
Abstract
Introduction Low back pain (LBP) is a major cause of disability and is progressively becoming worse on a global scale. [1,2] The prevention and rehabilitation of LBP lacks clarity in part due to the heterogeneity of the exercise programs prescribed to treat low back pain. Some authors have proposed stabilizing exercises for lower back pain which exert minimal loads on the spine. [3,4,5] Despite a multitude of existing exercise therapies, McGill has introduced three exercises for rehabilitating lower back pain, termed the McGill Big Three (MGB3). [6,7,8,9,10] These include the curl-up, side plank and bird-dog. The purpose of this review is to investigate the clinical outcomes from prescribing the MGB3 to individuals with chronic LBP.
Methods Inclusion criteria were randomized control trials that involved an intervention with MGB3 core stabilization exercises for patients with chronic low back pain. The research included articles published during any period in full English text. Studies were critically reviewed by two authors EL and GG independently and collaboratively.
Results In total, four randomized control trials were included in this review. Multiple cohorts, with varying age, demographics and occupation were studied. Outcomes studied included various pain scores, patient reported functional and performance measures.
Discussion Controlled clinical trials employing this method in low back pain treatment showed low quality data with mixed statistical significance, and little to no clinical significance irrespective of the measure used or even when compared to baseline. Limitations of these trials are detailed herein.
Conclusion Currently there is limited data supporting the clinical benefit of the McGill approach for the treatment of low back pain based on the available randomized clinical trials. More study is required prior to widespread adoption into clinical practice.
Introduction
Chronic low back pain (LBP), generally referred to as pain or stiffness in the lumbar region of the spine lasting a minimum of 12 weeks, is among the leading causes of disability globally. [11,12,13,14,15, 16,17] LBP poses an increasing medical and economic burden, attributable primarily to treatments costs and decreased work productivity. [1,2] The point prevalence and lifetime prevalence of LBP among the Canadian population is 28.4% and 84.1%, respectively. [18,19] The prevalence of chronic back issues within the Canadian Armed Forces (CAF) is 16%, and LBP specifically accounts for 12% of medical releases each year. [20, 21]
Mechanical LBP is hypothesized to occur from anatomical structures such as the muscles, ligaments, bones, joints, spinal nerve roots, intervertebral discs and abdominal organs. [22,23,24] Associated precursors for mechanical LBP can include traumatic injury, structural abnormalities, pregnancy, infection, inflammatory disorders, degenerative conditions, disc herniation, radiculopathy and spinal stenosis. [25,26] Risk factors for LBP may include specific types of repetitive spinal motion, low socioeconomic status, medical and psychiatric comorbidities, and inadequate coping mechanisms. [15,27, 28,29] There is also emerging evidence indicating LBP is not only a regional issue given the studies supporting altered cerebral functional gray and white matter in patients, although the directionality and temporality have yet to be established. [30] Treatments include but are not limited to pharmaceuticals, exercise therapy, manual therapies, injections and surgery. [15,25,31,32]
Possibly owing to the various underlying causes of LBP, heterogeneity of evaluation tools and measures of success, some authors argue it is nearly impossible to formulate standardized exercise interventions to treat chronic LBP. [5,6,25,33,34]. However, within prescribed exercise therapies for LBP, core stabilization exercises have gained increased attention over the recent decade. [5,35,36,37] This type of exercise therapy has evolved into a mainstay for treating chronic LBP with focus on core stabilization and muscle coordination. [3,38,39,40,41,42,43]
Spinal stability is theorized to be an integration of active muscle contraction, passive ligament support and neural control. [39,40,42] Active muscle control can be further classified into local (i.e., segmental stability) and global stabilizers and dynamic control. [39,42,43]. Core stabilizing exercises train patterns of muscle activity and posture without producing excessive loading of the spine. [44,45] Stability is determined by various motor patterns that differ in aspects such as demand, load and speed. [45]
Therefore, it is of great interest to validate the most clinically effective rehabilitation program for individuals with LBP. Various approaches have been studied including generalized flexibility, variable load anterior/posterior muscle training, along with the low to no load lumbo-pelvic region based on the global muscle stabilization described by McGill. [40,41,42,43] Based on numerous biomechanical and clinical studies, McGill has proposed stabilizing exercises which apply minimal loads on the spine to reduce and prevent LBP. [3] This includes tailored programs built around three exercises termed the “McGill Big Three” (MGB3) which include the curl-up, side plank and bird-dog (please see Figure 1 for examples of these exercises). [10]
Figure 1.1. Curl-up
Pls see https://www.healthaya.com/publications
Figure 1.2. Side-plank
Pls see https://www.healthaya.com/publications
Figure 1.3. Bird-dog
In order to further delineate the clinical impact of the McGill approach in the treatment of chronic low back pain, we undertook a review of the existing literature. To our knowledge this systematic evaluation has not been completed thus far.
Methods
A review of the literature was completed using the following search terms: McGill stabilization exercises, McGill Big Three, MGB3, low back pain (LBP), Stuart McGill, chronic low back pain (LBP), core stabilizing exercises. The PubMed, Ovid Medline, Embase and Google Scholar electronic databases were used. References of existing articles were inspected to identify additional relevant studies. Inclusion criteria were randomized control trials that involved an intervention with MGB3 core stabilization exercises for patients with chronic low back pain. The research included articles published during any period in full English text. Studies were critically reviewed by two authors EL and GG independently and collaboratively.
For the analysis, between group differences were calculated by using the absolute differences for various performance measures and patient reported pain and functional outcomes. For instance, if mean pain scores in the control group decreased from 8/10 to 4/10, this was considered to be a 40 percent improvement (not 50%), which was subsequently subtracted from the corresponding measure in the treatment group. Where range of motion was used, the total possible score was calculated using a maximum of 20 degrees of extension and 40 degrees of flexion, for a total range of motion of degrees [46]. Percentage improvement was calculated against degrees improvement divided by 60 degrees. One study provided mean scores using several graphs. [48] Percentage improvement for this study was therefore calculated from estimated scores. Finally, where multiple performance measures were used, the measure with a total possible maximum score was used. [3,43,47,48] A positive score represents an effect favoring the McGill approach for a given study. A trial reporting performance measures using covariate analysis was excluded from the analysis as the corresponding author was unable to provide mean scores. [3]
Results
In total, four randomized control studies satisfied the inclusion criteria. [3,43,47,48] 170 participants were recruited from the four studies with 23 lost to follow up. Participants ranged from 20 to 60 years of age. Plausible confounding variables including gender, age, weight and height were recorded in all studies, and the assessors were blinded to treatment allocation with the exception of Ghorbanpour et al. 2018. Ammar et al. 2011 recruited only postnatal female participants and Chan et al. 2020 recruited male military participants only.
Chan et al. 2020 provided 5 weeks of pre-trial passive pain treatment with heat and transcutaneous electrical stimulation (TENS). Ammar 2012 provided heat to all participants, while Ammar et. al 2011 provided heat to the control group only. No studies used non-treatment control groups, and protocols for the prescribed exercises varied with respect to type of exercises, duration, and intensity of exercises for both groups. Furthermore, the McGill stabilization exercises were not uniform throughout each study as Ghorbanpour et. al 2012 and Chan et al. 2020 focused only on the MGB3, while Ammar 2012 and Ammar et. al 2011 employed McGill stabilization exercises beyond the MGB3. [3,47,48,43] Treatment outcomes were measured at 4 or 6 weeks depending on the trial, and no longer-term measures were assessed in any trial. [3,43,47,48]
Two studies, Ammar et al. 2011 and Ammar 2012 monitored compliance using patient reported logs and were the only studies that showed statistical differences for outcomes between groups. Ammar et. al 2011 insufficiently differentiated groups, and mean scores and standard deviations for outcomes were identical for one group suggesting a possibility of error in the results. Ghorbanpour et al 2018 appear to have errors when reporting mean difference which were adjusted for in our analysis. Chan et al. 2020 was the only study conducted with a therapist present for all sessions. The same study provided a power analysis to justify recruitment and accounted for dropouts in their analysis. When looking at the relative improvements between groups, pain, function and performance scores saw an improvement of <10% across the studies, with the exception of Chan et. al which saw an improvement of 15% for pain scores. Table 1 describes the specifics of the studies while Figure 2 details the comparative differences between studies on select outcome measures.

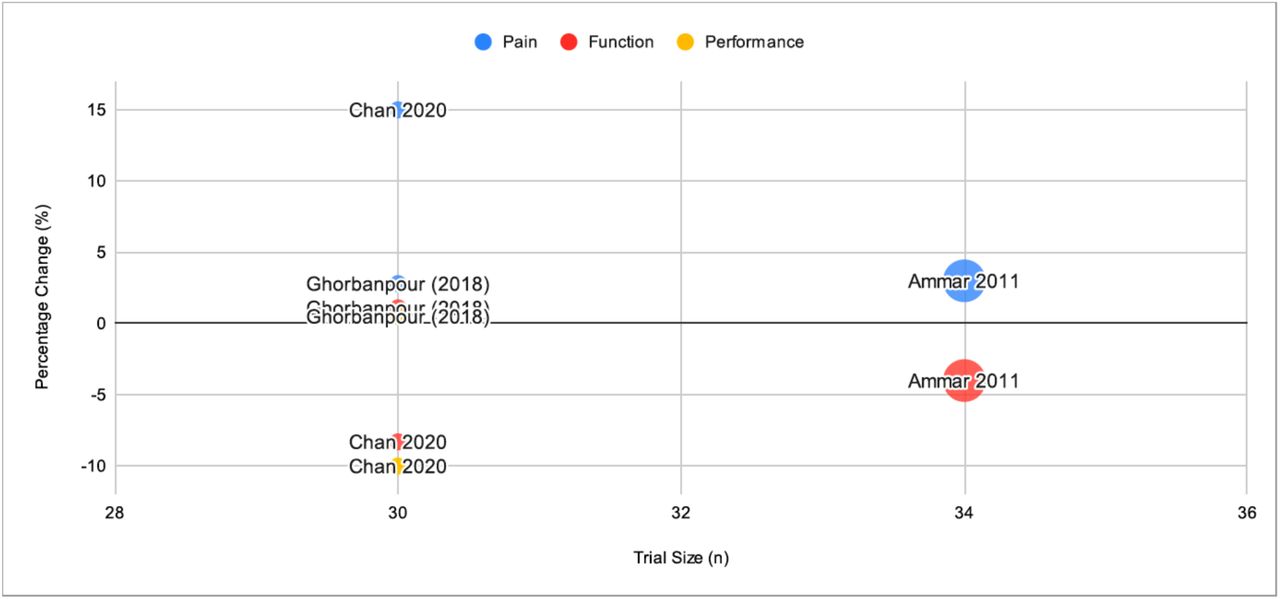{kind=link}
Note: Bubble size also represents total trial size
Discussion
Core stability training continues to be widely employed in therapy of LBP and injury prevention. The goal of this training is to stabilize the lumbopelvic region in a neutral state when performing spine-loading tasks by re-educating postural core muscles such as the transverse abdominis, multifidi, and pelvic floor muscles. It is hypothesized that this will provide segmental stability and control of the lumbar spinal segments during activity. [49, 50, 51]
There have been multiple studies looking at various types of core strengthening programs on pain and disability with mixed results. [47] As described, the McGill approach is one type of core strengthening program that incorporates the abdominal bracing strategy to recruit high trunk muscle activity with low spinal loads on the spine. [51] This review of the available randomized controlled clinical trials employing this method in low back pain treatment showed low quality data with mixed statistical significance, and little to no clinical significance irrespective of the measure used or even when compared to baseline. Limitations of these trials are detailed in Table 2. Practical limitations of the review include the exclusion of background biomechanical and cohort studies of the McGill approach, as well as the inclusion of other core strengthening approaches. This can certainly be considered in the future given the limited quality of the data available. Further investigation could consider 1) further comparing McGill or other stabilization programs to other conventional physical therapies 2) looking at these treatments alongside other types of treatments of low back pain 3) longer duration studies with carefully selected patients and robust treatment protocols and 4) impact on resource healthcare utilization and care seeking.
Conclusion
Currently there is limited data supporting the clinical benefit of the McGill approach for the treatment of low back pain based on the available randomized clinical trials. Further studies are required to verify the treatment efficacy prior to widespread adoption into clinical practice.
Disclaimer
The views expressed herein are those of the author and may not reflect those of the Canadian Armed Forces, Canadian Forces Health Services, the Department of National Defense or the Canadian Government.
Data Availability
All data produced in the present work are contained in the manuscript
Acknowledgements
We would like to thank Major Pauline Godsell and Captain Nicole Mahoney for their feedback and support on this project.
References



