-11). A time-dependent compartmental model was included to account for the desynchronization of healthcare teams. In addition to the availability of healthcare workers, we modelled productivity by incorporating different levels of work performed at home office.
The SLIW model showed that the desynchronization strategy is associated with an increase of the number of healthy workers compared to no desynchronization (Figure 2). This effect is present with both high and low levels of infection rates (Figure 3).
Next, we incorporated productivity of the workers in the period of home office. In practice, productivity of home office may depend on the tasks, which may be done outside the hospital such as writing reports. We have modelled the productivity rate of home office as a function of the infection rates. Figure 4 and figure 8 show that, for our case study model of COVID-19, a decrease of productivity to 50% during home office (only half of the time can be used for productive work) does not imply a substantial decrease of the overall productivity. However, if the productivity at home office is above 75%, overall productivity is increased with a desynchronization strategy for high infection rates.
When the SLIRW model was used to incorporate full recovery without the potential of reinfection, the protective effect of desynchronization weans over time (Figure 5). In this situation, however, the number of healthy workers with desynchronization increases, especially during the peak of infected workers (Figure 6). This observation is potentially the consequence of workers being immune to the infection thereby not requiring a desynchronization anymore. The protection of healthcare workforce (Figure 6) and productivity (Figure 7) also depends to the infection rate in SLIRW model.
Next, we aimed to determine the ideal level of productivity for each model (Figure 8). The ideal home office productivity strongly depends on infection rates in the model with reinfection (SLIW). In this model productivity is required to be around 60% for infection rates 3 and 10. In the model without reinfection (SLIRW), which is rather the case with COVID-19, the home office productivity needs to be higher in order to keep overall productivity similar between the one and two group strategy.
However, the way the model was designed, we artificially included a handicap to the desynchronization strategy. As long as it remains unclear if reinfection is possible, the desynchronization strategy would be maintained. Such strategy would be stopped for recovered workers if reinfection does not occur because of immunity.
Our model has limitations that be addressed in multiple ways. Accounting for noise will be required in our model to identify if the stochastic effects can change the studied mean-field dynamics. Another extension would be to add asymptomatic patients to the model, that is, patients that pass the infection without presenting symptoms. Furthermore, the model does neither address at what costs such a desynchronization strategy would come. Given that a complete set of workers is always present, there might be losses of acquired experience for the group absent. Furthermore, these models neither address the impact of length of duty shifts nor the impact of potentially impaired communication as a consequence of decreased interactions between healthcare workers.
In summary, our model is a starting point to study how to protect healthcare workers while determining economic impact during a pandemic outbreak.
Data Availability
All data are available in the manuscript.



