
Abstract
Positive framing has been proposed as a potential intervention to increase COVID-19 vaccination intentions. However, most available research has examined fictitious or unfamiliar treatments. This pre-registered study compared positively and negatively attribute-framed side effect information for real COVID-19 booster vaccines (AstraZeneca, Pfizer, Moderna) and measured intentions pre- and post-intervention in 1,222 UK-based participants. Positive framing increased booster intentions among those with low baseline intentions overall. As hypothesized, however, vaccine familiarity significantly modulated this effect, with positive framing being effective for the least familiar vaccine (i.e., Moderna), while standard negative framing appeared to increase intentions for familiar vaccines (AstraZeneca/Pfizer). These findings provide important new evidence that positive framing could improve vaccine uptake globally when switches or new developments require individuals to receive less familiar vaccines – as is currently the case for millions of booster vaccines across the world. Positive framing of familiar vaccines, however, should be treated with caution.
Introduction
With vaccine efficacy for Severe Acute Respiratory Syndrome Coronavirus 2 (COVID-19) waning over time1,2 and reduced for emerging variants3,4, many countries are currently accelerating their COVID-19 booster programmes5,6 to protect against COVID-19 viruses7,8. However, vaccine availability does not necessarily translate to vaccine acceptance9, with the World Health Organization (WHO) recognising vaccine hesitancy as a global health threat10. Side effect apprehension is a primary factor driving this hesitancy11, with one study finding 90% of COVID-19 vaccine refusers feared side effects more than the virus itself12. Given the recency of booster programmes, evidence for hesitancy among those already vaccinated is sparse. However, side effect severity associated with previous vaccine doses has already been associated with booster hesitancy in one study13. Reducing perceptions of negative side effects could be vital for increasing booster acceptance and thereby reducing the global burden of the current COVID-19 pandemic.
One method of reducing negative perceptions regarding side effects, suggested by the WHO14, concerns “message framing” of vaccine-relevant information15. Positive attribute framing, where side effect information is framed in terms of the inverse incidence rate (e.g., “60% will not get a sore arm”) as opposed to typical negative framing with the standard incidence rate (e.g., “40% will get a sore arm”) could be particularly useful for combatting COVID-19 vaccine hesitancy. First, it is directly applicable to side effects. Second, informed consent is maintained as a consequence of statistical consistency across frames16. Third, there is preliminary evidence that positive attribute framing can improve vaccination attitudes in other settings. For example, one study on the influenza vaccine found positive attribute framing (hereafter positive framing) reduced the expectation and experience of side effects, increased perceived protection from influenza, and reduced distortions in the perception of side effect risk17, with this pattern of results replicated for other vaccine types18.
Studies examining whether COVID-19 vaccine intention is amenable to framing techniques have produced mixed results19–21. However, these studies focused on vaccine-naïve individuals, did not employ attribute framing, and did not concern booster intentions. Critically, existing studies either used fictitious COVID-19 vaccines19,20 or did not name specific COVID-19 vaccines that at the time were being approved for administration21. As such, participants either had limited knowledge of, or investment in, the framed vaccines. As the pandemic has progressed, media discourse22,23 combined with direct and socially-observed experience of COVID-19 side effects24, means it is essential to understand whether positive framing is effective for real-world vaccines where prior knowledge and experience exists.
This is particularly important because there is reason to believe that prior knowledge regarding a given COVID-19 vaccine may moderate the strength of any positive framing effect. For example, the increased relevance of, or belief in, a particular treatment or societal issue has been shown to decrease the efficacy of different forms of framing25,26, including the effect of positive framing on the perception of hypothetical vaccines25,27. The effect of positive framing on vaccine intention may therefore be limited to less familiar vaccine types. However, there are two important reasons why attribute framing may still hold utility for COVID-19 vaccines even if limited to unfamiliar vaccines. First, new composition changes to COVID-19 booster vaccines have been recommended28 and are currently being developed29 to protect against emerging variants. Second, many booster programmes (e.g., in the United Kingdom) require individuals to switch from their previous COVID-19 vaccine (e.g., AstraZeneca Vaxzevria). Some alternatives (e.g., Pfizer Cominarty) are more familiar than others (e.g., Moderna Spikevax). As treatment switches have been demonstrated to result in poorer health outcomes and treatment discontinuation in general30,31, positive framing may be beneficial for increasing uptake for booster switches of this type. However, as medical research on positive framing has tended to focus on fictitious medications and patient scenarios25,27, 32–36, a paucity of evidence exists concerning the effect of familiarity on ecologically valid treatments, especially given the salience of COVID-19 vaccinations at the population level.
In this pre-registered study (aspredicted.org/53ph4.pdf), conducted in the UK, attribute framing was applied to side effects from genuine manufacturer Patient Information Leaflets (PILs) for the AstraZeneca, Pfizer, and Moderna vaccines. A factorial design was employed, with participants randomised to read positive or negatively framed PILs for the same vaccine they had previously received (either AstraZeneca/Pfizer), a familiar vaccine in the UK context (Pfizer/AstraZeneca), or an unfamiliar vaccine (Moderna). It was hypothesised that a) positive framing would increase booster intention, and b) the effect of positive framing would decrease with vaccine familiarity. Following previous research16,32, 37– 39 secondary outcome variables concerning booster side effect severity, perceived risk, and booster acceptance (satisfaction, happiness, anxiety) were explored as potential mediators of the framing effect on vaccine intention.
Results
Overview
Participants (N=1,222) were recruited via Pureprofile, an international recruitment service, between 27th October and 8th November 2021. All were pre-screened (see Methods) with data removed based on pre-registered quality control criteria (see Supplementary Materials 1). Only those who had received two doses of either the AstraZeneca or Pfizer COVID-19 vaccines were eligible to participate, with participants stratified by their previous vaccine type.
Participants from each stratum were subsequently randomised to one of six experimental conditions (3(Familiarity) * 2(Framing) factorial design; see Figure 1). Baseline ratings were collected regarding primary and secondary outcome measures—all recorded on a 100-point VAS. The primary outcome was the participant’s intention to receive a booster vaccine. Secondary outcomes were: 1) perceived booster side effect severity; 2) perceived booster risk; 3) booster acceptance (with satisfaction, happiness, and anxiety measured separately). Wording of items can be found in Figure 1. Familiarity with the side effects of the AstraZeneca, Pfizer, and Moderna vaccines were additionally assessed (100-point VAS) to determine whether side effect knowledge corresponded with the predetermined factorial categories of vaccine Familiarity (i.e., Same > Familiar > Unfamiliar).

Sample size, experimental design, and item wording for primary and secondary outcomes
Framed side effect information was subsequently presented dependent on condition. This information took the form of genuine manufacturer PILs for the AstraZeneca, Pfizer, and Moderna vaccines. Side effects were retained in their original form and order and presented in standard EU verbal prevalence categories and frequency bands. Positive framing was applied only to the frequency bands (for example see Figure 2, with full wording and PILs presented as Supplementary Materials 2-3). To manipulate familiarity, participants were randomised to view PILs from the following conditions: ‘Same’ (PIL for the COVID-19 vaccine previously received: AstraZeneca-AstraZeneca|Pfizer-Pfizer); ‘Familiar’ (PIL for a common vaccine not previously received: Pfizer-AstraZeneca|AstraZeneca-Pfizer); ‘Unfamiliar’ (PIL for a less common vaccine in the UK: AstraZeneca-Moderna|Pfizer-Moderna). Familiarity was judged based on UK data (22nd September 2021) outlining that 19.4 and 24.0 million second doses of the Pifzer and AstraZeneca vaccines had been delivered respectively, relative to 1.2 million of Moderna40. After timed PIL presentation of 2 minutes, all participants provided post-manipulation ratings for the primary and secondary outcomes (as above). Participants were then presented with 14 side effects from the PIL they had read and were required to: 1) assign each to a verbal prevalence category (i.e., very common, common, uncommon, rare, very rare); 2) estimate frequency of occurrence (number of people in 100,000 expected to experience the side effect.

Positive and negative wording used to frame common and uncommon side effects (wording for all prevalence categories can be found in Supplementary Materials 2)
Descriptive Statistics
Sample Demographics
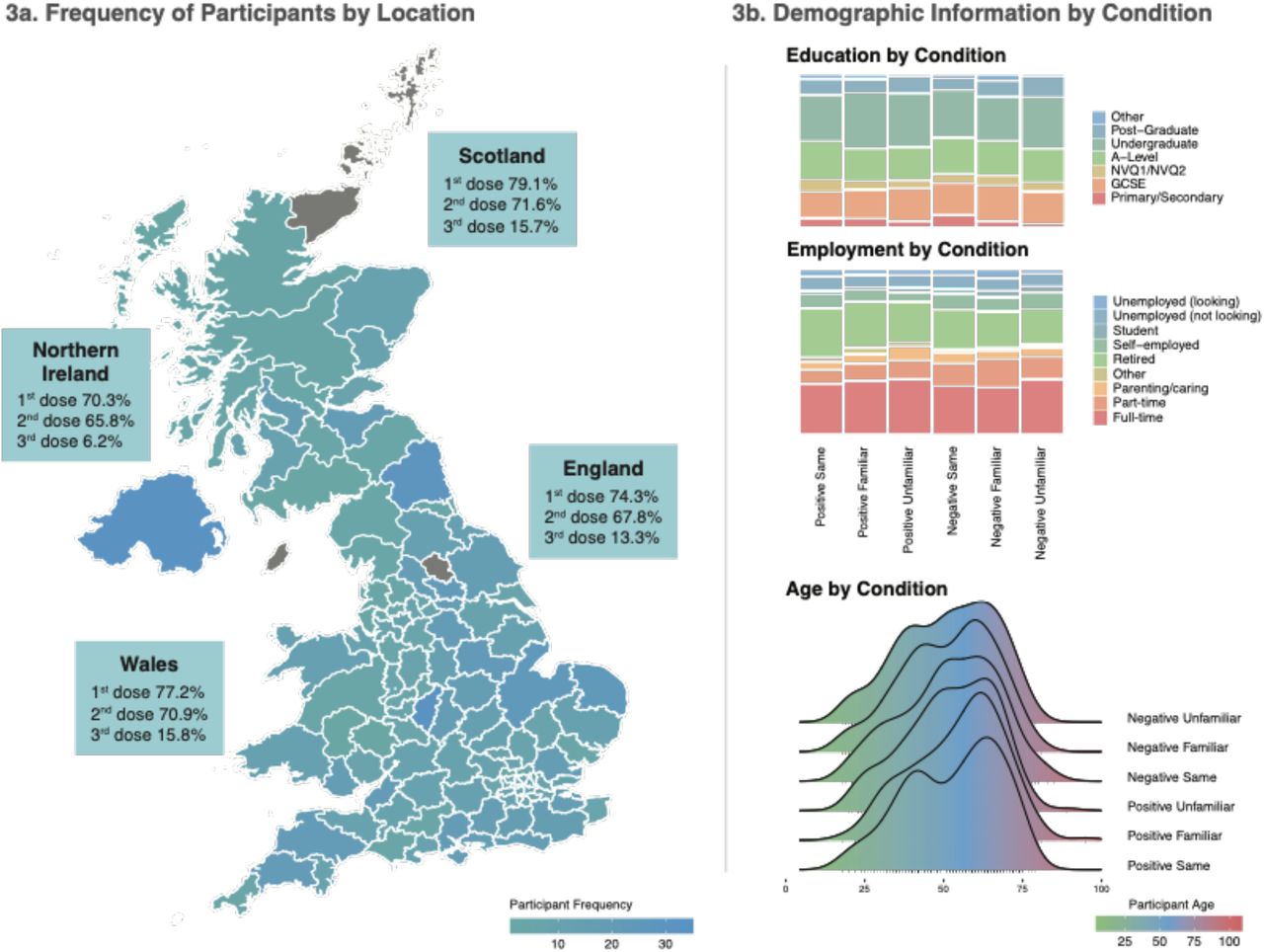
Information regarding participant location, age, education, and employment can be found in Figure 2a-b. Participants were 52.5 years of age on average (range=18-95). As presented in Figure 2a, they resided across most postal areas in the UK, with the largest proportion from London district (N= 53), Birmingham (N=35), and Belfast (N=34). Only Harrogate, and the Orkney and Shetland Islands were not represented. Most respondents identified as British (N=1,064; 87%). Those self-reporting as female were represented slightly more frequently than other genders (N=706; 58%), 34% of the sample had completed undergraduate-level education (N=413), and 33% were in full-time employment (N=407). Full descriptive statistics for the full sample, and by condition, are presented as Supplementary Materials (4-5).
COVID-19 Exposure and Vaccine History
Most participants (N=1,074; 88%) had not personally been infected with COVID-19, while 565 (46%) reported infections among family and close friends. On average, participants had their last COVID-19 vaccine 4.8 months ago. The largest proportion reported not experiencing side effects to either dose (N=579; 47%). Of those who did, the first dose was most associated with severe side effects (N=372; 30%).
Primary Analysis
Knowledge of vaccine side effects mirrors categorical levels of the Familiarity factor
To determine whether side effect familiarity corresponded with the predetermined factorial categories of Familiarity (i.e., Unfamiliar, Familiar, Same), a within-subjects one-way ANOVA (with Greenhouse–Geisser correction) was run on side effect familiarity ratings collected for the three vaccine types prior to the experimental manipulation. A robust main effect of Familiarity was observed (F(1.86, 2272.18)=659.17, p<.001, ηp2=.35). Awareness of side effects increased with Familiarity; being higher for the Same vs. Familiar vaccine (t(1221)=14.11, p<.001, Cohen’s dz =.40), and for the Familiar vs. Unfamiliar vaccine (t(1221)=23.97, p<.001, Cohen’s dz =.69). Mean differences are presented in Figure 4e.
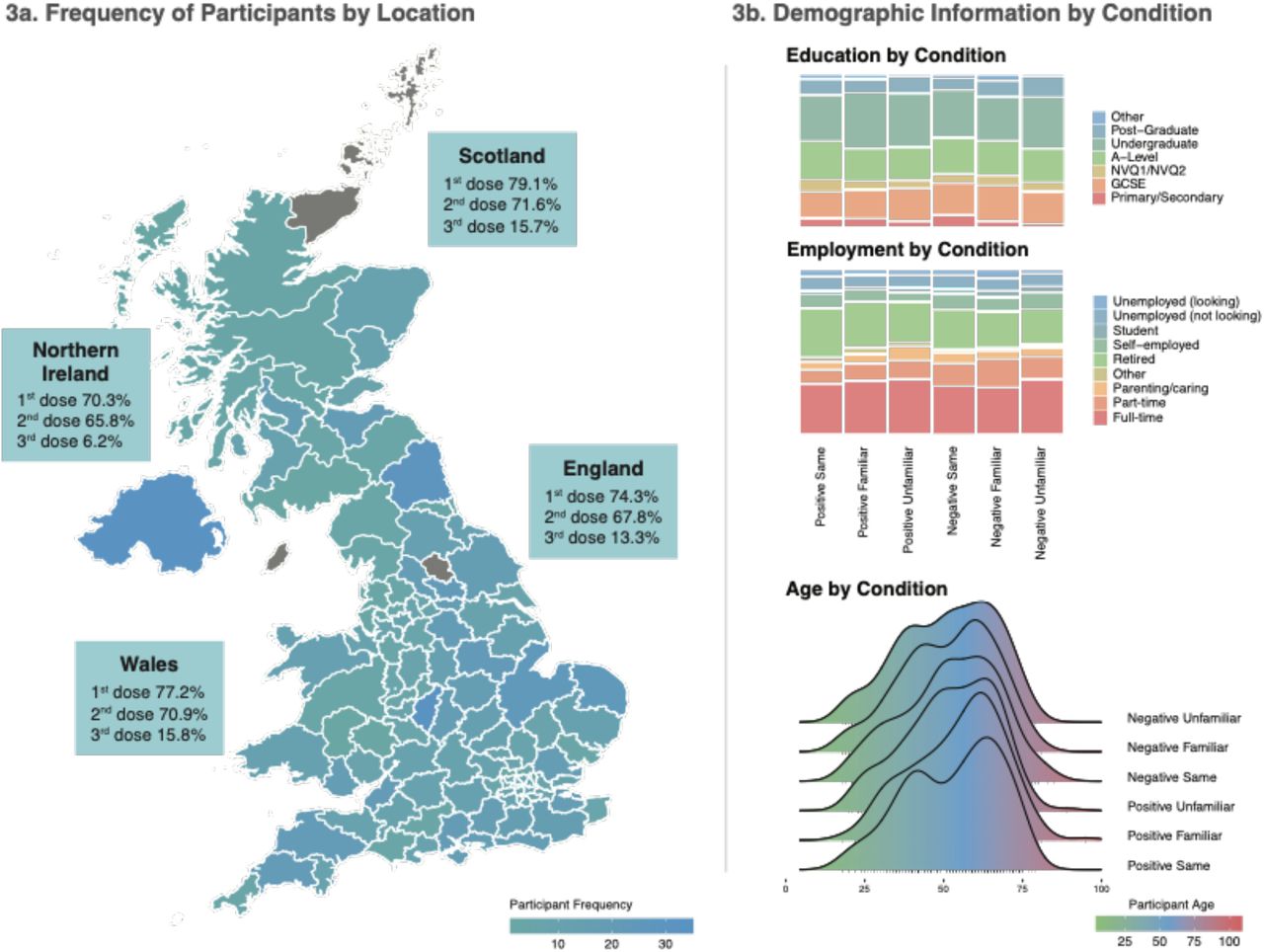
Demographic Information, where 3a plots the frequency of participants from each postal area of the UK against the vaccination rates reported by the UK government on the 3rd November (the final week of data collection) and 3b depicts education and employment categories, and age range, across experimental conditions.

Model estimated mean differences in the primary outcome (Booster Intention), depicted for the whole sample (4a and 4b), and for realistic switches occurring as part of the UK booster programme (4c and 4d). 4e presents data demonstrating that side effect familiarity ratings scaled with the factorial levels of Vaccine Familiarity. All error bars represent ± 1SEM.
Baseline Intention to be vaccinated
A 2(Framing) * 3(Familiarity) ANOVA was conducted on Baseline Booster Intention scores to assess the presence of between-group differences on this variable. Levels of Baseline Booster Intention were anticipated to be high across all conditions (see pre-registration), which was confirmed in the present sample (M=78.36 (/100-point VAS), SD=31.65; range:0-100). However, an unanticipated significant effect of Familiarity was observed on Baseline Booster Intention (F(2, 1216)=49.51, p<.0001, ηp2=.075). This effect reached significance for the orthogonal contrast comparing the Same vs. Other (i.e., combined Familiar and Unfamiliar) vaccine types (F(1, 1216)=96.51, p<.0001, ηp2=.074), but not for the Familiar vs. Unfamiliar comparison (F(1, 1216)=2.42, p=.120, ηp2=.002), indicating higher intentions for previously experienced vaccines.
Effect of framing and familiarity on the intention to be vaccinated
The pre-registered primary analysis plan was a 2(Framing: Positive vs. Negative)*3 (Familiarity: Same Vaccine, Familiar Vaccine, Unfamiliar Vaccine) factorial ANCOVA, with Baseline Booster Intention for the vaccine presented in the participant’s assigned PIL as the covariate, and Post-Manipulation Booster Intention the outcome. However, the fact that Baseline Intention unexpectedly differed systematically with Familiarity meant that including it as a covariate without including its interactions with the manipulated variables (Framing and Familiarity) would violate the assumptions of ANCOVA41. Therefore, to address this, we extended the model to include the interactions between Baseline Booster Intention and the manipulated variables in all analyses, as has previously been recommended when differences in the covariate exist42. Pre-specified orthogonal contrasts for Familiarity were: Contrast1 (Same vs. Other [Familiar and Unfamiliar combined]); Contrast2 (Familiar vs. Unfamiliar). A Framing*Familiarity interaction was hypothesised, with the effect of Framing (increased Booster Intention following Positive vs. Negative framing) reducing with increased Familiarity.
Main effects analysis revealed the anticipated Framing*Familiarity interaction (F(2, 1210)=10.75, p<.0001, ηp2=.018). Specifically, Framing interacted with Contrast1 (Same vs. Other: F(1, 1210)=5.07, p=.025, ηp2=.004) and Contrast2 (Familiar vs. Unfamiliar: F(1, 1210)=16.46, p=.0001, ηp2=.013). As demonstrated in Figure 4a which depicts the interaction means, this pattern of results was driven by Positive Framing increasing Booster Intention for the Unfamiliar vaccine. However, this was superseded by a three-way interaction with Baseline Booster Intention (F(2, 1210)=7.65, p=.0005, ηp2=.013), represented at both Contrasts (Baseline*Framing*Contrast1: F(1, 1210)=4.39, p=.036, ηp2=.004 |
Baseline*Framing*Contrast2: F(1, 1210)=11.19, p=.0008, ηp2=.009). Data presented in Figure 4b, that depicts this interaction, provides a more nuanced understanding of results. Viewing side effect information of any type appeared to increase average Booster Intention (i.e., post-manipulation model estimated means were above zero, for all levels of the baseline covariate). Positive Framing had limited efficacy at high levels of Baseline Intention across Conditions but took effect for the Unfamiliar Vaccine when model estimated VAS scores were lower than ∼80/100. At very low levels of Baseline Intention (i.e., VAS=0), model predicted Booster Intention Post-Manipulation increased from M=19.09 (SEM=2.76, 95% CIs[13.68, 24.50]) for the Negative Frame, to M=35.11 (SEM=2.77, 95% CIs[29.68, 40.50]) for the Positive Frame. Full model output is included as Supplementary Materials 6. We note that the same interaction between Framing and Familiarity was observed in the planned but invalid model excluding the interaction between these factors and Baseline Booster Intention (see Supplementary Materials 7).
The effect of positive framing on vaccine switches
Analyses were performed to investigate the effect of framing on pre-registered and realistic vaccine switches occurring as part of the UK’s booster programme. Specifically, those without medical exemption, who previously received the AstraZeneca vaccine will be required to switch to Pfizer or Moderna, while those who received Pfizer may be required to switch to Moderna.
First, previous vaccine type (AstraZeneca/Pfizer) was entered as a factor in the ANCOVA model above to check for interactions with Framing, Familiarity, and Baseline Booster Intention. While there was a main effect of previous vaccine type (F(1, 1198)=6.36, p=.012, ηp2=.005), with those receiving AstraZeneca reporting increased Booster Intention (M=80.83, SEM= 0.74, 95% CIs [79.37, 82.29]) compared to Pfizer (M=78.01, SEM= 0.74, 95% CIs [76.57, 79.46]), there were no two- or three-way interactions with Framing or Familiarity (all ps>.05; see Supplementary Materials 8).
Previous Vaccine: AstraZeneca
Representative of a switch from AstraZeneca to Pfizer or Moderna, a 2(Framing)*2(Familiarity: Familiar (Pfizer), Unfamiliar (Moderna)) ANCOVA, with interactions between the covariate (Baseline Booster Intention) and factors modelled, was conducted among those who had previously received the AstraZeneca vaccine (N=410). A three-way Framing*Familiarity*Baseline Intention interaction was observed (F(1, 402)=11.38, p=.0008, ηp2=.028). As demonstrated in Figure 4c, in the case of the Unfamiliar vaccine (Moderna) Booster Intention was increased in the Positive Frame at low levels of Baseline Booster Intention. However, the inverse of this pattern was observed for the Familiar vaccine (Pfizer), where Positive Framing decreased Booster Intention at low levels of Baseline Intention.
Previous Vaccine: Pfizer
Representative of a switch from Pfizer to Moderna, a one-way ANCOVA investigating the effect of framing on the perception of the Unfamiliar (i.e., Moderna) PIL was performed on the data of those who had previously received the Pfizer vaccine (N=202). There was a main effect of Framing (F(1, 198)=3.98, p=.048, ηp2=.020), but no statistically significant Baseline Booster Intention*Framing interaction (F(1, 198)=1.80, p=.181, ηp2=.009). However, as demonstrated in Figure 4d, slopes for the Positive and Negative Frame converged at high levels of Baseline Booster Intention.
Secondary Analyses
Positive framing decreases the perception of booster side effect severity
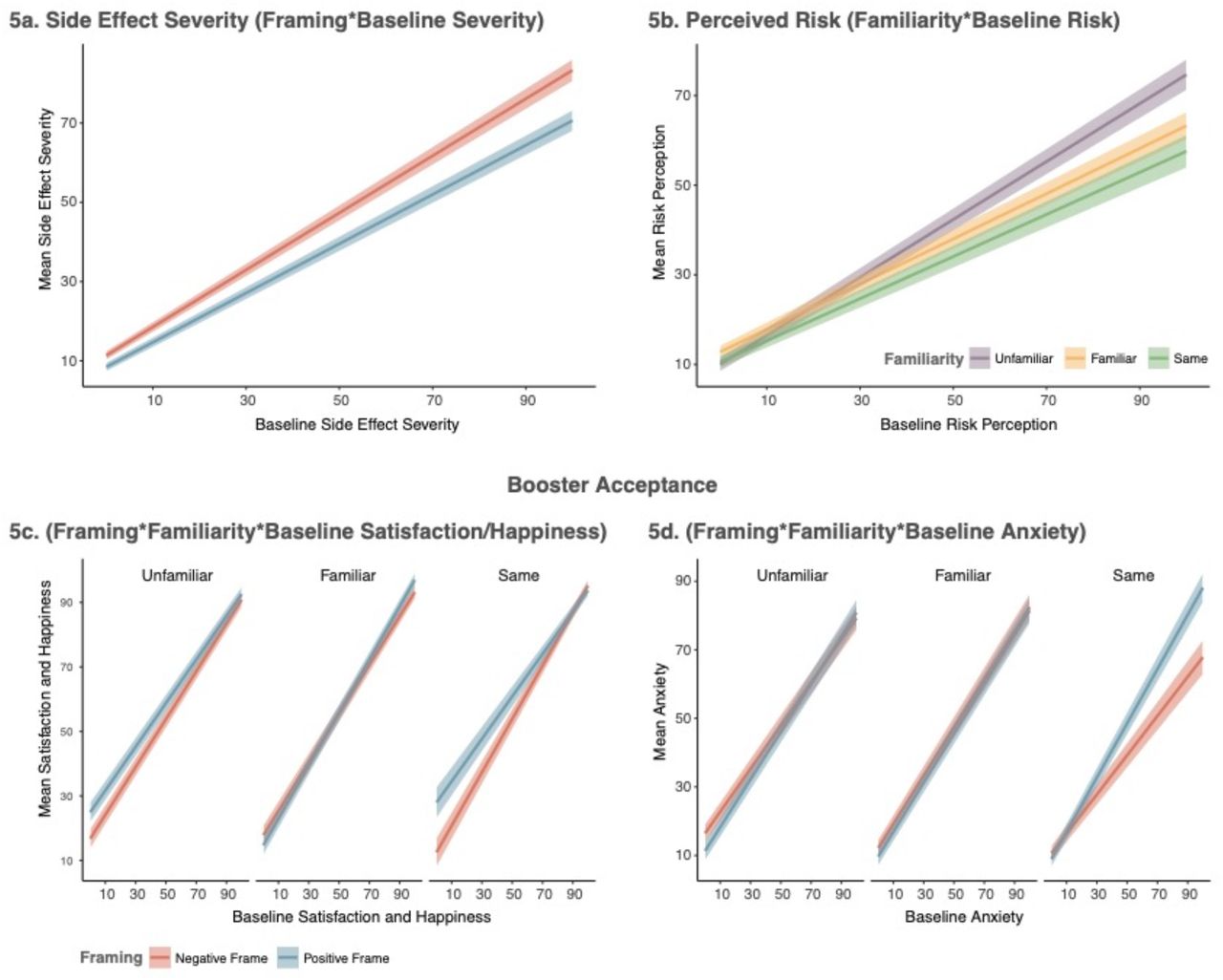
Perceived side effect severity associated with the vaccines was measured pre- and post-manipulation. A 2(Framing)*3(Familiarity) ANCOVA (contrasts as above), including interactions with the covariate (Baseline Side Effect Severity), revealed a main effect of Framing (F(1, 1210)=3.92, p=.048, ηp2=.003), and a Baseline Severity*Framing interaction (F(1, 1210)=4.52, p=.034, ηp2=.004). There were no other two- or three-way interactions (all ps>.35). As depicted in Figure 5a, reading about side effects in any frame increased the perception of their severity (i.e., post-manipulation model estimated means are above zero, for all levels of the baseline covariate). However, Positive Framing resulted in a lower perception of side effect severity, which was strongest when side effects were perceived as severe at baseline. Full model output is included as Supplementary Materials 8.
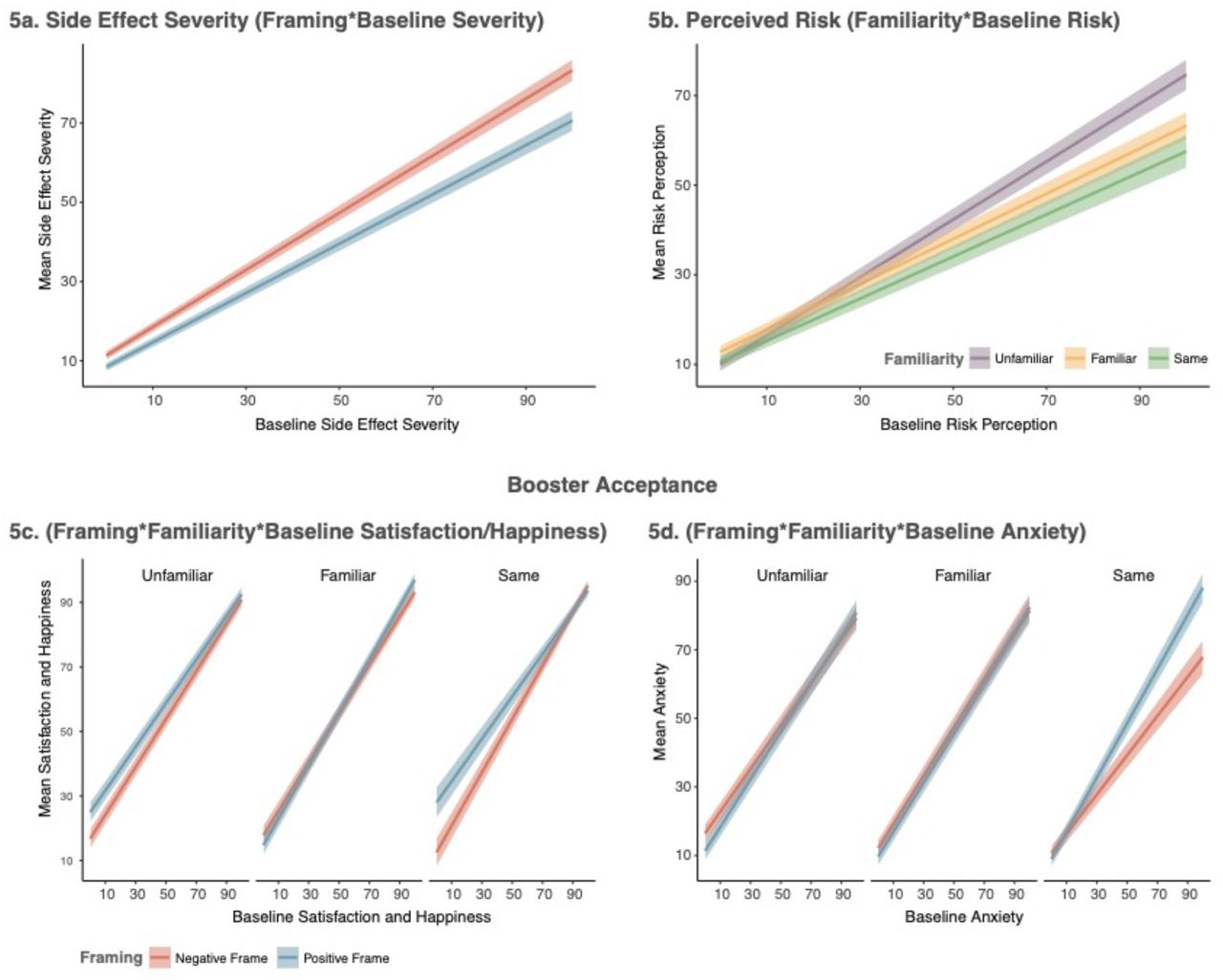
Mean values for secondary outcome measures, where 5a depicts model-estimated mean differences regarding side effect severity ratings, 5b perceptions of vaccine risk, 5c combined satisfaction and happiness associated with the framed vaccine, and 5d anxiety surrounding the framed vaccine. All error bars represent ± 1SEM.
Perception of booster vaccine risk decreases with vaccine familiarity
Perception of risk to participant’s health associated with receiving the vaccines was recorded pre- and post-manipulation. The main effect of Framing did not reach statistical significance (F(1, 1210)=1.04, p=.308, ηp2=.001). There was a Familiarity*Baseline Risk Perception interaction (F(2, 1210)=4.82, p=.008, ηp2=.008), evident in both contrasts (Baseline Risk*Contrast1: F(1, 1210)=4.28, p=.039, ηp2=.004 | Baseline Risk*Contrast2: F(1, 1210)=6.03, p=.014, ηp2=.005). No other statistically significant main effects or interactions were observed (all ps>.10). As depicted in Figure 5b, there was limited difference between Familiarity conditions when the perception of risk was low at baseline. At high levels of Baseline Risk, Post-Manipulation Risk Perception was lowest for the previously experienced vaccine and highest for the Unfamiliar vaccine. Full model output is included as Supplementary Materials 10.
Positive framing increases satisfaction and happiness with the framed booster but does not reduce anxiety
At pre- and post-manipulation, participants were asked to imagine that the framed vaccine was their only option for a booster and to rate their Satisfaction, Happiness and Anxiety regarding this outcome. In order to reduce the data for analysis, the three variables were entered into a principal components analysis. Component loading suggested that Satisfaction and Happiness loaded onto a similar latent construct, while Anxiety was associated with another. Therefore, Satisfaction and Happiness were averaged together for the subsequent analyses, while Anxiety was treated separately. Two ANCOVAs were run on these outcomes. The first revealed a main effect of Framing (F(1, 1210)=5.66, p=.018, ηp2=.005) and a Framing*Familiarity (F(2, 1210)=3.63, p=.027, ηp2=.006) and Baseline Satisfaction/Happiness*Framing*Familiarity (F(2, 1210)=3.43, p=.033, ηp2=.006) interaction. This three-way interaction was significant for Contrast1 (Same vs. Other: F(1, 1210)=4.11, p=.043, ηp2=.003), but not Contrast2 (Familiar vs. Unfamiliar: F(1, 1210)=2.56, p=.110, ηp2=.002). As shown in Figure 5c, for the Same and Unfamiliar vaccines, lowered satisfaction and happiness were generally associated with Negative Framing, particularly at low levels of Baseline Satisfaction/Happiness. There appeared to be no difference for the Familiar vaccine.
With respect to anxiety, there was a significant Baseline Anxiety*Framing interaction (F(1, 1210)=5.53, p=.019, ηp2=.005), but no other main effects or interactions (all ps>.05). As shown in Figure 5d, Positive Framing appeared to increase Post-Manipulation Anxiety at very high levels of Baseline Anxiety, but was limited to the Same Condition (i.e., among participants who had high Baseline Anxiety regarding continuation with their previous vaccine type), with this interaction nearing significance (Anxiety*Framing*Contrast1: F(1, 1210)=3.65, p=.056, ηp2=.003). Correlations, PCA, and Models are presented as Supplementary Materials 11.
Positive framing influences judgements regarding side effect prevalence
Participants were required to classify 14 side effects from their assigned PIL into verbal prevalence categories, as well as provide a frequency estimate regarding how many people, in 100,000, they thought would experience each side effect if they received the framed vaccine. Eleven side effects were associated with discrete prevalence categories. Three were presented in the PILs as of ‘unknown prevalence’. Raw frequency estimates of the latter were analysed separately to test whether framing alters perceptions regarding prevalence when no information is provided. Side effects from each PIL are included as Supplementary Materials 12. For side effects with a concrete category, the percentage of side effects correctly assigned across verbal prevalence categories, and frequency bands, were computed as outcome measures. Frequency estimates were judged correct based on the following frequency bands39: Very Common = 10,001–100,000 (>10%); Common = 1001–10,000 (>1–10%); Uncommon = 101–1000 (>0.1–1%); Rare = 11–100 (>0.01–0.1%); Very Rare = 0–10 (0–0.01%). ANOVAs were performed with Framing and Familiarity as factors.
Verbal Prevalence Categories
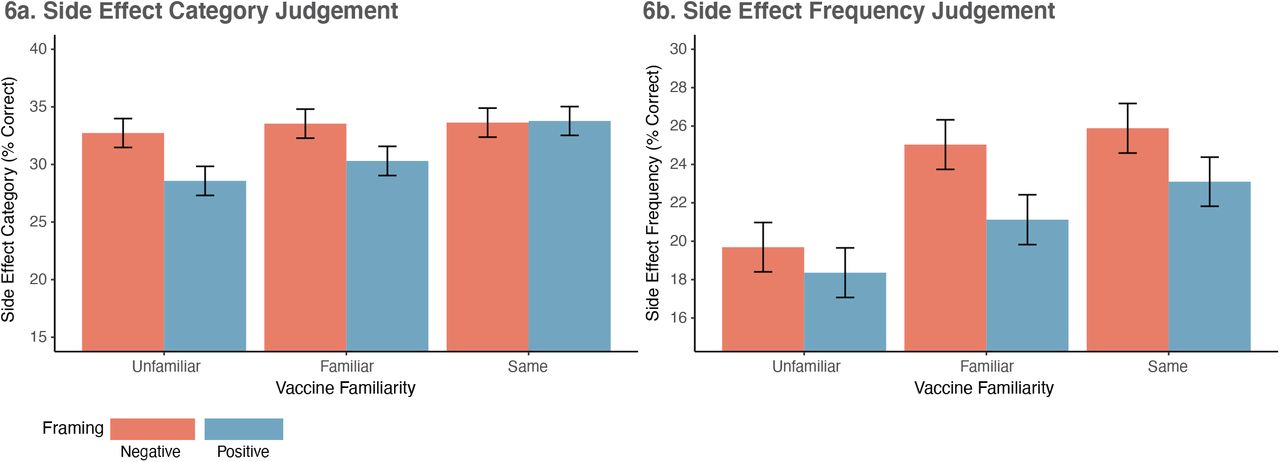
As depicted in Figure 6a, a main effect of Framing (F(1, 1216)=5.54, p=.019, ηp2=.005) was observed, while Familiarity neared significance (F(2, 1216)=2.98, p=.051, ηp2=.005). This was driven by Contrast1 only (Same vs. Other: F(1, 1216)=4.93, p=.027, ηp2=.004). While accuracy was generally low, fewer accurate classifications were made following Positive Framing (M=30.9%, SEM=0.73, 95% CIs [29.46, 32.31]), relative to Negative Framing (M=33.3%, SEM=0.73, 95% CIs [31.87, 43.73]). While the reduction in accuracy associated with positive, relative to negative, framing appeared to decrease with familiarity, the Framing*Contrast1(Same vs. Other) interaction did not reach statistical significance (F(1, 1216)=3.11, p=.078, ηp2=.003). Full model output is included as Supplementary Materials 13.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Mean percentage of correct category (6a) and frequency (6b) judgements. All error bars represent ± 1SEM.
Frequency Estimates
A main effect of Framing (F(1, 1216)=6.45, p=.011, ηp2=.005) and Familiarity (F(2, 1216)=9.71, p=.0001, ηp2=.016) was observed. As depicted in Figure 6b, accuracy was reduced with Positive Framing, but increased with Familiarity. Contrast1 (Same vs. Other: F(1, 1216)=9.52, p=.002, ηp2=.008) and Contrast2 (Familiar vs. Unfamiliar: F(1, 1216)=9.84, p=.002, ηp2=.008) reached significance. Overall, participants frequency estimates were less accurate following positive framing (M=20.7%, SEM=0.74, 95% CIs [19.40, 22.32]) relative to negative framing (M=23.54%, SEM=0.74, 95% CIs [22.08, 25.00]). Framing did not interact with the main effect of Familiarity, or the orthogonal contrasts (all ps>.30). Full model output is included as Supplementary Materials 14.
Neither Framing nor Familiarity had any effect on frequency estimates of side effects of ‘unknown’ frequency (all ps>.16; see Supplementary Materials 15). Those in the Positive Framing conditions estimated that these side effects would be experienced by 1,848/100,000 people on average, and those in the Negative Frame as 2,004/100,000.
Discussion
Message framing has been suggested as a potential intervention to increase COVID-19 vaccine uptake14. In the present study, positive and negative attribute framing was applied to genuine side effect information from manufacturer PILs for three COVID-19 vaccines (AstraZeneca, Pfizer, Moderna). Booster intention was measured pre- and post-manipulation. Primary analysis revealed that positive framing successfully increased the intention to be vaccinated for unfamiliar vaccines (i.e., Moderna), but appeared to reduce booster intention for the vaccine that had previously been received, as well as for a switch to the Pfizer vaccine among those previously receiving AstraZeneca. In all cases, effects were strongest when baseline booster intentions were low. Increasing booster acceptance among those with low intentions is of substantial importance in protecting against infection from, and transmission of, COVID-19 viruses. Our data suggest that any intervention that intends to employ attribute framing should be carefully tailored to match the framed information (i.e., positive vs. negative wording) with vaccine familiarity. Specifically, positive framing appears to have significant potential when the vaccine is unfamiliar, such as in situations such when a novel vaccine is being introduced or there are composition changes to the vaccine28,29. By contrast, our data also suggest that positive framing may actually be harmful when the vaccine is familiar.
The significant effect of positive attribute framing on booster intentions for the Unfamiliar vaccine is consistent with research concerning medical decision making. In those studies, framed information has typically been presented regarding fictitious medications and patient scenarios25,27, 32–36. In other cases using real treatments, data has been collected from samples where participants were either completely17,43 or largely44 naïve to the framed treatment, or where prior treatment experience was not assessed18,45. The current data thereby provide new insights into the effect of framing. Under conditions directly relevant to the COVID-19 pandemic (i.e., for real vaccines, at high levels of public involvement), the benefit of positive attribute framing was found to wane, or in some instances to be reversed, as familiarity and prior experience with the framed vaccine increased. As such, calls for all PILs to employ positive framing as standard (e.g.,32,46) appear premature. Positive framing appears beneficial only for unfamiliar vaccines whereas negative framing, the standard form for communicating side effect information within the European Union, appears beneficial when treatments are well known.
The reduced efficacy of positive framing observed as vaccine familiarity increased could be explained by a current theory of attribute framing that posits an interaction between familiarity (a specific manifestation of psychological distance) and the valence of the message surrounding a given attribute or event (e.g., the experience of vaccine side effects). At closer psychological distances (e.g., for vaccines that are more familiar and more likely to be received), negatively framed information has been shown to be more persuasive47. Further experimental research is needed to test this theory, while also considering alternative explanations, such as the role of potential backfire effects in persuasive or corrective messaging that are known to impact attitudes surrounding the COVID-19 pandemic48 and have been demonstrated to lower intentions for other vaccine types at high levels of concern49. However, when assessed in conjunction, results presented here highlight the fact that any intervention that strives to apply positive framing across all vaccine types irrespective of familiarity should be treated with caution.
Perceived booster side effect severity, perceived booster risk, and booster acceptance (satisfaction, happiness, and anxiety) were examined as secondary variables to explore potential mediators of the effect of positive framing on booster intention. None of the patterns of these secondary variables mirrored the results obtained for the primary outcome – booster intention. Instead, positive framing appeared to have a more general capacity to increase favourable perceptions of the COVID-19 vaccines, decreasing perceptions of side effect severity, and increasing satisfaction and happiness in some instances. These results may appear difficult to reconcile with the observed changes in vaccine intention. However, post-hoc analysis (see Supplementary Materials 15) plotting the Familiarity*Framing*Baseline interaction on side effect severity and booster acceptance for those who had high vs. low baseline booster intent, suggests that framing-induced changes on these secondary variables largely occurred among those with high vaccine intention at baseline. Notably, participants with high baseline booster intentions showed limited effect of framing on their behavioural intention to be vaccinated. Thus, rather than being inconsistent with the primary outcome data, this exploratory pattern of results simply suggests that changes in booster intention with framing are unlikely to driven by changes in the perception of the COVID-19 vaccines as measured here. Investigation of other factors combined with qualitative research may be better positioned to identify the driving factors behind changes in booster intention that occur with the framing of COVID-19 vaccinations.
Estimates of side effect prevalence were found to be quite poor (<∼35% accuracy) after reading the information contained in the PILs, irrespective of frame. This is consistent with previous research39,50–53 and highlights limitations with the current format of communicating side effect information. It was interesting to note that an additional reduction in accuracy was also observed for the positive frame, which did not interact with familiarity. However, patterns within the data were inconsistent, with reduced accuracy associated with the Unfamiliar vaccine appearing exacerbated for verbal prevalence categories but ameliorated for frequency estimates. As such, it is unclear whether positive framing has the potential to undermine informed consent16 by reducing accuracy concerning side effect prevalence. Further, because the present study employed genuine PILs, the side effects participants were required to judge differed across vaccine types. As such, the study was designed only to test for general inaccuracies in side effect representation and not systematic over- or under-estimation. Experimental studies are therefore needed to assess precisely how any inaccuracies associated with positively framed COVID-19 vaccine information manifest.
The primary strength of the present study is the application of attribute framing to real COVID-19 vaccines with real PILs. The PILs employed here are displayed on government and NHS websites in the UK, forming a primary official source of information regarding COVID-19 vaccination. Our findings therefore have real-world implications, demonstrating that the wording of PILs can directly impact the intention to receive a booster vaccine among individuals for whom this decision is both directly relevant and imminent. There are of course some limitations worth noting including the collection of cross-sectional data that limits an assessment of the durability of the framing effect, as well as a sample located within a single country. Given global differences in booster policy, cross-cultural replication of results is required to ensure that the data presented here is not contextually limited to the UK. While vaccine intention has been demonstrated to be a strong predictor of vaccine uptake[e.g.,54–56], including for COVID-19 vaccination57, we do not assume that the two are synonymous58. While beyond the scope of the present study, we recommend that future research incorporate longitudinal designs where the rate of conversion from intention to vaccine uptake can be tracked. Further, the results presented here are specific to booster intentions among those already vaccinated. While side effect apprehension has been associated with hesitancy regarding COVID-19 vaccination11 and booster vaccination13, whether a similar pattern of results would hold among those who have never been vaccinated is unknown.
In summary, the present study demonstrates that the ability of positive framing to successfully increase booster intention for genuine COVID-19 vaccines is critically moderated by the familiarity of that vaccine. Positive framing can improve vaccine intention for unfamiliar vaccines, but may actually decrease intentions for familiar vaccines. The data therefore provide novel insights into the benefits of positive framing for COVID-19 vaccines and beyond. As such, we recommend that if positive attribute framing is to be employed, close attention must be paid to the type of treatment being framed as well as the likely recipients of the framed information. Importantly, in the context of the current COVID-19 pandemic, positive framing appears capable of improving uptake of COVID-19 vaccines when switches or new developments require individuals to receive unfamiliar vaccines, as is the case for many booster vaccine programmes globally, but should be treated with caution for familiar vaccines.
Methods
Recruitment and Sample
Recruitment took place in the initial weeks of the UK booster programme (27th October - 8th November 2021). Figure 3a provides a summary of the number of boosters administered in the UK at the time of data collection. The sample was obtained from Pureprofile, an ISO-certified panel provider for online research, and balanced on national quotas for age, gender, and region. All potential participants were screened using the following inclusion criteria: 18 years of age or older, currently residing in the UK, self-reported English fluency, previously received two doses of either the Pfizer or the AstraZeneca COVID-19 vaccines (no other combination), not having received a third COVID-19 booster vaccine, and no known medical reason (e.g., allergy) prohibiting potential administration of the Pfizer, AstraZeneca, or Moderna COVID-19 vaccines. After screening, 1896 participants provided electronic consent and 1459 completed the experiment. To reduce statistical noise due to random and inconsistent responding, 237 completing participants were removed based on pre-registered quality control criteria (see Supplementary Materials). The experiment was approved by the University of Sydney Human Research Ethics Committee. All completing participants were provided with an electronic debrief at the end of the survey and were paid £3.50 for a ∼15-minute survey.
Data Collection and Procedure
Cross-sectional data were collected online via Qualtrics, with the survey accessible to personal computer, tablet, and smartphone. The ‘force response’ option was used to ensure complete cases for all outcome variables. Participants completed the survey in one sitting and were not able to return to the study URL. After pre-screening, those meeting the inclusion criteria were provided with a participant information statement detailing the aims of the study and gave their digital informed consent. Those not meeting these criteria were directed away from the survey.
Participants completed demographic items and identified which COVID-19 vaccine they had previously received (AstraZeneca or Pfizer). Stratified randomisation to the six experimental groups occurred at this point using the inbuilt Qualtrics randomisation function. Quotas were set to limit data collection to 600 participants from each vaccine type (AstraZeneca/Pfizer), with 100 from each group randomised to the six experimental conditions. Because Qualtrics tallies quotas on survey completion but does not account for participants currently in the experimental pipeline, the final sample contained 22 more participants than projected. Statistical analysis did not take place until after exclusions had been made and all quotas were closed.
After randomisation, participants responded to items concerning the number of months since their last COVID-19 vaccine and familiarity with side effects of the three framed vaccines. For each vaccine type, participants then rated their booster intention, perceived booster side effect severity, perceived booster risk, and booster acceptance (satisfaction, happiness, and anxiety). Responses made to the vaccine type that matched with the experimental condition to which the participant had been assigned were employed as baseline measures. Responses to all other vaccine types were recorded for use in a concurrent, but separate, pre-registered study (#78370; aspredicted.org/8e6af.pdf). PILs containing the positively or negatively framed side effect information were then displayed for two minutes, using a timer embedded in the survey. Participants could not proceed until this time had elapsed. Post-manipulation booster intention, perceived booster side effect severity, perceived booster risk, and booster acceptance were then recorded. Finally, fourteen side effects described in the PILs were presented, with participants required to assign each to a verbal prevalence descriptor (very common, common, uncommon, rare, very rare) and estimate how many people (out of 100,000) taking the vaccine would experience the side effect. On completing the survey, all participants were provided with an electronic debrief for download and URLs to the UK government landing page where the original PILs for the vaccines used in the study could be found.
Several additional items concerning general COVID-19 booster intentions, perceived risk of previous COVID-19 vaccines, specific COVD-19 vaccination side effects, general perceptions of COVID-19 and COVID-19 vaccinations, and severity of previous COVID-19 infection, were included in the survey for use in a separate pre-registered study (#78370; aspredicted.org/8e6af.pdf), but are not analysed or reported on here.
Survey Materials
Demographic Information
Participants responded to items concerning their age, gender, ethnicity, highest level of education and employment status, and geographic region (postal area code). Exact wording can be found in the Demographic Information section, Supplementary Materials 4.
Previous exposure to COVID-19
Items were employed to capture personal exposure to COVID-19, as well as exposure through close friends and family. Item wording (To your knowledge, are you, or have you been, infected with COVID-19? / To your knowledge, have any of your close family members or friends been infected with COVID-19?) was taken from the WHO BeSD documentation14.
Previous COVID-19 Vaccination History
Previous COVID-19 vaccine (Pfizer/AstraZeneca) was recorded as a forced-choice option. Participants indicated the number of months since their last COVID-19 vaccine, and whether their most severe side effects occurred to their first dose, second dose, whether they were equal across doses, or not experienced at all.
Familiarity with COVID-19 vaccine side effects
For the three framed vaccines, participants were asked to rate their “familiarity with the potential side effects” on a 100-point VAS, with anchor labels (’not at all familiar’ / ’extremely familiar’) positioned to the left and right of the scale. Those who had not heard of the vaccine were asked to check a separate ‘not heard of vaccine’ box but received a score of zero (not at all familiar). This response-type was used to exclude inconsistent responders (see Supplementary Materials 1).
Baseline Measures: COVID-19 Vaccine Perceptions
Four items were used as baseline measures. All were rated on a 100-point VAS. For each of the three vaccines, participants responded to questions concerning: 1) booster intention ‘If you were offered [vaccine type] as a booster vaccine to maintain protection against COVID-19 viruses, how likely would you be to accept?’ (labels: ‘definitely would not accept vaccine’ vs. ‘definitely would accept vaccine’); 2) perceived booster side effect severity ‘Overall, how severe do you think the [vaccine type] side effects are?’ (labels: ‘not at all severe’ vs. ‘extremely severe’); 3) perceived booster risk ‘What do you think the risk to your health would be if you received [vaccine type] as a booster vaccine, bearing in mind its side effects?’ (labels: ‘extremely low risk’ vs. ‘extremely high risk’); 4) booster switch perceptions ‘Imagine that switching to the [vaccine type] vaccine was your only option for a booster. Please rate how satisfied, happy, and anxious, you would be with this outcome’ (labels: ‘not at all’ vs. ‘extremely’). Satisfaction, happiness, and anxiety were rated as sub-items, each yielding a score of 0 – 100. Where the vaccine type was the same as that previously received by the participant, wording was changed from ‘switching to’ to ‘continuing with’. Wording of 1 – 3 was adapted from previous research39.
Patient Information Leaflets (PILs): Experimental Manipulation
Genuine PILs for the AstraZeneca, Pfizer, and Moderna vaccine were abridged to include the manufacturer’s description of each vaccine, what it is used for, and critically, the possible side effects resulting from administration. Side effects were retained in their original form and order. For both the negatively and positively framed PILs, verbal descriptors were in keeping with those published by the manufacturer (i.e., very common, common, uncommon, rare, very rare, not known). Wording of assigned frequency bands employed in the negatively framed PILs was also identical to that of the manufacturer. However, this was inverted in the positively framed PILs to stress the number of individuals not affected (e.g., “Common (90 in 100 or more people may not be affected)”). As multi-modal forms of side effect presentation (e.g., written, pictorial, verbal) may elicit larger framing effects16, and numeracy is less likely to moderate the effect of attribute framing for graphical presentations59, positive PILs additionally included a graphical representation of side effect risk to enhance the manipulation. For an example of the wording used to frame side effects see Figure 2.
Post-Manipulation Measures: COVID-19 Vaccine Perceptions
Participants responded to the four vaccine perception items listed above under Baseline Measures (booster intention, booster side effect severity, booster risk, booster acceptance), but only in relation to the vaccine type outlined in the PIL to which they were assigned.
Post-Manipulation Side Effect Perceptions
To determine whether positive framing augments the perception of side effect occurrence relative to true prevalence rates, fourteen side effects were presented from each PIL. Eleven of these were associated with concrete prevalence brackets in the original PILs, while the remaining three were assigned to the ‘unknown’ category (i.e., could not be estimated at the time of PIL publication). For each side effect, participants were required to identify the correct verbal descriptor (very common, common, uncommon, rare, very rare): “based on the information that you read, how common do you think [side effect] is?” (forced-choice answer). They were then asked, “In 100,000 people, how many do you think would experience [side effect] if they received a [framed vaccine name] booster vaccine?” (free-response, limited to numbers at up to 10 decimal places). The three ‘unknown’ side effects were analysed separately to determine the effect of framing when prevalence rates are not provided.
Statistical Analysis
Statistical analysis was performed using R (version 4.1.1). Statistical analyses were a combination of ANCOVAs (where baseline measures were available) or ANOVAs, reported with Type III Sum of Squares. An alpha of .05 was accepted as the threshold for statistical significance. Sample size (estimated N=1200) was calculated based on an a priori power analysis (95% power, alpha=.05, effect size f2=0.02) for a separate study run concurrently that contained more predictor variables (N=9), and therefore required more power, than the study presented here (further details are contained in the study pre-registration form). An effect size for attribute framing was additionally derived from previous research (average effect size r= 0.175)16. An a priori power analysis based on this effect size required a total of 491 participants, providing reassurance that the projected sample size for the study above provided ample power to detect an effect of framing in the present study.
Data Availability
All data produced are available online through the Open Science Framework repository
https://osf.io/d5cvn/?view_only=cb90eca9ddf446c8901652ab0344fa05
Sources of Funding
This research was supported by Australian Research Council grants DP180102061 and DP200101748. The funding body had no involvement in study design, analysis, interpretation, writing, or the decision to submit the present article for publication.
Data Availability
The code and raw data necessary to replicate the reported analysis is available through the Open Science Framework repository (means/SEMs needed to reproduce the analysis figures are included with the raw data): https://osf.io/d5cvn/?view_only=500c83d90bb9416796e464108ad2fc41
Author contributions
KB and BC conceived the experimental design. KB was responsible for collecting and analysing the data. KB wrote the first draft of the article. BC edited and contributed to the final version.
Acknowledgements
References



