
Abstract
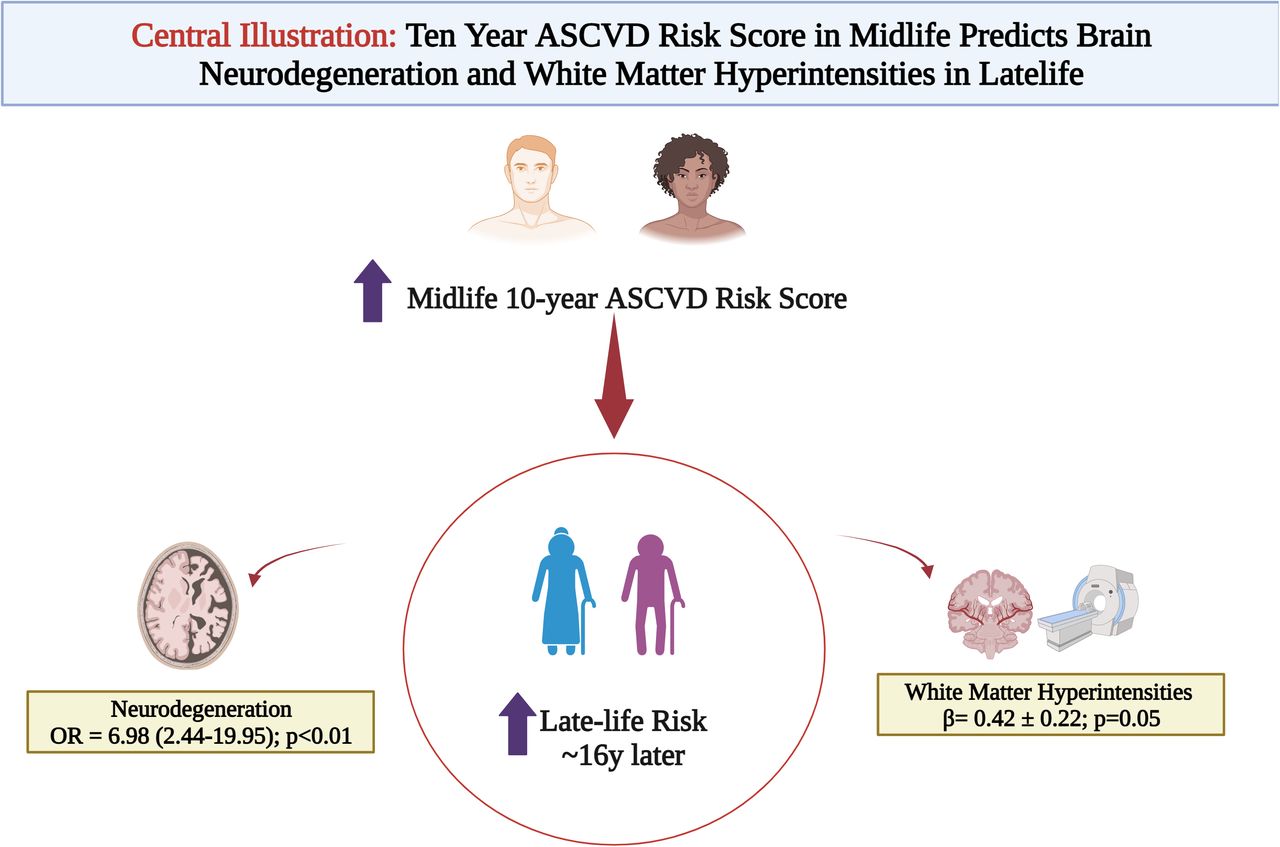
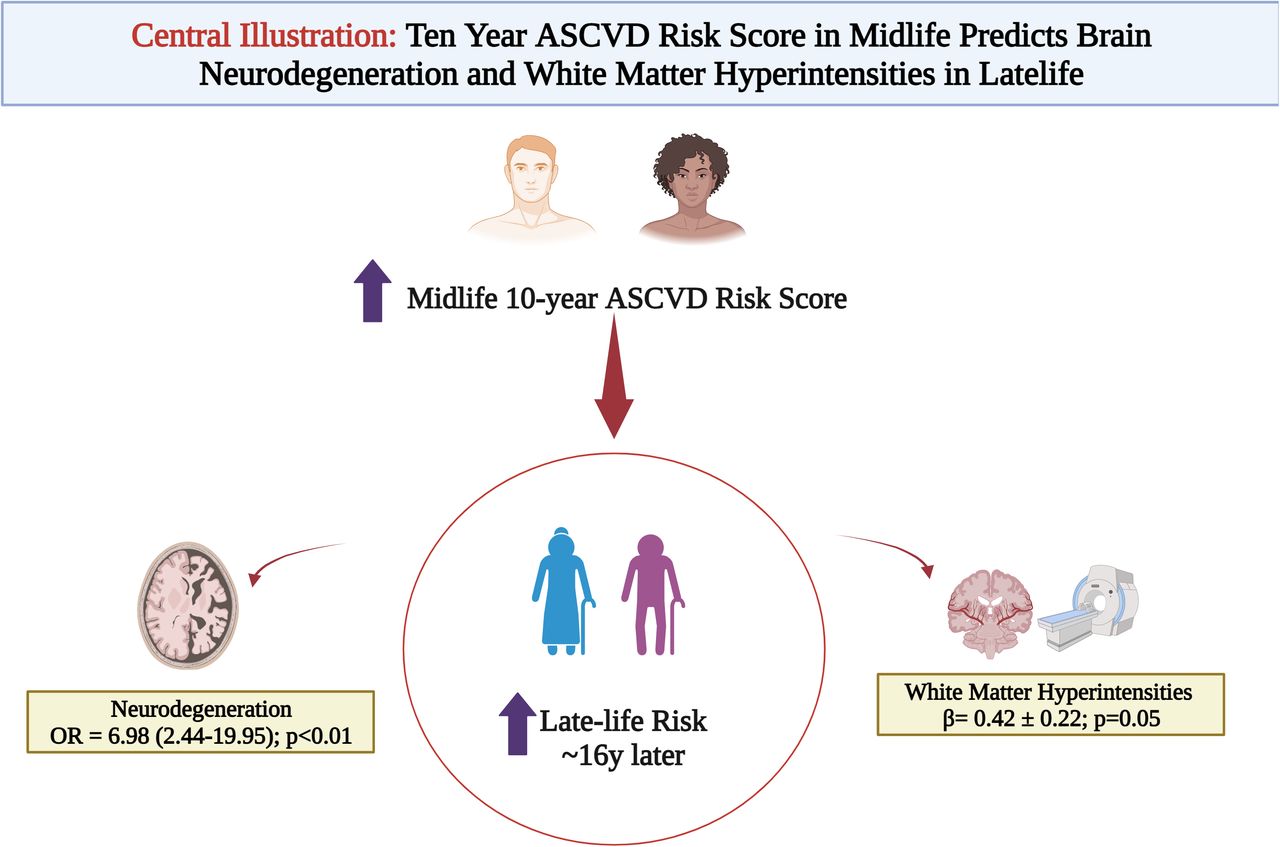
Introduction Atherosclerotic cardiovascular disease (ASCVD) risk factors in mid-life have been associated with cognitive decline and late-life dementia. However, the role of these risk factors in preclinical Alzheimer’s disease (AD) pathophysiology remains elusive. We investigated whether mid-life 10-year pooled cohort equations (PCE) based ASCVD risk is associated with late-life amyloid, tau, neurodegeneration [AT(N)] measures and white matter hyperintensities (WMHI).
Methods Participants enrolled in the Heart Strategies Concentrating on Risk Evaluation (Heart SCORE) study between 2003-2005 (mid-life) and underwent brain MRI and PET scans in 2018-2022 (age >65 years, late-life) to detect and quantify amyloid (A, PiB-PET) and tau (T, Flortaucipir (FTP) PET) deposition, cortical thickness (N) and white matter hyperintensities (WMHIs). Mid-life PCE ASCVD risk was categorized as; borderline (5%-7.4%), intermediate (7.5%-<15%), or high (≥15%). Association of midlife ASCVD risk HR (5% CI) was assessed using logistic and linear regressions with A, T, or N and chi square beta coefficients for WMHI in latelife.
Results Over a ∼16y follow up, in 135 participants (mean age 73y), A and T showed no significant association with mid-life ASCVD risk. Neurodegeneration had a graded association with mid-life ASCVD risk categories (ORASCVD high vs low risk% 6.98 [2.44-19.95]; p<0.05) driven by self-identified Black race and age. In a subset n=60, ASCVD risk score was also associated with WMHIs ((β=0.42 ± 0.22; p=0.05) in a model adjusted for inflammation and education.
Conclusions In this asymptomatic, diverse cohort, 10y ASCVD risk was predictive of late-life neurodegeneration and white matter hyperintensities but not amyloid or tau. These data suggest that ASCVD risk factors in midlife may lead to a state of vulnerability (through increased neurodegeneration and white matter hyperintensities) which may progress to cognitive decline and dementia. Further mechanistic studies are warranted to test this hypothesis.
{kind=link}
Competing Interest Statement
The authors have declared no competing interest.
Funding Statement
SOURCES OF FUNDING This work was funded by grants R01-AG072641, R01-AG052446 and R01-AG064877 from the National Institute on Aging. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Author Declarations
I confirm all relevant ethical guidelines have been followed, and any necessary IRB and/or ethics committee approvals have been obtained.
Yes
The details of the IRB/oversight body that provided approval or exemption for the research described are given below:
Institutional Review Board permission by the University of Pittsburgh was obtained. CONSENT STATEMENT All human participants provided informed consen
I confirm that all necessary patient/participant consent has been obtained and the appropriate institutional forms have been archived, and that any patient/participant/sample identifiers included were not known to anyone (e.g., hospital staff, patients or participants themselves) outside the research group so cannot be used to identify individuals.
Yes
I understand that all clinical trials and any other prospective interventional studies must be registered with an ICMJE-approved registry, such as ClinicalTrials.gov. I confirm that any such study reported in the manuscript has been registered and the trial registration ID is provided (note: if posting a prospective study registered retrospectively, please provide a statement in the trial ID field explaining why the study was not registered in advance).
Yes
I have followed all appropriate research reporting guidelines, such as any relevant EQUATOR Network research reporting checklist(s) and other pertinent material, if applicable.
Yes
The Chan Zuckerberg Initiative, Cold Spring Harbor Laboratory, the Sergey Brin Family Foundation, California Institute of Technology, Centre National de la Recherche Scientifique, Fred Hutchinson Cancer Center, Imperial College London, Massachusetts Institute of Technology, Stanford University, University of Washington, and Vrije Universiteit Amsterdam.



