
Abstract
The French sanitary pass led to an increase in vaccination rates in France, but local heterogeneities in vaccination rates remain. To identify potential determinants of these heterogeneities and how the French sanitary pass influenced them, we used a data-driven approach on exhaustive nationwide data, gathering 181 socio-economic and geographic factors. Our analysis reveals that, both before and after the introduction of the French sanitary pass, factors with the largest impact are related to poverty, with the most deprived areas having greater than 10 times the odds of being among the districts with lower vaccination rates.
Introduction
The rapid development of effective COVID-19 vaccines brought the hope of a rapid return to normalcy, but heterogeneous vaccination rates, both among countries because of inequitable distributions of doses [Usher21] and within countries [Caspi21, Murthy21], jeopardize epidemic control.
Hesitancy and hostility toward vaccination have been comparatively high in France in recent decades [Ward19], a trend confirmed with the COVID-19 pandemic [Lazarus21, Spire21], although acceptance of the COVID-19 vaccine gradually grew during 2021 [SantePubliqueFrance21].
Attitudes toward vaccination are known to be influenced by social and territorial inequalities. Surveys conducted in 2020 in France showed that respondents with lower education [Schwarzinger21, Spire21], lower income levels or less trust in authorities [Spire21] were more likely to be hostile to COVID-19 vaccines. Whether differential intentions translated into effective differences in vaccination, as described in other countries [Caspi21, Murthy21], remained to be shown in France.
To speed up vaccination, President Macron announced on 12 July 2021 the implementation of a domestic “sanitary pass” (le passe sanitaire), which came fully into force on 9 August 2021. It was required in most cultural venues, for both indoor and outdoor dining and in health structures. This announcement led to an unprecedented demand for vaccination, which was celebrated internationally. Vaccination rates climbed from 54% of the whole population by 12 July 2021 to 69% on 4 September 2021. Because it targeted pay-for social activities, however, the “sanitary pass” was feared to have a limited impact on vaccination inequities.
This study aims to obtain further insights into the association between social inequities, vaccination and sanitary pass implementation in France using nationwide data.
Methods
The French state health insurance service (Assurance Maladie) provides public datasets of exhaustive weekly first-dose vaccination data at the district scale nationally and at the suburban scale for the Paris, Lyon, and Marseille metropolitan areas. Our data included 1552 districts in mainland France (63,601,670 individuals; median district size 22,705 inhabitants; interquartile range 6,282--39,128). We associated these data with 176 socioeconomic and 5 geographic indicators at the same geographic scales from public datasets.
We considered the association between being a district in the lowest quartile of the first-dose vaccination rate and being above the median value of each indicator. We computed odds ratios and their 95% confidence intervals at three time points: week 27 (just before the sanitary pass announcement), week 31 (when the sanitary pass came fully into force), and week 35 (end of data collection). For the two indicators achieving the highest odds ratios, we computed vaccination levels for each indicator quartile on the same dates. Analyses were done using R (v4.0.3).
Results
The two indicators most associated with local vaccination rates (figure 1) were the income rate coming from unemployment benefits (w27: OR=12.6 [8.7; 18.9]; w31: OR=13.3 [9.1; 20.0]; w35: OR=11.9 [8.2; 17.6]; the brackets correspond to 95% CI) and the proportion of overcrowded households (w27: OR=11.6 [8,3; 16.4], w31: OR=12.0 [8.6; 17.1], w35: OR=15.7 [11.0; 23.0]).
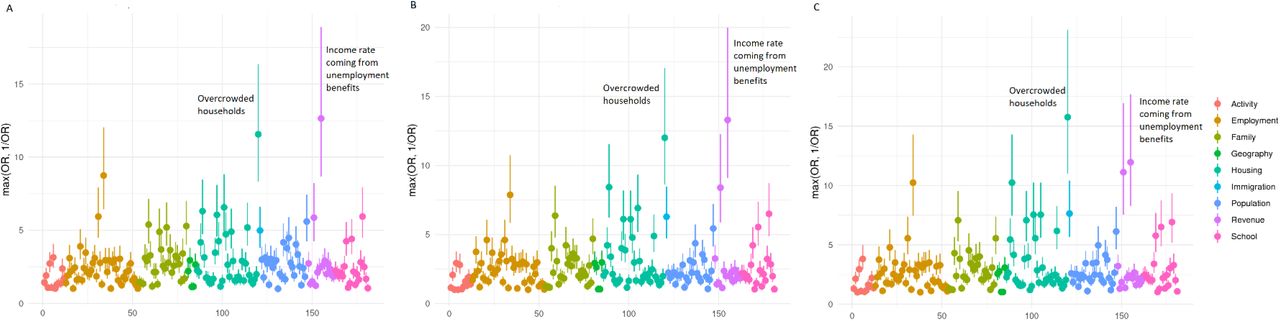
Odds ratio (OR) and their 95% confidence intervals for the association between vaccination rate and each of the 181 selected indicators at week 27 (panel A), 31 (panel B) and 35 (panel C)

{kind=link}
{kind=link}
Local vaccination rates depending on the quartile of the two main indicators (Overcrowding rate, left and Unemployment rate, right) and over time (weeks 27, 31, 35, with increasingly darker shading)
The difference in vaccination rates (in percentage points) between the first and fourth quartiles of the two indicators remained similar across weeks (figure S1): unemployment w27: ΔQ1-4= 7.6 [6.6; 8.7], w31: ΔQ1-4= 8.0 [7.0; 9.0], w35: ΔQ1-4= 7.9 [6.9; 8.9], and overcrowding w27: ΔQ1-4= 6.9 [5.7; 8.1], w31: ΔQ1-4= 7.6 [6.6; 8.8], w35: ΔQ1-4= 8.2 [7.2; 9.1].
Discussion
Our results based on exhaustive national datasets indicate that the most deprived areas have greater than 10 times the odds of being among the districts with lower vaccination rates. Lower vaccination rates in France are still associated with poverty, meaning that the sanitary pass did not resolve vaccine inequities. Specifically, living in a district with a large fraction of overcrowded housing or in which unemployment benefits represent a large share of the local income is a strong determinant of a lower COVID-19 vaccination rate in France.
Our study confirms the strong impact of social inequalities on COVID-19. The most deprived areas have already been shown to have been disproportionately infected and hospitalized during the pandemic [Jannot21, Bajos21]. We show that poorer districts are also the least vaccinated and, hence, the most still at risk, despite the widely celebrated domestic sanitary pass. There is an urgent need to define new vaccination policies that truly address social inequities.
Data Availability
This study involves only openly available data: - INSEE: https://www.insee.fr/fr/statistiques/5359146#consulter - Assurance Maladie: https://datavaccin-covid.ameli.fr/explore/dataset/donnees-devaccination-par-epci/https://datavaccin-covid.ameli.fr/explore/dataset/donnees-de-vaccination-parcommune/information/
https://www.insee.fr/fr/statistiques/5359146#consulter
https://datavaccin-covid.ameli.fr/explore/dataset/donnees-devaccination-par-epci/
https://datavaccin-covid.ameli.fr/explore/dataset/donnees-de-vaccination-parcommune/information/
Acknowledgements
We thank the producers of public datasets, in particular David Levy at INSEE and and Antoine Rachas at Assurance Maladie.
Footnotes
Funding EL received funding to match socio-economic data with medical data from AP-HP Centre Université de Paris.
Conflict of interest statement No conflict of interest to disclose
Data sources INSEE: https://www.insee.fr/fr/statistiques/5359146#consulter
Assurance Maladie: https://datavaccin-covid.ameli.fr/explore/dataset/donnees-devaccination-par-epci/https://datavaccin-covid.ameli.fr/explore/dataset/donnees-devaccination-parcommune/information/



