
Abstract
Importance While much of the attention on the COVID-19 pandemic was directed at the daily counts of cases and those with serious disease overwhelming health services, increasingly, reports have appeared of people who experience debilitating symptoms after the initial infection. This is popularly known as long COVID.
Objective To estimate by country and territory of the number of patients affected by long COVID in 2020 and 2021, the severity of their symptoms and expected pattern of recovery
Design We jointly analyzed ten ongoing cohort studies in ten countries for the occurrence of three major symptom clusters of long COVID among representative COVID cases. The defining symptoms of the three clusters (fatigue, cognitive problems, and shortness of breath) are explicitly mentioned in the WHO clinical case definition. For incidence of long COVID, we adopted the minimum duration after infection of three months from the WHO case definition. We pooled data from the contributing studies, two large medical record databases in the United States, and findings from 44 published studies using a Bayesian meta-regression tool. We separately estimated occurrence and pattern of recovery in patients with milder acute infections and those hospitalized. We estimated the incidence and prevalence of long COVID globally and by country in 2020 and 2021 as well as the severity-weighted prevalence using disability weights from the Global Burden of Disease study.
Results Analyses are based on detailed information for 1906 community infections and 10526 hospitalized patients from the ten collaborating cohorts, three of which included children. We added published data on 37262 community infections and 9540 hospitalized patients as well as ICD-coded medical record data concerning 1.3 million infections. Globally, in 2020 and 2021, 144.7 million (95% uncertainty interval [UI] 54.8–312.9) people suffered from any of the three symptom clusters of long COVID. This corresponds to 3.69% (1.38–7.96) of all infections. The fatigue, respiratory, and cognitive clusters occurred in 51.0% (16.9–92.4), 60.4% (18.9–89.1), and 35.4% (9.4–75.1) of long COVID cases, respectively. Those with milder acute COVID-19 cases had a quicker estimated recovery (median duration 3.99 months [IQR 3.84–4.20]) than those admitted for the acute infection (median duration 8.84 months [IQR 8.10–9.78]). At twelve months, 15.1% (10.3–21.1) continued to experience long COVID symptoms.
Conclusions and relevance The occurrence of debilitating ongoing symptoms of COVID-19 is common. Knowing how many people are affected, and for how long, is important to plan for rehabilitative services and support to return to social activities, places of learning, and the workplace when symptoms start to wane.
Question What are the extent and nature of the most common long COVID symptoms by country in 2020 and 2021?
Findings Globally, 144.7 million people experienced one or more of three symptom clusters (fatigue; cognitive problems; and ongoing respiratory problems) of long COVID three months after infection, in 2020 and 2021. Most cases arose from milder infections. At 12 months after infection, 15.1% of these cases had not yet recovered.
Meaning The substantial number of people with long COVID are in need of rehabilitative care and support to transition back into the workplace or education when symptoms start to wane.
Introduction
Much of the attention of disease surveillance of the coronavirus disease 2019 (COVID-19) pandemic has concentrated on the number of infections, the large number of cases requiring hospital care for severe infection, and those who have died from the disease. Less attention has been given to the quantification of those who continue to experience symptoms past the acute infection stage. Terms such as long COVID, COVID long haulers, brain fog, post-COVID-19 condition, or post-acute sequelae of COVID-19 have been used to describe a diverse array of ongoing symptoms. In October 2021, the World Health Organization released a clinical case definition for post-COVID-19 condition as symptoms that are present at three months after SARS-CoV-2 infection with a minimum duration of 2 months and cannot be explained by an alternative diagnosis.1–6 We will use the term long COVID in this paper.
Post-acute infection fatigue syndromes have been described for other viruses and bacteria.7–10 An ongoing low-grade inflammation has been postulated to cause these symptoms, but the pathology remains largely unknown and treatments are based on symptom relief.2,11,12 The impact on affected individuals is substantial, and special clinics dealing with patients of long COVID have arisen to respond to an increasing need for supportive and rehabilitative care.13–16
A meta-analysis of 45 follow-up studies of COVID patients, of which only three had a follow-up time greater than three months, found 84 long-term effects of COVID-19, with shortness of breath, fatigue, and sleep disorders or insomnia as the most common symptoms.17 Studies have most frequently just reported on individual symptoms or counts of symptoms but less on severity, overlap of symptoms and pattern of recovery.1,18–22
In this paper, we have collated the information on long COVID into three common clusters of symptoms largely based on joint analyses with custodians of follow-up studies after COVID-19 diagnosis in ten countries, supplemented by published data and medical record databases. From this pooled information on the occurrence of these three symptom clusters, their severity, and the limited information on duration, we derived estimates of incidence, prevalence, and severity-weighted prevalence for 204 countries and territories for the years 2020 and 2021.
This analysis complies with the Guidelines for Accurate and Transparent Health Estimates Reporting (GATHER).23 The full GATHER checklist is provided in eTable 1.
Methods
Incidence of SARS-CoV-2 infection
We derived estimates of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection from the IHME COVID model, a statistical Susceptible-Exposed-Infected-Removed (SEIR) compartmental model fit to data on daily reported deaths, hospitalizations, and infections; seroprevalence; and excess mortality data. Greater detail of the relevant aspects of this model and its data and assumptions is available in the Supplement eSection 3.24–26
Incidence of symptomatic infection
We took estimates of new, daily infections from this COVID model and assumed that long COVID only occurs in those with symptomatic infection. From a published review, we selected studies that estimated the proportion of asymptomatic infections in representative screened samples with antibody testing (Supplementary Appendix Data Inputs).27 We pooled the logit-transformed proportions of asymptomatic cases from six studies in a random effects meta-analysis (eFigure 5) and multiplied one minus the predicted proportion by infections to estimate the incidence of symptomatic infection.
Incidence and prevalence of long COVID
Case definition
We define the incidence of long COVID as newly onset or persisting symptoms three months after an acute episode of COVID-19 which impact daily functioning and were not preexisting symptoms before SARS-CoV-2 infection. This aligns with the WHO clinical case definition of post-COVID condition, their preferred term for long COVID.5
Input data
From the long list of persisting symptoms reported by a proportion of COVID-19 cases after the acute phase, we selected three major symptom clusters based on frequency and the ability to quantify their relative severity using health state descriptions and corresponding disability weights (DWs) from the Global Burden of Disease (GBD) study. GBD uses 236 health states and DWs to quantify the non-fatal consequences of diseases and injuries.28 Table 1 shows the health states, lay descriptions, and disability weights used for long COVID. The three symptom clusters were a) fatigue with bodily pains and/or symptoms of depression or anxiety; b) cognitive problems such as forgetfulness or difficulty in concentrating, commonly referred to as “brain fog”; and c) ongoing respiratory problems with shortness of breath and persistent cough as the main symptoms. We decided to distinguish between two severity levels for cognitive problems and three levels of severity for the ongoing respiratory symptoms. From here on, we refer to the “fatigue”, “respiratory”, and “cognitive” clusters.
Health states, lay descriptions, and disability weights used for the three symptom clusters of long COVID.
We conducted a systematic review of published papers on the long-term consequences of COVID-19 but found that no published study provided enough detail for our quantification purposes. From 7362 unique search hits and additions screened from a living systematic review29, we included 46 published articles from 44 studies that contain follow-up data of at least one defining symptom included in our defined symptom clusters (Supplementary Appendix Data Inputs). We used the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines;30 our PRISMA checklist is in the appendix (eSection 5), and the search protocol was registered with the International Prospective Register of Systematic Reviews (PROSPERO, CRD42020210101).31
Instead of relying on published reports only, we contacted study authors of published studies and ongoing COVID-19 follow-up studies that were registered at the ISRCTN registry.32 From 23 positive responses of 42 study authors contacted, ten were able to share symptom cluster data in time for inclusion in our study (Table 2). With researchers from the ten follow-up studies, we developed algorithms to define the three symptom clusters by severity level by choosing symptom questions and measures employed in each study that would most closely match the wording of the lay descriptions that were presented to respondents of the GBD DW surveys (Table 1). In the Supplement eSection 5, we present details of the algorithms for each of the included studies. We utilized the cohort data with explicit questions comparing current symptoms to those pre-COVID to adjust the remainder of the cohort data lacking pre-COVID comparisons (Table 2, Supplementary Appendix Data Inputs).
Follow-up studies of long COVID, their inclusion of community and/or hospitalized cases, sample size, follow-up period, comparison method, and reported symptoms
In addition, we received analyses from collaborators at the Veterans Affairs Health Administration and from PRA Health Sciences, a data collection of private health insurance plans, based on ICD codes for the primary symptoms belonging to the three symptom clusters of interest among COVID patients compared to matched non-COVID patients (Supplementary Appendix Data Inputs).33–35 ICD codes are provided in the Supplement eTable 4.
Modelled symptom cluster recovery patterns and proportions
We first undertook a meta-regression of studies with multiple follow-up measurements to determine the recovery pattern of symptoms. Given the relative scarcity of data, we assumed a similar pattern of recovery for all three symptom clusters. We used separate models for community cases and hospitalized cases using a Bayesian meta-regression tool, MR-BRT (meta-regression—Bayesian, regularized, trimmed), to pool the logit-transformed proportions of cases with any of the three symptom clusters by follow-up time since the end of the acute episode (eFigure 10).36,37 For community cases, we used data from the Zürich and Faroe studies supplemented with data derived from three published studies.18–20,38–40 With a dummy in the meta-regression, we adjusted the Cirulli, United Kingdom COVID Symptom Study (CSS), and United Kingdom COVID-19 Infection Survey (CIS) studies as proportions were reported for aggregates of many individual symptoms, rather than only the symptom clusters of our interest.18–20,40 For hospitalized cases, we used data from the COVID-19 Follow-up care paths and Long-term Outcomes Within the Dutch health care system (CO-FLOW), Sechenov StopCOVID, PronMed ICU, and the Zürich SARS-CoV-2 Cohort studies supplemented with data derived from two published studies in Switzerland and Spain, both adjusted as in the community cases duration model.38,41 The longest follow-up from these studies was 12 months in the Zürich, Co-FLOW and Sechenov studies. In both models, an exponential decline was assumed in the proportion of cases affected by long COVID. The coefficients on the rate of decline in these initial models were then entered as priors into the models that used all available follow-up data, described below.
Next, we used all the data in models of long COVID in community and hospitalized cases separately. We ran separate models for each of the three clusters and the overlap between clusters and adjusted their outputs proportionally to sum to the values of the models for any of the three clusters of long COVID (eFigures 11-15). We had too few data points to run separate models for ICU-admitted cases; in the hospital models for each symptom cluster, we used a dummy variable for those admitted to ICU in order to predict their proportions, with the coefficient informed by the observed relationship between ICU and non-ICU hospitalized data.33,35 We also included variables for sex, whether the data were from an administrative source, and indicator variables for individual symptoms reported in the published articles (cognitive dysfunction, shortness of breath, fatigue).
To estimate the severity distributions, we pooled data from cohorts that had enough detail to determine the two levels of severity of cognitive symptoms and the three levels of severity of ongoing respiratory problems using a random effects meta-analysis with a fixed effect on hospitalized data (eFigures 16–17).
Incidence, prevalence, and severity-weighted prevalence of long COVID
To estimate the incidence of long COVID, we first subtracted deceased patients from the incidence numbers of symptomatic COVID infection and then multiplied these surviving patients by the estimated proportions of cases with each symptom cluster at 3 months.42,43(p19),44–46 Daily incident cases of long COVID at three months post-infection were multiplied by the average duration, estimated separately for community cases and hospitalized cases. We then summed the prevalent days of long COVID for each of the symptom clusters and their overlap by level of severity where applicable across the years 2020 and 2021. Each of these was multiplied by the corresponding DW to get severity-weighted prevalence, equivalent to the GBD metric of years lived with disability (YLDs). For overlapping clusters, we assumed a multiplicative function to constrain the combined DW to a value between zero and one.47
We present uncertainty intervals (UIs) for all estimates based on the 25th and 975th values of the ordered 1000 draws of the posterior distributions.
Results
Globally within 2020 and 2021, of 3.92 billion (95% UI 3.77–4.05) infections with SARS-CoV-2 through the end of 2021, 3.7% (1.4–8.0) or 144.7 million (54.7–312.6) persons developed long COVID defined as experiencing one or more of the three symptom clusters three months after infection (Table 3). Of these, 130 million (42.1—301) had experienced mild to moderate acute infections in the community, 11.5 million (4.91—20.5) developed long COVID after severe disease needing hospitalization, and 3.03 million (0.892—7.48) after critical acute disease needing ICU care. We estimated that 6.17% (2.43– 13.31) of symptomatic SARS-CoV-2 infections who survived the acute episode developed long COVID. This proportion was greater in those who were admitted to intensive care units (ICU) (43.1% [22.6– 65.2]) and general hospital wards (27.5% [12.1–47.8]) than in those with less severe symptomatic infections in the community (5.68% [1.85–13.1]). Note that our estimate of the number of global infections is much higher than reported as diagnosed cases because excess deaths, infection-to-death ratios and seroprevalence surveys suggest many more cases must have occurred. We estimated a median duration of long COVID of 3.99 months (IQR 3.84–4.20) in community infections, while hospitalized cases were estimated to experience a longer median duration of 8.84 months (IQR 8.10– 9.78) (eFigure 10). The global prevalence of long COVID in 2020-2021 was 5.11 million (2.31–8.72) cases among more severe, hospitalized patients and 31.4 million (10.2–73.5) cases among those who had milder infections.
Incident and prevalent cases of long COVID by sex and severity of initial infection in 2020-2021, in millions.
The fatigue, respiratory, and cognitive clusters occurred in 51.0% (16.9–92.4), 60.4% (18.9–89.1), and 35.4% (9.4–75.1) cases of long COVID, respectively. In 38.4% (7.94–96.0) of long COVID cases, two or all three of the clusters overlapped (Figure 1).

Proportions of incident long COVID symptom clusters and their overlap in 2020 and 2021 globally
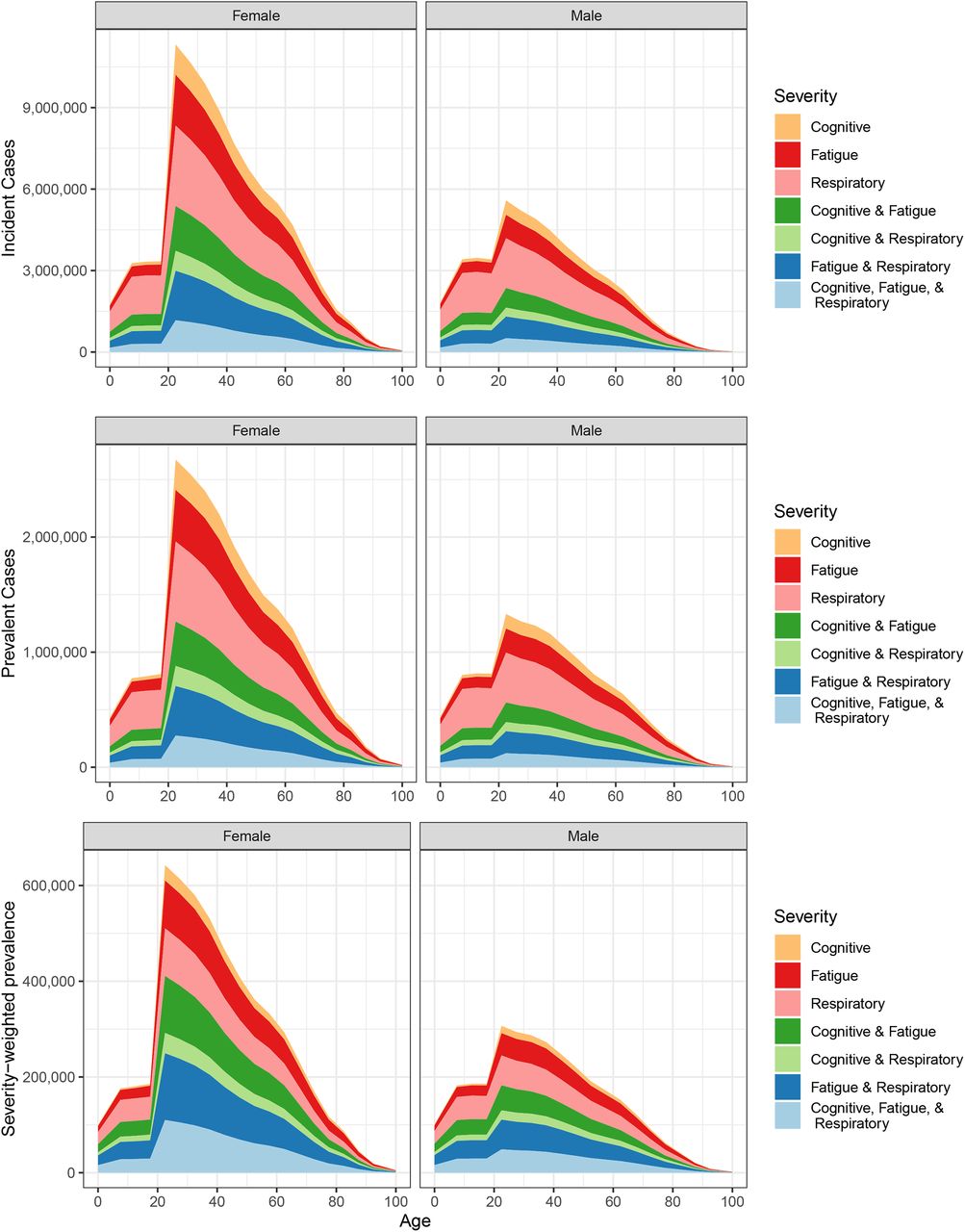
Globally, among prevalent long COVID cases, 63.2% (59.7–66.3) were female. The risk of long COVID at 3 months follow-up under the age of 20 was lower than in adults in milder community infections, 2.73% (0.808–6.65) in children versus 4.76% (1.53–11.3) in adult males and 9.88% (3.38–21.2) in adult females (eTable 15a). The peak ages of long COVID cases were between 20 and 29 (Figure 2).
{kind=link}
{kind=link}
Global incident cases, prevalent cases, and severity-weighted prevalence of long COVID by age, sex, symptom cluster, and overlap of symptom clusters in 2020 and 2021
The average level of disability among long COVID cases, estimated as the ratio of overall long COVID severity-weighted prevalence to prevalence, was 0.231 (0.134–0.370)—equivalent to the GBD DWs for severe neck pain, Crohn’s disease, or long-term consequences of moderately severe traumatic brain injury.28
The age and geographical pattern of incidence and prevalence of long COVID closely follows that of SARS-CoV-2 infections, as we assumed the same risk among survivors of acute infection, severity distributions, and duration in all locations. The counts of incident and prevalent cases of long COVID by country are provided in Table 4.
Incident and prevalent cases of long COVID by country, 2020 and 2021.
Among COVID patients who develop long COVID in 2020 and 2021, 15.1% (10.3–21.1) continued to have persistent symptoms at 12 months after COVID infection, or 21.0 million (9.19–41.7) people. In the United States, the Social Security Administration is mandated to financially assist those who are still unable to work after 12 months, corresponding to 946,000 (365,000—2,130,000) people aged 20-64 in the US in 2021 and 2022.
Discussion
A substantial proportion of COVID-19 patients do not recover after the initial infection. We estimated that 144.7 million (54.7–312.6) cases globally in 2020 and 2021 suffered from one or more of three common symptom clusters of long COVID. The risk of long COVID is greater in females and in those with more severe initial infection. The peak ages of those experiencing long COVID were between 20 and 29 years. This pattern by age and sex is distinct from that of severe acute infection, which affects more males and increases with age.48 From seventeen follow-up studies that included children, we also know that long COVID affects a lower but substantial number of children, while severe acute infection is very uncommon at younger ages.49–51 These differences suggests that the underlying mechanism of long COVID may be different from that of the severity of acute infection.
A prolonged state of low-grade infection with a hyperimmune response, coagulation/vasculopathy, endocrine and autonomic dysregulation, and a maladaptation of the angiotensin converting enzyme-2 (ACE-2) pathway have been postulated as the underlying pathophysiology of long COVID.52 Deconditioning due to prolonged immobilization during hospitalization may compound these problems.53 Direct tissue damage due to COVID-19 has been demonstrated in many parts of the body, including the lung, heart, kidney, and brain.54–59 Due to the large reserves in capacity of most body organs, tissue damage does not immediately lead to symptomatic disease. It may, however, become apparent over time that COVID-19 will contribute to an earlier onset and greater occurrence of long-term symptomatic major organ disease with increasing age or if these organs become diseased by other mechanisms. The rate of recovery from long COVID, moreover, suggests that less permanent factors may underlie these debilitating symptoms.
We have adopted the WHO case definition which stipulates a minimum period of three months after infection before calling ongoing symptoms long COVID or post-COVID-19 condition. Others have suggested a threshold of three weeks to define a case of long COVID, arguing that no competent virus has been replicated beyond three weeks of infection, but a period of up to 12 weeks has been suggested to define the start of long COVID.12,52,60 This analysis accounts for COVID infections through the end of 2021 and therefore does not cover the omicron wave, and it is currently unclear what the risk of long COVID is after infection with omicron. The large proportion of asymptomatic infections with omicron and the fact that if symptoms arise they mostly affect the upper airways suggests that the risk of long COVID will be much smaller.
The recovery pattern among community cases for the three symptom clusters quantified suggests that the majority of cases resolve, a sign of hope for those experiencing these debilitating symptoms. It is not yet clear if there is a smaller proportion of patients, especially among those with more severe acute episodes, who develop a more chronic course of long COVID. Given that the longest follow-up time among the studies we examined was 12 months, the true long-term pattern of recovery will only be revealed as studies conduct longer follow-up periods. The time-limited course of long COVID in most cases has led to the advice to provide rehabilitative support in the community, with specialist rehabilitation services required only for those with protracted and more severe problems, particularly when compounded by post-intensive care syndrome.12,61 Important to patients is that they feel empathy and recognition from health-care workers even if they can only provide symptomatic and supportive care.62 Quantifying the number of incident and prevalent cases of long COVID will help policy makers ensure adequate access to services to guide patients towards recovery, return to the workplace or schooling, and restoration of their mental health and social life. The attention given to long COVID may also provide greater recognition to patients who suffer from the longer-term consequences of other infectious diseases and who may have received less attention from health services. The large number of people affected by long COVID should also create new opportunities to unravel phenotypical and genotypical characteristics, with an aim to find new treatments and predictors of post-acute disease syndromes including those known to occur after other infectious disease and intensive care for other critical illness.
The main strength of this study is the willingness of researchers from ten follow-up studies to share data and analyses with consistent approaches to deal with the diverse study methods and instruments. This collaborative effort also allowed us to go beyond the reporting of individual symptoms or counts of symptoms reported in the literature. With access to individual patient data, we were able to define clusters of symptoms that frequently occur together and to quantify the overlap among symptom clusters. Importantly, we were able to correct for over-reporting from studies that did not have a comparison with previous health status, leveraging information from the cohort studies that explicitly asked respondents to recall their pre-COVID health status or existence of symptoms. In addition, the very large health insurance databases from the USA allowed us to identify controls matched on demographic and disease characteristics and thus correct for the occurrence of these symptoms unrelated to SARS-CoV-2 infection. This may in part explain why our estimates of long COVID are lower than often reported in the literature. Direct comparisons are not easy, as we have defined clusters of symptoms that are not reported by others. However, we think this is a strength of this analysis in comparison to studies reporting individual symptoms or counts of symptoms.
There are also important limitations to our analysis. First, the uncertainty intervals around the estimates are wide, reflecting as yet limited and heterogeneous data. Second, we had to derive separate algorithms for each contributing study to achieve consistency in case definitions of the three chosen symptom clusters. Efforts to achieve standardization of questions and instruments for studies of long COVID are underway.5,63 This would make pooling estimates among studies less prone to measurement bias. Third, we assumed that long COVID follows a similar course in all countries and territories. We used data from western European countries, Iran, Russia, India, China, South Africa, Turkey, Saudi Arabia, Israel, Australia, and the USA. Additional reports from Brazil and Bangladesh suggest that long COVID similarly affects other parts of the world.21,22 As more information becomes available, we can explore whether there is geographical variation in the occurrence or severity of long COVID. We also note that the duration estimates relied on studies from high income countries only. With repeated follow-up being planned in many of the studies and with new studies appearing, it will become clearer over time how generalizable our findings on duration are. Fourth, apart from symptoms and symptom clusters, new diseases have been reported to occur more frequently in patients after COVID-19 diagnosis, including cardiovascular complications like myocarditis, acute myocardial infarction, and thromboembolic events as well as kidney, liver, gastrointestinal, endocrine, and skin disorders.64–66 The data sources to quantify these COVID-19-related changes may not yet be sufficient due to lags in reporting of clinical informatics data, disease registries, or surveys, which form the basis of estimation for such diseases. Fifth, with limited follow-up time available, the pattern of recovery cannot yet be fully described. Importantly, longer follow-up can reveal if there is a subset of cases that go on to have a protracted course of long COVID and need longer care. Sixth, we made the assumption that long COVID only affects those with a symptomatic course of the initial infection. The participating cohorts included few asymptomatic cases: the Faroe Islands, Zurich SARS-CoV-2 Cohort, HAARVI, Rome ISARIC pediatrics and adults cohorts observed 22, 182, 9, 27, and 26 asymptomatic COVID cases, respectively. Long COVID was not identified among asymptomatic cases that were followed in HAARVI and Rome ISARIC cohorts. In the Faroe Islands and Zurich SARS-CoV-2 cohorts, three and five of their asymptomatic cases, respectively, developed at least one long COVID symptom cluster at follow-up. The total number of asymptomatic cases followed in these studies is very low and we chose to be cautious and exclude them from our calculations. In a review of medical records in the University of California COvid Research Data Set (UC CORDS), 32% of those with long COVID symptoms at two months after a positive PCR test reported no symptoms at testing, but it is not clear how many of these developed acute symptoms after testing.60 Seventh, we chose three commonly reported symptom clusters but have not quantified other common symptoms. The main symptoms of our three symptom clusters are those that reached the highest degree of consensus in the Delphi process WHO used to create a clinical case definition for post COVID-19 condition.5 In the most complete cohort, the Sechenov StopCOVID cohort, we had information on a wide range of symptoms and general health status with explicit comparison with the pre-COVID-19 status (eSection 5). Among 1309 respondents with PCR-confirmed COVID-19 needing hospitalization, 136 qualified for at least one of our three symptom clusters of long COVID at six months follow-up. Another 62 respondents reported not having fully recovered. Of these, 48 reported at least one symptom of our three symptom clusters but had failed to meet all criteria by reporting either no or slight problems with usual activities or no worsening of this item compared to before COVID-19. Other more common symptoms that were reported by this group included problems with vision, sleep problems, loss of smell, palpitations, and hair loss. Quantifying vision loss requires measurement of visual acuity, which is not measured in long COVID studies. There are no DWs for loss of smell, hair loss, or palpitations. While there is a disability weight for insomnia, it has not been used in any GBD study as sleep disorders are not (yet) included in the GBD cause list. Estimates therefore do not reflect the burden of the full range of long COVID outcomes.
Conclusion
We have quantified the frequency at which common symptom clusters of long COVID have occurred across the world and made an estimate of their severity and expected duration. Many countries and territories have already responded by setting up specialized treatment centers for those affected.67,68 Understanding the magnitude of the problem will help other countries and territories to respond likewise. Early studies indicate that for most patients with long COVID, there is hope for recovery, but time will tell if all patients recover. The attention given to long COVID during this pandemic should trigger research into the underlying pathology and potential treatment or prevention, the long-term trajectory of long COVID, the potential transition from long COVID into chronic fatigue syndrome, the level of protection from vaccination and the risk of long COVID following more recent omicron variants. Such research may also benefit those who experience similar outcomes following a range of other infectious diseases, an issue that has not received much attention from clinical and global heath communities.
Data Availability
All data produced in the present study are available upon reasonable request to the authors.
Declaration of interests
C Adolph reports support for the present manuscript from the Benificus Foundation. P Bobkova, A Gamirova, A Shikhaleva, and A Svistunov report grants from the British Embassy in Moscow ‘StopCOVID Cohort: Clinical Characterisation of Russian Patients’ 2020-2021” paid to Sechenov University, outside the submitted work. X Dai reports support for the present manuscript from Bloomberg Philanthropies and the Bill & Melinda Gates Foundation, paid to the Institute for Health Metrics and Evaluation. A Flaxman report stock options from Agathos, Ltd., and provides technical advising on simulation modeling for Janssen, SwissRe, Merck for Mothers, and Sanofi, outside the submitted work. R Frithiof reports support for the present manuscript from The Swedish Research Council and the Swedish Kidney Foundation, paid to Uppsala University. N Fullman reports funding from WHO for consultant work in 2019 and funding from Gates Ventures since 2020, outside the submitted work. A Gamirova reports grants and contracts from the British Embassy in Moscow (PI): ‘StopCOVID Cohort: Clinical Characterisation of Russian Patients’ 2020-2021, paid to Sechenov University. J Haagsma reports grants from the EuroQol Foundation, outside the submitted work. M Heijenbrok-Kal and R van den Berg-Emons report support for the present manuscript from ZonMW Program COVID-19, Laurens, and Rijndam Rehabilitation, paid to Erasmus MC. M Hultström reports support for the present manuscript from Knut and Alice Wallenburg Foundation, Swedish Heart-Lung Foundation, and Swedish Society of Medicine, paid to Uppsala University. M Lipcsey reports grants or contracts from Hjärt-lungfonden Sweden and is a member of the PROFLO RCT and COVID-19_HBO data safety monitoring boards, outside the submitted work. D Munblit reports report grants from the British Embassy in Moscow ‘StopCOVID Cohort: Clinical Characterisation of Russian Patients’ 2020-2021”, Russian Foundation for Basic Research Grant ‘Cell therapy and prevention of ARDS during COVID infection: from basic science to clinical practice’ 2020-2022, all paid to Sechenov University, and was awarded a UK Research and Innovation/National Institute for Health Research grant, payment for lectures given to Merch Sharp & Dohme and Bayer, and reports unpaid leadership positions as co-chair of International Severe Acute Respiratory and Emerging Infection Consortium (ISARIC) Global Paediatric Long COVID Working Group and co-lead of the PC-COS project aiming to define the Core Outcome Set for Long-COVID in collaborator from WHO, and is a member of the ISARIC working group on long-term COVID follow-up in adults, all outside the submitted work. S Nomura reports support for the present manuscript from the Ministry of Education, Culture, Sports, Science, and Technology of Japan. M S Petersen reports support for the present manuscript from Cooperation’s p/f Krunborg and Borgartun, grants or contracts from the Velux Foundation, special COVID-10 funding from the Faroese Research Council, the Faroese Parkinson’s association, and the Faroese Health Insurance Fund, participation on the Board of the Faroese National Data Protection Authority, and receipt of equipment, materials, drugs, medical writing, gifts, or other services from Wantai Total Ab ELISA, outside the submitted work. M Puhan reports support from the University of Zurich Foundation and the Department of Health, Canton of Zurich. A Shikhaleva reports grants and contracts from the British Embassy in Moscow (PI):’StopCOVID Cohort: Clinical Characterisation of Russian Patients’ 2020-2021, paid to Sechenov University. E Spiridonova reports grants and contracts from the British Embassy in Moscow (PI):’StopCOVID Cohort: Clinical Characterisation of Russian Patients’ 2020-2021, paid to Sechenov University. A Svistunov reports a grant from the Russian Foundation for Basic Research Grant ‘Cell therapy and prevention of ARDS during COVID infection: from basic science to clinical practice’ 2020-2022, paid to Sechenov University. R van den Berg-Emons reports support for the present manuscript from ZonMW Program COVID-19, grant for CO-FLOW study project number 10430022010026, Laurens funding for the CO-FLOW study, and from Rijndam Rehabilitation for the CO-FLOW study, all paid to Erasmus MC.
Author access to data
TV and SWH had full access to all the data in the study and took responsibility for the integrity of the data and the accuracy of the data analysis. DB, DaM, DeM, DoM, FS, MeH, MiH, MS, NM, NS, RH, and ZA were responsible for the data collection of the ten collaborating cohort studies. ZA was responsible for the data collection and matching of the administrative data from Veterans Affairs.
Data sharing
All tabulated input data are available upon publication as Supplementary Appendix Data Inputs. Proposals to access de-identified individual-level data up to one year after publication for researchers who provide a methodologically sound proposal for individual participant data meta-analysis should be directed to swulf{at}uw.edu.
Sources of funding and support
The Institute for Health Metrics and Evaluation received funding from the Bill & Melinda Gates Foundation. The COFLOW study is funded by the COVID-19 Program Care and Prevention of The Netherlands Organization for Health Research and Development (ZonMw, grant number 10430022010026), and Rijndam Rehabilitation and Laurens (both in Rotterdam, The Netherlands). A Ferrari and D F Santomauro D F Santomauro are affiliated with the Queensland Centre for Mental Health Research, which receives core funding from the Department of Health, Queensland Government. C Adolph gratefully acknowledges support from the Benificus Foundation. C Wiysonge’s work is supported by the South African Medical Research Council. H Xu received support from the National Institute on Aging (R21AG061142; R03AG064303) and the National Institute on Minority Health and Health Disparities (U54MD012530). R C Reiner’s and A Aravkin’s work was partially supported by NSF Rapid grant #2031096. N Sarrafzadegan, S Haghjooy Javanmard, and N Mohammadifard report support for the Isfahan cohort study from grant number 199093 from the IUMS, grant number RPPH 20 76 from the WHO/EMR, grant number 996353 from the National Institute of Health Researches of Iran, and grant number 99008516 from the Iran National Science Foundation. M S Petersen reports support for the present manuscript from Cooperation’s p/f Krunborg and Borgartun, grants or contracts from the Velux Foundation, special COVID-10 funding from the Faroese Research Council, the Faroese Parkinson’s association, and the Faroese Health Insurance Fund. For this work, Lorenzo Monasta received supported from the Ministry of Health, Rome, Italy, in collaboration with the Institute for Maternal and Child Health IRCCS Burlo Garofolo, Trieste, Italy.
Role of the funding source
The funders of the study had no role in study design, data collection, data analysis, data interpretation, or the writing of the report. Members of the core research team for this topic area had full access to the underlying data used to generate estimates presented in this paper. All other authors had access and reviewed estimates as part of the research evaluation process, which includes additional stages of formal review.
Acknowledgments
References
- 1.↵
- 2.↵
- 3.
- 4.
- 5.↵
- 6.↵
- 7.↵
- 8.
- 9.
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.
- 15.
- 16.↵
- 17.↵
- 18.↵
- 19.
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.
- 56.
- 57.
- 58.
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.
- 66.↵
- 67.↵
- 68.↵
- 69.
- 70.
- 71.
- 72.
- 73.
- 74.
- 75.
- 76.
- 77.
- 78.
- 79.
- 80.
- 81.
- 82.
- 83.
- 84.
- 85.
- 86.
- 87.
- 88.
- 89.
- 90.
- 91.
- 92.
- 93.
- 94.
- 95.
- 96.
- 97.
- 98.
- 99.
- 100.
- 101.
- 102.
- 103.
- 104.
- 105.
- 106.
- 107.
- 108.
- 109.
- 110.
- 111.
- 112.
- 113.
- 114.
- 115.
- 116.
- 117.



