
Abstract
Clinical Pharmacogenomics Implementation Consortium (CPIC) guidelines exist for many medications commonly prescribed prior to hospital discharge, yet there is limited data regarding the contribution of gene-x-drug interactions to hospital readmissions. The present study evaluated the relationship between prescription of CPIC medications prescribed within 30 days of hospital admission and 90-day hospital readmission from 2010-2020 in a study population (N=10,104) who underwent sequencing with a 14-gene pharmacogenetic panel. The presence of at least one pharmacogenetic indicator for a medication prescribed within 30 days of hospital admission was considered a gene-x-drug interaction. Multivariable logistic regression analyzed the association between one or more gene-x-drug interactions with 90-day readmission. There were 2,211/2,354 (93.9%) admitted patients who were prescribed at least one CPIC medication. Univariate analyses indicated that the presence of at least one identified gene-x-drug interaction increased risk of 90-day readmission by more than 40% (OR=1.42, 95% confidence interval (CI) 1.09-1.84)(p=0.01). A multivariable model adjusting for age, race, sex, employment status, body mass index, and medical conditions, slightly attenuated the effect (OR=1.33, 95% CI 1.02-1.75)(p=0.04). Our results suggest that the presence of one or more CPIC gene-x-drug interactions increases the risk of 90-day hospital readmission, even after adjustment for demographic and clinical risk factors.
1. Introduction
Despite a major national program to reduce hospital readmissions, 30-day hospital readmission rates for acute myocardial infarction, heart failure, and pneumonia are more than 17%,1 representing a major quality gap.2 A recent systematic review found that 21% of hospital readmissions were due to adverse drug reactions.3 Several large-scale pharmacogenetic implementation consortia have evaluated medical outcomes, but few have reported associations between a composite panel of gene-x-drug interactions and all prescribed medications that have evidence-based guidance from the Clinical Pharmacogenomics Implementation Consortium (CPIC).4
Studies from the Mayo Clinic Biobank have reported mixed results regarding associations between pharmacogenetic (PGx) phenotypes and hospital admissions,5,6 but these analyses did not evaluate gene-x-drug interactions. A Implementing GeNomics In pracTiCe (IGNITE) Network7 multisite pragmatic investigation demonstrated that the risk of major adverse cardiovascular events for patients prescribed clopidogrel with a loss-of-function (LOF) CYP2C19 allele was more than two-fold higher than patients without a LOF allele prescribed clopidogrel (adjusted hazard ratio (HR) 2.26, 95% CI 1.18-4.32).8 The Electronic Medical Records and Genomics (eMERGE) Network’s9 multi-center pilot of electronic health record (EHR)-based preemptive pharmacogenetics (PGx) of the following gene-drug pairs (CYP2C19/clopidogrel, CYP2C9/VKORC1/warfarin, and SLCO1B1/simvastatin)11 showed that patients prescribed warfarin within the CPIC dosing guideline range had a statistical trend toward faster time to first stable target international normalized ratio (INR) compared to starting dose outside this range.12 Although IGNITE and eMERGE have not yet reported hospitalization outcomes for most of their projects, there is evidence from smaller studies of preemptive PGx genotyping in elderly patients,13 patients with mental health disorders,14 and home health patients15 that have shown reductions in hospitalizations,14,15 readmissions,15 and improvements in medication adherence.16
The aim of our study was to evaluate the relationship between gene-x-drug interactions and risk of 90-day hospital readmission. Given that there is no standard of care for pharmacogenetic medication tailoring prior to hospital discharge nationally, we anticipated that patients with gene-x-drug interactions would be more likely to have less optimal management and adherence, which over time would contribute to clinical manifestations requiring hospital readmission. Although there is not standard coding for every type of suboptimal drug response other than acute adverse drug reactions, we focused on the presence of actionable gene-x-drug interactions for these preliminary analyses. We hypothesized that patients with gene-x-drug interactions for medications prescribed up to and during hospital admission and discharge would be more likely to be readmitted within 90 days of hospital discharge.
2. Materials and Methods
2.1. Patient Population
The study population were primary care patients ages 18 or older who were offered, consented, and underwent Color™ (Burlingame, CA) next generation sequencing (NGS) for genetic screening of cancer and cardiovascular risk and a 14-gene pharmacogenetic panel between April 2019 and February 2020.17 Results were integrated into primary care health maintenance visits and communicated by primary care physicians. Electronic medical records were searched for all hospital admissions from 2010-2020, medications with Clinical Pharmacogenomics Implementation Consortium guidelines (CPIC medications) prescribed within 30-days of hospital admission, and 90-day hospital readmissions and associated admission diagnoses, patient demographics, major chronic disease conditions, smoking, and COVID-19 status. Age, sociodemographic variables, and medical history represent the most recent available data extracted through September 2021.
2.2. Data Extraction
Data on medication prescriptions was extracted for medications with accompanying 2021 CPIC guidelines at the time of this writing. These medications included amitriptyline, atazanavir, atomoxetine, azathioprine, capecitabine, celecoxib, citalopram, clomipramine, clopidogrel, codeine, desipramine, doxepin, efavirenz, escitalopram, fluorouracil, flurbiprofen, fluvoxamine, fosphenytoin, ibuprofen, imipramine, lansoprazole, lornoxicam, meloxicam, mercaptopurine, nortriptyline, omeprazole, ondansetron, pantoprazole, paroxetine, peginterferon alfa-2a/2b, phenytoin, piroxicam, sertraline, simvastatin, tacrolimus, tamoxifen, tenoxicam, thioguanine, tramadol, trimipramine, tropisetron, voriconazole, and warfarin. Genetic indicators (metabolic phenotypes and genotypes) for genes with evidence for variability in drug response were curated, annotated, and extracted for CYP2B6, CYP2C19, CYP2C9, CYP2D6, CYP3A4, CYP3A5, CYP4F2, DPYD, F5, IFNL3, NUDT15, SLCO1B1, TPMT, VKORC1. Covariate data were extracted for sociodemographic variables (age, gender, ethnicity, employment and marital status), and clinical variables (body mass index (BMI), smoking status, COVID-19 test results, and history of cancer, chronic obstructive pulmonary disease (COPD), type 1 or 2 diabetes, myocardial infarction (MI), heart failure (HF), peripheral vascular disease (PVD), asthma, or stroke (cerebrovascular accident; (CVA)). For the purposes of this investigation, patients were considered to have a gene-x-drug interaction if they were prescribed at least one CPIC medication within 30 days of hospital admission for which they possessed a pharmacogenetic genotype that portends altered drug pharmacokinetics, pharmacodynamics and/or efficacy. ICD-10 if available or ICD-9 diagnostic codes and conditions were binned into the following 21 categories for descriptive purposes: behavioral/psychiatric, cancer/neoplasm, cardiovascular, developmental/disability, endocrine/metabolic, hematological, gastrointestinal (GI), gynecological, infection/dermatological/abscess, infection/abscess/other, infection/respiratory, infection/GI, infection/genitourinary, inflammatory/rheumatological, obstetrical, orthopedic/musculoskeletal, otolaryngological, pain, pulmonary, renal, and vascular/non-cardiac.
2.3. Statistical Analysis
Clinical and demographic variables were compared between patients with 90-day readmissions and non-readmissions using a Wilcoxon rank sum test for continuous variables and a Chi-square or Fisher’s exact test for categorical variables. Patient descriptive statistics were reported as median and interquartile range (IQR) for continuous variables and frequency and percentage for categorical variables. Univariate and multivariable logistic regression analyses were performed to determine the association between drug interaction and 90-day readmission. Variables with statistically significant group differences and p-value less than 0.1 in univariate analysis were included in multivariable logistic regression model as predictors of 90-day hospital readmission. Odds ratios (ORs) and corresponding 95% confidence intervals (CIs) are reported. P-values less than 0.05 were considered significant. All statistical analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA).10
3. Results
A total of all 10,104 DNA10K patients were included in the analyses. Table 1 presents the main participant demographic and clinical characteristics of the study population. Of these individuals, there were 2,354 participants (23.3%) with a history of at least one hospital admission from 01/01/2010 through 12/31/2020. Compared with patients who were not admitted, patients with a 10-year history of at least one hospital admission were more likely to be female (p<0.0001), have higher BMI (p<0.0001), more likely to be White/non-Hispanic (p=0.0002), more likely to be married (p<.0001), less likely to be employed (p<.0001), and were more likely to have a history of a major medical condition including asthma, cancer, COPD, CVD, diabetes, HF, hypertension, MI, or PVD (ps<0.0001). There were no statistically significant differences in age, COVID-19 test results, or smoking status between patients with history of admission and no admissions from 2010-2020. Compared to patients with 10-year histories of at least one hospital admission who were not readmitted to hospital, patients with a history of 90-day hospital readmissions were older (median = 59, IQR: 44-67 years vs median = 47, IQR: 37-62 years)(p<0.0001), and readmitted patients were more likely to have a history of a major medical condition.
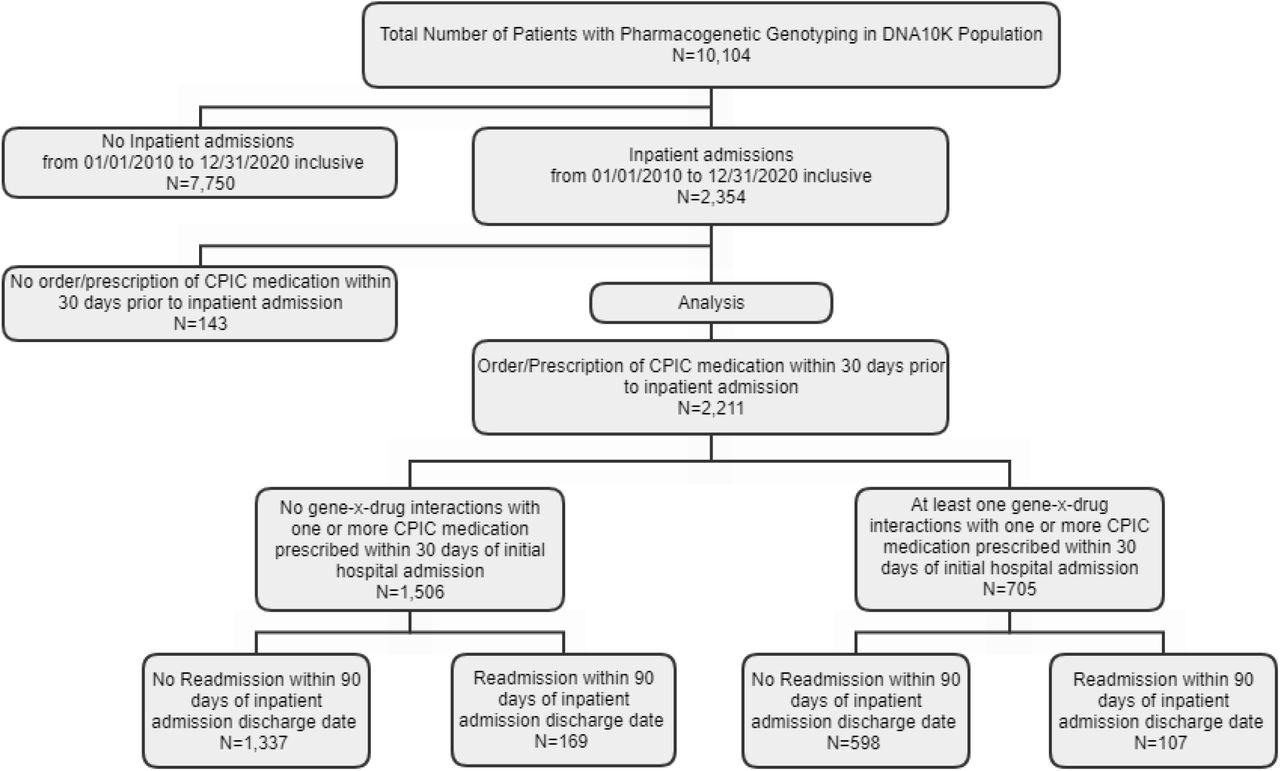
Of the 10,104 patients, 7,885 (78%) were prescribed at least one CPIC medication at least once and of the 2,354 patients admitted between 2010 and 2020, 2,333 (99.1%) were prescribed at least one CPIC medication. Of patients admitted during this period, 2,221 (93.9%) were prescribed at least one CPIC medication within 30 days of their initial hospital admission, whereas only 9 (0.1%) of patients who were not admitted had been prescribed a CPIC medication within 30 days prior to admission. Of the 281 patients readmitted to hospital within 90 days, 276 (98.2%) were prescribed a CPIC medication within 30 days of their initial hospital admission compared with 1,935/2,073 (93.3%) of patients not readmitted to hospital within 90 days. Figure 1 is a flow diagram of patients included in the analyses based on admission and CPIC medication gene-x-drug interaction status.
{kind=link}
Flow diagram of inclusion of patients in study population of whom all underwent genotyping and phenotyping with a next generation sequencing Color™ (Burlingame, CA) panel. Patients (n=2,211) who had a history of at least one hospital admission from 2010-2020 were included in the logistic regression analyses.
Supplemental Table S1 lists CPIC medications prescribed within 30 days of initial hospital admission. The most frequently prescribed CPIC medications for patients readmitted within 90 days were ondansetron (n=257, 93.1%), omeprazole (n=125, 45.3%), ibuprofen (n=101, 36.6%), tramadol (n=95, 34.4%), warfarin (n=52, 18.8%), celecoxib (n=49, 17.8%), escitalopram (n=27, 9.8%), simvastatin (n=25, 9.1%), clopidogrel (n=19, 6.9%), and codeine (n=19, 6.9%). Sufficiently detailed data are not presently available to determine relationship between medication prescribed and cause of hospital admission or readmission. There were 234 different diagnostic codes for 90-day hospital readmission. Supplemental Table S2 reports admission diagnostic categories for patients with 90-day hospital readmissions. The most frequent admission diagnostic categories were endocrine/metabolic (n=48, 17.4%), cancer/neoplasm (n=32, 11.6%), infectious (n=31, 13.9%), gastrointestinal (n=30, 10.9%), obstetrical (n=21, 7.6%), cardiovascular (n=16, 5.8%), hematological (n=16, 5.8%), orthopedic/musculoskeletal (n=13, 4.7%), neurological (n=10, 3.6%), or pulmonary (n=10, 3.6%) conditions.
Table 2 presents results of multivariable logistic regression of risk of 90-day hospital readmission (dependent variable) for patients prescribed a CPIC medication within 30 days of an initial hospital admission with at least one gene-x-drug interaction compared with prescription of at least one CPIC medication with no gene-x-drug interactions (reference). The unadjusted 90-day readmission rate for patients with a gene-x-drug interaction was 15.2% (107/705) compared with 11.2% (169/1,506), (OR=1.42, 95% CI 1.09-1.84)(p=0.01). Age increasing per year (OR=1.03, 95% CI 1.02-1.04)(p=<0.0001), male sex (OR=1.76, 95% CI 1.34-2.33)(p=<0.0001), Black (OR=1.98, 95% CI 1.20-3.25)(p=0.005)) or Asian race (OR=0.43, 95% CI 0.21-0.85)(p=0.01), employment status (OR=2.03, 95% CI 1.57-2.62)(p=0.02), or the presence of 3 or more comorbidities (OR=4.06, 95% CI 2.84-5.81) were also associated with higher rates of 90-day hospital readmission. Adjusting for sociodemographic variables and comorbidity, the odds of hospital admission for patients with at least one gene-x-drug interaction compared to no gene-x-drug interaction involving a CPIC medication prescribed within 30 days of initial hospital admission was slightly attenuated but statistically significant (OR=1.33, 95% CI 1.02-1.75)(p=0.04).
4. Discussion
To our knowledge, this is the first published study to report the net effect of a panel of pharmacogenetic variants on hospital readmission in a large, primary care based patient population. Most other studies have reported on results for special patient populations for specific gene-x-drug combinations. These data suggest that even though taking a CPIC medication may be a proxy of risk for hospital admission, the presence of one or more gene-x-drug interactions increases risk of 90-day hospital readmissions above and beyond the risk contributed by the conditions under treatment by these medications.
This study has several limitations. Data are not available on all potential adverse drug reactions that result from suboptimal dosing or selection of medications because our data were limited to admission diagnoses and some admission diagnoses (e.g., orthopedic conditions or bleeding) were not coded as inadequate pain control for a specific medication or bleeding resulting from dosing outside the recommended range for an anticoagulant based on genotype. Thus, we could not stratify with specificity the causes of hospital admission and readmission. Another limitation is that we did not have data curated for medication dose and its relationship to evidence-based dosing recommendations for a given genotype. Therefore, we were not able to determine adherence to CPIC prescribing guidelines.
However, even with advanced physician decision support and guidance in our system,17-19 the presence of gene-x-drug interactions could theoretically affect drug response and risk of adverse events if not translated into tailored prescribing at every point of the care continuum. Evidence is needed from real-world health systems to justify the system-level investment in high-level pharmacogenetic decision support and patient monitoring. These results may contribute to this body of evidence, but additional investigations will need to address limitations in our present data using additional tools of data integration and innovation such as machine learning, natural language processing, and artificial intelligence20 to capture and conduct more sensitive phenotyping of potential adverse drug reactions and discordant dosing for specific genotypes over time. However, results from smaller studies noted earlier of special patient populations have suggested that preemptive pharmacogenetic genotyping can affect more favorable outcomes for a number of patient populations including the elderly,13 patients with mental health disorders,14 and home health patients15 that have shown reductions in hospitalizations,14,15 readmissions,15 and medication adherence.16
5. Conclusions
This study showed an association between gene-x-drug interactions and risk of 90-day hospital admissions for a general patient population amongst patients prescribed one or more medications with evidence for genetic variability in drug response. Replication and deeper phenotyping are needed to provide more clinical context for these observations. However, the effect size observed for this difference if taken to scale, indicates that gene-x-drug interactions may contribute substantially to the risk of preventable hospital admissions. Future, prospective studies are needed to evaluate the potential of preemptive genotyping and pharmacogenetic tailoring of patients at risk for hospital admission and readmission as a potentially effective intervention to prevent the morbidity and suboptimal treatment of clinical conditions following hospital discharge that can lead to hospital readmission.
Data Availability
All data produced in the present work are contained in the manuscript.
Author Contributions
SPD conceived the study design in collaboration with HMD, DOM, and PO, oversaw analyses, and he wrote the first draft of the manuscript. HMD extracted and curated the pharmacogenetic data. JP extracted data from the EDW and generated data reports and an integrated database. PH and HMD oversaw and managed the DNA10K patient offering that resulted in genotype data for the present study. AH conducted a literature review and contributed to review of medical records data. All coauthors participated in the preparation of and reviewed the final draft of the manuscript.
Funding
The DNA10K initiative was funded by the Transformation through Innovation Fund at NorthShore University HealthSystem. Additional funding that supported this project was provided to Dr. David from the NorthShore Auxiliary Research Award.
Institutional Review Board Statement
This study protocol (EH21-273) was deemed quality improvement according to criteria from the NorthShore Institutional Review Board and the study protocol was approved by the NorthShore Data Governance Committee in June of 2021.
Informed Consent Statement
Informed consent was obtained from all patients for genotyping and the present study was a quality improvement evaluation that did not involve collection of new information from patients and was secondary data analyses and therefore not considered human subjects research.
Conflicts of Interest
Dr. David acts as a scientific advisor to Genalyte, Inc. (San Diego, CA). No other disclosures were reported.
Acknowledgements
We wish to thank Dr. Bernard Ewigman, Ms. Margo Quinn, and the NorthShore Outcomes Research Network Administrative Core for support of this project.
References



