
Abstract
The SARS-CoV-2 Omicron variant has a growth advantage over the Delta variant, due to higher transmissibility, immune evasion, or a shorter serial interval. Using S-gene target failure (SGTF) as indication for Omicron, we identify 220 SGTF and 869 non-SGTF serial intervals in the same week. Within households, we find a mean serial interval of 3.4 days for SGTF and 3.9 days for non-SGTF cases. This suggests that the growth advantage of Omicron is partly due to a shorter serial interval.
The SARS-CoV-2 Pango lineage B.1.1.529, also known as the Omicron variant, was first reported by South Africa on 24 November 2021, and designated by the WHO as a variant of concern on 26 November 2021 (1). It is characterized by a fast epidemic growth relative to the B.1.617.2 (Delta) variant (2). Several epidemiological factors may contribute to the fast relative growth rate of this new variant. Firstly, immune evasion (3-5). Secondly, higher intrinsic transmission potential (6) (an increase in the basic reproduction number, defined as the average number of secondary cases generated by an infectious individual in a susceptible population). Thirdly, a shorter serial interval (i.e., the duration of time between symptom onset of a case and its infector). A variant with a shorter serial interval as compared to another variant with the same reproduction number, would have an increased epidemic growth rate. Whereas early reports provide evidence for substantial immune evasion and suggest an increased transmission potential (3-6), little is known about the serial interval of the Omicron variant. We assess whether the serial intervals of the Omicron and Delta variant differ by comparing transmission pairs of both variants during the same time period.
The Omicron variant was first identified in the Netherlands in a case whose sample was obtained on November 19, 2021. Symptom onset dates and postal codes of diagnosed SARS-CoV-2 cases are reported to a national surveillance database. If an infector of the case has been identified through source and contact tracing, a unique identifier of this infector is reported as well. We identified pairs of a primary case and a secondary case from this national surveillance database and measured the serial interval as difference between symptom onset day of a case and its infector.
A fraction of the cases reported in the national surveillance database were tested in two laboratories that analyze specimens with the TaqPath COVID-19 RT-PCR Kit (ThermoFisher Scientific). This PCR kit targets three genes. Failure of the probe targeting the S-gene, while the Orf1ab and N probe result in a proper signal (S-gene target failure (SGTF), also referred to as S-dropout), identifies the presence of a deletion in the S-gene (spike amino acid residues Δ69–70) which has been associated with the Omicron variant but not with Delta. Non-SGTF is highly predictive of the Delta variant and SGTF is highly predictive for the Omicron variant (4). With lower viral loads SGTF allocation is less accurate as the S-gene target is the least sensitive target of the three genes. Therefore, a stringent threshold of ≤ 30 cycle threshold (Ct) values were used on the Orf1ab and N targets for inclusion in further analyses.
We included transmission pairs with a minimum serial interval of -5 days and a maximum serial interval of 15 days. We included transmission pairs with a symptom onset date for the infector between December 13 and December 19, 2021, as reported by January 6, 2022. The overall share of Omicron variant detected in test positive cases was 9.0% during this period (7). A cohort approach was followed to minimize the impact of data truncation and differences in epidemic growth by variant on the outcome. Analysis showed that most cases were tested and reported within five days after symptom onset. Combined with a maximum serial interval of 15 days, this would mean that a secondary case of the cohort would be tested and reported at the time the data were retrieved from the notification system. We excluded transmission pairs where infector or case had a missing postal code, where both infector and case lacked SGTF results, or where infector and case had differing SGTF results.
We will refer to transmission pairs with an SGTF case or an SGTF infector as SGTF transmission pairs, and to transmission pairs with a non-SGTF case or a non-SGTF infector as non-SGTF transmission pairs. We will refer to transmission pairs with a case and infector with the same postal code as within-household transmission pairs, and to transmissions with a case and infector with a different postal case as between-household transmission pairs, because 97% of transmission pairs with identical postal code live within the same household (8).
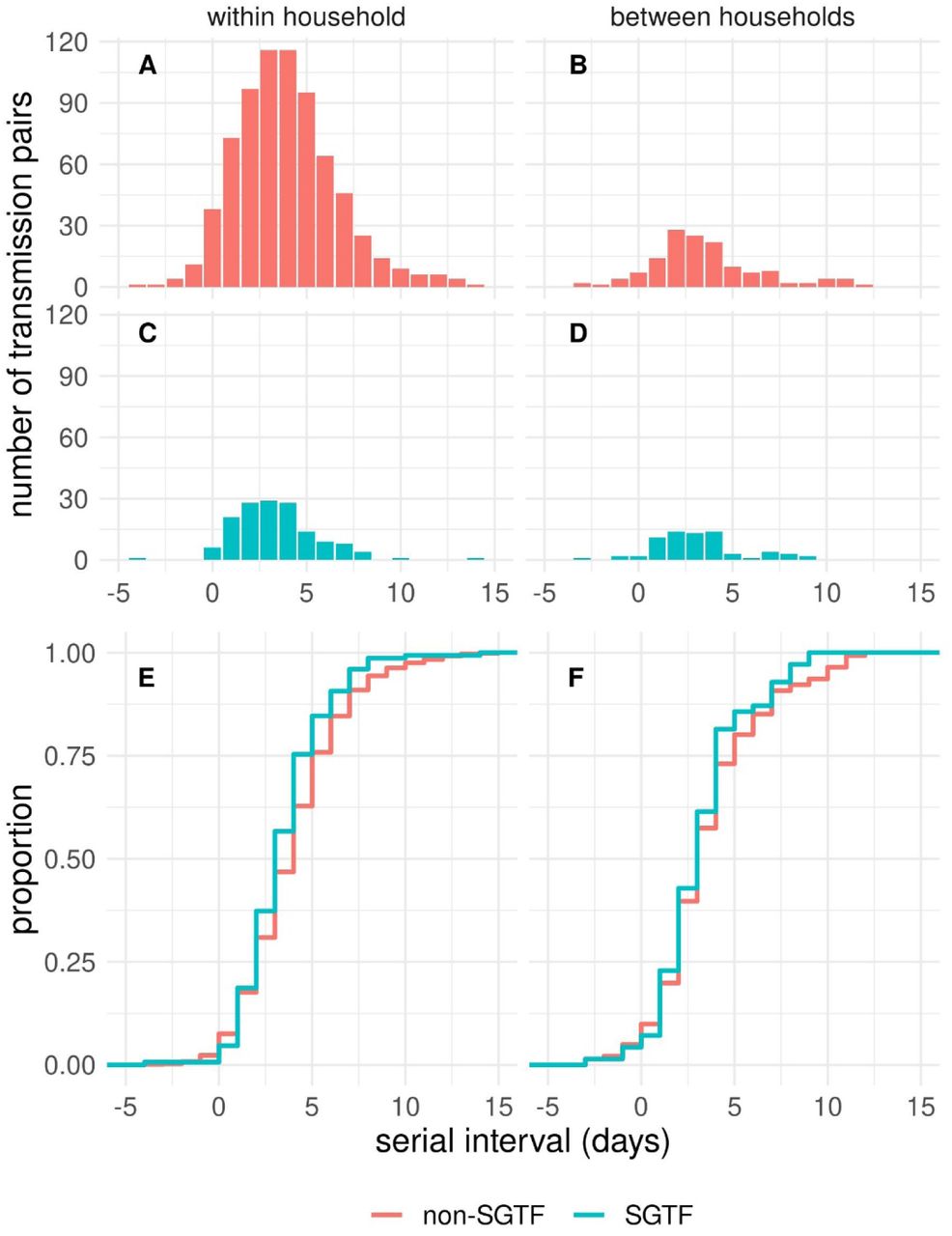
We identified 220 SGTF transmission pairs, and 869 non-SGTF transmission pairs (i.e., 20% of all transmission pairs identified in the study week), excluding 11 pairs with opposing SGTF results, and 6 pairs without postal code. The mean serial interval of 3.4 days for the 150 SGTF within-household pairs was significantly shorter than the mean serial interval of 3.9 days for the 728 non-SGTF within-household pairs (Figure 1, one-sided Welch’s test, df = 247, p = 0.0044). A similar but not significant difference was found between the mean serial interval of 3.1 days for the 70 SGTF between-household pairs and the mean serial interval of 3.5 days for the 141 non-SGTF between-household pairs (one-sided Welch’s test, df = 165, p = 0.15).

Observed distribution of serial interval of SARS-CoV-2 transmission pairs with infectors having their symptom onset date during the period 13 - 19 December 2021 in The Netherlands, (A) for non-SGTF within-household transmission pairs, (B) non-SGTF between-household transmission pairs, (C) SGTF within-household transmission pairs, (D) SGTF between-household transmission pairs, and the difference between the empirical cumulative density functions for SGTF and non-SGTF transmission pairs (E) within households and (F) between households (see Appendix for data).
In addition to the transmission pairs, we studied cases with known exposure information that allows to infer the incubation period (9). We identified 117 SGTF cases and 163 non-SGTF cases with reported symptom onset date between 1 and 26 December 2021 (i.e., 13% of all cases with known exposure information in that period). The median incubation period is estimated to be 3.4 days for SGTF cases and 4.0 days for non-SGTF cases, but the 95% posterior distribution of the difference includes 0 (see Appendix).
This early investigation of recent SGTF cases as a proxy for Omicron, offers evidence to support a shorter serial interval among the identified cases studied. This lends support to the hypothesis that the recent rapid growth of the Omicron variant is in part driven by a shortened serial interval as compared to infections with the Delta variant. The observed difference of half a day is similar to the difference in the incubation period between the two variants.
During the study period the contact tracing guidelines differed for the two variants regarding contacts outside the household. Until 23 December 2021 guidelines for the Omicron variant were stricter than for Delta infections, with longer isolation and quarantine periods and requiring quarantine also for immune contacts. These differences might offer a possible explanation for the observed shorter serial interval of the SGTF transmission pairs between households. However, these differences do not explain for the observed shorter serial interval of the SGTF transmission pairs within households and the shorter incubation period of SGTF cases. Therefore, the observed difference in between-household pairs is expected to be due to the variant. To generalize the observed differences between serial interval for SGTF and non-SGTF transmission pairs, proper control for the control measures in place and other confounding factors such as age and vaccination status of the case and its infector are required.
The reported values of mean serial interval and median incubation period for the Omicron variant are in line with earlier reported tentative estimates. A mean serial interval of 2.8 days (range 1-7 days) for Omicron was reported for outbreaks in South Korea (10). A median incubation period of 3 days for Omicron was reported for a superspreading event in Norway (11) and for a cluster in Nebraska (12). Although none of these earlier reports allowed for a direct comparison between the reported values for the mean serial interval and the median incubation period between the Omicron and Delta variant in the same period, the reported low values suggest that also in these different settings the serial interval and the incubation time of the Omicron variant are shorter than those for the Delta variant.
There are indications for a different place of replication and a different route of entry for the Omicron variant, which suggests a mechanism to account for a shorter serial interval and a shorter incubation period (6, 13). Further studies that include the viral load and shedding dynamics relative to the symptom onset date of the primary case are crucial.
A short serial interval offers, next to immune evasion and higher transmissibility, an explanation for the growth advantage of the Omicron variant over the Delta variant. A short serial interval and a short incubation period will make timely contact tracing more challenging, which will have a negative impact on reducing onward transmission (14). Mitigating the observed rapid spread of the new virus variant will therefore continue to require multi-layered interventions such as case finding and contact tracing, as well as booster vaccination and non-pharmaceutical interventions.
Data Availability
All data produced in the present work are contained in the manuscript
Funding
The study was financed by the Netherlands Ministry of Health, Welfare and Sport. This project has received funding from the European Union’s Horizon 2020 research and innovation programme - project EpiPose (grant agreement number 101003688).
Appendix
Data
Number of observed transmission pairs by serial interval, type (within or between households) and SGTF result; data shown in Figure 1 in main text.
Incubation period
For 117 SGTF cases and 163 non-SGTF cases, with a symptom onset date between 1 and 26 December 2021, the exposure window and symptom onset are reported. Assuming a Weibull distribution for the incubation period, the parameters are estimated using a previously published method (9). The incubation period for SGTF cases seems slightly shorter than for non-SGTF cases (Fig. S1 and Tab. S2) but the credible intervals are largely overlapping.

{kind=link}
{kind=link}
Estimated cumulative density function of the incubation period for 163 non-SGTF cases and 117 SGTF cases, with a symptom onset date between 1 and 26 December 2021.
Posterior parameter estimates for Weibull distributed incubation period, based on 163 non-SGTF cases and 117 SGTF cases.



