
ABSTRACT
Background This study describes primary surgical reconstructions performed for children born with a cleft lip and/or palate in the United Kingdom.
Methods Data were obtained from the Cleft Collective, a national longitudinal cohort study. Data forms completed at the time of surgery included details on timing, technique and adjuncts used during the operative period. Demographic data on participants were validated via parental questionnaires.
Results Between 2015 and 2021, 1782 Cleft Collective surgical forms were included, relating to the primary reconstructions of 1514 individual children. The median age at primary cheiloplasty was 4.3 months. Unilateral cleft lips were reconstructed with an anatomical subunit approximation technique in 53%, whereas bilateral cleft lips were reconstructed with a broader range of eponymous techniques. Clefts of the soft palate were reconstructed at a median age of 10.3 months with an intravelar veloplasty in 94% cases. Clefts of the hard palate were reconstructed with a vomer flap in 84% cases in a bi-modal age distribution, relating to reconstruction carried out simultaneously with either lip or soft palate reconstruction. Antibiotics were used in 96% of cases, with an at-induction-only regimen used more commonly for cheiloplasties (p<0.001) and a 5–7day post-operative regime used more commonly for soft palatoplasties (p<0.001). Peri-operative steroids were used more commonly in palatoplasties than cheiloplasties (p<0.001) but tranexamic acid use was equivalent (p=0.73).
Conclusion This study contributes to our understanding of current cleft surgical pathways in the United Kingdom and will provide a baseline for analysis of the effectiveness of utilised protocols.
BACKGROUND
More than 1000 babies are born with cleft lip and/or palate (CLP) in the United Kingdom (UK) each year1 mirroring the global incidence of CLP approximated at 1/700 live births.2 The Clinical Standards Advisory Group (CSAG) in 1998 revolutionised cleft care in the UK by demonstrating superior aesthetic and functional outcomes were achieved in multidisciplinary cleft units treating high volumes of patients.3 The follow-up Cleft Care UK study in 2015 demonstrated that centralising care into 11 managed clinical networks and adhering to a national standard of care, including minimum numbers treated per surgeon, improved outcomes.4–8 The Oslo CLP surgical protocol; cheiloplasty and vomer flap repair of anterior hard palate at 3-6 months followed by soft palate repair at 6-9 months, greatly influenced UK cleft surgery pathways as it led to superior maxillary growth and dental arch relationships.4–7 Although the UK does not currently have a nationally agreed cleft surgery protocol, the national cleft quality indicators (published by the National Health Service) specify that cleft lips are repaired by 6 months and cleft palates by 13 months (in the absence of specific clinical reasons for delay).8
Determining current surgical practice for the primary reconstruction of CLP on a national level is a challenge. Previous efforts globally have tended to utilise surveys sent to cleft surgeons,9,10 which are limited by the reliance on the surgeon’s memory, risking that the recollected description may not accurately represent the surgeon’s approach to the range of heterogeneous cleft phenotypes. In the UK, the CSAG report had important ramifications for cleft research and led to the development of the Cleft Collective in 2012, a longitudinal cohort study set up to explore the causes, treatment and outcomes associated with CLP on individuals and their families.11,12 The aim of this study was to use Cleft Collective Birth Cohort Surgical Data to establish the current UK pathways for primary reconstructions of CLP in terms of operative timings, techniques and adjuncts used peri-operatively.
METHODS
Participants and Resource
Children born between 2014-2021 undergoing primary surgical reconstructions for CLP in the UK enrolled in the birth cohort of Cleft Collective Cohort studies were included.12,13 Secondary surgical interventions for speech, alveolar bone grafting, orthognathic or revisional procedures were excluded. The Cleft Collective resource comprises biological samples, speech audio recordings, medical and educational records and parent and child completed questionnaires. The resource is available for clinical and academic communities to use to address a range of cleft related research questions. More information on the study and how to access the dataset is available at http://www.bristol.ac.uk/cleft-collective/professionals/access/.
Data collection and extraction
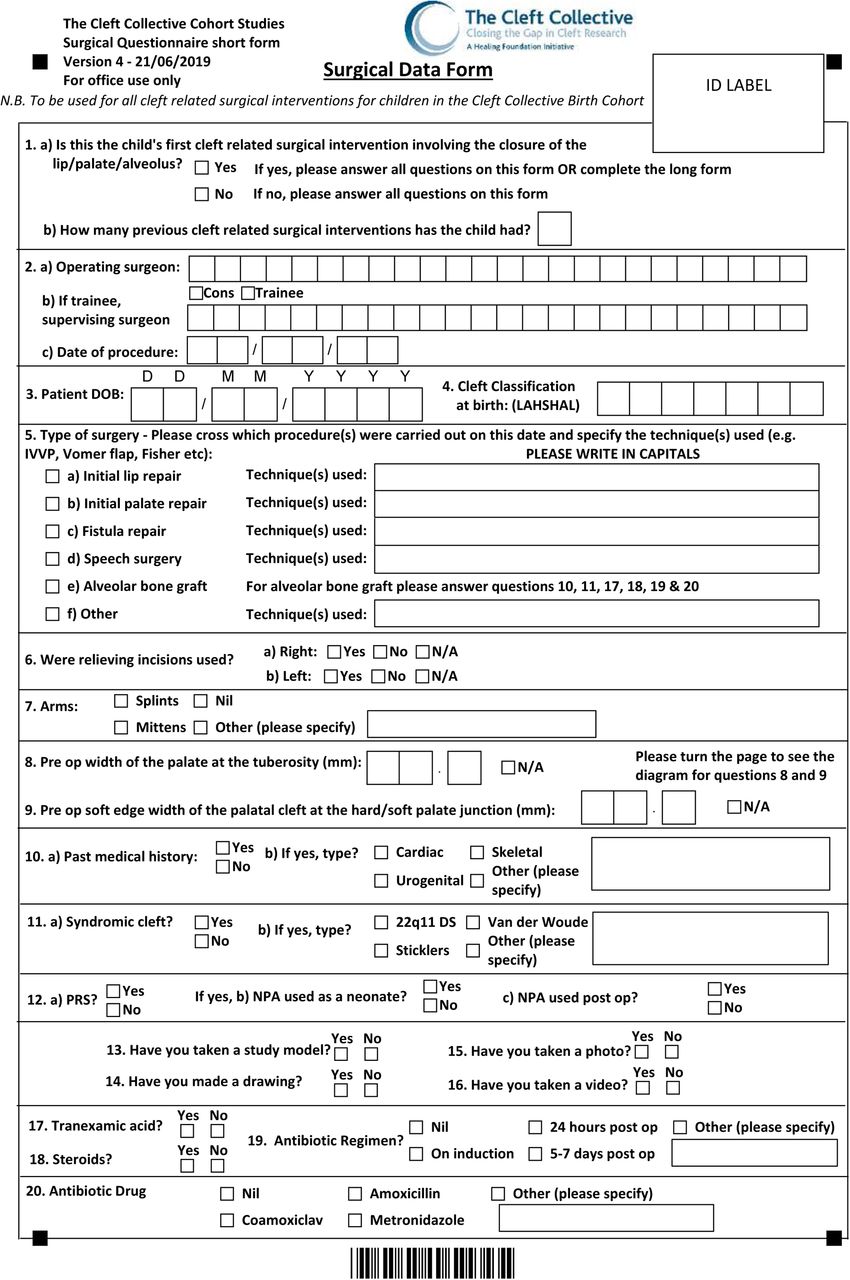
Details of surgical reconstruction were collected using the Cleft Collective Short Surgical Form (SSF) dataset, completed at the time of surgery by the operating surgeon, or delegated member of the team. The content and layout of the SSF was developed in discussion with UK cleft surgeons as a modification of the original Long Surgical Form, aiding completion by minimising the time required to complete it (see Supplementary Figure 1). Where the Long Surgical Form was completed, the truncated SSF dataset was extracted, but an analysis of the broader dataset was not included in this paper.
The SSF records patient demographics, cleft phenotype (LAHSHAL classification14 supplementary Table 1), date of surgery, reconstructive technique used (narrative) and use of perioperative antibiotics, tranexamic acid and steroids. Form data were uploaded into a database using scanning software in conjunction with manual checks. Cleft phenotype was validated with parent questionnaire and clinical data to verify accuracy.
Data synthesis
Data were stratified by cleft phenotype as unilateral cleft lip only (UCL), bilateral cleft lip only (BCL) cleft palate only (CPO), unilateral cleft lip and palate (UCLP) and bilateral cleft lip and palate (BCLP). Narrative descriptions of surgical repair techniques were categorised independently by the first and second author using published techniques of reconstruction in cleft surgery.15 Differences were resolved through discussion to reach a consensus.
Data analysis
The data were initially explored using descriptive and inferential statistics with medians (inter-quartile range (IQR)) used to describe continuous variables, and frequencies (percentages) used to describe categorical variables. The use of surgical adjuncts in primary cheiloplasty compared to soft palatoplasty was analysed using the Pearson chi-square test of independence. Odds ratios (OR), 95% confidence intervals (CIs) and P values were reported and interpreted as continuous measures of the strength of evidence against the null hypothesis.16 Due to the large sample size, we took a complete-case analysis approach and excluded missing data (See supplementary Table 2).17 Analysis was performed using the R Foundation for Statistical Computing Platform version 4.0.5 (http://www.R-project.org/).
Ethical Approval
Ethical approval to establish the Cleft Collective Cohort Study was granted by the Southwest Central Bristol Ethics Committee (13/SW/0064). Global research and development (R&D) approval was provided by University Hospitals Bristol NHS Foundation Trust. Local R&D approvals were subsequently obtained from each National Health Service (NHS) Trust. National ethical approval (IRAS project ID 259689) to analyse this subset of data (Cleft Collective Project Number CC015) was approved by the NHS Health Research Authority.
RESULTS
Participants
From July 2015 to July 2021, the Cleft Collective received data for 1782 SSFs with completed cleft phenotype data relating to the primary cleft reconstructions of 1514 individual children. Demographic information is reported in Table 1. Of the 1782 forms, 849 had indicated a primary cheiloplasty (of which 312 had simultaneous repair of the hard palate) and 933 forms had indicated a primary palatoplasty (soft palate +-hard palate) had been performed. All 16 UK cleft surgical sites provided data contributing to this study.
Demographic information of 1514 individual participants
Primary cleft lip reconstruction
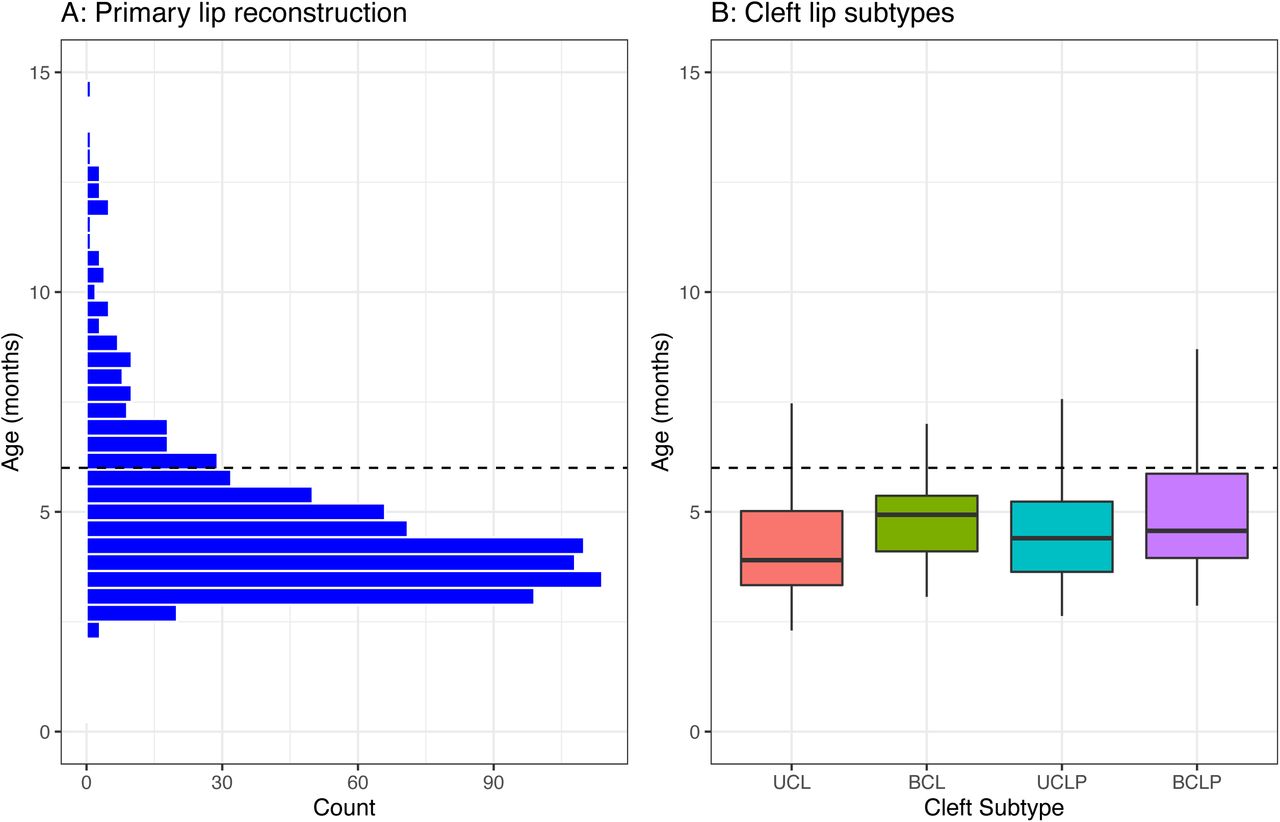
Primary cheiloplasty was recorded on 849 forms with a median age of 4.3 months (IQR 3.6 to 5.4) (Figure 1) and did not differ markedly by cleft phenotype (see supplementary Table 3). Cheiloplasties were completed by the NHS threshold of 6 months in 700 (82%) cases.8

Age at primary lip reconstruction. A: Histogram shows distribution of age at all primary lip reconstruction and B: Box and whisker plot to show age of lip reconstruction by cleft subtype (unilateral cleft lip (UCL), bilateral cleft lip (BCL), unilateral cleft lip and palate (UCLP) and bilateral cleft lip and palate (BCLP)). The dashed line represents the UK National Health Service threshold age for lip reconstruction at 6 months of age.
Reconstructive techniques documented for UCL phenotype on 475 forms, showed the anatomical subunit approximation technique (often described as a Fisher18), reported in 252 (53%) cases (Figure 2), to be the most common, with a modified technique reported in an additional 28 (6%) cases. The second most common techniques were rotation advancement; described as a Millard23 in 71 (15%) cases, with modifications (including Mohler19, Noordhof20 and Cutting21) reported in a further 85 (18%). The least common technique was the inferior triangle reconstruction (described as a Tennison22 or Randall23) in 12 (3%) cases.
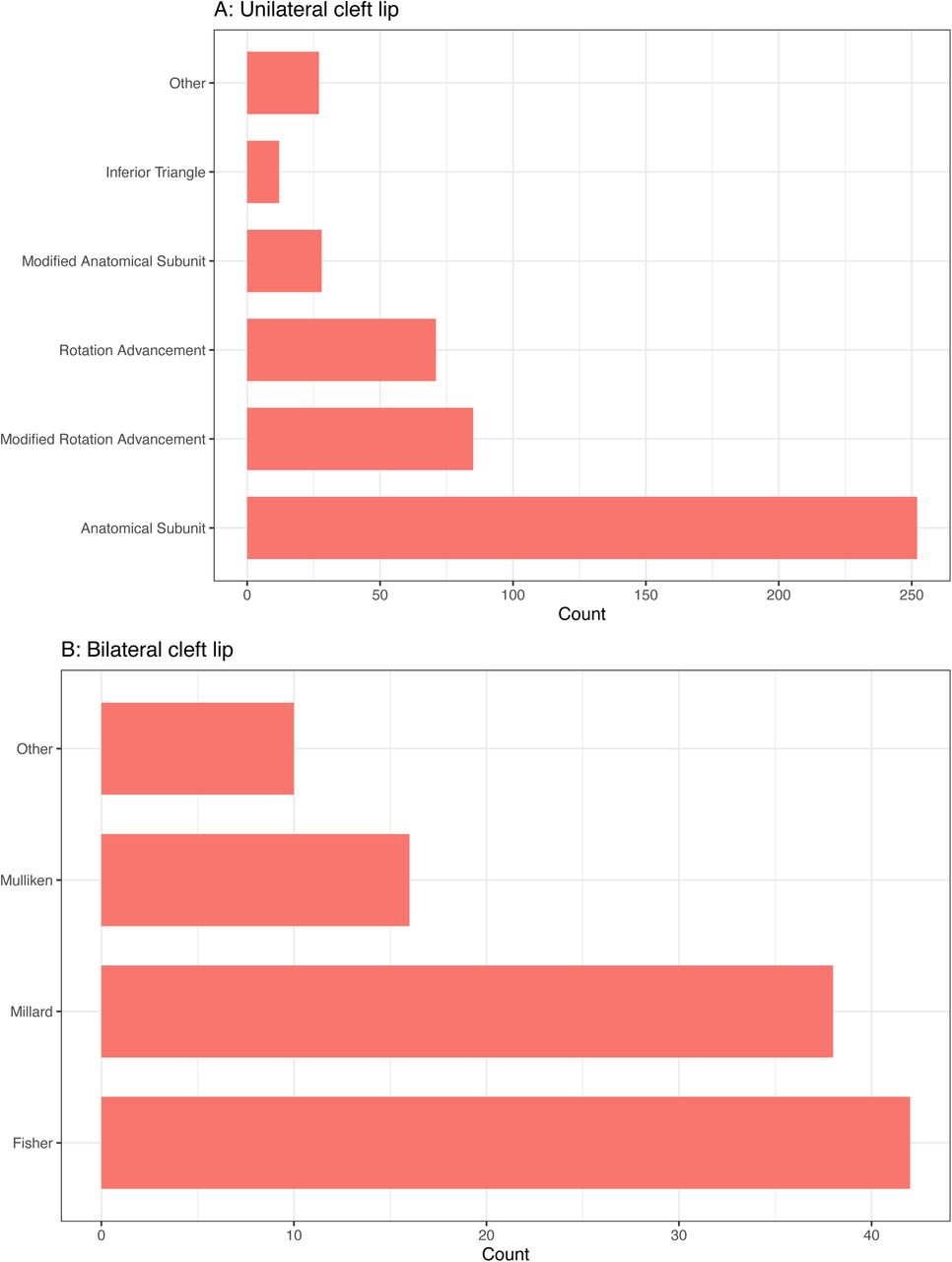
Named surgical reconstructive techniques for cleft lip. A: unilateral cleft lip reconstruction and B: bilateral lip reconstruction.
Reconstructive techniques for BCL phenotype on 142 forms documented a first stage lip adhesion in 36 cases (25%), 6 of which had additional forms submitted for subsequent definitive repair. For the 106 definitive BCL reconstructions, the most common techniques were eponymously named as Fisher24 in 42 cases (40%), Millard25 in 38 cases (36%) and Mulliken26 in 16 cases (15%).
Primary palate reconstruction
Soft palate reconstructive techniques were recorded on 614 forms at a median age of 10.3 months (IQR 8.4 to 11.9) and occurred by the NHS threshold of 13 months in 526 (84%) cases (see Figure 3).8 The intravelar veloplasty (described as Sommerlad27,28) was the most used technique in 536 cases (94%) as shown in Figure 4. Relieving incisions were reported in combination with an intravelar veloplasty in 237 of the 536 cases (44%).

Age at primary soft palate reconstruction. A: Histogram shows distribution of age at all primary soft palate reconstructions and B: Box and whisker plot to show age of soft palate reconstruction by cleft subtype (unilateral cleft lip and palate (UCLP), bilateral cleft lip and palate (BCLP) and cleft palate only (CPO)). The dashed line represents the UK National Health Service threshold age for palatoplasty at 13 months of age.

Named surgical reconstructive techniques for cleft palate A: hard palate reconstruction and B: soft palate reconstruction.
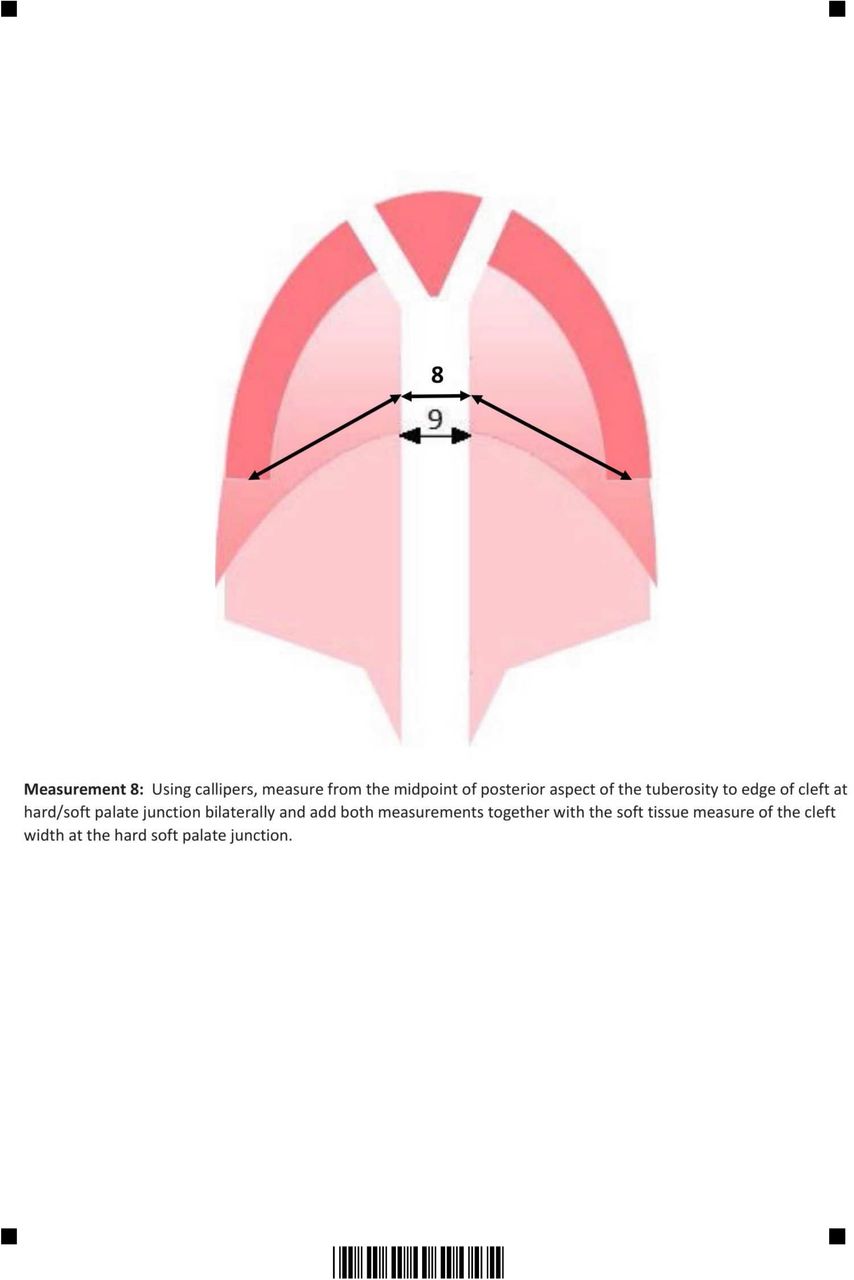
Hard palate reconstructive techniques were recorded on 203 forms; 136 (67%) were simultaneous with a primary cheiloplasty at median age of 4.4 months (IQR 3.7-5.4) as shown in Figure 5. Hard palate reconstruction exclusive of primary cheiloplasty occurred in 67 cases (33%), at a median age of 11.3 months (IQR 9.5-13.6). The vomer flap was the most used surgical technique in 171 cases (84%) as shown in Figure 4.

Age at primary hard palate reconstruction. A + B: distribution of age at reconstruction for hard palates when reconstructed simultaneously with a cleft lip, C+D: distribution of age when hard palate reconstructed without a lip repair. Cleft subtypes include unilateral cleft lip and palate (UCLP), bilateral cleft lip and palate (BCLP) and cleft palate only (CPO).
Adjuncts
Of 1758 forms, antibiotics were used peri-operatively in 1694 (96%) primary cleft reconstructions with a variety of regimens used (See Table 2). There was strong evidence to suggest antibiotics were used more frequently at-induction-only for cheiloplasties compared to soft palatoplasties (OR 1.90, 95%CI 1.53-2.37; P<0.001) and a 5–7day post-operative course antibiotics was used more commonly in soft palatoplasty (OR 0.55, 95%CI 0.45-0.69; P<0.001). Co-amoxiclav was the most frequently used antibiotic, in 1311 cases (77%) (Supplementary Table 4).
Antibiotic use within the sample overall with comparison made between cleft lip and soft palate reconstructions.
Tranexamic acid was used in 810 of 1697 (48%) primary cleft reconstructions with weak evidence to show less common usage in cheiloplasty compared to soft palatoplasty (OR 0.96, 95%CI 0.78-1.19; P=0.73) (Table 3). Steroids were used in 1120 of 1663 (67%) primary cleft reconstructions with strong evidence to show less common usage in cheiloplasty compared to soft palatoplasty (OR 0.62, 95%CI 0.49-0.79; P<0.001).
Adjuncts used at operative induction within the sample overall and comparison made between cleft lip and soft palate reconstructions.
DISCUSSION
This paper presents a unique insight into surgical pathways used in the UK for the primary reconstruction of CLP, using contemporaneous data collection at the point of care on a case-by-case basis. Previous national efforts have relied on retrospective surveys sent to surgeons to describe their practice.10,29–37
Timing
The timing of cleft lip reconstruction (IQR 4 to 5 months) and soft palate reconstruction (IQR 8 to 12 months) is similar to previous UK reports,9,35,38 and does not appear to have altered with centralisation of care over the last three decades. Where primary reconstruction was delayed beyond the NHS threshold ages, the SSF data could not elucidate the reason, but has been reported elsewhere to occur more commonly in children with co-morbidities.39 We would hope the baseline data from this study in conjunction with outcome data that is being collected will contribute to the debate around optimal timing for palatal surgery in relation to critical speech development,43 psychological and growth outcomes.44-46 The bimodal timing of hard palate closure at 4-5 months and 10-14 months confirms hard palates commonly being reconstructed in combination with a lip or soft palate and rarely as a stand-alone procedure.
Cleft Lip Techniques
The anatomical subunit approximation as described in 2005 by Fisher18 was the most used technique for UCL in 53% cases. This represents a change in the UK from 1988, where the favoured approach was the rotation-advancement.35 The anatomical subunit technique aims to leave a scar on lip subunit boundaries, achieving lip lengthening via the Rose-Thompson effect, and in most cases a small triangle above the white roll.15 The rotation-advancement technique, originally described by Millard40 in the 1950s, involves a curvilinear incision on the medial lip element to provide rotation and a triangular flap on the lateral element to provide advancement.15 Modifications of the rotation-advancement were used more frequently in this study compared to the original Millard technique itself. Rotation-advancement modifications recorded on the surgical form included Mohler,19 which extends the incision into the columella to enhance the lip lengthening and Noordhof20,41 which adds a small triangle above the white roll and a laterally based vermillion triangle.
Globally the rotation-advancement technique, and its modifications, is reported to be the most used for UCL repair.29,31–33 It is described as a “cut as you go” technique, whereas the anatomical subunit has been termed a “measure twice, cut once” technique.42 Given its relatively recent introduction in 2005, the popularity of the anatomical subunit reconstruction in the UK is quite remarkable. The reason for its adoption cannot be ascertained from data in our study but a surgeon’s choice of UCL repair technique has been previously described to be a hybrid of training, experience and imagination.43
A first stage lip adhesion was recorded in 25% cases of BCL in this study, which is higher than the 11% of surgeons reported to use a staged approach in the USA, where pre-surgical orthopaedics are commonly utilised.30 There was greater variation in techniques used for definitive BCL reconstruction compared to UCL in this study. The three eponymous techniques of Fisher24, Millard25 and Mulliken26 all share a common principle of recruiting tissue from the lateral lip elements to recreate the Cupid’s bow and vermillion across the prolabium.44 The Manchester45 repair uses vermillion native to the prolabium but was not reported in our cohort, in contrast to its use by 12% of US surgeons.30 The use of Millard and Mulliken techniques for BCL reconstruction does not come as a surprise due to the longevity and volume of the technique descriptions in the literature.44 The common use of Fisher’s approach to the BCL suggests a rapid adoption following its more recent description in 2009.24
Cleft Palate Techniques
Clefts of the soft palate were reconstructed almost exclusively using the intravelar veloplasty (94% cases) and this is a change from 1988 in the UK, where the most used technique was the straight-line closure described by Von-Langenbeck.35 The intravelar veloplasty, described initially in 1970 by Kriens46 was popularised in the UK by Sommelad following his publications in 200327,28 on the radical method of muscle retro-positioning and use of the operating microscope. The von Langenbeck47 technique of incisions along the medial cleft margins with lateral incisions can be used in combination with an intravelar veloplasty.48 The UK appears relatively unique in its sole adoption of the intravelar veloplasty for soft palate reconstruction, as, in comparison, the double-opposing z-plasty described by Furlow49 often has equivalent popularity elsewhere.30,31,34
Clefts of the hard palate were reconstructed with a vomer flap in 84% cases, as first described by Pichler.50 A vomer flap can be used variably; performed simultaneously with a cheiloplasty in a single-layered closure of the nasal mucosa, or in conjunction with a soft palate repair where a vomer flap(s) will likely reconstruct the nasal mucosa within a two-layered closure. Asher-McDade and Shaw (1990) noted an increase in its popularity35 for anterior hard palate reconstruction in the UK. Globally, surgeons have reported using a variety of techniques for reconstruction of the hard palate which commonly include the pushback technique described by Veau-Wardill-Kilner51–53 and the Bardach54 two-flap technique.10,31,33,34 The sequence of reconstructing the lip and anterior hard palate first followed by the soft palate later is in accordance with the Oslo protocol and has been previously described as the most commonly used in the UK.7,9 There is not yet global consensus on the optimal protocol for a cleft of the lip and palate.15,55–57
Adjuncts
Reconstructions of CLP are classified as clean-contaminated surgical procedures with gram-positive organisms reported at the surgical site in multiple studies.58,59 Although little evidence or guidance is available to support the use of prophylactic antibiotics in elective cleft surgery, prophylactic intravenous antibiotics were used in 97% of cases within this cohort, no change from a survey of UK cleft surgeons in 2004, which reported most prescribing prophylactic antibiotics.58 We found strong evidence to suggest UK cleft surgeons more commonly prescribe a 5-7day post-operative course of antibiotics following soft palatoplasty than cheiloplasty, possibly reflecting concerns of intra-oral infection leading to palatal fistulae. A randomised trial conducted in India compared two groups of cleft patients, being given a single pre-operative dose of antibiotics or an additional five days of post-operative antibiotics. The study concluded, in spite of high loss to follow up, there was no difference in the early complication rate. Some evidence suggested a reduced fistula rate if post-operative antibiotics were given in this setting.60
Tranexamic acid was used intravenously on induction in half of the cases in this cohort, with weak evidence to show any difference in use between soft palatoplasty and cheiloplasty. The efficacy of tranexamic acid in palatoplasty has been evaluated in two randomised trials with one concluding that tranexamic acid markedly improved surgeon reported satisfaction61 and the other reporting no difference in in the amount of blood loss.62
Steroids were used intravenously on induction in 67% cases in this cohort, with strong evidence to show use more commonly for soft palatoplasty than cheiloplasty and this may be due to the perceived benefit to the child in terms of reducing post-operative airway swelling and improving oral intake.63 A randomised study to compare 0.25mg/kg steroid on induction to placebo in palatoplasty reported reductions in airway distress and post-operative fever associated with the steroid group.64 A more recent correspondence described a randomised study of 0.5mg/kg IV dexamethasone on induction in palatoplasty and reported an improvement in oral intake in the steroid group.65
Strengths and Limitations
This study describes the operative pathways used within the centralised UK cleft services without the risk of recall bias associated with surgeon questionnaires previously used in this field. The large number of participants, inclusion of all CLP subtypes and contributions from all cleft centres in the UK ensures this cohort is broadly representative of UK cleft practices.
Reporting bias should be considered a limitation, as one description of an operation by name might not match either the original description or another’s interpretation of the same operation. There are limitations regarding the extent to which the intra-operative decision-making process and the techniques used by the cleft surgeon can be gleaned from SSF data. The principles involved with the reconstruction of an orofacial cleft include planning, wide surgical release and reconstruction of component parts in layers.42 The name of an operation gives an indication of the planning stage but no information on the other principle elements of the reconstruction. The SSF did not facilitate documentation of the approach to the nose in primary cheiloplasties and this is an important part of the reconstruction.66
CONCLUSION
This paper presents a unique insight into UK cleft surgical pathways, providing information on the timing of surgical interventions, the operative techniques, and the use of surgical adjuncts. The provision of cleft care in the UK was changed significantly with the implementation of centralisation 20 years ago. Although the timing of primary CLP surgery has not changed, there has been a paradigm shift in the surgical techniques used. The anatomical subunit approximation technique has gained in popularity for UCL repair and the intravelar veloplasty is by far the most commonly used method for soft palate repair. The findings from this report can be used in conjunction with growing outcome data from national registries to analyse the effectiveness of the cleft protocols in use within the UK.
Data Availability
All data produced in the present work are contained in the manuscript
Supplementary data

Cleft Collective Short Surgical Form
Stratification by cleft phenotype was performed according to the LAHSHAL classification. Surgeons noted the LAHSHAL on the Cleft Collective Surgical from and this was verified with clinical data to check for accuracy. We were not able to differentiate between incomplete and complete clefts in this study, therefore code for incompletes (denoted by non-capitalised letters) was included.
Missing data from the 1782 Cleft Collective Short Surgical Form dataset included in this study
Age in months at primary cleft reconstruction stratified by cleft phenotype. Cleft phenotypes are stratified according to the LAHSHAL classification into All (any cleft lip and/or palate), UCL (unilateral cleft lip only), BCL (bilateral cleft lip only), CPO (cleft palate only), UCLP (unilateral cleft lip and palate) and BCLP (bilateral cleft lip and palate). Age in months is reported in median, lowest age, highest age, first quartile (1stQ), third quartile (3rdQ) and interquartile range (IQR)
Antibiotics prescribed in the peri-operative period for primary reconstruction of a cleft lip and/or palate.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
ACKNOWLEDGEMENTS
This publication involves data derived from independent research funded by The Scar Free Foundation (REC approval 13/SW/0064). We are grateful to the families who participated in the study, the UK NHS cleft teams, and The Cleft Collective team, who helped facilitate the study. The views expressed in this publication are those of the author(s) and not necessarily those of The Scar Free Foundation or The Cleft Collective Cohort Studies team.
Footnotes
Financial Disclosure: Matthew Fell is supported by the VTCT Foundation for a research fellowship with the Cleft Collective. All other authors did not receive support from any organisation for the submitted work. Funders had no role in the study design; in the collection, analysis and interpretation of data; in the writing of the report; and in the decision to submit the article for publication. The authors can confirm their independence from funders and that all authors had full access to all of the data (including statistical reports and tables) in the study and can take responsibility for the integrity of the data and accuracy of the data analysis.
COPYRIGHT LICENCE The Corresponding Author has the right to grant on behalf of all authors and does grant on behalf of all authors, a world-wide licence to the Publishers and its licensees in perpetuity, in all forms, formats and media (whether known now or created in the future), to i)publish, reproduce, distribute, display and store the Contribution, ii)translate the Contribution into other languages, create adaptations, reprints, include within collections and create summaries, extracts and/or abstracts of the Contribution, iii)create any other derivative works(s) based on the Contribution, iv)to exploit all the subsidiary rights in the Contribution, v)the inclusion of electronic links from the Contribution to third party material where-ever it may be located and, vi)licence any third party to do any or all of the above.
REFERENCES



