
Abstract
In the studies to date, the estimated fold-drop in neutralisation titre against Omicron ranges from 2- to over 20-fold depending on the study and serum tested. Collating data from these results in a combined estimate of the drop in neutralisation titre against Omicron of 9.7-fold (95%CI 5.5-17.1). We use our previously established model to predict that six months after primary immunisation with an mRNA vaccine, efficacy for Omicron is estimated to have waned to around 40% against symptomatic and 80% against severe disease. A booster dose with an existing mRNA vaccine (even though it targets the ancestral spike) has the potential to raise efficacy for Omicron to 86.2% (95% CI: 72.6-94) against symptomatic infection and 98.2% (95% CI: 90.2-99.7) against severe infection.
On 25th November 2021 the SARS-CoV-2 variant Omicron (B.1.1.529) was declared a Variant of Concern (VOC) by the World Health Organisation. Omicron is proposed to escape immune recognition from existing vaccines due to the number of mutations in the spike protein, targeted by most of the widely available vaccines (1). We have previously developed a method for estimating vaccine efficacy based on neutralisation titres and shown that once the loss of neutralisation against a novel VOC is known it is possible to reliably predict vaccine efficacy against that variant (2, 3). On 8th December 2021 the first data demonstrating a drop in neutralisation titres against Omicron emerged from the Sigal Lab (4) and was closely followed by similar data from Sheward et al. (5), the Ciesek Lab (6) and Pfizer Inc. / BioNTech SE (7, 8). Here, we use these early reports to predict vaccine efficacy against Omicron using our previously established approach (2, 3).
In the studies to date, the estimated fold-drop in neutralisation titre against Omicron ranges from 2- to over 20-fold depending on the study and serum tested. This large range is not surprising, since we have shown in a large meta-analysis of the neutralisation of prior VOC that the drop in neutralisation against a variant varies dramatically between laboratories and assays, and also depends on the potency of the serum and limit of detection of the assay. Further, we identified that, after accounting for these laboratory and censoring effects, there were no significant differences between vaccines in the fold drop in neutralisation titres for each VOC. Thus, we found that to estimate neutralisation against a new variant it was most robust to aggregate a range of estimates from multiple laboratories rather than rely on a single laboratory result (3).
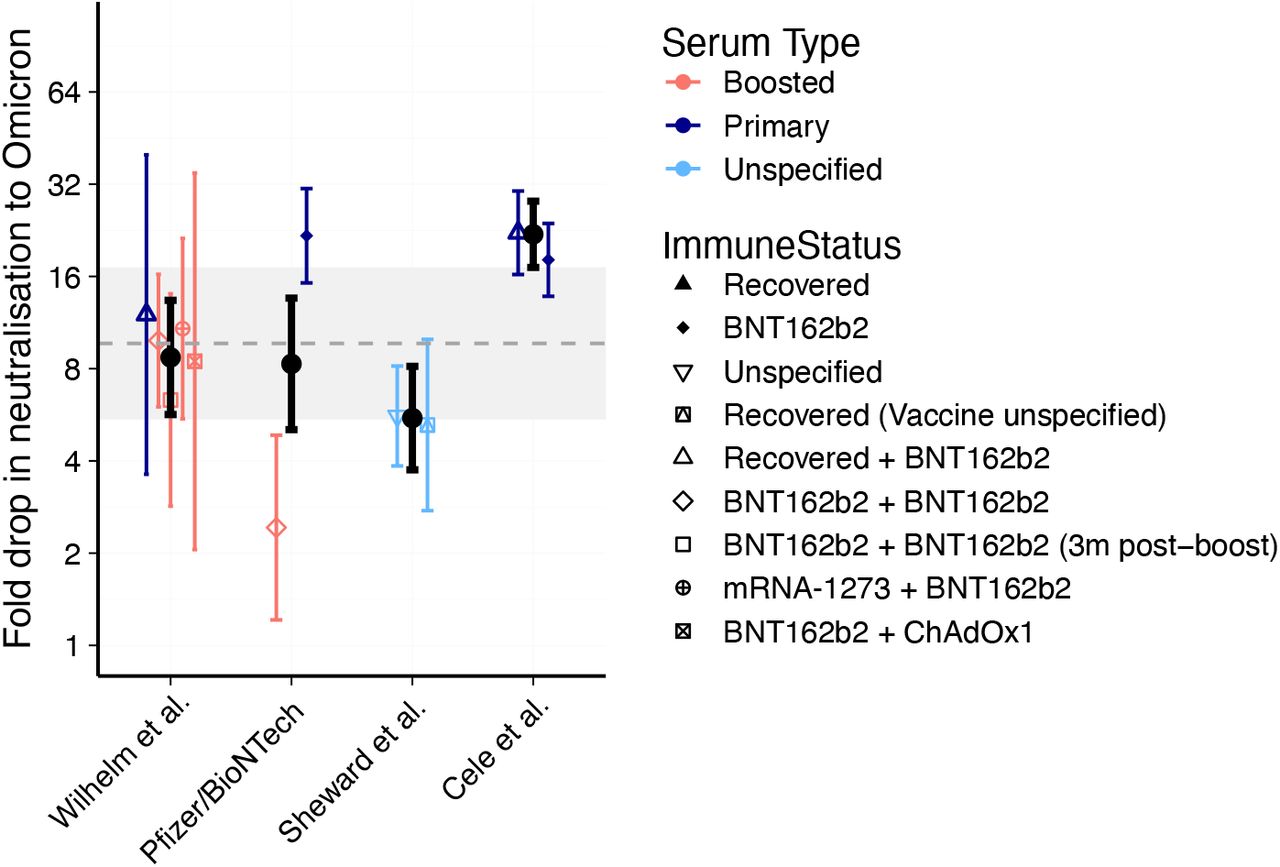
Collating data from the four studies listed above and accounting for censoring of neutralisation titres below the limit of detection (which is critical since many samples are below detection for Omicron) results in a combined estimate of the \ drop in neutralisation titre against Omicron of 9.7-fold (95%CI 5.5-17.1). This is shown in Figure 1 (grey line) along with the censored estimates of the fold drops by study (black lines) and within each cohort of a study (coloured lines).
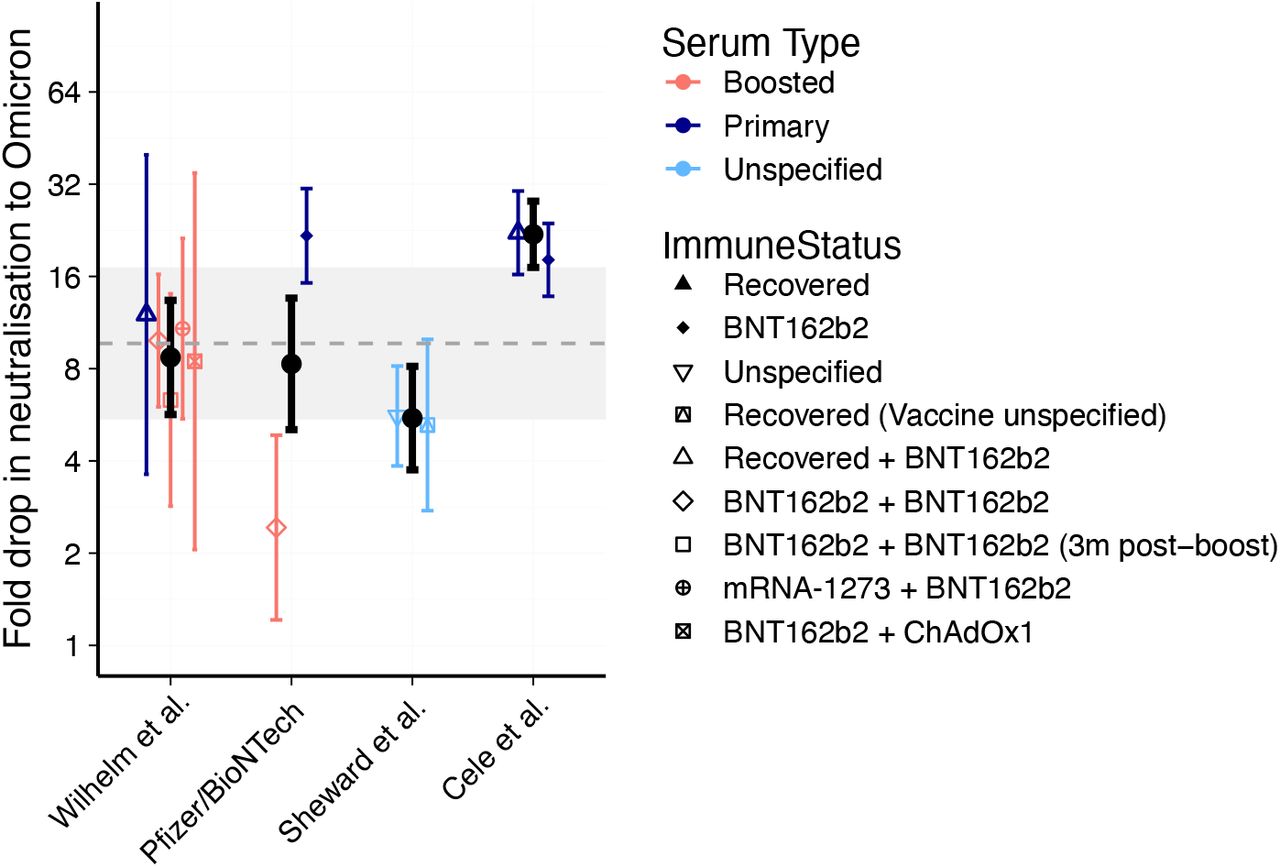
Estimated fold drops in Neutralisation levels against Omicron compared to the ancestral strain of SARS-Cov-2 across studies and cohorts available as of 13th December 2021. Black dots indicate the geometric mean fold drop in neutralisation observed in each study across the different cohorts tested (with censoring at the limit of detection). All error bars indicate the 95% confidence intervals of the mean for each group. The grey dashed line indicates geometric mean of the studies (i.e. geometric mean of the black dots) and grey shading region indicates the 95% confidence interval of this mean of the studies.
Combining this estimate of the drop in neutralisation to Omicron (fig. 1) we next estimate vaccine efficacy (or protection for convalescent individuals) for vaccines shortly after vaccination and six months later (2) (approach described in (3). We predict that prior infection (with the ancestral SARS-Cov-2 strain) provides 34.3% (95% CI: 16.6-53.2) protection against symptomatic infection with Omicron and 76.6% (95% CI: 39.3-93.5) protection against severe symptoms. As predicted by earlier studies, protection following primary vaccination is similar for ChAdOx1 nCoV-19 to protection from prior infection, and higher for the mRNA vaccines (Figure 2A and C). However, six months after primary immunisation with an mRNA vaccine, efficacy for Omicron is estimated to have waned to around 40% against symptomatic and 80% against severe disease (Figure 2B and D). A booster dose with an existing mRNA vaccine (even though it targets the ancestral spike) has the potential to raise efficacy against Omicron to 86.2% (95% CI: 72.6-94) against symptomatic infection and 98.2% (95% CI: 90.2-99.7) against severe infection. These estimates are in very good agreement with recent vaccine efficacy estimates from a Test Negative Case Control study published by the UK Health Security Agency (9). The comparison between the UK data and our model estimates is shown in Figure 3.

Predictions of Vaccine Efficacy against Omicron for symptomatic (panels A and B) and severe (panels C and D) disease. Vaccine efficacies are shown early after exposure / vaccination (panels A and C) and six months after exposure / vaccination (panels B and D). Vaccine efficacy was calculated using the mean neutralisation titres associated with each vaccine//convalescent cohort/ mRNA boosted cohort using the method outlined in (2, 3). Neutralisation titres after vaccination with each vaccine regimen are based on levels reported in Phase 1/2 trials relative to the average convalescent individual in the same study (as calculated in (2)). Note, the AstraZeneca neutralisation titre is that associated with a 4 week interval between doses. mRNA boosted neutralisation levels are based on average levels reported in previously infected individuals boosted with an mRNA vaccine from (3). The neutralisation levels 6 months after infection, vaccination or boosting were calculated using a decay half-life of neutralizing antibodies of 108 days (as reported in (3)). Error bars indicate 95% confidence intervals calculated by bootstrapping as in (3).
{kind=link}
{kind=link}
{kind=link}
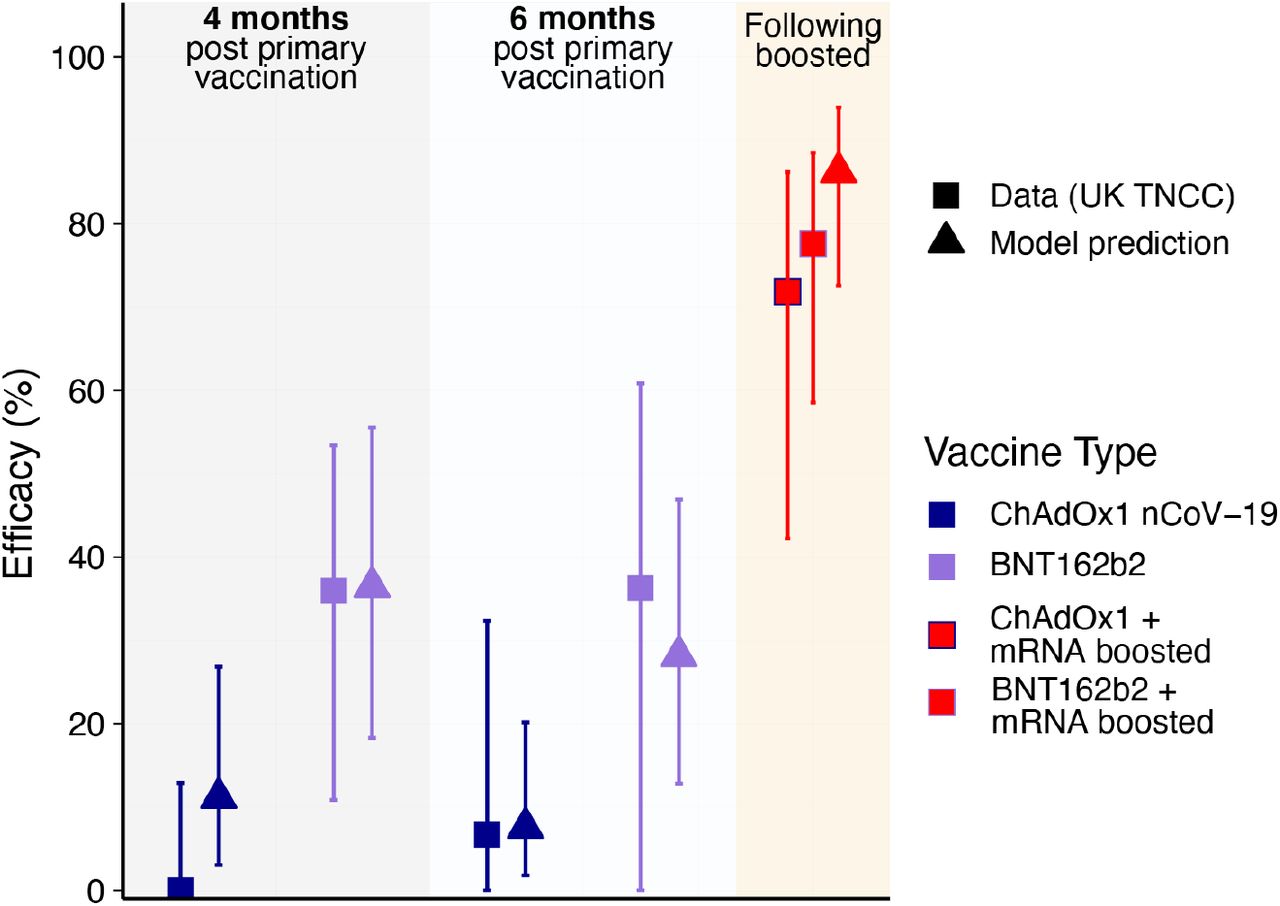
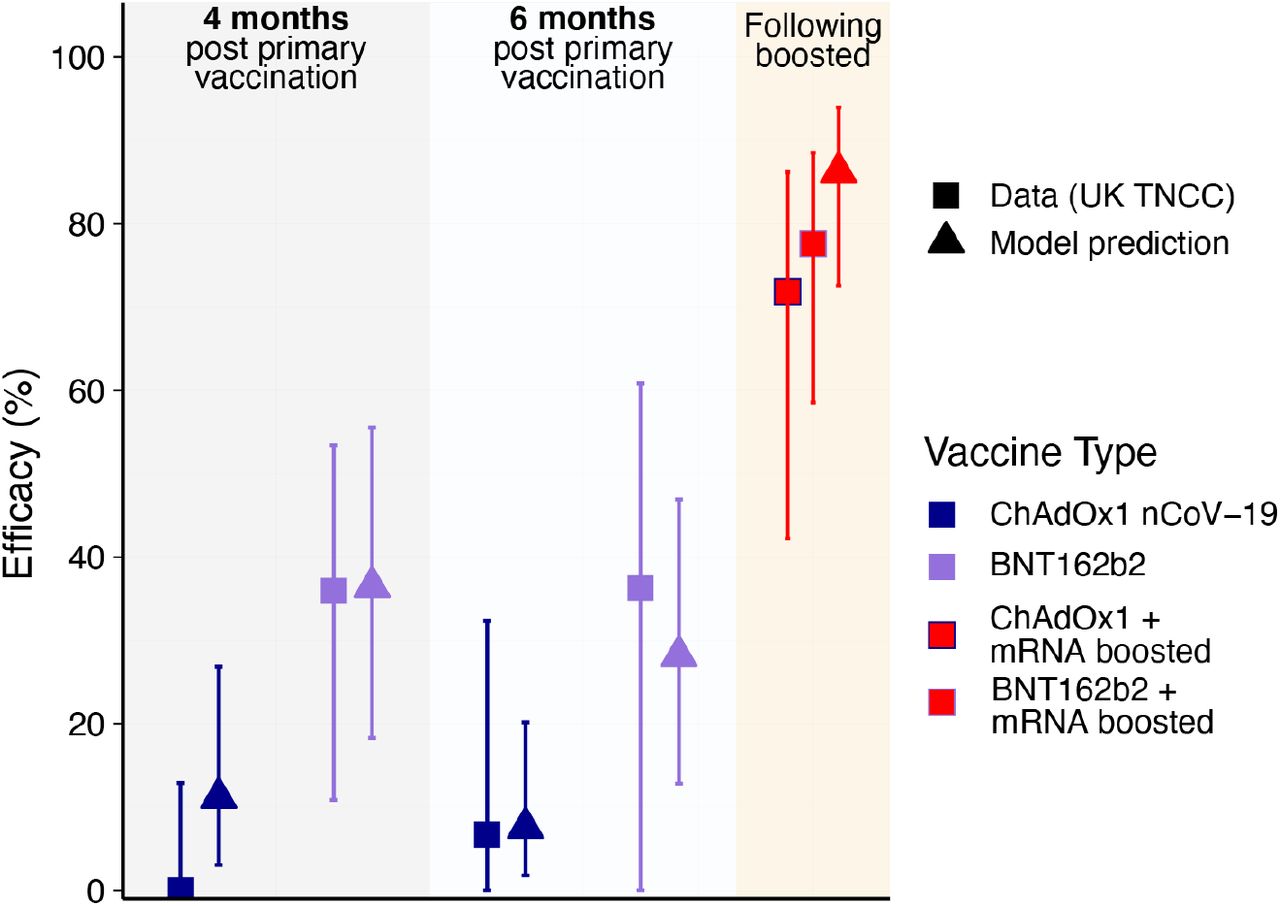
Comparison between estimates of Vaccine Efficacy against Omicron from a UK TNCC study (9) (squares) and our model estimate (triangles) at four months, six months and after boosting with an mRNA vaccine for AstraZeneca (blue) and Pfizer (purple).
Emerging data on the loss of neutralisation against the Omicron variant reveals considerable escape of neutralizing responses, but indicates that high levels of protection to symptomatic and severe infection is likely to be achieved by boosting with existing vaccines that target ancestral spike protein.
Data Availability
All data produced in the present study are available upon reasonable request to the authors



