
Abstract
Background The Omicron SARS-CoV-2 variant is responsible for a major wave of COVID-19, with record case counts reflecting high transmissibility and escape from prior immunity. Defining the time course of Omicron viral proliferation and clearance is crucial to inform isolation protocols aiming to minimize disease spread.
Methods We obtained longitudinal, quantitative RT-qPCR test results using combined anterior nares and oropharyngeal samples (n = 10,324) collected between July 5th, 2021 and January 10th, 2022 from the National Basketball Association’s (NBA) occupational health program. We quantified the fraction of tests with PCR cycle threshold (Ct) values <30, chosen as a proxy for potential infectivity and antigen test positivity, on each day after first detection of suspected and confirmed Omicron infections, stratified by individuals detected under frequent testing protocols and those detected due to symptom onset or concern for contact with an infected individual. We quantified the duration of viral proliferation, clearance rate, and peak viral concentration for individuals with acute Omicron and Delta variant SARS-CoV-2 infections.
Results A total of 97 infections were confirmed or suspected to be from the Omicron variant and 107 from the Delta variant. Of 27 Omicron-infected individuals testing positive ≤ 1 day after a previous negative or inconclusive test, 52.0% (13/25) were PCR positive with Ct values <30 at day 5, 25.0% (6/24) at day 6, and 13.0% (3/23) on day 7 post detection. Of 70 Omicron-infected individuals detected ≥ 2 days after a previous negative or inconclusive test, 39.1% (25/64) were PCR positive with Ct values <30 at day 5, 33.3% (21/63) at day 6, and 22.2% (14/63) on day 7 post detection. Overall, Omicron infections featured a mean duration of 9.87 days (95% CI 8.83-10.9) relative to 10.9 days (95% CI 9.41-12.4) for Delta infections. The peak viral RNA based on Ct values was lower for Omicron infections than for Delta infections (Ct 23.3, 95% CI 22.4-24.3 for Omicron; Ct 20.5, 95% CI 19.2-21.8 for Delta) and the clearance phase was shorter for Omicron infections (5.35 days, 95% CI 4.78-6.00 for Omicron; 6.23 days, 95% CI 5.43-7.17 for Delta), though the rate of clearance was similar (3.13 Ct/day, 95% CI 2.75-3.54 for Omicron; 3.15 Ct/day, 95% CI 2.69-3.64 for Delta).
Conclusions While Omicron infections feature lower peak viral RNA and a shorter clearance phase than Delta infections on average, it is unclear to what extent these differences are attributable to more immunity in this largely vaccinated population or intrinsic characteristics of the Omicron variant. Further, these results suggest that Omicron’s infectiousness may not be explained by higher viral load measured in the nose and mouth by RT-PCR. The substantial fraction of individuals with Ct values <30 at days 5 of infection, particularly in those detected due to symptom onset or concern for contact with an infected individual, underscores the heterogeneity of the infectious period, with implications for isolation policies.
Introduction
SARS-CoV-2 viral dynamics differ by variant and by the immune status of infected individuals, but data on the Omicron variant have been lacking, especially for viral abundance and clearance relative to other SARS-CoV-2 variants. The Omicron variant features enhanced inherent transmissibility1, less severe disease2, partial immune escape3–5 and a potentially shorter generation interval6,7 relative to previous variants, necessitating the reevaluation of policies for testing and isolation. Such policies may be informed by an understanding of the degree and duration of viral shedding during an infection with Omicron. A useful proxy for viral shedding is viral RNA8, measurable by PCR, recognizing that the relationship between viral RNA, intact virus, and infectiousness may be influenced by a number of factors, including the variant, phase of infection (proliferation vs clearance), the anatomical site tested by PCR, and the extent of immune response.
We sought to describe SARS-CoV-2 Omicron variant viral dynamics in individual infections. To do so, we collected and analyzed a longitudinal set of 10,324 SARS-CoV-2 viral samples obtained from 537 participants as part of the occupational health program of the National Basketball Association (NBA) between July 5th, 2021, and January 10th, 2022. This program consists of a mix of frequent (daily) testing as well as testing triggered by COVID-19 symptoms and concern for contact with infected individuals. Cases detected in this way bear similarities to Omicron cases routinely detected in the general population, and thus these results can help inform optimal isolation durations and testing strategies.
Methods
Study design
The data reported here represent a convenience sample including team staff, players, arena staff, and others affiliated with the NBA. The retrospective study includes samples collected between July 5th, 2021, and January 10th, 2022. Clinical samples were obtained by combined swabs of the anterior nares and oropharynx for each patient administered by a trained provider. Viral load was measured using the cycle threshold (Ct) according to the Roche cobas target 1 assay. Ct values were converted to viral genome equivalents using a standard curve9. Vaccination information was reported and verified by NBA staff and clinical operational team.
Study oversight
In accordance with the guidelines of the Yale Human Investigations Committee, this work with de-identified samples was approved for research not involving human subjects by the Yale Institutional Review Board (HIC protocol # 2000028599). This project was designated exempt by the Harvard Institutional Review Board (IRB20-1407).
Study participants
We tagged each series of positive tests buffered by at least 14 days of negative or missing tests on each side as a distinct infection. Positive samples were tested with an additional RT-qPCR assay to initially differentiate between Delta and Omicron by the presence or absence of S-gene detection spanning the S 69/70 deletion found in Omicron lineage BA.1 (the dominant Omicron lineage)10. Results with an S-gene target failure were marked as suspected Omicron, and some lineages were confirmed by sequencing. The cases used in this analysis include 107 infections with Delta and 97 with Omicron (49 confirmed by sequencing + 48 suspected by S-gene target failure). Note that although the Alpha variant is also subject to S-gene target failure, given the time period of the study these samples were likely of Omicron. To quantify key viral kinetics parameters using a previously described modeling framework11,12, we further subset the data to 55 Delta and 84 Omicron infections (46 confirmed + 38 suspected) based on the following additional criteria: individuals with at least three positive PCR tests (Ct <40), at least one test with Ct <32, and at least one negative PCR test.
Study outcomes
For all distinct infections with Omicron (n=97) or Delta (n=107), we determined the percentage with Ct values <30, a threshold chosen based on a combination of antigen sensitivity and studies of virus culture by Ct, where the presence of culturable virus is often assumed to correlate with infectivity13–17, by number of days post detection by positive RT-qPCR test, stratifying by those who had a negative or inconclusive test ≤ 1 day prior to detection and those whose last negative or inconclusive test was ≥ 2 days ago. For the purposes of calculating these percentages, we assumed that individuals testing negative at the end of an acute infection remained negative for the remainder of the study period, whereas those ending in a positive test are right-censored. Inconclusive tests are those with a detectable Ct value to E but not ORF1a/b. Here we focus on Ct values to ORF1a/b, and thus group these inconclusive tests with negatives; we evaluate including them instead as positive in a sensitivity analysis. We also performed a sensitivity analysis using a cutoff of Ct <25. We quantified the viral proliferation duration (time from first possible detection to peak viral concentration), the viral clearance duration (time from peak viral concentration to clearance of acute infection), the duration of acute infection (proliferation duration plus clearance duration), and the peak viral concentration for each person. We determined the population mean values of these quantities separately for Delta infections (n = 55) and Omicron infections (n = 84).
Genome sequencing and lineage assignments
RNA was extracted and confirmed as SARS-CoV-2 positive by RT-qPCR10. Next Generation Sequencing was performed with the Illumina COVIDSeq ARTIC viral amplification primer set (V4, 384 samples, cat# 20065135). Library preparation was performed using the amplicon-based Illumina COVIDseq Test v033 and sequenced 2×74 on Illumina NextSeq 550 following the protocol as described in Illumina’s documentation. The resulting FASTQs were processed and analyzed on Illumina BaseSpace Labs using the Illumina DRAGEN COVID Lineage Application;18 versions included are 3.5.0, 3.5.1, 3.5.2, 3.5.3 and 3.5.4. The DRAGEN COVID Lineage pipeline was run with default parameters recommended by Illumina. Lineage assignment and phylogenetics analysis using the most updated version of Pangolin19 and NextClade20, respectively. All sequenced Omicron infections (n=49) were lineage BA.1. Sequenced Delta infections were a combination of lineages B.1.617.2 and AY.x.
Statistical analysis
Following previously described methods9,12, we used a Bayesian hierarchical model to estimate the proliferation duration, clearance duration, and peak viral concentration for each person and for the sub-populations of interest. The model describes the log10 viral concentration during an acute infection using a continuous piecewise-linear curve with control points that specify the time of acute infection onset, the time and magnitude of peak viral concentration, and the time of acute infection clearance. The assumption of piecewise linearity is equivalent to assuming exponential viral growth during the proliferation period followed by exponential viral decay during the clearance period. The control points were inferred using the Hamiltonian Monte Carlo algorithm as implemented in Stan (version 2.24). We used priors informed by a previous analysis9,12 for the main analysis and conducted a sensitivity analysis using vague priors as well as a strongly biased set of priors to assess robustness to the choice of prior.
Results
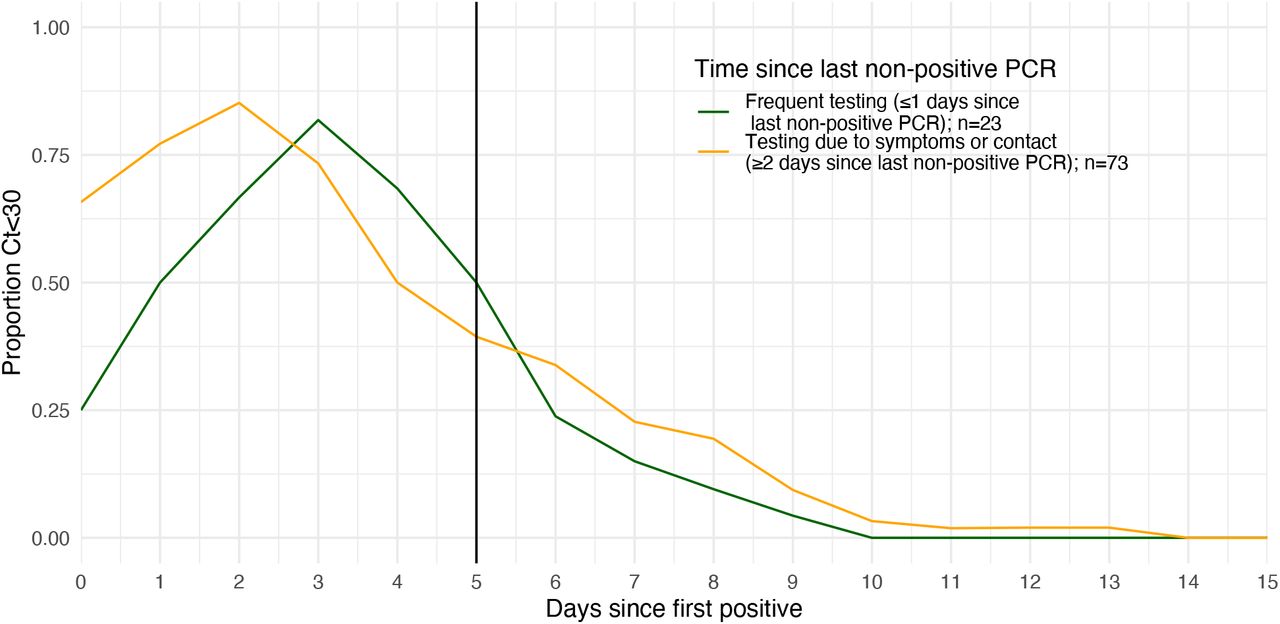
Individual viral trajectories from Omicron infection demonstrated substantial heterogeneity, though all individuals were RT-PCR negative by day 15 post detection (Fig. 1A). All individuals exhibited Ct values <30 at some point in their infection, and by day 11 post detection all tested individuals had Ct values ≥ 30. Of 27 individuals with a negative or inconclusive test ≤ 1 day prior to a first positive test for Omicron, 52.0% (13/25) were PCR positive with Ct values <30 at day 5, 25.0% (6/24) at day 6, and 13.0% (3/23) on day 7 post detection (Fig. 1B, Table S1). 51.9% (14/27) individuals exhibited Ct values <30 at some point from day 5 post detection onward. These were individuals undergoing frequent near-daily testing at the time of detection. In comparison, 70 individuals were last tested ≥ 2 days prior to detection by positive RT-PCR and primarily represent those who underwent testing either because of COVID-19 symptoms or because of concern for exposure to a SARS-CoV-2 infected individual. In this group, 39.1% (25/64) were PCR positive with Ct values <30 at day 5, 33.3% (21/63) at day 6, and 22.2% (14/63) on day 7 post detection (Fig. 1B, Table S1). 49.3% (34/69) individuals exhibited Ct values <30 at some point from day 5 post detection onward.

(A) PCR Ct value trajectories for each acute Omicron (red) and Delta (blue) infection. Solid colored lines show mean Ct value over time, counting negative tests as Ct=40. Horizontal dotted line shows cutoff of PCR Ct=30. (B) Solid vertical line indicates 5 days post detection. Individuals are grouped by the gap between detection and their most recent negative or inconclusive PCR test. Individuals detected ≤ 1 day of a previous negative or inconclusive test are classified as under a “Frequent testing” regime (green line), whereas individuals detected ≥ 2 days since their last negative or inconclusive test are predominantly those detected due to recent symptom onset or through contact tracing (orange line).
The daily proportion of individuals with Ct value <25 is shown in Fig. S1. We also evaluated the proportion of individuals with Ct value <30 over time for Delta infections (Fig. S2, Table S2). Finally, we found that including inconclusive PCR test results as positives rather than negatives had a negligible impact on the proportion with Ct values <30 over time since detection (Fig. S3, Table S3).
For those infected with the Omicron variant, we observed a proliferation phase of 4.52 days (95% credible interval 3.61-5.54), peak viral RNA of 7.28 log10 genome equivalents per ml (95% CI 7.02-7.54), and clearance phase of 5.35 days (95% CI 4.78-6.00), with an overall inferred mean duration of 9.87 days (95% CI 8.83-10.9) (Fig. 2A-D). The length of the proliferation phase for Omicron infections was especially variable, with individual posterior mean values ranging from 1.1 to 9.7 days (Fig. 2B). The peak viral RNA based on Ct values was lower than for those infected with the Delta variant (Ct 23.3, 95% CI 22.4-24.3 for Omicron, as compared to 20.5, 95% CI 19.2-21.8 for Delta) and the clearance phase was shorter (6.23 days, 95% CI 5.43-7.17 for Delta), though the rate of clearance was similar (3.13 Ct/day (95% CI 2.75-3.54) for Omicron; 3.15 Ct/day (95% CI 2.69-3.64) for Delta) (Fig. 2E). Delta infections had a mean duration of 10.9 days (95% CI 9.41-12.4).

(A) Peak viral RNA concentration, (B) proliferation time, (C) clearance time, and (D) acute infection duration for omicron (red) and delta (blue) infections. Points depict the individual-level posterior mean values. Hatched lines depict the population mean and 95% credible intervals. (E) Mean posterior viral trajectories for Omicron (red) and Delta (blue) infections. Lines depict the mean values and shaded regions depict 95% credible envelopes.
Discussion
Isolation has the greatest impact on transmission when infections are detected early, and individuals remain isolated for the duration of their infectious period. However, there are clear costs to isolating longer than necessary, such as when the duration of infection is short or when individuals first test positive late in infection. Thus, isolation guidelines ideally should be individually informed and tailored or should reflect the typical time course of infectiousness.
To define the time course for viral RNA detection indexed to the day when the infection is first detectable by PCR, we used a cohort undergoing prospective frequent testing. Most individuals rapidly reached high viral RNA following initial detection with a high proportion persisting at Ct values <30, as a rough proxy for infectiousness, on day 5 post detection. All individuals reached Ct ≥ 30 by day 11 post detection. For individuals with no negative or inconclusive test recorded in at least 2 days preceding detection, the proportion with Ct values <30 over time showed a similar shape to those with a more recent negative or inconclusive test but with a higher proportion of cases with Ct value <30 at the time of detection. Similar kinetics between cases detected immediately after infection or those detected after some delay suggest that either symptoms appear rapidly relative to PCR positivity, or that rapid contact tracing, testing, or other factors may have accelerated case identification. Similar viral kinetics were recently observed in a cohort of hospitalized Omicron cases in Japan, with a large proportion of cases maintaining high viral loads up to 9 days post detection, while shedding was limited from day 10 onwards regardless of symptom status21.
We found that infections with the Omicron variant, relative to Delta infections, feature lower peak viral loads and shorter clearance times, but similar proliferation times and clearance rates. However, these differences may be attributable to factors beyond inherent variant characteristics. Importantly, we did not control for prior immune history12, which could partially explain the lower peak viral concentrations and shorter clearance times for Omicron infections given that vaccination and infection were more prevalent during the emergence of Omicron. This may be particularly relevant in this population, with uptake of booster vaccination doses occurring after most Delta infections and before most Omicron infections. Analyses of these data stratifying individuals by number of prior vaccinations and infections are ongoing.
Based on the similarity of viral dynamics between Omicron and Delta found here, these data do not support increased viral load, as measured by RT-PCR, as an explanation for why Omicron exhibits such high infectivity nor its potentially earlier onset of infectiousness6,7,17,22. This is consistent with recent findings of poor correlation between RNA genome copies and infectious viral titers23, suggesting that factors other than viral RNA load are needed to explain differences between the Omicron and Delta infectivity profile. These data also suggest that the less severe disease demonstrated by Omicron infection is not obviously accounted for by decreased viral loads in the nasopharynx or oropharynx2.
There are a number of limitations to these data and analyses. First, Ct values report viral RNA copies and do not necessarily capture infectiousness. While we chose a Ct value cutoff of 30 as a proxy for infectiousness13–17, this threshold should not be considered a perfect predictor of infectiousness. Second, the Ct values reported here are from samples that each combined anterior nares and oropharyngeal swabs and were performed on the Roche Cobas platform; results may differ by anatomical site and by PCR platform24–27. Third, this relatively small sample set was obtained in a population that is not representative of the general population. The study population of working individuals is younger and generally healthier, with high vaccination coverage, than to the general population, thus infections in this group may have a shorter clearance phase on average than in the general population. Furthermore, this cohort is under intensive testing, behavior protocols, and case-finding efforts; individuals detected due to symptom onset or concern for contacts may be detected earlier in infection than would be typical in the community. While results from a Japanese study suggest similar viral kinetics in a distinct population21, additional analyses from larger cohorts and across additional demographic groups are urgently needed. Finally, not all infected individuals were serially tested until obtaining a negative test result. As some of the trajectories reported here are right censored, it is not known when those individuals would have turned negative. Thus, the proportion of test results with Ct <30 over time should be interpreted with this limitation in mind.
The uncertainty about the true timing of the end of the infectious period for individuals identified as infected with COVID-19 outside of frequent testing regimens argues that a cautious approach for shortening isolation may be warranted. Testing may be beneficial for tailoring individual decision-making and reducing the risk of premature release from isolation28 while also limiting unnecessarily prolonged isolation.
Data Availability
Code and data to regenerate these analyses, including individual cycle threshold value trajectories, are available at https://github.com/gradlab/CtTrajectories_Omicron.
Supplementary figures

Identical to Figure 1 but using a cutoff of PCR Ct value <25. Solid vertical line indicates 5 days post detection. Individuals are grouped by the gap between detection and their most recent negative or inconclusive PCR test. Individuals detected ≤ 1 day of a previous negative or inconclusive test are classified as under a “Frequent testing” regime (green line), whereas individuals detected ≥ 2 days since their last negative or inconclusive test are predominantly those detected due to recent symptom onset or through contact tracing (orange line).
Number of samples per day since detection and number with Ct value <30. Note that not all individuals are tested on each day post detection. Note also that individuals testing negative at the end of their infection were assumed to contribute as negatives in the denominator for the remainder of the 15 days post detection.

Identical to Figure 1 for Delta-confirmed infections. Solid vertical line indicates 5 days post detection. Individuals are grouped by the gap between detection and their most recent negative or inconclusive PCR test. Individuals detected ≤ 1 day of a previous negative or inconclusive test are classified as under a “Frequent testing” regime (green line), whereas individuals detected ≥ 2 days since their last negative or inconclusive test are predominantly those detected due to recent symptom onset or through contact tracing (orange line).
Number of samples per day since detection and number with Ct value <30. Note that not all individuals are tested on each day post detection and that individuals testing negative at the end of their infection were assumed to contribute as negatives in the denominator for the remainder of the 15 days post detection. Note also that one individual was reported as having two Delta infections.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Identical to Figure 1 but assuming that the date of first detection includes positive and inconclusive tests. Solid vertical line indicates 5 days post detection. Individuals are grouped by the gap between detection and their most recent negative PCR test. Individuals detected ≤ 1 day of a previous negative test are classified as under a “Frequent testing” regime (green line), whereas individuals detected ≥ 2 days since their last negative test are predominantly those detected due to recent symptom onset or through contact tracing (orange line).
Number of samples per day since detection and number with Ct value <30. Note that not all individuals are tested on each day post detection and that individuals testing negative at the end of their infection were assumed to contribute as negatives in the denominator for the remainder of the 15 days post detection. Note that the sample sizes differ to Table S1, as inclusion of inconclusive tests results in some different time delays between last negative and first detection.
Footnotes
↵** Co-senior authors.
Funding Statement: Supported in part by CDC contract 200-2016-91779, Emergent Ventures at the Mercatus Center, the Huffman Family Donor Advised Fund, the Morris-Singer Fund, the National Basketball Association, and the National Basketball Players Association.
Data availability: Code and data to regenerate these analyses, including individual cycle threshold value trajectories, are available at https://github.com/gradlab/CtTrajecto-CtTrajectories_Omicron
Reference



