
ABSTRACT
Objective To investigate the association between SARS-CoV-2 vaccination and myocarditis death
Design Population based comparative mortality study
Setting Japan
Participants Vaccinated population was 99 834 543 individuals aged 12 years and older who have been received SARS-CoV-2 vaccine once or twice by 14 February 2022. Reference population was defined persons aged 10 years and older from 2017 to 2019.
Main outcome measures The primary outcome was myocarditis death, defined as the case with “myocarditis” for cause of death and with onset 28 days or less after vaccination disclosed on 5 August 2022. Myocarditis mortality rate ratio (MMRR) of the SARS-CoV-2 vaccinated to the reference population by 10-year age group and standardised mortality ratio (SMR) were calculated. Mortality odds ratios (MORs) by 10-year age group were also calculated for supplementary analysis. Healthy vaccine effect-adjusted MMRRs (adMMRRs) or adjusted SMR (adSMR) were calculated by dividing MMRRs or SMR by 0.24 respectively.
Results Number of myocarditis death which met the inclusion criteria were 38 cases. MMRR (95% confidence interval) was 4.03 (0.77 to 13.60) in 20s, 6.69 (2.24 to 16.71) in 30s, 3.89 (1.48 to 8.64) in 40s, respectively. SMR of myocarditis was 2.01 (1.44 to 2.80) for overall vaccinated population, 1.65 (1.07 to 2.55) for those 60 years or older. Estimated adMMRRs and adSMR were about 4 times higher than the MMRRs and SMR. Pooled MOR for myocarditis were 205.60 (133.52 to 311.94).
Conclusion SARS-CoV-2 vaccination was associated with higher risk of myocarditis death, not only in young adults but also in all age groups including the elderly. Considering healthy vaccinee effect, the risk may be 4 times or higher than the apparent risk of myocarditis death. Underreporting should also be considered. Based on this study, risk of myocarditis following SARS-CoV-2 vaccination may be more serious than that reported previously.
ALREADY KNOWN ON THIS TOPIC There are many epidemiological studies showing increased myocarditis incidence after SARS-CoV-2 vaccination. There are also some case reports of fulminant myocarditis after receiving SARS-CoV-2 vaccine. However, no epidemiological studies focusing the association between vaccination and myocarditis death.
WHAT THIS STUDY ADDS Myocarditis mortality rate ratios (MMRRs) and their 95% confidence intervals (95% CIs) after receiving SARS-CoV-2 vaccine compared with that in the reference population (previous 3 years) were significantly higher not only in young adults (highest in the 30s with MMRR of 6.69) but also in the elderly. Standardised mortality ratio (SMR) for myocarditis was 1.65 (1.07 to 2.55) for those 60 years or older and 2.01 (1.44 to 2.80) in overall age. The risk of myocarditis mortality in the SARS-CoV-2 vaccinated population may be 4 times or higher than the apparent MMRRs considering healthy vaccinee effect. Unreported post-vaccination deaths should also be considered as suggested by the extremely high myocarditis mortality odds ratio (205.60; 133.52 to 311.94).
INTRODUCTION
Amongst the several safety concerns of SARS-CoV-2 vaccination, myocarditis is one of the most important adverse reactions which package insert warn as “Post marketing data demonstrate increased risks of myocarditis and pericarditis”.1,2 After a notification of a possible link between SARS-CoV-2 vaccination and myocarditis by the US Centers for Disease Control and Prevention (CDC),3 a number of case reports have been published 4 and several fatal cases have also been published.5-12 In Japan, a 27-year-old professional athlete with no history of symptomatic illness except orthopedic problem was rushed to hospital with cardiac arrest on day eight of the first dose of mRNA-1273 (Moderna) vaccine and subsequently died, with autopsy results revealing myocarditis.12 A non-comparative epidemiological study indicated that the highest incidence of myocarditis was reported in male patients between the ages of 16 and 29 years.13 Comparative epidemiological studies showed that SARS-CoV-2 vaccination is associated with increased risk of myocarditis especially in adolescent and young adults without exception.14-18 However, they reported that myocarditis after vaccination was mild14,16 and did not focus on the fatal cases.14-18 The package inserts of SARS-CoV-2 vaccine do not mention the possibility of death from myocarditis after the vaccination.1,2 To our best knowledge, no epidemiological studies have conducted to investigate the association of increased risk of SARS-CoV-2 vaccine on myocarditis death.
The primary objective of this study is to investigate association between SARS-CoV-2 vaccine and myocarditis deaths comparing mortality rate with general population, then to provide a new discussion on the healthy vaccinee effect in using SARS-CoV-2 vaccine, especially on death. In addition, all-cause death after vaccination was also investigated and under-reporting of deaths was discussed.
METHODS
This study compared myocarditis mortality rate in the SARS-CoV-2 vaccinated with that in the general population in Japan. The study was based on the materials and the vital statistics disclosed by the Japanese government.
Data sources and case definition
1. Vaccinated population
The vaccinated population was defined as those who had received the first or the second doses of SARS-CoV-2 vaccine since the start of the vaccination program (17 February 2021) until 14 February 2022. The number of persons received vaccine by number of doses was disclosed by the Japanese Cabinet Office by 10-year age group without background information for sex, vaccine type and others.19 According to this information, 99 834 543 persons received the first dose and 99 117 143 persons received the second dose. Of the Japanese population aged 12 years or older, 89.6% received at least one dose of SARS-CoV-2 vaccine.
The number of vaccinated populations by number of doses, by vaccine type for all age groups combined was also disclosed.20 This information was used to estimate the interval between the first and the second dose. The discrepancy between the total number of vaccinees by age group and the total number of vaccinees by vaccine type may be due to the presence of vaccination cases of unknown age group at the time of reporting.
2. Death cases after receiving SARS-CoV-2 vaccine
Data for the death cases after receiving SARS-CoV-2 vaccine were based on “the summary list of death cases after SARS-CoV-2 vaccination” as pdf files that were disclosed by the panels of experts on vaccination and adverse reactions under Japan’s MHLW at 5 August 2022.21-23 Both authors independently converted the pdf data into excel files and confirmed data matched. Total number of death cases reported by 22 July and disclosed on 5 August was 1 797 (Fig 1).

In Japan, doctors are required to report serious adverse reactions to vaccine in general including death within 28 days if they suspected an association with vaccination.24 For SARS-CoV-2 vaccine, those occurred during the period considered by a physician as highly relevant to vaccination were required to report at the beginning of the vaccination program.24 Subsequently, physicians were required active consideration of reporting myocarditis, pericarditis and thrombosis occurring within 28 days after vaccination if they suspected an association with vaccination. 25 Therefore, we defined the death cases for comparison of mortality rate as those in which the onset (start of signs and symptoms leading to death) was known as occurred within 28 days after the last dose of SARS-CoV-2 vaccine (reasons for inclusion of onset within 28 days are explained later in detail). We restricted the vaccinee who received one or two dose and excluded those with third or fourth dose to avoid further healthy vaccinee effect.26,27 Number of included death cases was 1 362 in total (Fig 1).
3. Myocarditis death after SARS-CoV-2 vaccination
“Myocarditis death case” after vaccination was defined as the cases in which “myocarditis” was described in the cause of death column of the above summary list, regardless of diagnostic method. They were classified as death from I40 (acute myocarditis) under the 10th revision of the International Statistical Classification of Diseases and Related Health Problems (ICD-10).
On the 5 August 2022 list, number of included myocarditis death reports was 38, of which 27 were on the 18 February 2022 list and 11 new deaths were added since then.
Diagnostic bases for myocarditis are classified according to the information on the summary list of death cases disclosed on 5 August 2022 as follows: 1. Autopsy and/or myocardial biopsy, 2. Elevated Troponin with blood test, 3. Other blood test and/or (ECG and/or UCG), 4. Only symptoms. Diagnostic basis for the lower number does not include the diagnostic basis for the higher number.
4. Calculation of person-years of exposure for vaccinated population
Average days from first to second dose are different among three products: 21 days for BNT162b, 1 28 days for mRNA-1273, 2 and 40 days for ChAdOx1 nCoV-19.28,29 The number of second dose were 84 023 380 for BNT162b, 16 090 036 for mRNA-1273, and 58 300 for ChAdOx1 nCoV-19 (Table S1). However, the number of doses by age group and by vaccine type was not disclosed. Therefore, weighted average days from first to second dose for overall ages was estimated as 22.14 days in overall ages (Table S2).
Based on the above information, the person-years of observation for the first dose and the second dose were calculated as follows: D = (A ×22.14+B ×5.86)/365, E =C×28/365, F= D + E. where 22.14 is the weighted average days from the first dose to the second dose and 5.86 is 28 days of observation period - 22.12, A is the number of vaccinees who received the first dose, B is that with only the first dose, C is that with the second dose, D is the person-years for the first dose, E is for the second dose and F is total person-years.
5. Reference population and death
We chose the general Japanese population during the period from 2017 through 2019 in the pre-COVID-19 pandemic era as reference population and death for comparison based on the vital statistics in 2017, 2018 and 2019.
Myocarditis mortality rates in the reference population were calculated from the total number of myocarditis deaths by total population by 10-year age groups in three years from 2017 to 2019.30-35
Outcome measures and statistical analyses
Primary outcome measure was myocarditis mortality rate. We compared the observed mortality rate of myocarditis with the expected mortality rate using data for reference population. Myocarditis mortality rate ratios (MMRRs) and their 95% confidence intervals (95%CIs) by 10-year age group were calculated.
Sensitivity analysis was performed as follows:
Standardised mortality ratio (SMR) for overall age stratified by 10-year age groups.
SMRs for 3 age groups (12-39, 40-59 and 60 or older) stratified by 10-year age groups.
SMR by the vaccination status after the first or second dose.
SMR for all-cause death.
Mortality odds ratio (MOR) by 10-year age group for myocarditis applying reporting odds ratio (ROR).36
MMRRs and SMR adjusted by the healthy vaccinee effect were estimated: Healthy vaccinee effect by SARS-CoV-2 vaccination expressed as the rate ratio of mortality rate in vaccinated to that in the reference general population was shown approximately as 0.10 to 0.24 (95% CI were not given). 26,27 An approximate healthy vaccinee effect-adjusted MMRRs (adMMRRs) or adjusted SMR (adSMR) were yielded by dividing MMRRs or SMR by 0.10 to 0.24 respectively without 95% CI.
The valid reasons for comparing myocarditis mortality rate of vaccinee with onset within 28 days from the last dose and of the reference population are based on the following. In the reference population, death cases in which signs and symptoms of myocarditis leading to death develop during the observation period (From the beginning through the end of the year) and die after the observation period are not included in the mortality calculation, whereas cases that develop before the observation period and die during the observation period are included in the mortality calculation (Fig S1a).
In the post-vaccination population, on the other hand, a case in which signs and symptoms of myocarditis leading to death had already developed before vaccination would have never been reported as a death case possibly or probably associated with vaccine and is never included in the mortality analysis. Hence, cases in which signs and symptoms of myocarditis leading to death develop during the observation period should be included in the mortality analysis among vaccinated population for fair comparison with the reference population (Fig S1b).
Using the same method, number of all-cause deaths in the post-vaccinated population was calculated and compared with the expected number of deaths from all-cause.
All statistical analyses were performed with Stats Direct (Version 3.3.5). The significance level was set at P<0.05. Statistical multiplicity was not tested because this is rather an exploratory study but not a hypothesis confirming study.
Ethical approval was not obtained for this study because it was based on the disclosed data and is not required to obtain ethics approval under Japanese law and guidelines.
Patient and Public involvement
Patients and public were not involved in the design, analyses, in this study because the research agenda was urgent.
RESULTS
The number of included death cases for analysis is 1 362 including 38 myocarditis death and their characteristics are shown in Table 1.
Characteristics of included death cases after receiving SARS-CoV-2 vaccine. *a
Persons who died from myocarditis death were younger, used more mRNA-1273 and occurred more after the second dose than those from other causes after SARS-CoV-2 vaccination. Myocarditis was diagnosed by autopsy and/or myocardial biopsy in half cases.
Table 2 shows the number of vaccinated persons by age and the person-years of observation calculated from them. Table 3 shows the population, causes of death, and their crude mortality rates for 2017-2019, used as reference. Details for each year are shown in the Table S3.
Myocarditis mortality in SARS-CoV-2 vaccinated population compared with reference population
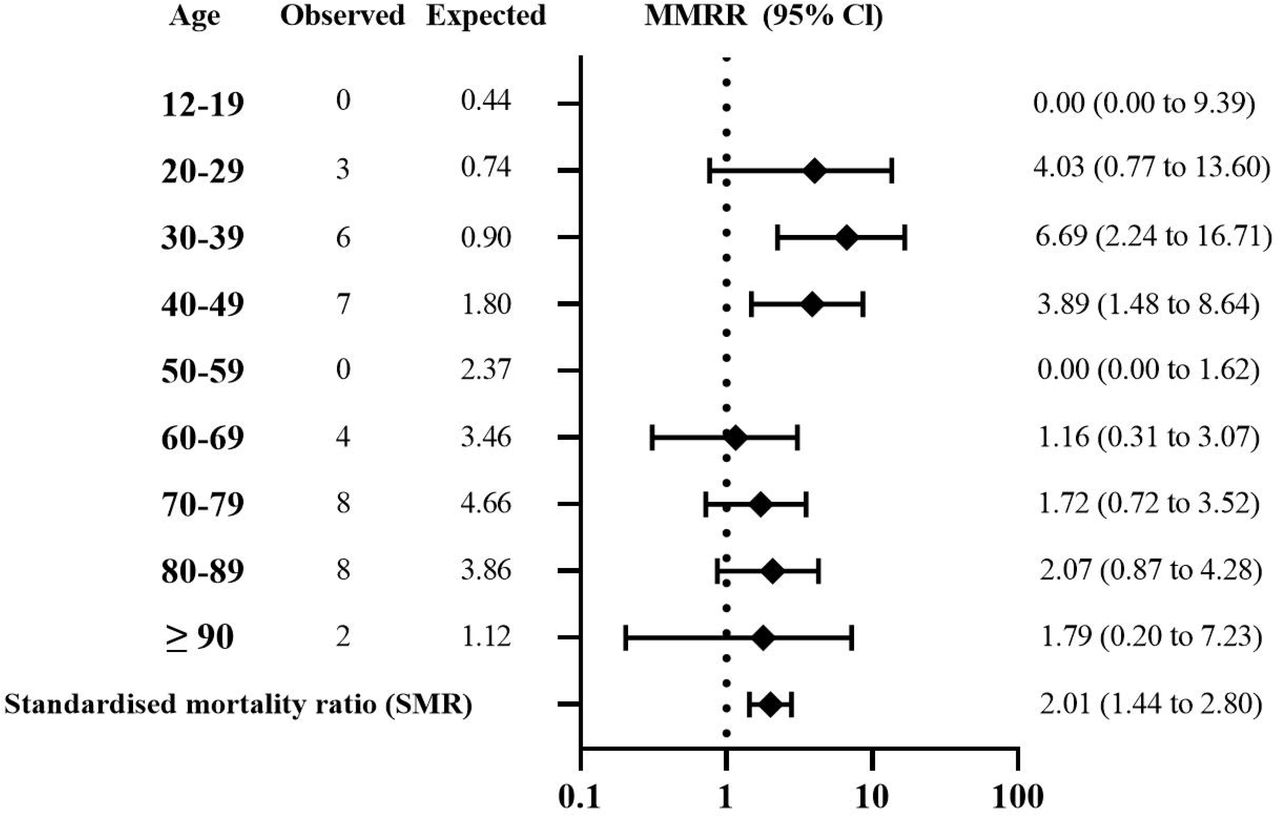
MMRRs and their (95%CI) after receiving SARS-CoV-2 vaccine were as follows: 4.03 (0.77 to 13.60) in 20s, 6.69 (2.24 to 16.71) in 30s, and 3.89 (1.48 to 8.64) in 40s. Except 10s and 50s in which myocarditis death was zero, each point estimates of the MMRR exceeded 1.0. SMR of myocarditis was 2.01 (1.44 to 2.80) for overall vaccinated population, 1.63 (0.95 to 2.78) after the first dose and 2.21 (1.45 to 3.37) after the second dose. Details were shown in Fig 2 and Table 4. SMR of myocarditis in those aged 12-39, 40-59 and the elderly overall (60 years or older) was 4.06 (2.02 to 8.18), 1.83 (0.85 to 3.93) and 1.65 (1.07 to 2.55) respectively.

{kind=link}
{kind=link}
All-cause mortality in SARS-CoV-2 vaccinated population
The apparent rate ratios for all-cause death after receiving SARS-CoV-2 vaccine were shown in Table S4. The apparent SMR for all-cause mortality was 0.01.
Mortality odds ratio for myocarditis
Age-stratified and pooled MORs for myocarditis death after receiving SARS-CoV-2 vaccine were shown in Table S5. Except 10s and 50s in which reported myocarditis death were zero, point estimates MORs for myocarditis were above 60. The pooled MOR (95% CI) for myocarditis death was 205.60 (135.52 to 311.94).
Healthy vaccinee effect adjusted MMRRs
Estimated point adMMRRs were approximately 17 to 39 in 20s, 28 to 64 in 30s, 16 to 37 in 40s, 5 to 11 in 60s, more than 7 in 70s or older and adSMR was 9 to 19 in overall vaccinated population (95%CI were not calculated).
DISCUSSION
Principal findings
Using the disclosed data by the Japanese government, we observed increased myocarditis mortality rate ratio in the SARS-CoV-2 vaccinated population compared with general population during three years pre-COVID-19 pandemic era, especially in young adults (MMRR: 6.69 in 30s). However, not only in young adults, but also in the middle aged (40s) and in the elderly and overall vaccinated, increased risk of myocarditis death is associated with vaccination even without consideration of healthy vaccinee effect. The pooled MOR for myocarditis death was as high as 205.6. Very rough estimation of healthy vaccinee effect adjusted MMRRs showed as high as 28 to 64 in 30s and about 9 to 19 for adSMR which were closer to pooled MOR. Increased risk was higher after the second dose than the first dose as shown in previous epidemiologic studies focusing on hospitalised myocarditis patients.14-18
Strengths of our study
This study has several strengths. First this is the first epidemiological study that show the increased risk of myocarditis mortality after the SARS-CoV-2 vaccination. Previous epidemiological studies which reported the increased risk of myocarditis did not report the increased death from myocarditis 14-18 with emphasis that most cases were mild,14,16 that deaths were rare with no deaths of persons younger than 40 years 17 and that one person died with fulminant myocarditis in the nationwide Israeli study.14
One of the most important reasons for such disregard of fatal myocarditis may be due to the differences in the population investigated between the present study and previous comparative epidemiological studies. The largest vaccinated populations involved among the previous studies are up to about 18 million vaccinees from England 18 and Nordic 4 countries.17 Both populations are less than one-fifth of vaccinee population of this study (about 100 million).
Mortality rate from myocarditis in England and Wales in 2017 to 2019 is about 30% lower than that in Japan stratified by 10-year age group (relative risk: 0.71, 95%CI: 0.54 to 0.94, P=0.018, by random effect, I2=43 %) by our calculation. From these data, expected myocardial death in Patone’s vaccinee population in England is estimated at approximately 2.0 without vaccination.18 Hence it may be very difficult to detect increased mortality, if vaccine is associated with increased risk of myocarditis death. Moreover, it is difficult to assess risk of death by self-controlled case series method that Patone et al 18 used. It is also reasonable that there were no deaths among cases for patients younger than 40 years in Karlstad’s study17 and that one person died with fulminant myocarditis in the nationwide Israeli study.14
Second, we showed that increased risk of myocarditis death was seen in all age groups even without consideration of healthy vaccinee effect.
Third, we pointed out that if healthy vaccinee effect is considered, the risk of SARS-CoV-2 vaccine on myocarditis death may be much higher, with rate ratio up to 28 to 64 in 30s.
Fourth in addition, we showed that pooled MOR is extremely high although it is assumed that reports of cases with myocarditis after SARS-CoV-2 vaccine may be enhanced because it was widely reported in the media.
Fifth these results show that myocarditis mortality is increased in vaccinated persons and provide important insights into the consideration of benefits and harms of the SARS-CoV-2 vaccine.
Limitations of this study
This study has several limitations. First, diagnosis of myocarditis death after SARS-CoV-2 vaccine is based on the physician’s diagnosis and is not based on exactly the newly proposed Brighton’s case definition.37 However, 50 % of myocarditis cases were diagnosed by autopsy and/or myocardial biopsy. They are exactly the level 1 myocarditis (definite case) by the Brighton’s case definition. Including above definite cases, almost 90% of cases were diagnosed at least blood test and/or ECG and/or UCG. Cases based on symptoms only or unknown methods were 11%. Moreover, diagnostic base of the myocarditis death in the reference general population in 2017 through 2019 is not known and is also based on physician’s diagnosis. Previous studies 14-18 supported a high incidence of post-SARS-CoV-2 vaccination myocarditis, making it difficult to believe that diagnostic accuracy is a factor in overestimating myocarditis mortality after vaccination.
Second, because myocarditis after SARS-CoV-2 vaccine received media attention, it is likely that physicians paid more attention and reported more. It might be one of the reasons for extremely high pooled MOR for myocarditis death. However, this may be resulted from underreporting of death from other causes, because not all deaths after SARS-CoV-2 vaccine were reported. There is no obligation to report all post-vaccination deaths, therefore only those cases where a physician suspected association to vaccination are reported and disclose by the MHLW. In the United States (US), 610 million doses of the SARS-CoV-2 vaccine had been administered until 31 August 2022, and about 16 000 post-vaccination deaths had been reported, 38 while in Japan, only about 1 500 post SARS-CoV-2 vaccination deaths had been disclosed against 200 million doses of the vaccine until 14 February 2022. If post-vaccination deaths were reported on a par with the US, this could be about 3.5 times higher. The apparent SMR for all-cause deaths were as low as 0.01. It is far lower than those estimated by other data. For example, randomized control trials have shown that the SARS-CoV-2 vaccine was not effective in reducing all-cause death.39,40 The results of analysis 26,41 using data from UK statistics 42 showed that age adjusted non-COVID-19 mortality rate in the ever vaccinated compared with that in the general population was estimated at 0.61 in January 2021. These results indicate that there was substantial underreporting of SARS-CoV-2 post-vaccination deaths. Mevorach revealed that the risk of myocarditis morbidity after vaccination was highest among second-time vaccinators aged 16-19 years.14 On the other hand, Japan’s MHLW database had not yet listed any myocarditis deaths between the ages of 12 and 19 years. Subsequently, vaccination of people aged 5-11 years began in Japan, and as of 5 August 2022, one person had died from myocarditis.43
Third, SMR was only adjusted for age, MMRRs and SMRs were not adjusted for sex and for other cofounding factors such as calendar period, health care worker status, nursing home resident, and comorbidities that Husby et al 16 and/or Karlstad et al 17 adjusted. However, proportion of male among patients died from myocarditis (65.8%) was not statistically significant as compared with that among reference 3-year population (59.0%). Mevorah 14 discussed that although selection bias in their study was possible, they considered it unlikely, since they used data from the entire nation. At the end of the study period, proportion of vaccinated at least one dose was 59.0 % on 31 May 2021 for their study 14, 75.3 % on 7 Oct 2021 for Danish study 16 and 76.3 % on 15 December 2021 for UK study 18, while it was 81.6 % on 14 Feb 2022 in our study according to the Data on COVID-19 by Our World in Data 44 and 89.6 % among the age of 12 years or older (the vaccine-indicated population) in Japan.
Mevorah et al 14 reported similar results as those adjusted for potential confounders other than age and sex, although they were unable to adjust for them. Moreover, according to the results of Mevorah’s data analysis by us, most “adjusted” incidence rate ratios were higher than the “crude” rate ratios. Hence, only adjustment for age and not for other potential cofounders may not affect the results.
Forth, we could not compare relative risk among products, BNT162b2 (Pfizer-Biotech) or mRNA-1273 (Moderna), because precise data for number of persons who received each product by age group until the cut off day (14 February 2022) were not disclosed. However, according to the analysis by National Institute of infectious diseases, 45 proportion of reports for myocarditis among male 10s and 20s who received second dose of mRNA-1273 was 102.1 and 47.2 /million person respectively, while 15.4 and 10.0 /million person for second dose of BNT162b2. If the distribution of number of persons who received each product by age group at the cut off day (14 February 2022) were the same as reported on 3 December 2021, mortality rate ratio from myocarditis among those who were younger than 40 years and received mRNA-1273 compared with those who received BNT162b2 show no significant increase: 3.12 (95%CI: 0.84 to 11.63, P=0.073), while it was not significant among those 40 years or older.
Fifth, we have no evidence on healthy vaccinee effect of SARS-CoV-2 vaccine in Japan. However, there are more than one evidence that indicates healthy vaccinee effect of SARS-CoV-2 vaccine in the world. One 26,41 is the results of analysis using data from UK statistics 42 and the other 27,41 is the results of analysis using the published data in the peer review journal.46,47
According to the former analysis, COVID-19-related mortality rate ratio (MRR) of those who died 21 days or more after the second dose to the unvaccinated was 0.02 at the beginning of the immunization program in UK (January 2021), while the non-COVID-19 MRR of those who died 21 days or more after the second dose to the unvaccinated was 0.11 (95%CI: 0.08 to 0.14) for January 2021 and 0.13 (0.10 to 0.17) for February 2021. These indicate that healthy vaccinee effect may work to lower the apparent risk of death from COVID-19 and may increase the apparent effectiveness of SARS-CoV-2 vaccine. Dividing the COVID-19-related MRR of 0.02 by the non-COVID-19 MRR of 0.11, yields a healthy vaccinee effect-adjusted COVID-19-related MRR of 0.18 (95%CI: 0.09 to 0.37). This may be considered to be closer to the true COVID-19-related MRR.26
Under similar conditions to this study, the healthy vaccinee effects estimated using UK statistics are as follows. Healthy vaccinee effect by SARS-CoV-2 vaccination expressed as MRR in ever vaccinated to expected mortality rate for 2021 assuming that COVID-19 is not epidemic in England and Wales (932.1/100 000 person years) was estimated 0.61 in January 2021 and 0.10 to 0.24 at the day of vaccination, by applying the analysis results 27 using data from Israeli study, 46 as shown in the following another evidence.
The analysis results show that odds ratio (OR) of symptomatic COVID-19 on day 1 of vaccination was 0.40 (95%CI: 0.31 to 0.51) and ORs of hospitalisation, severe COVID-19 and death due to COVID-19 on day 1 are roughly estimated as 0.27, 0.18 and 0.13 respectively (95%CI was not calculated).27 Vaccination can never work at the day of vaccination; these low risk of mortality and morbidity is highly probably derived from the fact that the vaccinated people were much healthier than the unvaccinated. This bias could not be adjusted by ordinary methods for matching by adjusting age, sex, sector, and residence, history of influenza vaccination, pregnancy and total number of coexisting risk factors that Dagan et al used.
Theoretical basis of healthy vaccinee effect is shown by Fine et al. 48 Jackson et al 49 reported that the relative risk of death, hospitalisation due to pneumonia and ischemic heart disease for influenza vaccinated persons compared with unvaccinated persons was 0.36 (95%CI: 0.30 to 0.44), 0.65 (0.53 to 0.80) and 0.92 (0.83 to 1.02) before influenza season respectively in the United States. They concluded that the reductions in risk before influenza season indicate preferential receipt of vaccine by relatively healthy seniors and adjustment for diagnosis code variables did not control for this bias just as in the Dagan’s study. 46
These results indicate that the more serious the disease, the lower the apparent risk of vaccination and are consistent with the results of analysis 27 on Dagan’s data. 46
In fact, Husby et al 16 mentioned the fact that SARS-CoV-2 vaccines are rarely given to people with an acute or terminal illness as a likely explanation of low 28-day risk of cardiac arrest or death in their study. This explanation is exactly the “healthy vaccinee effect”.
Considering these, healthy vaccinee effect works in the direction of positive for vaccination (more effective and safer) universally on observational studies even if many variables were matched and/or adjusted by the ordinary methods used in most observational studies including propensity score matching. Hence, it may be rational to take the health vaccinee effect into account in the present study. Because death is a rare event, the extent of the healthy vaccinee effect on death which were estimated using previously disclosed data showed wide range (0.10 to 0.24). If the least healthy vaccinee effect (the highest MRR: 0.24) is used, risk of SARS-CoV-2 vaccine on myocarditis death is estimated about 4 times higher than those without adjustment.
Lastly, this study is rather an exploratory study but not a hypothesis confirming study. However, we found several strong associations especially in the age of 30s without adjustment for healthy-vaccinee effect and that very high MMRR were estimated if they were adjusted for healthy-vaccinee effect. Moreover, we got very high age-stratified and pooled mortality odds ratio for myocarditis death. Hence, we discuss the causal inference on the increased myocarditis mortality and SARS-CoV-2 vaccine use primarily according to the modified criteria of US Advisory Committee to the Surgeon General 50 (modified US Surgeon General criteria) with some supplementary discussion using viewpoints of causation by Hill 51 (Hill’s viewpoints) (Table S6). Because “specificity of association” both in US Surgeon General criteria and Hill’s viewpoints is an extreme type of “strength of association”, we included it into “strength of association” and classified into 4 criteria: (1) temporarily, (2) consistency, (3) strength and (4) coherence of association.
We found all 4 criteria were satisfied and we conclude that the association of high myocarditis mortality rate ratio after SARS-CoV-2 vaccination may be causal.
Points to be clarified in future research
Post-vaccination death should be more precisely investigated, not only from myocarditis but also from other causes. These should be closely monitored by nation-wide investigation as done in England and Wales or in the country with larger population. In these investigations, “healthy vaccinee effect” must be taken into account.
Conclusions and policy implications
Despite above limitations, this study revealed that SARS-CoV-2 vaccination was associated with higher mortality rate from myocarditis, especially in young adults compared with 2017 to 2019 population. But it also revealed that myocarditis death occurs in older persons. If healthy-vaccinee effect is taken into account, the risk increases at least approximately 4 times more than the unadjusted mortality risk. In addition, underreporting deaths after receiving vaccine should be considered. Based on the results of this study, it is necessary to inform public about that the risk of serious myocarditis including death may be far more serious than the risk reported before and that it occurs not only in young persons but also in elderly.
Data Availability
All data produced in the present study are available upon reasonable request to the authors.
Footnotes
COMPETING INTERESTS: All authors have completed the ICMJE uniform disclose form available at https://www.icmje.org/disclosure-of-interest/, RH wrote a book entitled “Drugs to avoid, and infectious diseases including COVID-19” published on 1 December 2020.
FUNDING This survey does not receive any financial support from businesses or public institutions.
ETHICAL APPROVAL This study was conducted based only on data disclosed by the Japanese government. Japanese law and guidelines do not require an ethical approval for such research.
DISCLAIMER The content is the personal view of the author and is not related to the official view of the authors’ organization.
References



