
ABSTRACT
Background The Omicron (B.1.1.529) variant of SARS-CoV-2 has rapidly achieved global dissemination, accounting for most infections in the United States by December 2021. Risk of severe outcomes associated with Omicron infections, as compared to earlier SARS-CoV-2 variants, remains unclear.
Methods We analyzed clinical and epidemiologic data from cases testing positive for SARS-CoV-2 infection within the Kaiser Permanente Southern California healthcare system from November 30, 2021 to January 1, 2022, using S gene target failure (SGTF) as assessed by the ThermoFisher TaqPath ComboKit assay as a proxy for Omicron infection. We fit Cox proportional hazards models to compare time to any hospital admission and hospital admissions associated with new-onset respiratory symptoms, intensive care unit (ICU) admission, mechanical ventilation, and mortality among cases with Omicron and Delta (non-SGTF) variant infections. We fit parametric competing risk models to compare lengths of hospital stay among admitted cases with Omicron and Delta variant infections.
Results Our analyses included 52,297 cases with SGTF (Omicron) and 16,982 cases with non-SGTF (Delta [B.1.617.2]) infections, respectively. Hospital admissions occurred among 235 (0.5%) and 222 (1.3%) of cases with Omicron and Delta variant infections, respectively. Among cases first tested in outpatient settings, the adjusted hazard ratios for any subsequent hospital admission and symptomatic hospital admission associated with Omicron variant infection were 0.48 (0.36-0.64) and 0.47 (0.35-0.62), respectively. Rates of ICU admission and mortality after an outpatient positive test were 0.26 (0.10-0.73) and 0.09 (0.01-0.75) fold as high among cases with Omicron variant infection as compared to cases with Delta variant infection. Zero cases with Omicron variant infection received mechanical ventilation, as compared to 11 cases with Delta variant infections throughout the period of follow-up (two-sided p<0.001). Median duration of hospital stay was 3.4 (2.8-4.1) days shorter for hospitalized cases with Omicron variant infections as compared to hospitalized patients with Delta variant infections, reflecting a 69.6% (64.0-74.5%) reduction in hospital length of stay.
Conclusions During a period with mixed Delta and Omicron variant circulation, SARS-CoV-2 infections with presumed Omicron variant infection were associated with substantially reduced risk of severe clinical endpoints and shorter durations of hospital stay.
Trial registration Not applicable
INTRODUCTION
Following its first detection in Gauteng Province, South Africa, the Omicron (B.1.1.529) variant of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was declared by the World Health Organization (WHO) to be a variant of concern on November 25, 2021 [1]. Rapid transmission of the Omicron variant fueled a fourth wave of SARS-CoV-2 infections in South Africa, during which daily diagnosed infections exceeded totals recorded during all previous periods in the country. As of January 2022, the Omicron variant has achieved wide dissemination including in the United States, where 95% of all SARS-CoV-2 infections diagnosed during the week ending January 1, 2022 were estimated to be caused by the Omicron variant [2].
Understanding the potential for new SARS-CoV-2 variants to differ in clinical severity or in susceptibility to vaccine-derived immunity is crucial to inform public health responses. Such concerns are pronounced with the Omicron variant, which harbors a constellation of mutations in the spike protein associated with altered cell entry and immune evasion. Reduced neutralization of the Omicron variant has been reported in studies using plasma specimens from individuals with complete (two- or three-dose) mRNA vaccine series [3], and from patients with prior SARS-CoV-2 infection [4]. Epidemiologic data from South Africa have suggested higher rates of Omicron variant infections among persons with prior SARS-CoV-2 infection, as compared to observations with previous variants [5], while early observational studies have suggested reduced effectiveness of COVID-19 vaccines against Omicron variant infection [6–8]. However, increases in SARS-CoV-2 infections following emergence of the Omicron variant have not been associated with parallel increases in hospitalizations and deaths in the same proportions experienced during previous waves [9–11].
The first known Omicron variant infection in the United States was reported in California on December 1, 2021 [12], and by January 2, 2022 California experienced daily case totals surpassing those of all previous epidemic waves [13]. We undertook a prospective cohort study monitoring clinical outcomes among patients suspected to have infection due to the Omicron variant versus other variants on the basis of S gene target failure (SGTF) in reverse transcription polymerase chain reaction (RT-PCR) testing [14]. We compared risk of severe clinical outcomes among patients with or without SGTF infections, as well as epidemiologic characteristics of these patients, including their history of vaccination and prior SARS-CoV-2 infection.
METHODS
Setting
Kaiser Permanente of Southern California (KPSC) is an integrated, comprehensive healthcare organization serving 4.7 million members (∼19% of the population of southern California) enrolled through employer-provided, prepaid, or federally sponsored insurance plans. Members of KPSC closely resemble the sociodemographic profile of the surrounding geographic area in terms of age, racial/ethnic composition, and community characteristics [15]. Care delivery including diagnoses, immunizations, and prescriptions across virtual, outpatient, emergency department, and inpatient settings is recorded in near real-time through patients’ electronic health record (EHR), while out-of-network care is captured through insurance reimbursements. The study protocol was reviewed and approved by the KPSC institutional review board, which waived requirement for informed consent.
Testing procedures
Polymerase chain reaction (PCR) testing for SARS-CoV-2 occurred in a variety of clinical settings within KPSC during the study period. A majority of tests conducted in outpatient settings are submitted to regional laboratories, where >90% of samples are processed using the ThermoFisher TaqPath COVID-19 Combo Kit. Samples collected in hospitals are processed by either these regional laboratories or by in-house hospital laboratories, which use the ThermoFisher TaqPath COVID-19 Comboo Kit as well as the Roche cobas 8800 system for diagnostic testing. Previous evidence has indicated that the Δ69-70 amino acid deletion in the spike (S) protein of Omicron variant specimens causes a failure in PCR probes targeting the S gene, whereas the Orf1ab and nucleocapsid (N) probes retain sensitivity; in contrast, SGTF is rare in Delta variant SARS-CoV-2 infections [7,9,14]. We therefore considered SGTF in RT-PCR-positive specimens processed using the ThermoFisher TaqPath COVID-19 Comboo Kit to serve as a proxy for Omicron variant infections. We validated the concordance of SGTF with Omicron variant identification by tabulating the number of Omicron and non-Omicron variant infections identified over this period using whole genome sequencing and viral lineage designation among cases whose tests did or did not exhibit SGTF.
Inclusion criteria and outcome measures
All KPSC members who received a positive SARS-CoV-2 reverse transcription-polymerase chain reaction (RT-PCR) test result from tests performed between 30 November, 2021 and 1 January, 2022, and processed using the ThermoFisher TaqPath COVID-19 Combo Kit, were eligible for inclusion in the study. Individuals with a positive PCR test in the 90 days prior to the start of the study period were excluded.
As primary endpoints, we considered five markers of clinically severe illness: any hospital admission, hospital admission associated with new-onset acute respiratory symptoms, intensive care unit (ICU) admission, mechanical ventilation, and mortality. Hospitalizations and ICU admissions were considered to be COVID-19-related if they occurred between 7 days before to 28 days after the date of each patient’s positive SARS-CoV-2 RT-PCR test. Symptomatic hospital admissions were those with acute respiratory infection symptoms beginning on or ≤14 days before the admission date; we ascertained presence of symptoms and dates of symptoms onset via natural language processing of open-text EHR fields including clinical notes and patient-provided questionnaire responses, which are submitted by all KPSC patients who seek SARS-CoV-2 testing regardless of test setting [16]. We considered new-onset respiratory symptoms following a positive test as a secondary endpoint for further exploratory analyses among cases who were asymptomatic at the time of their original test.
We recorded the first date that each study endpoint occurred, censoring observations at January 1, 2022 or patients’ dates of disenrollment, whichever was earliest. Because our sample excluded a proportion of hospitalized cases who were tested using in-house assays other than the ThermoFisher TaqPath COVID-19 Combo Kit, our primary analyses addressed cases whose SARS-CoV-2 infections were first ascertained by outpatient testing. We additionally present results from analyses that included all cases tested using the ThermoFisher TaqPath COVID-19 Combo Kit, regardless of outpatient or inpatient test setting.
Last, for a duration-of-hospital-stay analysis, we recorded dates of discharge, in-hospital mortality, or censoring for all hospitalized patients. Patients who died in hospital or were discharged to hospice were considered to have experienced fatal COVID-19 hospitalizations, while patients discharged for any other reason were considered to have experienced non-fatal COVID-19 hospitalizations. Living patients who had not yet been discharged by January 1, 2022 were considered censored for the duration-of-stay analysis. Duration-of-stay analyses included all patients admitted to hospital whose samples were processed using the ThermoFisher TaqPath COVID-19 Combo Kit, regardless of outpatient or inpatient test setting.
Exposures
Exposures of interest included demographic characteristics of patients (age, sex, race/ethnicity, and neighborhood-level median household income) as well as clinical risk factors recorded within the prior year (including history of smoking, body mass index, Charlson comorbidity index, and healthcare utilization across outpatient, emergency department, and inpatient settings). We additionally recorded patients’ history of a positive SARS-CoV-2 test result of any type or COVID-19 diagnosis ≥90 days prior to their first positive RT-PCR test during the study period, as well as the dates of receipt of any COVID-19 vaccine doses (BNT162b2 [Pfizer/BioNTech], mRNA-1973 [Moderna/National Institutes of Health], or Ad.26.COV2.S [Janssen]). Patients’ history of receipt of COVID-19 vaccines was obtained through patient’s EHR or the California Immunization Registry. COVID-19 vaccines were provided at no cost to KPSC members following emergency use authorization and were therefore captured in the EHR. Vaccinations administered outside of KPSC were captured via the California Immunization Registry, to which providers are required to report all COVID-19 vaccine administrations within 24 hours.
Statistical analysis
We compared times from the first positive test to each outcome event or censoring among patients who tested positive for SARS-CoV-2 by RT-PCR, with and without SGTF. We used Cox proportional hazards models to estimate the adjusted hazard ratio (aHR) for each endpoint associated with SGTF, adjusting for all demographic and clinical covariates listed above. We repeated analyses of the symptomatic hospital admission endpoint within subgroups defined by patient age, sex, Charlson comorbidity index, and history of documented SARS-CoV-2 infection and vaccination, controlling for all other risk factors via covariate adjustment. In secondary analyses that included patients tested in inpatient settings, times to events were recorded as 0.5 days for patients tested on or before the date of an outcome event occurring.
We conducted multiple (m=5) imputation of missing covariate values and pooled results obtained with each imputed dataset via Rubin’s rules [17]. We verified proportional hazards assumptions by testing for slopes in Schoenfeld residuals [18]. When hazard ratios could not be computed due to zero-valued event totals within either the SGTF or non-SGTF sample, we computed p-values to compare risk across groups via the binomial likelihood of observing zero cases under the null hypothesis of equal daily risk relative to the other sample.
We further compared lengths of stay among hospitalized patients with SGTF and non-SGTF infections. We fit Weibull distributions to patients’ lengths of hospitalization via parametric competing risk models accommodating three outcomes of fatal, non-fatal, or censored discharge dispositions. We used these fitted distributions to compute differences in median lengths of stay for patients hospitalized with SGTF and non-SGTF infections, conducting statistical inference via bootstrap resampling.
To compare demographic and clinical attributes of cases by variant type, we estimated adjusted odds ratios (aORs) of each exposure among cases with SGTF versus non-SGTF infections via logistic regression. We again pooled results across multiple imputed datasets. As a sensitivity check, we repeated analyses within the subgroup of patients who were continuously enrolled in KPSC health plans ≥1 year before the date of their first positive SARS-CoV-2 RT-PCR test during the study period.
We conducted all analyses using R (version 4.0.3; R Foundation for Statistical Computing, Vienna, Austria). We used the survival [19] and cfc [20] packages for time-to-event analyses, and the Amelia II [21] package for multiple imputation.
RESULTS
Among plan members tested at KPSC between November 30, 2021 and January 1, 2022, there were 88,576 positive SARS-CoV-2 detections among individuals tested as outpatients, including 69,279 (78.2%) ascertained via the ThermoFisher TaqPath COVID-19 Combo Kit, enabling determination of SGTF. Among patients hospitalized during the study period with SARS-CoV-2 infection, 457 of 1,721 (26.6%) were tested using the ThermoFisher TaqPath COVID-19 Combo Kit. Of positive specimens tested via this assay, SGTF was identified in 52,297 (75.5% of 69,279), including 235 (51.4% of 457) patients tested in inpatient settings. Both the absolute number and the proportion of patients with SGTF results increased steadily over the study period, except during the week following the Christmas holiday on 25 December when both testing volumes and the proportion of samples processed by regional laboratories using the ThermoFisher TaqPath COVID-19 Combo Kit declined (Figure 1). Mean lengths of follow-up were 5.5 days for cases with SGTF infections and 15.8 days for cases with non-SGTF infections. Among 1,477 infected patients whose SARS-CoV-2 isolates were selected for sequencing over the study period, the Omicron variant was detected in all SGTF samples (382/382) and the Delta variant was detected in 1,092 of 1,095 non-SGTF samples (99.7%; Table S1), validating the interpretation of SARS-CoV-2 infections with and without SGTF as Omicron and Delta variant infections, respectively.
Concordance of SGTF infection status with Omicron or Delta variant detection.
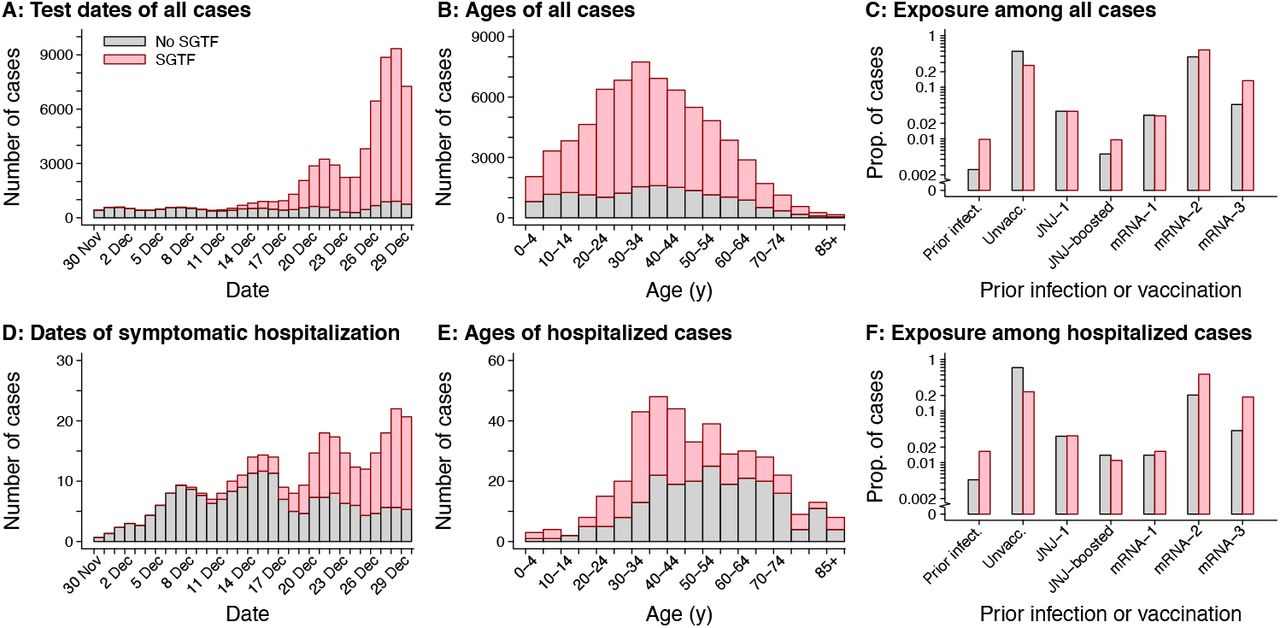
Panels include (A) test dates for all cases analyzed (truncated at 29 December, 2022 to accommodate ±1 day jittering); (B) age distribution of all cases analyzed; (C) exposure history (prior documented infection and vaccination) among all cases analyzed; (D) dates of symptomatic hospital admission (truncated at 29 December, 2022 to accommodate ±1 day jittering); (E) age distribution of cases with symptomatic hospitalizations; and (F) exposure history (prior documented infection and vaccination) among cases with symptomatic hospitalizations. Pink and grey bars correspond to detections with and without SGTF (interpreted as a proxy for SARS-CoV-2 Omicron variant infection; Table S1), respectively. Totals correspond to samples processed on RT-PCR TaqPath COVID-19 High-Throughput Combo Kit and do not reflect all cases at KPSC.
Over a total of 288,534 person-days of follow-up following an outpatient positive test, 88 patients with Omicron variant infections were admitted to hospital, as were 189 patients with Delta variant infections over 264,408 person-days of follow-up (Figure 1; Figure 2; Table 1). Onset of acute respiratory symptoms on or ≤14 days before hospital admission was recorded for 84 patients with Omicron variant infections (95.5% of 88) and 187 patients with Delta variant infections (98.9% of 189), who were thus classified as experiencing symptomatic hospitalizations (Table S2). Adjusted hazard ratios for hospital admission and symptomatic hospital admission associated with Omicron variant infection, relative to Delta variant infection, were 0.48 (95% confidence interval: 0.36-0.64) and 0.47 (0.35-0.62), respectively (Table 1; Table S3). Findings of reduced risk of symptomatic hospitalization in association with Omicron variant infection following outpatient positive tests held within subgroups defined by patient age, sex, Charlson comorbidity index, history of documented SARS-CoV-2 infection, and COVID-19 vaccination status (Table S4). Findings also held in subgroup analyses restricted to cases with ≥1 year of continuous enrollment prior to their testing date (Table S5). In analyses not restricted to cases who were first ascertained in outpatient settings, adjusted hazard ratios for any hospitalization and symptomatic hospitalization associated with Omicron variant infection were 0.72 (0.58-0.88) and 0.62 (0.49-0.77), respectively.
Onset of acute respiratory symptoms on or before dates of testing and hospital admission.
Predictors of symptomatic hospital admission among cases with SGTF infections and non-SGTF infections.
Association of SGTF infection status with symptomatic hospitalization in various patient subgroups.
Association of SGTF infection status with adverse clinical outcomes, limiting analyses to cases with ≥1 year of continuous enrollment.
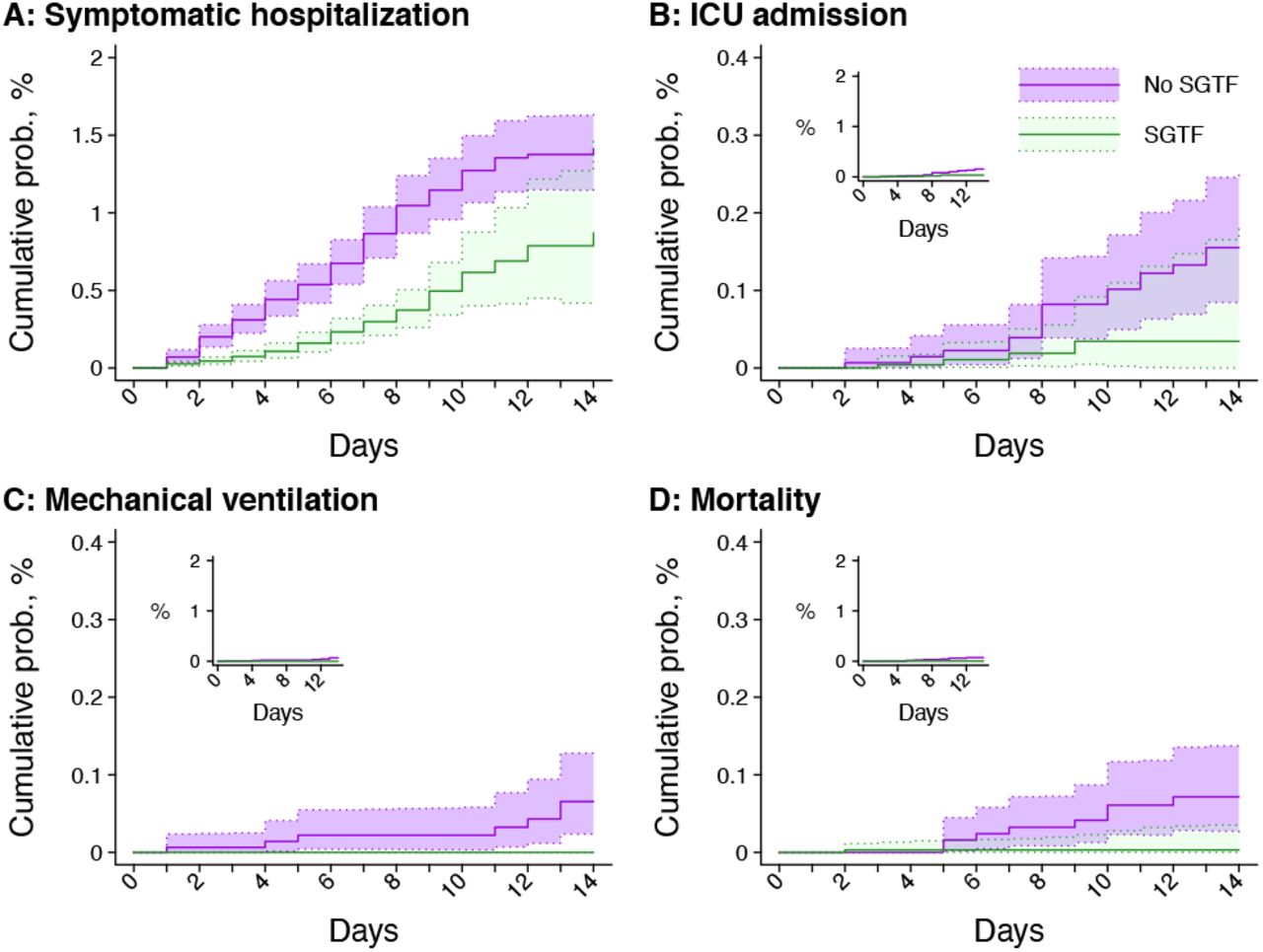
Panels include (A) symptomatic hospital admissions; (B) ICU admissions; (C) initiations of mechanical ventilation; and (D) mortality. Inset plots within each panel illustrate cumulative probabilities on the same y-axis scale as panel A. Shaded regions denote 95% confidence intervals. Green and violet correspond to detections with and without SGTF (interpreted as a proxy for SARS-CoV-2 Omicron variant infection; Table S1), respectively.
Among patients with Omicron variant infections, 7 received intensive care (including 5 whose infections were first identified in outpatient settings), 1 died, and none received mechanical ventilation, as compared to 23 ICU-admitted patients, 14 deceased patients, and 11 ventilated patients among those with Delta variant infections (Table 1). The observed number of patients meeting each of these endpoints was inadequate for multivariate analyses due to the absence of counts within multiple covariate strata. Unadjusted hazard ratios of ICU admission and mortality associated with Omicron variant infection were 0.26 (0.10-0.73) and 0.09 (0.01-0.75), respectively, among cases whose infections were first ascertained in outpatient settings. Additionally, the daily risk of mechanical ventilation among patients with Delta variant infections was significantly higher than among patients with Omicron variant infections (0.04 vs 0 per 1000 person-days at risk following a positive outpatient test; 2-sided p<0.001).
Acute respiratory symptoms were reported on or before testing dates for 79.7% of cases with Omicron variant infections first ascertained in outpatient settings (41,552/51,333) and 80.0% of cases with Delta variant infections first ascertained in outpatient settings (13,547/16,929; Table S2). Among cases without symptoms at the time of outpatient testing, new-onset respiratory symptoms during follow-up were reported for 991 (9.4% of 10,581) cases with Omicron variant infections and 553 (16.4% of 3,382) with Delta variant infections (aHR=0.69 [95% confidence interval: 0.62-0.77] for Omicron vs. Delta variant infections; Table S6).
Association of SGTF infection status with occurrence of respiratory symptoms, among cases without symptoms at the time of testing.
By January 1, 2022, symptomatic hospitalizations were complete for 152 (83.5% of 182) hospitalized patients with Omicron variant infections and 168 (77.8% of 216) with Delta variant infections (Table S7). All patients with Omicron variant infections who completed hospitalizations by January 1 were discharged alive to home or home-based care, as compared to 156 (92.9% of 168) patients with Delta variant infections (two-sided p<0.001). Among 154 Omicron variant-infected patients who completed hospitalization by January 1, 2022, 129 (83.8%) were discharged in ≤2 days, as compared to 52 (31.0% of 168) patients with Delta variant infections. Accounting for censoring in a parametric survival model, we estimated that the median duration of stay for patients with Omicron variant infections experiencing symptomatic hospitalizations was 1.5 (1.3-1.6) days, with 90% of patients expected to complete hospitalizations within 3.1 (2.7-3.6) days. Among symptomatic hospitalized patients with Delta variant infections, the estimated median duration of stay was 4.9 (4.3-5.6) days, representing a difference of 3.4 (2.8-4.1) days in median duration of stay from patients with Omicron variant infections (Figure 3). This difference corresponded to a 69.6% (64.0-74.5%) shorter median length of hospital stay among patients with Omicron variant infections as compared to patients with Delta variant infections.
Disposition at completion of hospitalization among patients with completed hospital stays.

{kind=link}
{kind=link}
{kind=link}
Panels include: (A) fitted distribution functions of the lengths of symptomatic hospitalizations for cases with SGTF and non-SGTF detections (with inset panel illustrating the distribution of the difference in median lengths of stay), and (B) fitted cumulative distribution function of times to death or discharge for symptomatic hospitalized patients with SGTF and non-SGTF infections. Weibull-distributed event times are fitted via parametric competing risk models accounting for right-censoring of lengths of stay for patients remaining in hospital. Solid and dotted lines correspond to detections with and without SGTF (interpreted as a proxy for SARS-CoV-2 Omicron variant infection; Table S1), respectively.
As compared to cases with Delta variant infection, cases with Omicron variant infection had higher adjusted odds of being aged 20-29 and 30-39 years, and had lowest odds of being young children and older adults (Figure 1; Table 2; Table S8). Patients with Delta variant infection were more often white, resided in lower-income neighborhoods, and had greater burden of comorbid conditions. Similar patterns held when restricting comparisons to cases who had been enrolled in KPSC plans ≥1 year previously (Table S9).
Demographic and clinical characteristics of all cases with SGTF infections and non-SGTF infections, regardless of test setting.
Demographic and clinical characteristics of cases tested in outpatient settings with SGTF infections and non-SGTF infections, limiting analyses to cases with ≥1 year of continuous enrollment.
Demographic and clinical characteristics of cases tested in outpatient settings with SGTF and non-SGTF SARS-CoV-2 infections.
Among cases first ascertained in outpatient settings, adjusted odds of documented prior SARS-CoV-2 infection ≥90 days before individuals’ first positive test during the study period were 4.45 (3.24-6.12) fold higher among cases with Omicron variant infections than among cases with Delta variant infections infection (Figure 1; Table 2). Similarly, adjusted odds of prior receipt of each vaccine series (1, 2, or 3 doses of BNT162b2/mRNA-1973, or Ad.26.COV2.S with or without a booster dose of any vaccine) were higher among cases with Omicron as compared to Delta variant infections. In a model including interaction terms between documented prior SARS-CoV-2 infection and vaccination, the adjusted odds of prior infection were higher among cases with Omicron variant infections than cases with Delta variant infections within the vaccinated strata; adjusted odds of prior vaccination were also higher among cases with Omicron variant infections as compared to Delta variant infections, irrespective of prior documented SARS-CoV-2 infection (Table S10).
Combined history of documented SARS-CoV-2 infection and COVID-19 vaccination among cases with SGTF infections and non-SGTF infections.
DISCUSSION
Using data from a large, comprehensive healthcare system that captured information on SARS-CoV-2 testing and clinical outcomes among its members, and using SGTF as a proxy for Omicron versus non-Omicron (predominantly Delta) variant infections, we identified substantially reduced risk of severe clinical outcomes among patients with presumed Omicron variant infections. Within the subset of our cohort tested in outpatient settings, among whom prospective follow-up adverse outcomes was possible, Omicron variant infections were associated with 52%, 53%, 74%, and 91% reductions in risk of any subsequent hospitalization, symptomatic hospitalization, ICU admission, and mortality, relative to Delta variant infections. Median duration of hospital stay for patients admitted with symptomatic Omicron variant infections was approximately 70% (∼3.4 days) shorter than that observed among patients with symptomatic Delta variant infections. Reductions in disease severity associated with Omicron variant infections were evident among both vaccinated and unvaccinated patients, and among those with or without documented prior SARS-CoV-2 infection. Prior vaccination against COVID-19 was associated with a dose-dependent lower risk of detection of the Delta variant as compared to the Omicron variant; likewise, Delta variant infections were less commonly detected among cases with documented prior SARS-CoV-2 infection.
Several lines of evidence support the hypothesis that the Omicron variant might have a lower propensity to result in severe illness as compared with the Delta variant. Consistency of the association of Omicron variant infection with reduced risk of hospitalization across age and comorbidity categories, and regardless of prior immunity from vaccination or SARS-CoV-2 infection, during the same month and in the same population, argues against host or behavioral factors as causes of the observed disease attenuation with the Omicron variant. Notably, the risk of symptomatic hospitalization was markedly reduced among cases who had tested positive for SARS-CoV-2 infection ≥90 days prior (0.32 vs 2.08 symptomatic hospitalizations per 1000 person-days at risk among cases with Omicron vs. Delta variant infections, respectively). Although ascertainment of SARS-CoV-2 infection history is imperfect because many infections may have gone untested or may not have been documented in a patient’s EHR, prior infection among individuals with a history of a positive SARS-CoV-2 test result should be accurately coded and false positive PCR tests are rare. Thus, the finding of a reduction in severity of Omicron in patients with known prior infection is compelling evidence of an intrinsically less severe infection, rather than only different (more immune) persons becoming infected with the Omicron variant.
Several studies have found similar reductions in severity with infection from Omicron compared to infection from other SARS-CoV-2 variants. In other settings, estimated reductions in risk of hospitalization with Omicron variant infection have ranged from 20-80% [9–11,22,23]. Variability in estimates between studies is likely in part due to different definitions of the primary endpoint (e.g. any attendance at hospital, admission to hospital, or admission to hospital with symptoms at the time of testing), differing lengths of follow-up, as well as varying levels of vaccination and prior infection across populations. However, these findings collectively suggest that differences in viral factors between the Omicron and the Delta variants, such as differences in viral tropism or virulence factors, might be driving the observed relative reductions in disease severity. Recent ex vivo studies demonstrate higher replication of the Omicron variant in the human upper respiratory tract as compared to the small airways of the lung [24], consistent with animal experiments suggesting that disease from infection with the Omicron variant might be confined to the large airway [25].
In this analysis, prevalence of prior vaccination differed among cases with Omicron and Delta variant infections. While our analysis cannot infer absolute vaccine effectiveness against the distinct variants, our findings suggest vaccine protection against infection with the Omicron variant may be lower than protection against infection with the Delta variant. This result is consistent with studies showing reduced neutralization efficiency of two and three doses of BNT162b2 vaccine against the Omicron variant (versus non-Omicron variants) [3,26]. Similarly, in multiple settings, vaccination with two doses showed slightly lower effectiveness against hospitalization with Omicron vs. Delta variant infections [6–8]. Our finding of higher relative protection against Delta variant infections is reassuring considering the greater severity observed in infections with the Delta variant as compared to the Omicron variant. However, evidence for a reduction in severe outcomes among vaccinated cases with both Delta and Omicron variant infections in our study (Table S3) suggests substantial public health benefits from continued COVID-19 vaccination.
Our study has certain limitations. While limited follow-up time was available for identifying hospitalizations of long duration, discharge dispositions were known for 84% of cases hospitalized with Omicron variant infections and 78% of those with Delta variant infections, providing a robust basis for time-to-event analyses. Incidental detections of SARS-CoV-2 among hospitalized patients might also have been more commonly associated with Omicron variant than Delta variant infections, leading to underestimates of attenuated disease severity in analyses of all hospitalizations. This consideration supports our use of EHR data on symptoms (assessed for all patients tested at KSPC) to define an endpoint of hospitalizations associated with acute respiratory symptoms, and our use of a prospective cohort design monitoring for new inpatient admissions among cases first ascertained by outpatient testing. This analytic framework also helped to mitigate bias that could result from exclusion of cases who were first tested using assays that would not identify SGTF, as such tests were used more often for patients tested in hospital settings. Follow-up was shorter for Omicron variant infections because these became most common near the end of the study period; use of a Cox proportional hazards model accounted for the resulting censoring. As access to testing may differ among KPSC members versus the general population, case-to-hospitalization ratios for Omicron and non-Omicron variant infections in our study may not hold at the population level. Differences in prevalence of prior infection and vaccination among KPSC members versus the general public may also impact transportability of effect size estimates from this study.
We have quantified two aspects of comparative severity of Omicron vs. Delta variant infections: the risk of progression to severe endpoints among diagnosed cases, and the risk of progression to acute respiratory symptoms among those first diagnosed before symptoms onset. While attenuation of disease severity in association with the Omicron variant is an encouraging finding, prior evidence of higher transmissibility of Omicron variant infections [27], as well as immune evasion from prior infection [28] and vaccination [6–8], are concerning. Rapid spread of the Omicron variant in a compressed time period has led to unprecedented surges in COVID-19 among our study population and others globally. High rates of infection in the community have overwhelmed health-care systems and could translate to high absolute numbers of hospitalizations and deaths, even with lower severity of the Omicron variant as compared to non-Omicron variants. Thus, implementation of concurrent prevention strategies including vaccination, masking, and appropriate infection mitigation strategies remains important to curb transmission, decrease morbidity and mortality, and reduce burden on health systems nationwide.
Data Availability
Requests for access to data should be submitted to Sara.Y.Tartof{at}kp.org.
ACKNOWLEDGMENTS
This work was funded by the US Centers for Disease Control and Prevention.
Footnotes
Disclaimer: The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the CDC.
REFERENCES



