
Abstract
Background Sugar sweetened beverages (SSBs) are the primary source of dietary added sugars in children, with high consumption commonly observed in more deprived areas where obesity prevalence is also highest. Associations between SSB consumption and obesity in children have been widely reported. In March 2016, a two-tier soft drinks industry levy (SDIL) on drinks manufacturers to encourage reformulation of SSBs in the UK was announced, and then implemented in April 2018. We examined trajectories in the prevalence of obesity at ages 4-5 years and 10-11 years, 19 months after the implementation of SDIL, overall and by sex and deprivation.
Methods and Findings Data were from the National Child Measurement Programme and included annual repeat cross-sectional measurement of over one million children aged 4-5 and 10-11 years in state-maintained primary schools. Interrupted time series analysis of monthly obesity prevalence data from September 2013 to November 2019 was used to estimate absolute and relative changes in obesity prevalence compared to a counterfactual (adjusted for temporal variations in obesity prevalence) estimated from the trend prior to SDIL announcement. Differences between observed and counterfactual estimates were examined in November 2019 by age (4-5 or 10-11 years) and additionally by sex and deprivation quintile. In 10-11 year old children there was an overall absolute reduction in obesity prevalence (defined as >95th centile on the UK90 growth charts) of 0.8% (95%CI: 0.3, 1.3). In 10-11 year old girls the reduction was 1.6% (95%CI: 1.1, 2.1), with greatest reductions in the two most deprived quintiles (e.g. there was an absolute reduction of 2.4% (95%CI: 1.6, 3.2) in prevalence of obesity in the most deprived quintile). In 10-11 year old boys, there was no change in obesity prevalence, except in the least deprived quintile where there was a 1.6% (95%CI: 0.7,2.5) absolute increase. In 4-5 year old children, relative to the counterfactual, there were overall increases in obesity prevalence in both genders (combined) and all deprivation quintiles except the most deprived where there was no change.
Conclusions Our results suggest the SDIL was associated with decreased prevalence of obesity in 10-11 year old girls, with the greatest effects in those living in the most deprived areas. Additional strategies beyond SSB taxation will be needed to reduce obesity prevalence overall, and particularly in older boys and younger children.
Trial registration ISRCTN18042742
Introduction
There is strong evidence that consumption of sugar sweetened beverages (SSBs) increases the risk of serious diseases including type II diabetes, cardiovascular disease, dental caries and obesity[1–3]. SSBs are the primary source of free-sugar in the diets of children and are associated with weight gain, obesity and fatness in children [4–6] with consumption highest in older ages and those from lower socioeconomic groups[11]. In England 26% of children in their last year of primary school were recorded as living with obesity in 2020/2021, with those living in the most deprived areas being twice as likely to have obesity than those from the least deprived areas[8]. Recently born cohorts of children are much more likely to have obesity than children from older cohorts such that ten year-olds born after the 1980s are 2-3 times more likely to develop obesity than those born before the 1980s[9]. The persistence of obesity from childhood into adulthood [10] and its acute and chronic negative physical [11–14] and mental [11,15] health consequences in children has led to governments around the world focusing on preventative strategies to reduce obesity in early life.
The UK government has proposed a number of strategies to reduce prevalence of obesity in childhood [16], including a soft drinks industry levy (SDIL) on manufacturers, importers and bottlers of SSBs. This is in alignment with the World Health Organization recommendation of taxes on SSBs to reduce consumption of added-sugars to improve health[17]. The two-tier SDIL (announced in March 2016 and implemented in April 2018) was designed to incentivise reformulation of soft drinks and included a charge of £0.24/litre on soft drinks containing ≥ 8g of sugar per 100ml, £0.18/litre on soft drinks containing between ≥ 5 to <8g of sugar per 100 ml and no levy on drinks containing <5g sugar per 100ml[18]. Levy exempt drinks include milk, milk-based drinks, 100% fruit juice and powders used to make drinks. As part of the broader health strategy for young people, the UK government indicated they would use revenues raised through the SDIL to fund physical education in schools and breakfast and after-school clubs[19].
Evidence suggests that the UK SDIL led to substantial reformulation of the UK soft drinks market[20] and an overall reduction in sugar purchased from soft drinks[21]. A number of modelling studies [22–25] have predicted that the introduction of SSB taxes would lead to a modest reduction in obesity in children and adults at the population level, but no study to date has used empirical data to examine whether the response of the SSB industry to the UK SDIL was associated with a subsequent change in the prevalence of childhood obesity. A few studies have used empirical data to estimate associations between SSB taxes and weight-related outcomes in children and adolescents and have either shown no association [26,27] or small to modest effects in specific subgroups such as low-income households [28] or in adolescent girls but not boys[29]. Differences in these findings may also be related to reliance on subjective measures of self-reported weight, minimal increases in prices of SSB (<5%) or possible substitutions to higher calorie untaxed drinks[27].
In this study we use cross-sectional data on monthly prevalence of objectively assessed obesity in children when they enter (reception class; ages 4/5) and exit (year 6; ages 10/11) English primary schools to examine whether 19 months following the implementation of the UK SDIL there were changes in the trajectory of prevalence of obesity 1) overall and 2) by sex and deprivation.
Methods
Data source
We used data from the National Child Measurement Programme (NCMP). This surveillance programme began in 2006 and measures the height and weight of approximately one million children from English state-maintained primary schools in reception (ages 4/5 years) and year 6 (ages 10/11 years) annually, with the aim of monitoring national rates of overweight and obesity in children. Local authorities oversee the data collection and letters are sent to the parents of eligible children where they are informed about why the data is collected and how it is stored. There is also an opportunity to opt out of measurement. Approximately 99% of eligible schools (∼ 17,000 schools) take part each year and individual response rates are high with ∼ 95% of eligible pupils taking part[30].
Surveillance data provided by NCMP includes prevalence of children with overweight or obesity by school class (reception or year 6), sex (male or female), school year (e.g. 2013/14), month of measurement (August is excluded), and the index of multiple deprivation (IMD) quintile of the primary school location which the child attends. IMD scores are commonly used in England as measures of multiple deprivation by considering seven distinct domains including income, employment, education, barriers to housing, health and disability, crime and living environment[31]. The body mass index thresholds used to derive overweight and obesity prevalence values were based on the 85th and 95th centiles, respectively, of a reference sample of measures taken in the UK in 1990 taking account of height, weight, sex and age, reflecting the definitions used by Public Health England for population surveillance [32]. The study period was initially planned to end two years following the implementation of SDIL but follow-up was curtailed in November 2019 (4 months prior to the proposed end date) to avoid any influence of potential household storing of food and drink in preparation of: i) the UK leaving the European Union (December 2019) and ii) national lockdown because of the COVID-19 pandemic (March 2020)[33] to avoid contamination with documented changes in weight status occurring in the pandemic[34].
Statistical analysis
Interrupted time series (ITS) analyses were conducted to assess obesity prevalence in relation to the UK SDIL in children attending primary school reception or year 6 classes, overall and by sex and index of multiple deprivation (IMD) quintile. The ITS used monthly data from September 2013 (study month 1) until November 2019 (study month 69), including the months of the SDIL announcement (March 2016; study month 29) and implementation (April 2018; study month 52).
Generalised least squares models were used. Autocorrelation in the time series was examined visually using plots of autocorrelation and partial-autocorrelation and statistically using Durbin-Watson tests; an autocorrelation-moving average (ARIMA) correlation structure was used, with the order (p) and moving average (q) parameters chosen to minimise the Akaike Information Criterion (AIC) in each model. Since seasonal factors such as school holidays are reported to influence weight-related outcomes in school children, models included adjustment for months that showed significant changes in obesity prevalence (September, October, June and February for reception class and September and July for year 6)[35]. Counterfactual scenarios were estimated based on pre-announcement trends (figure S1). Absolute and relative differences in prevalence of obesity between observed and counterfactual values were estimated at month 69 (November 2019). Confidence intervals were calculated from standard errors estimated using the delta method [36]. All statistical analyses were performed in R version 4.1.0.
Sensitivity Analysis 1: Inclusion of two alternative interruption points
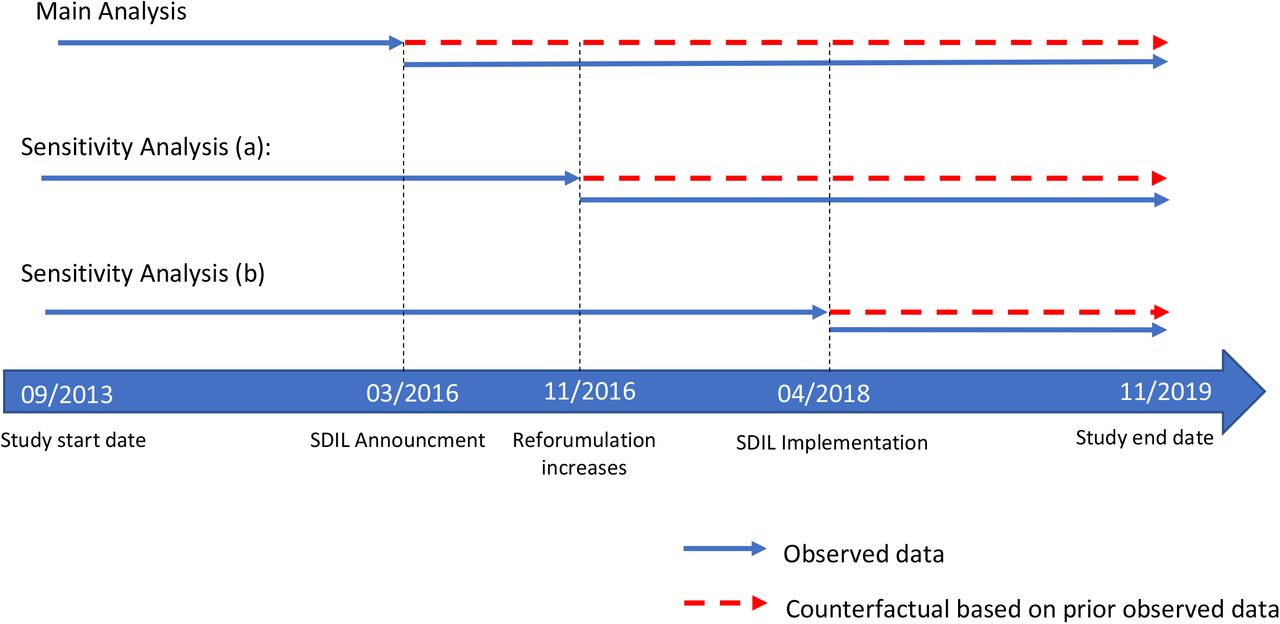
The main analysis included a counterfactual based on the pre-announcement trend (i.e. a scenario where neither the announcement or implementation happened); however, previous research suggests that reformulation of drinks began some months after the announcement of SDIL but before implementation [20]. Therefore, as well as capturing the earliest possible time when reformulation could come into effect, in sensitivity analyses (figure S1) we used two alternative interruption points. First (sensitivity analysis 1a), we used a counterfactual based on the trend from September 2013 to November 2016 (equivalent to 8 months post-announcement and the point at which reformulation increased rapidly)[20]). Second (sensitivity analysis 1b) we used a counterfactual based on the pre-implementation trend, i.e. from September 2013 to April 2018.
Sensitivity Analysis 2: Combining overweight and obesity prevalence
In addition to examining prevalence of obesity, the main analysis was repeated and broadened to examine trajectories of excess weight prevalence, in relation to the SDIL, using monthly measures of overweight in addition to obesity.
Results
Table 1 summarises the mean obesity prevalence in the study period (i) before the SDIL announcement and (ii) after the SDIL announcement, in primary school children in reception and year 6, overall and by sex and IMD quintile. Highest levels of obesity were observed in the most deprived areas regardless of age and sex; pupils in schools from the most deprived IMD quintiles had nearly twice the prevalence of obesity as those in the least deprived IMD quintiles.
Mean obesity prevalence (standard deviation) in the pre and post announcement periods of the UK soft drinks industry levy, by school class, sex and IMD quintiles.
Changes in obesity prevalence in relation to SDIL
Unless stated otherwise below, all estimates of changes in prevalence of obesity are based on values from November 2019 with respect to the counterfactual scenario of no SDIL announcement or implementation having occurred.
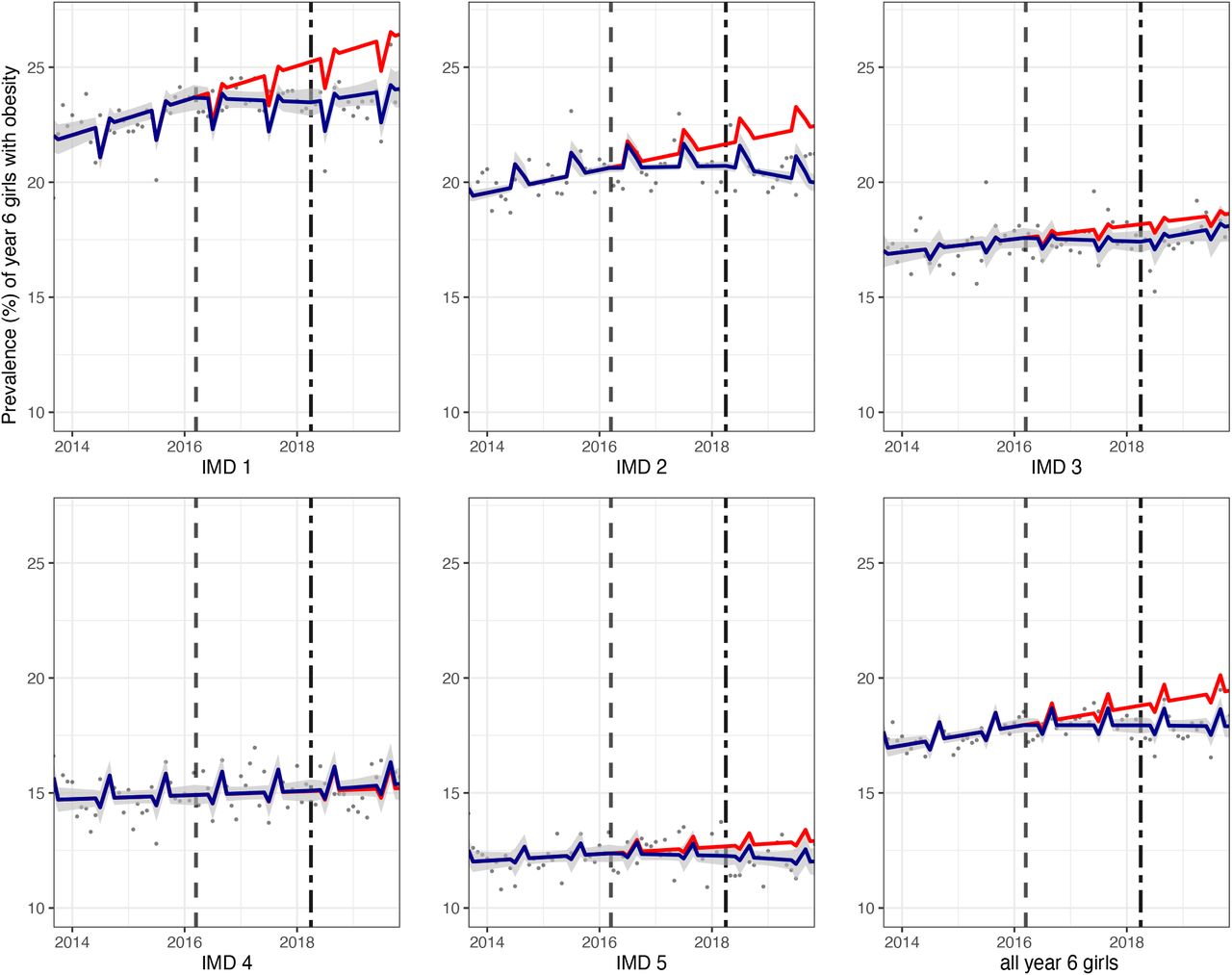
Across all year 6 children there was a 0.8% (95% CI: 0.3, 1.3) absolute reduction or 3.6% (95% CI:1.2, 5.9) relative reduction in obesity prevalence compared to the counterfactual (see Table 2). Year 6 children in schools from the most deprived IMD quintiles (IMD1 and 2) had the greatest (relative) reductions in obesity prevalence of 4.1% (95%CI:1.8, 6.3) and 5.5% (95%CI:3.3, 7.7), respectively; however large differences between year 6 girls and boys were observed. In year 6 girls, there was an overall relative reduction in obesity prevalence of 8.0% (95% CI: 5.4, 10.5) and analysis by IMD revealed greatest reductions in the two most deprived IMD quintiles 1 and 2, of 9.0% (95%CI: 5.9, 12.1) and 11.0% (95%CI:9.2, 12.7), respectively and in the least deprived IMD(5) quintile by 7.0% (95%CI: 2.3, 11.6) (figure 1). In year 6 boys there was no overall change in obesity prevalence and no obvious pattern in changes in prevalence by IMD quintile, although there was a large relative increase in obesity prevalence of 10.1% (95%CI: 4.3, 15.9) in the least deprived IMD quintile and a small reduction in prevalence of obesity in IMD2 of 3.30% (95% CI:0.4, 6.2) (figure 2).
Absolute and relative changes in prevalence of obesity (95% confidence intervals), compared to the counterfactual1, in reception and year 6 boys and girls, by Index of multiple deprivation at 19 months post-implementation of the UK soft drinks industry Levy

Prevalence (%) of obesity in year 6 girls between September 2013 and November 2019. Observed and modelled prevalence of obesity is shown by IMD quintile and overall. Dark blue points show observed data and dark blue lines (with grey shadows) shows modelled data (and 95% confidence intervals) of obesity prevalence. The red line indicates the counterfactual line based on the pre-SDIL announcement trend (assuming the announcement and implementation had not occurred). The first and second dashed vertical lines indicate the announcement and implementation of SDIL, respectively.

Prevalence (%) of obesity in year 6 boys between September 2013 and November 2019. Observed and modelled prevalence of obesity is shown by IMD quintile and overall. Dark blue points show observed data and dark blue lines (with grey shadows) shows modelled data (and 95% confidence intervals) of obesity prevalence. The red line indicates the counterfactual line based on the pre-SDIL announcement trend (assuming the announcement and implementation had not occurred. The first and second dashed vertical lines indicate the announcement and implementation of SDIL, respectively.
In reception children, compared to the counterfactual there was no overall change in obesity prevalence, but increases were observed in all IMD groups, except the most deprived (IMD1). Examination by IMD and sex showed a consistent increase in prevalence of obesity, compared to the counterfactual, in the least deprived IMD groups in both girls (figure 3) and boys (figure 4) in reception class.

Prevalence (%) of obesity in girls in reception class between September 2013 and November 2019. Observed and modelled prevalence of obesity is shown by IMD quintile and overall. Dark blue points show observed data and dark blue lines (with grey shadows) shows modelled data (and 95% confidence intervals) of obesity prevalence. The red line indicates the counterfactual line based on the pre-SDIL announcement trends (assuming the announcement and implementation had not occurred). The first and second dashed vertical lines indicate the announcement and implementation of SDIL, respectively.

Prevalence (%) of obesity in boys in reception class between September 2013 and November 2019. Observed and modelled prevalence of obesity is shown by IMD quintile and overall. Dark blue points show observed data and dark blue lines (with grey shadows) shows modelled data (and 95% confidence intervals) of obesity prevalence. The red line indicates the counterfactual line based on the pre-SDIL announcement trends (assuming the announcement and implementation had not occurred). The first and second dashed vertical lines indicate the announcement and implementation of SDIL, respectively.
When the interruption point was changed to December 2016 (8 months post SDIL-announcement, the point at which reformulation began, sensitivity analysis 1a), changes in obesity prevalence were consistent with the main findings, with reductions in obesity prevalence evident in year 6 children, specifically girls from schools in the most deprived areas (IMD 1 and 2), (Table S1) and increases in obesity prevalence in year 6 boys from the least deprived areas (IMD 4 and 5). When the interruption point was changed to April 2018 (month of SDIL implementation, sensitivity analysis 1b, Table S2) findings varied from the main analysis, with an overall absolute increase in the prevalence of obesity in reception age children by 0.7% (95%CI: 0.1,1.3). Compared to the counterfactual, there were few significant changes in obesity prevalence in the different year 6 groups, although reductions (e.g.3.8% (95%CI 5.7, 2.0) in year 6 girls from IMD 2) and increases (e.g.3.8% (95%CI 0.2, 7.4) in boys in IMD4) were observed in some groups.
Absolute and relative changes in prevalence of obesity (95% confidence intervals), compared to a counterfactual scenario of eight months post-announcement, overall and by Index of multiple deprivation in reception and year 6 children, 19 months post-implementation of UK SDIL
Absolute and relative changes in prevalence of obesity (95% confidence intervals), compared to a counterfactual scenario based on pre-SDIL implementation trends, overall and by Index of multiple deprivation in reception and year 6 children, 19 months post-implementation of the UK SDIL
Changes in prevalence of excess weight (overweight or obesity) in relation to the UK SDIL were comparable to the main findings on changes in trends in prevalence of obesity, with greatest reductions in excess weight observed in girls from schools in IMD quintiles 1 and 2 and no change in prevalence of excess weight overall in year 6 boys or reception age children (Table S3). However, compared to the counterfactual scenario of no announcement or implementation, there was an observed absolute reduction in excess weight of reception age girls from the most deprived IMD(1) of 1.6% (95%CI 1.1, 2.1).
Absolute and relative changes in prevalence of excess weight (overweight or obesity) and 95% confidence intervals, compared to the counterfactual*, in year 6 boys and girls, by Index of multiple deprivation at 19 months post-implementation of the UK soft drinks industry Levy
Discussion
This is the first study that we are aware of that uses empirical data to examine changes in childhood obesity prevalence in England in relation to the UK SDIL. After accounting for prior trends in obesity, there was a 0.8% absolute reduction of year 6 children living with obesity, 19 months after the implementation of the SDIL. These reductions in year 6 children were predominantly driven by changes in girls, where there was a 1.6% absolute or 8.0% relative reduction in obesity prevalence. Assuming, based on our 2019 data, that there are 337, 658 year 6 girls in England (of whom 18.4% have obesity), this reduction is equivalent to 5,234 averted cases of obesity in year 6 girls. Relative to the counterfactual no overall change was observed in year 6 boys. We observed that for year 6 girls, reductions in obesity were greatest in the 40% most deprived IMD areas, with a 2.4% absolute or 9.0% relative reduction in the most deprived IMD quintile. Overall, the prevalence of obesity in reception class children was unchanged, compared to the counterfactual.
Strengths and weaknesses
This study includes the use of a large on-going nationally representative sample covering ∼ 95% of children in reception and year 6 in state-run primary schools and measures of overweight and obesity in over one million school children annually. Obesity prevalence data was based on objective measures of height and weight rather than parental self-report, where there is a tendency to underestimate overweight [37]. The NCMP uses 85th and 95th centiles of the UK1990 growth reference to monitor overweight and obesity in children (accounting for age and sex), respectively[32,38]. However, other cut points are sometimes used [39] and there is some debate over whether this is the best measure of adiposity, particularly in younger children [40]
Parental consent in NCMP involves a selective opt-out, which is designed to increase participation rates. However, it has been suggested that girls with obesity are less likely to participate[41]. This may have led to an underestimation of the relative effect of SDIL on obesity prevalence in girls. These effects are, however, likely to be small given that obesity levels in girls have not changed dramatically and participation in the sample overall remained high throughout our study period. Socioeconomic disadvantage was assessed using an area-level indicator (IMD) of the school that each child attended, a less sensitive measure than capturing socioeconomic disadvantage at the household level. However, there is a strong correlation between school-level IMD and the proportion of pupils eligible for free school meals, a measure of the number of children attending a school with a low household income,[42] suggesting that the measure used here is a suitable proxy measure of household deprivation.
Data on time trends of expected childhood weight loss in relation to diet interventions is sparse with studies not monitoring weight-related outcomes with regularity and from early in the intervention. This makes it particularly challenging to estimate how long from the SDIL announcement we would expect to observe changes in obesity prevalence in children. However, there is evidence that changes in energy balance in children can lead to rapid changes in weight loss, for example, seasonal differences in BMI are observed in school children, with weight gain typically occurring during the summer periods especially in children with overweight or obesity[35].
The ITS approach used modelled counterfactuals on the obesity prevalence trends immediately prior to the SDIL announcement. Given that estimates of the overall difference between observed and counterfactual obesity prevalence can be sensitive to the time points at which the counterfactuals are modelled, as part of a sensitivity analysis, we included two extra interruption points. The first additional interruption was eight months post-announcement of SDIL, a time when reformulation of SSBs was visibly starting to increase; here we observed very similar findings to the main analysis indicating that they are robust. The second additional interruption was assigned to the date of the SDIL implementation; using this model we observed fewer significant changes in obesity prevalence compared to the counterfactual (for example no significant difference was observed in year 6 girls overall). This finding may be explained by the fact that companies had already reformulated most of their products prior to the implementation date and trajectories of obesity prevalence had responded rapidly. Furthermore, examining trajectories of “excess weight” prevalence rather than prevalence of obesity as the outcome of interest led to findings broadly consistent with the main analysis.
Comparison with other studies and interpretation of results
Alongside making comparisons with other studies, in this section we also discuss why we think the introduction of the SDIL is causally linked to the observed falls in obesity prevalence. In doing this we draw on the Bradford-Hill criteria [43].
First, our findings are plausible since associations between SSB consumption and risk of obesity are well described in the literature [4–6]. Furthermore, a relationship between the UK SDIL and an overall reduction in sugar purchased from soft drinks across the population has previously been reported [21] although it remains unclear whether this equates to any health advantages. Several modelling studies have also predicted that SSB taxes are likely to be most effective at targeting sugar intake in children and younger adults [44,45].
Second, the magnitude and pattern of associations in our results are consistent with recent findings from Mexico that report a modest reduction in overweight or obesity prevalence in adolescent girls (aged 10-18) with a 1.3% absolute decrease two years after a 10% SSB price increase (compared to a 1.6% absolute decrease observed in this study in 10-11 year old girls 19-months after the levy was introduced) [29]. Moreover, similar to the findings of this study, no significant reductions in weight-related outcomes were observed in adolescent boys in Mexico.
Third, we found that reductions in sugar intake in relation to the levy were greatest in children who were likely to be higher consumers of SSBs (e.g. older children and those from the most deprived areas)[7]. This suggests a possible dose-response gradient between consumption levels and effectiveness of the levy in reducing obesity. This also adds to the growing international evidence that SSB taxes may reduce inequalities in diet-related health outcomes. For example, some studies from other countries have shown that lower income households were more likely to reduce their purchases or intake of sugar from SSBs following introduction of SSB taxes[28,46,47] although this is not always the case [48–50].
In this study, we also demonstrate that the UK SDIL is not associated with a change in obesity prevalence in children in the first year of primary school. This result is congruous with findings from a cohort of British children showing that SSB consumption at ages 5 or 7 are not related to adiposity at age 9 years[51]. Added sugars from drinks make up 30% of all added sugars in the diet of young children (aged 1-3 years) but this increases to more than 50% by late adolescence[52]. The lower intake of sugars from soft drinks at very young ages may lower the potential of a tax on SSBs, making it harder to observe health effects at the population-level. Fruit juices, which are not included in the levy, are thought to contribute similar amounts of sugar in young children’s diets as SSBs and may explain why the levy alone is not sufficient to reduce weight related outcomes in reception age children. In addition to drinks, confectionery, biscuits and cakes are also important high added sugar items which are regularly consumed by young children and could be a target of additional obesity-reduction strategies [52].
While our findings on gender differences in obesity prevalence changes in relation to sugar taxes on SSBs are consistent with previous studies[29], it is unclear why the UK SDIL might affect obesity prevalence in girls and boys differently, especially since boys are higher consumers of SSBs[7]. One explanation is that there were factors (e.g. in food advertising and marketing) at work around the time of the announcement and implementation of the levy that worked against any effects of the SDIL on boys. There is evidence that soft drink manufacturers altered their marketing strategies in different ways in response to the SDIL including re-packaging and re-branding products [53]. Numerous studies have found that boys are often exposed to more food advertising content than girls [54–57], both through higher levels of TV viewing[57] and through the way in which adverts are framed. Physical activity is often used to promote junk food and boys, compared to girls, have been shown to be more likely to believe that energy dense junk foods depicted in adverts will boost physical performance[54] and thus they are more likely to choose energy-dense, nutrient-poor products following celebrity endorsements. There is also evidence that girls tend to make healthier choices when it comes to diet (e.g. consuming more fruit and vegetables and less energy dense foods) and other health behaviours (e.g. brushing teeth)[58]. One possibility for the observed differences between boys and girls may be that girls were more responsive to public health signalling arising from discussions around the SDIL or that they were more likely to choose drinks that had been reformulated to contain less sugar following the SDIL-announcement.
Even the strongest effect of the SDIL on the most levy-responsive groups (e.g. year 6 girls) reflected only a dampening of the rate of increase in obesity prevalence compared to the counterfactual rather than a reversal in trends. This highlights that alongside the SDIL, additional evidence-informed obesity-reduction strategies need to be in place to improve weight-related outcomes, especially in boys and younger children, as they enter primary school education.
Conclusion
The UK SDIL was proposed by the UK government to tackle childhood obesity. The pattern of findings of this study suggests that the SDIL can contribute to reducing obesity prevalence in older primary school children. The SDIL announcement and implementation was associated with an overall relative decrease in obesity prevalence in girls aged 10/11 years of approximately 8% compared to the counterfactual scenario based on pre-announcement trends. These effects were even greater in girls from schools in the 40% most deprived areas, suggesting the SDIL could help to reduce inequalities in child obesity. Further obesity-reduction policies are needed alongside taxes on SSBs to improve and reverse the current obesity prevalence in children.
Supplementary

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Schematic diagram of the interrupted time series. Blue solid lines indicate observed data. Dashed red lines represent counterfactuals. Counterfactual for 1)main analysis based on obesity prevalence trends from 09/2013 – 03/2016; 2)sensitivity analysis (a) based on obesity prevalence trends from 09/2013 – 12/2016 and 3)sensitivity analysis (b) based on obesity trends from 09/2013 – 04/2018.
References



