
Abstract
Background Reports of SARS-CoV-2 causing laryngotracheobronchitis (commonly known as croup) have been limited to small case series. Early reports suggest the Omicron (B.1.1.529) strain of SARS-CoV-2 (the dominant circulating US strain since the week of 12/25/2021) replicates more efficiently in the conducting airways. This may increase the risk of a croup phenotype in children as they have smaller airway calibers.
Methods Description of the incidence, change over time, and characteristics of children with SARS-CoV-2 and upper airway infection (UAI) diagnoses within the National COVID Cohort Collaborative (N3C) before and during the rise of the Omicron variant. We compare the demographics, comorbidities, and clinical outcomes of hospitalized SARS-CoV-2 positive children with and without UAI.
Results SARS-CoV-2 positive UAI cases increased to the highest number per month (N = 170) in December 2021 as the Omicron variant became dominant. Of 15,806 hospitalized children with SARS-CoV-2, 1.5% (234/15,806) had an UAI diagnosis. Those with UAI were more likely to be male, younger, white, have asthma and develop severe disease as compared to those without UAI.
Conclusions Pediatric acute UAI cases have increased during the Omicron variant surge with many developing severe disease. Improved understanding of this emerging clinical phenotype could aid in therapeutic decision-making and healthcare resource planning.
Introduction
SARS-CoV-2 can cause severe pediatric disease including acute COVID-19 and multisystem inflammatory syndrome in children (MIS-C)1. Published reports of SARS-CoV-2 causing laryngotracheobronchitis (commonly known as “croup”), however, have been limited to small case series2. Other coronaviruses (e.g. type NL63) are known to cause croup.
The Omicron (B.1.1.529) strain of SARS-CoV-2 became dominant in the U.S. during the week of 12/25/20213. Early reports suggest Omicron may cause lower severity disease than the Delta variant4. This may be because Omicron replicates less efficiently in lung parenchyma and more efficiently in the conducting airways5. However, these mechanistic hypotheses have not been confirmed.
Young children are especially vulnerable to acute upper airway infection (UAI) because their airways are small and relatively collapsible. Inflammation from UAI can rapidly decrease air flow. Accordingly, croup is classically an early childhood disease. We conducted this retrospective cohort study to determine if acute UAI is more common as Omicron has become the dominant U.S. SARS-CoV-2 variant.
Methods
We leveraged the National COVID Cohort Collaborative (N3C)6 and a pipeline we built for a NIH-funded pediatric COVID-19 dashboard (https://covid.cd2h.org/pediatrics-dashboard/) to conduct this study. Among all children in N3C <19-years-old with a positive SARS-CoV-2 test (polymerase chain reaction, antigen, or antibody), we identified those with a croup or tracheitis diagnosis. We included bacterial tracheitis because it can be difficult to distinguish from □— and can be a complication of □— viral croup. We compared groups using chi-square and Fisher exact tests for categorical variables and Mood’s Median test and t-tests for continuous variables. The N3C Data Enclave, data transfer from sites to N3C, and this analysis were approved under separate institutional review board protocols as documented elsewhere1.
Results
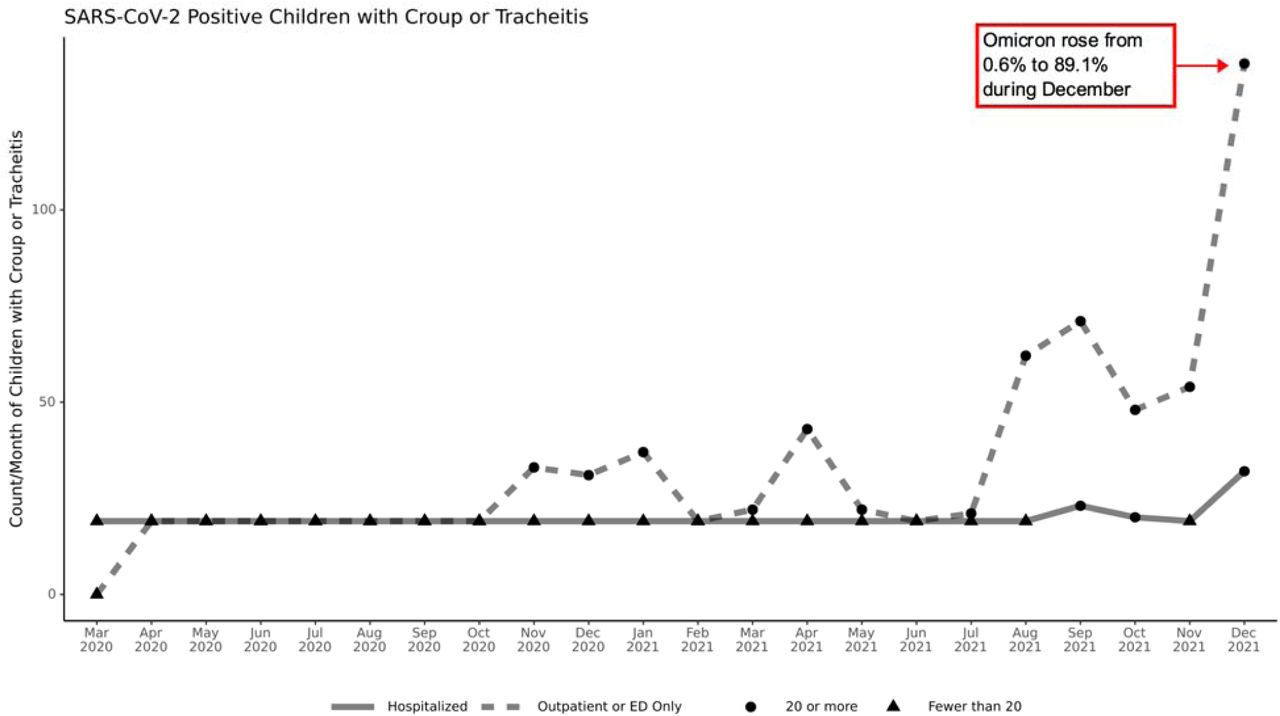
SARS-CoV-2 positive UAI cases have increased as the Omicron variant has become dominant (Figure 1). During December 2021, we observed the largest monthly number thus far of hospitalized (N=32) and non-hospitalized (N=138) SARS-CoV-2 positive UAI cases. Of December 2021 hospitalizations, 2.5% (32/1302) had UAI. Overall, the 1/13/2022 N3C data release contains 15,806 hospitalized SARS-CoV-2 positive children, of whom 1.5% (234/15,806) had UAI (Table 1). Compared to those without UAI, those with UAI were more likely to be male (59.8% versus 50.4%, p=0.003), younger (2.4 versus 10.1 years, p<0.001), white (54.7% versus 43.3%, p=0.02), and have asthma (15% versus 10%, p=0.02). Children with UAI experienced severe disease (invasive ventilation, vasopressors, ECMO, or mortality) more often compared to children without UAI (31.6% versus 13.5%, p<0.001).
{kind=link}
This figure shows the count per month of inpatient (solid line) and outpatient/Emergency Department (dotted line) encounters with a diagnosis of croup or tracheitis for children less than 19-years old with positive SARS-CoV-2 tests in the National COVID Cohort Collaborative (N3C) January 13th, 2022 data release. The percentage of SARS-CoV-2 samples found to be the Omicron strain is from the U.S. Centers for Disease Control COVID Data Tracker, available at https://covid.cdc.gov/covid-data-tracker/#variant-proportions and accessed January 19, 2022. Triangles represent individual counts 1-19 that are censored as per N3C policy and shown as n = 19 in the figure.
This table shows demographic and clinical characteristics for children less than 19 years old with positive SARS-CoV-2 tests, with and without a diagnosis of croup or tracheitis. Per N3C policy, cells with less than 20 patients are reported as “<20 (x%)” where x is the percentage if n = 20.
Discussion
Overall, pediatric acute UAI has increased during the Omicron variant surge. Nearly a third of affected children develop severe disease. This observed clinical phenotype of pediatric infection by the Omicron variant appears to confirm recent mechanistic reports.
A limitation of this analysis is that diagnosis codes will only be present for completed hospitalizations in N3C; children who are still hospitalized are not represented.
Although many children with acute UAI are managed as outpatients, those with severe croup and/or tracheitis are at risk of cardiac arrest from rapid-onset upper airway obstruction. They may require therapies typically provided in intensive care units including frequent administration of nebulized racemic epinephrine, helium/oxygen mixtures, and intubation. While SARS-CoV-2 pediatric UAI rates are not overwhelmingly high, understanding this new clinical phenotype is important to health systems under severe strain. Anticipation of the potential for acute upper airway obstruction may guide therapeutic decision-making and hospital planning for available equipment and personnel.
Data Availability
All data and analyses utilized in the present study are available within the N3C data enclave and accessible following N3C registration and submission of a Data Use Request. For more information visit: https://ncats.nih.gov/n3c/about/applying-for-access
Acknowledgements
The N3C was funded by NCATS grant number U24 TR002306 and other support as documented at https://covid.cd2h.org/acknowledgements. This analysis was supported by NICHD grant number R01HD105939-01S1.



