
ABSTRACT
Background Buprenorphine is an evidence-based treatment for Opioid Use Disorder (OUD). Standard buprenorphine induction requires a period of opioid abstinence to minimize risk of precipitated opioid withdrawal (POW). Our objective was to study the impact of the increasing presence of fentanyl and its analogs in the opioid supply of the United States, on buprenorphine induction and POW, using social media data from Reddit.
Methods This is a data-driven, mixed methods study of opioid-related forums, called subreddits, on Reddit to analyze posts related to fentanyl, POW, and buprenorphine induction. The posts were collected from seven subreddits using an application programming interface for Reddit. We applied natural language processing to identify subsets of salient posts relevant to buprenorphine induction, and performed manual, qualitative, thematic analyses of them.
Results 267,136 posts were retrieved from seven subreddits. Fentanyl mentions increased from 3 in 2013 to 3870 in 2020, and POW mentions increased from 2 (2012) to 332 (2020). Manual review of 384 POW-mentioning posts and 106 ‘Bernese method’ (a microdosing induction strategy) mentioning posts revealed common themes and peoples’ experiences. Specifically, presence of fentanyl caused POWs despite long abstinence durations, and alternative induction via microdosing were frequently recommended in peer-to-peer discussions.
Conclusions This study found that increased social media chatter on Reddit about POW correlated with fentanyl mentions. A subset of posts described microdosing as a self-management strategy to avoid POW. Reddit posts suggest that people are utilizing these strategies to initiate buprenorphine due to challenges arising from fentanyl prevalence in the opioid supply.
Highlights
Increase in mentions of precipitated opioid withdrawal (POW) on Reddit from 2012 to 2021 was closely correlated with the increase in fentanyl mentions.
Experiences of precipitated opioid withdrawal (POW) were described by individuals who reported sufficient periods of abstinence by standard buprenorphine induction protocols.
People with Opioid Use Disorder (OUD) on Reddit are using and recommending microdosing strategies with buprenorphine to avoid POW.
People who used fentanyl report experiencing POW following statistically longer periods of abstinence than people who use heroin.
1. BACKGROUND
Buprenorphine (Suboxone®, a combination of buprenorphine and naloxone) is an effective, evidence-based treatment for patients with opioid use disorder (OUD).1 Buprenorphine has unique pharmacologic properties: it is a partial mu-opioid receptor agonist and has very high affinity for the mu-opioid receptor.2 Therefore, to avoid buprenorphine from displacing lower affinity opioids (e.g., heroin, oxycodone) from the opioid receptor, patients seeking buprenorphine treatment must wait until they start experiencing mild withdrawal symptoms before initiating standard dosing regimens.2 If buprenorphine is initiated prior to withdrawal onset, it can displace residual opioids, causing an uncomfortable and sometimes severe acute withdrawal syndrome known as precipitated opioid withdrawal (POW).3 POW has been defined as an increase in the Clinical Opiate Withdrawal Scale (COWS), which measures the signs and symptoms of opioid withdrawal, of 6 or more while initiating buprenorphine.4 Fear of POW poses a barrier to both clinicians and patients to initiate buprenorphine.5 Additionally, the necessity of waiting until withdrawal symptoms occur before initiating buprenorphine creates a hurdle for patients and increases the risk of failed treatment initiation.2
Multiple recently published reports from patients and providers suggest that POW can occur even after waiting the recommended amount of time in patients with a history of fentanyl use.3,5 It has been proposed that this phenomenon may occur due to the high lipophilicity of fentanyl, resulting in a long tail of elimination after chronic use.6 Despite fentanyl’s therapeutic use as a short acting analgesic, one study showed that in patients with OUD and chronic fentanyl use, urinary metabolites of fentanyl could be detected 2-3 weeks after last use when hospitalized in a treatment program.7 One potential alternative approach to avoid these pitfalls is a microdosing strategy which involves overlapping induction of buprenorphine in very small doses while still using full agonist opioids, of which the ‘Bernese Method’ is the first described regimen. However, several different regimens have been described in the medical literature.2,6,8,9 While there is growing literature on this subject, many people with OUD have discovered these methods through their own lived experiences.10 Paradoxically, POW is not a consistent phenomenon, as fentanyl use is highly prevalent in some regions of the United States now and buprenorphine initiation is not routinely complicated by POW in most areas.
The primary aim of this study was to describe how people with OUD are exploring and sharing information about emerging buprenorphine initiation methods to avoid precipitated withdrawal. Since it is difficult to obtain a large cohort of people with OUD to study their buprenorphine initiation experiences, we utilized public social media data from Reddit to conduct this study.11 Reddit is one of the most popular and fastest growing social networks currently, with over 430 million monthly active users (in comparison, Twitter has ∼390 million monthly active users).12 Reddit allows users to remain completely anonymous if they desire.13 Due to this anonymity, it is a major hub for the open discussion of sensitive or stigmatized topics. Consequently, there is a considerable amount of self reported information on this social network on substance use disorder (SUD) including OUD, and a number of recent studies on the topic have utilized Reddit data.15–17 We designed this study to be primarily data-driven, and hypotheses were generated and refined iteratively based on exploration of the data. The specific research questions that we attempted to answer via the analyses described in this study are as follows:
What is the association between fentanyl and posts about POW?
What are the common themes in Reddit discussions regarding POW?
What self-management strategies are people with OUD utilizing to avoid POW?
How can the experiences of people with OUD be used to better understand microdosing of buprenorphine?
2. METHODS
2.1 Data collection
Seven opioid-related subreddits on Reddit were selected for data analysis (r/fentanyl, r/heroin, r/microdosing, r/opiates, r/OpiatesRecovery, r/OurOverUsedVeins and r/suboxone). We selected these subreddits based on consensus among the authors regarding their relevance for the objectives of this study, after previewing several subreddits for thematic content and total number of posts. The number of subscribers for each of these subreddits and their inception years are provided in Table A1 of the Supplementary material. Among these subreddits, r/opiates is the oldest (created in 2009) and r/fentanyl is the newest (created 2015). We excluded other potentially relevant subreddits because they focused on a wider range of substances (e.g., r/Drugs) or were primarily dedicated to recreational use and experimentation (e.g., r/DrugNerds).
From the chosen subreddits, we collected all the posts that were publicly available and were retrievable via the PRAW Python application programming interface (API) for Reddit.17 We searched for mentions of ‘precipitated withdrawal’ and ‘Bernese method’ in all the posts within the retrieved posts from the subreddits. We extracted posts that mentioned these phrases for further manual analysis. The iterative, data-driven strategy of data retrieval, filtering, and analysis is depicted as a flow diagram in Figure 1.

Flow diagram illustrating the extraction, analyses, and steps included in this study, along with the number of posts included where relevant. Starting with a set of predetermined key phrases (a), we generated their lexical variants (b) and computed their frequencies in data from the seven included subreddits (c). Posts about precipitated withdrawal and Bernese method were filtered (d) and manually coded for themes (e). Topics of interest were discovered during the manual coding (f) and natural language processing methods were applied to retrieve more posts related to the topics (g). Descriptive analyses were performed on the retrieved posts (h). NLP: natural language processing.
2.2 Analyses of distribution of terms and posts
Initial statistical analysis included computing the total number of posts retrieved, total number of mentions of ‘precipitated withdrawal’ or its lexical variants, total number of mentions of ‘Bernese method’ or its lexical variants, and the total number of ‘fentanyl’ mentions or its lexical variants and analogs. Texts from the subreddits were lowercased prior to searching and no other preprocessing of text was performed. Counts were grouped by year to evaluate for observable popularity trends. We used an automatic tool to generate lexical variants18 and manually added variants that were not lexically similar but often used in the subreddits (see Table A2 of Supplementary material for all lexical variants).
2.3 Thematic analysis
Two toxicology experts (JL and JP) reviewed a small sample of posts to identify relevant categories into which the posts could be classified. Categories were developed using a modified grounded theory approach.19,20 Some candidate themes were collapsed if (i) they were too similar, (ii) they were too generic and could be described by combinations of the other themes, or (iii) the number of posts belonging to such categories was too low. This iterative process finalized eight themes/categories and one additional category (other/none of the above) for posts that could not be labeled. Table 1 presents the themes and their definitions.
Codes for manual characterization, their definitions. Examples are provided in Table A3 of the Supplementary material.
A guidebook was developed to code a larger sample of posts (see Table A3 in the Supplementary material for sample posts). One annotator (WH) coded posts mentioning precipitated withdrawal or Bernese method and the codes were reviewed by the other authors of this study. The process was a multi-label classification—each post could be assigned one or many codes. Posts that did not meet the criteria for any theme were labeled as ‘other/none of the above’. In addition to assigning these codes to the posts, the annotator noted if posts (1) represented personal experiences, and (2) referred to fentanyl.
Following the annotation, individual coded posts were reviewed by authors with expertise in the treatment of patients with OUD (ASp and JP) for emergent themes. Through discussion, the authors identified and agreed upon the dominant themes within each code and their relationship to one another. Themes most relevant to each code were decided by expert consensus and two themes were chosen for further investigation.
2.3.1 Time to precipitated withdrawal
To better understand the association between fentanyl and POW, we analyzed a subset of the posts from people who reported to have experienced POW. We specifically attempted to identify time intervals between the last opioid use and buprenorphine use, and the opioids that were associated with these time intervals. Posts that were unrelated to OUD, did not include specific timing intervals or did not specifically mention that POW was experienced were excluded. We noted all the opioids mentioned within the reviewed posts (e.g., fentanyl & analogs, heroin, oxycodone), and if the specific opioid used prior to buprenorphine was not mentioned, it was categorized as ‘unknown’. The time intervals, between last opioid use and buprenorphine use, that resulted in precipitated withdrawal were compared for different opioids (e.g., fentanyl & analogs vs. heroin).
2.3.2 Bernese method microdosing strategies
We applied natural language processing (NLP) to curate a set of posts that were likely to contain all the relevant details about microdosing regimens, and we manually reviewed these curated posts. Guided by the toxicologists (JP, LN JL) in this study, we developed NLP expressions to detect patterns in texts that indicated the presence of (i) an opioid (e.g., ‘suboxone’, ‘subs’, ‘fent’), (ii) a dosage (e.g., ‘1 mg’, ‘0.5mg’), and (iii) a duration (eg., ‘each day’, ‘12 hrs’, ‘week’). To detect the opioids, we used their generic names, trade names (for prescription opioids), street names and automatically-generated misspellings. To detect dosages and durations, we applied regular expressions. The expressions and spelling variants are provided in Table A4 of the Supplementary material. Only posts that matched all three of the abovementioned types of expressions were manually reviewed to identify if they were referring to buprenorphine-related microdosing and understand the regimens described.
3. RESULTS
3.1 Distribution of terms, posts and users
We were able to retrieve a total of 267,136 posts from the seven subreddits. In line with the growth in popularity of Reddit, the number of posts increased significantly over time. The first post was from May 19, 2012 and the last post was from April 23, 2021 (i.e., the date when the data was collected). Among the years for which we had full data, 2020 had the highest number of posts: 113,901 in 2020, compared to 245 posts in 2012. 43,986 posts were collected in less than four months of 2021. Similarly, the total number of people posting in these subreddits steadily increased over time: 21,286 unique users posted in 2020 and 10,174 users posted in less than the first four months of 2021. Full distributions of posts and users per year are shown in Figures A1 and A2 of the Supplementary material.
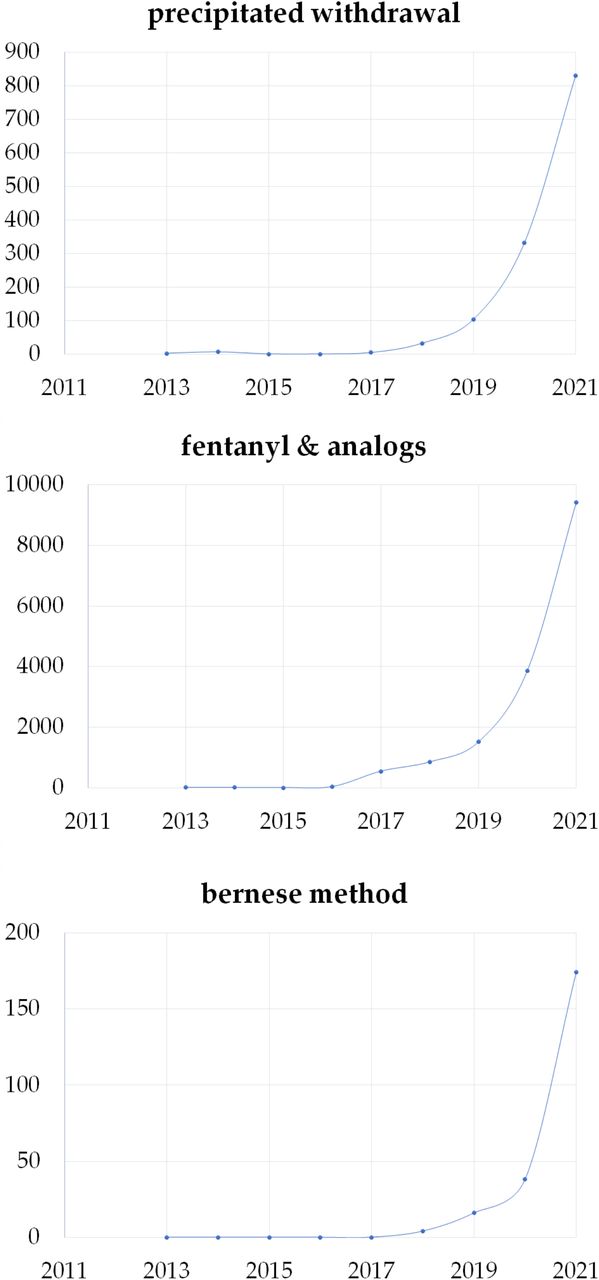
The total number of mentions of fentanyl and analogs (eg., carfentanil), POW, and the Bernese method have also steadily increased over the years. The number of posts mentioning fentanyl and analogs increased from 3 in 2013 to 3870 in 2020, and 2917 in less than four months in 2021. The number of posts mentioning POW increased from 2 in 2012 to 332 in 2020 (257 in 2021). As depicted in Figure 2, for fentanyl and analogs, mentions were relatively rare before 2017 and steadily increased. POW mentions appeared in 2018, with large increases in later years. We did not find any mentions of the ‘Bernese method’ before 2018 and it is the only expression that has a higher mention count within the first four months of 2021 compared to 2020. In Figure 2, the values for the year 2021 are estimates based on the number of days of the year up to the date of collection (i.e., April 23). Spearman correlation between ‘precipitated withdrawal’ and ‘fentanyl/analog’ yearly mentions was 0.882 (p=0.0016) and between ‘fentanyl/analog’ and ‘Bernese method’ yearly mentions was 0.917 (p=0.0005) from 2013 to 2021.

Yearly distributions of mentions of fentanyl and analogs (top), precipitated withdrawal (middle), and Bernese method (bottom) within our chosen six subreddits. Counts of distinct lexical variants are aggregated. For 2021, the values presented are estimates based on the number of days that had elapsed up to the day of collection (April 23; 113 days). The true count is multiplied by the fraction  .
.
3.2 Thematic coding results
We manually coded 384 posts mentioning ‘precipitated withdrawal’ and 106 posts mentioning ‘Bernese method’. Table 2 presents the distribution of codes assigned to each set of posts. Among posts about POW, the most common theme was specific triggers of POW (232 posts; 60.4%), followed by buprenorphine dosing strategies (140 posts; 36.5%) posts, and experiences of opioid use disorder (134 posts; 34.9%). Among posts about the Bernese method, the most common theme was buprenorphine dosing strategies (47 posts; 44.3%), followed closely by experience of opioid use disorder (43 posts; 40.6%), and specific triggers of POW (38 posts; 35.8%). 36 (34.0%) posts recommended the Bernese method without any further context. 235 (61.2%) posts mentioning POW and 67 (63.2%) posts mentioning the Bernese method referred to personal experiences. 121 (31.5%) precipitated withdrawal posts and 40 (37.7%) Bernese method posts referred to fentanyl or analogs.
Distribution of manually-assigned codes in the sample of precipitated withdrawal and Bernese method reviewed.
3.3 Descriptive analysis results
There were many posts that gave advice regarding the use of adjunctive non-opioid medications to treat the symptoms of opioid withdrawal.
“Uppers def. make opiate withdrawals worse my friend. The only thing that helps with fentanyl withdrawals, are (Benzodiazepines) such as; Xanax, Ativan, Valium Etc.”
Some of these posts were advice for using the adjuncts to prolong the abstinence period before initiating buprenorphine due to the concern that POW would occur if buprenorphine was taken too early. Many of the posts discussed the pharmacology of fentanyl and buprenorphine, in fact many posts shared research articles related to the pharmacokinetics of these drugs.
“Fentanyl is a full mu antagonist, which means your opiate receptors are full (think of fentanyl as a full glass of water and buprenorphine as a half glass of water) when you take buprenorphine too soon, it instantly removes the full mu antagonist (fentanyl) and replaces it with a partial mu antagonist (buprenorphine) which will put you into something called “precipitated withdrawl.”“
Many of the posts described the time intervals between last opioid use and buprenorphine initiation, the doses of buprenorphine, and whether the posters had positive experiences overall or negative experiences like precipitated withdrawal. There were several posts that recommended the Bernese method as a strategy for initiating buprenorphine.
“Bernese method is the only way I have ever been able to get on subs after taking fent. Fent is in it’s own category and is a whole other beast than any other opiate when trying to get on subs.”
Overall, posts contained detailed descriptions of first-hand experiences with fentanyl, discussions of complex pharmacology topics, and the desire to seek alternatives for the treatment of their OUD or avoiding POW. Further examples of the quotes that illustrate themes that emerged from the quotes can be found in Table A3.
3.4 Time to precipitated opioid withdrawal
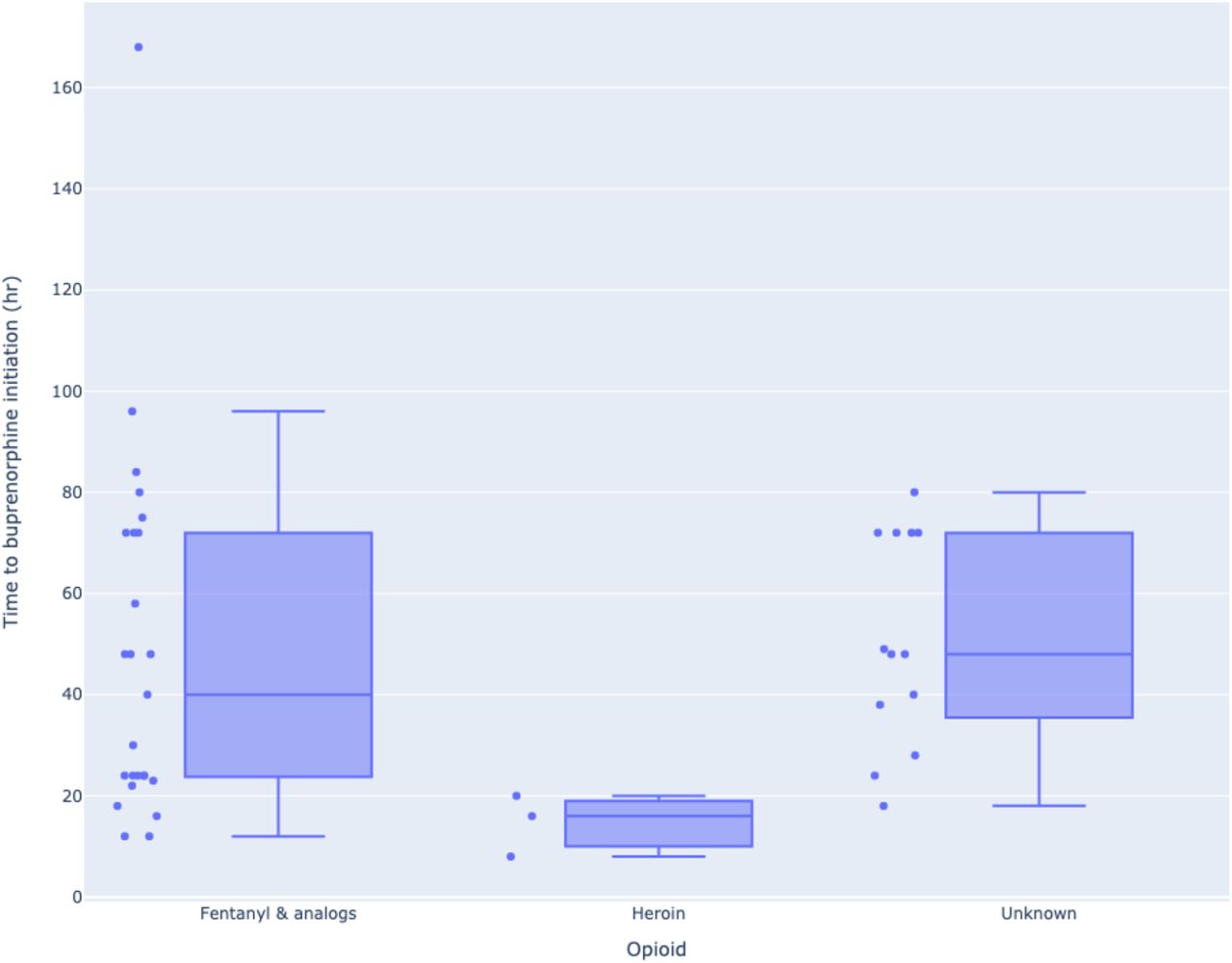
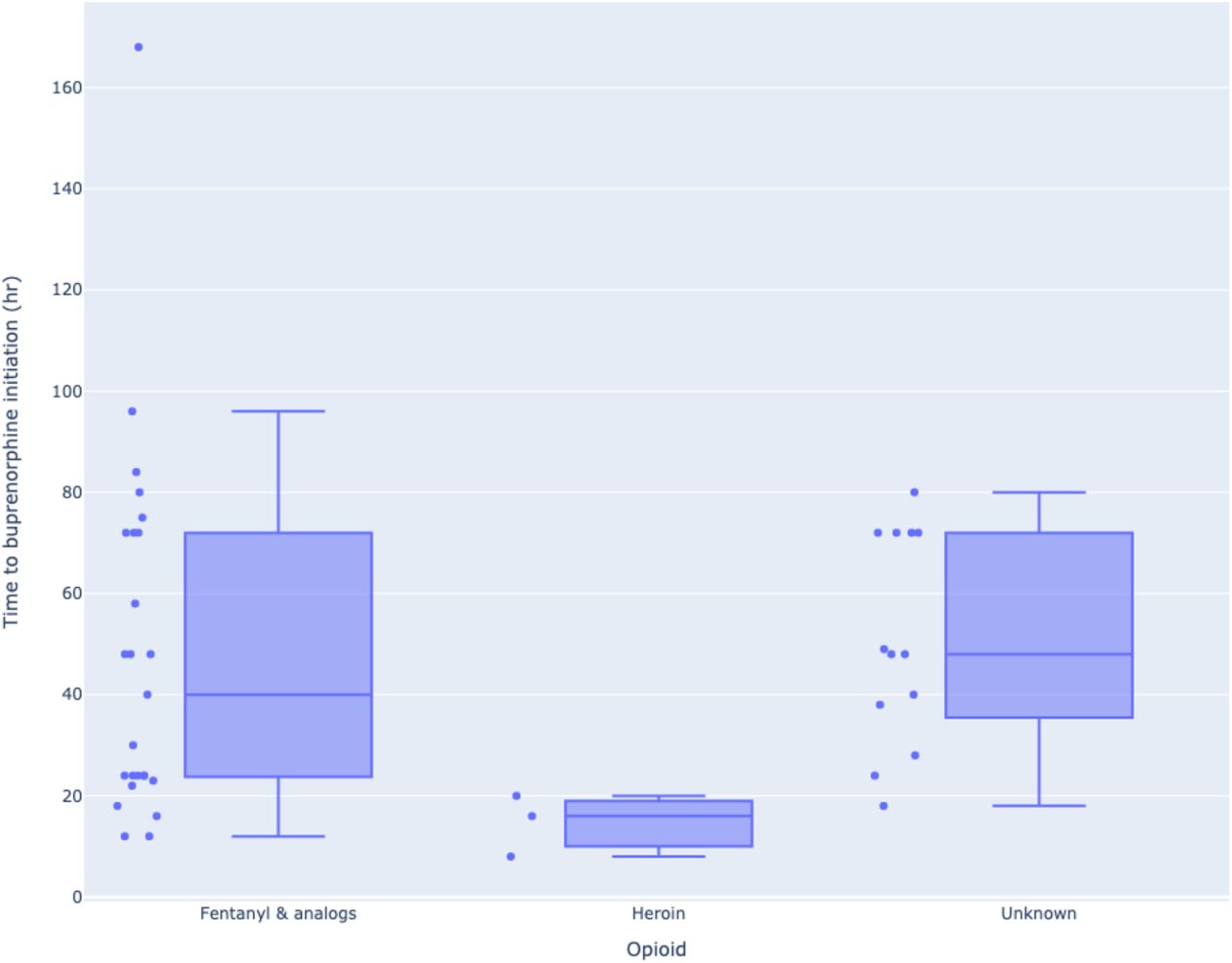
Figure 3 summarizes the durations between last opioid use and buprenorphine initiation that led to POW. We found 25 posts that referred to fentanyl or its analogs and specified the durations, 13 posts that specified durations but did not explicitly mention which opioid caused it, and 3 posts that attributed POW to heroin. The boxplots show that the durations for fentanyl vary considerably, with the median being 40 hours. The longest abstinence duration after which a user expressed experiencing precipitated withdrawal was 168 hours (7 days). The durations were considerably shorter for heroin (median: 16 hours) and similar for the unknown category, which most likely included fentanyl. The reported time intervals between last fentanyl use to buprenorphine initiation that led to POW were compared with the reported intervals for heroin using the Wilcoxon ranked sum test. The intervals for fentanyl were found to be statistically significantly longer (p=0.02) despite the small number of posts mentioning heroin.
{kind=link}
{kind=link}
{kind=link}
Boxplots showing the distributions of time between last opioid use to buprenorphine initiation that led to precipitated withdrawal for fentanyl & analogs, heroin and unspecified opioids.
3.5 Bernese method microdosing strategies
Only 11 posts matched all three types of NLP patterns to detect posts describing microdosing strategies. Some posts that matched the patterns partially lacked complete details about the microdosing strategies. For example, some posts referred to sources on the Internet for details about the specific microdosing regimens. For posts that contained sufficient details, we extracted and summarized relevant details. A sample of summarized strategies is presented in Table 3. These posts are paraphrased/edited for easier comprehension. The strategies extracted had a range of initial buprenorphine dosing ranging from 0.125mg to 1mg, and gradually increased over a “few day” to 8 days.
Buprenorphine microdosing regimens discussed on subreddits
4. DISCUSSION
In this study, we analyzed anonymous posts from the social media platform Reddit to better characterize specific aspects of the current opioid crisis, which is now dominated by fentanyl use. Using Reddit data, we found that POW related posts increased in parallel with increasing fentanyl related posts over the studied timeframe of 8 years. We employed NLP methods to evaluate shared experiences by people with OUD about buprenorphine initiation strategies in the era of rising fentanyl prevalence. We found numerous anecdotal reports of buprenorphine microdosing strategies specifically to avoid POW. Few published studies have reported on the contemporary experiences and challenges of people with OUD. Specifically, there is a paucity of studies focusing on people who primarily use fentanyl and seek to initiate buprenorphine. Some recent studies have suggested that treatment seeking people with OUD are often thwarted by POW despite self-reported abstinence periods of up to 96 hours.3,10
This study adds to the body of literature focusing at the intersection of social media and OUD by using NLP to uncover discussions about a medical phenomenon, precipitated opioid withdrawal, associated with buprenorphine initiation after chronic fentanyl use. Similar to Graves et al. (2019), this study draws from the experiences and voices of patients with OUD, often shared anonymously, to address evolving buprenorphine initiation strategies.16 Our finding of multiple dosing regimens of buprenorphine microdosing (Table 3) is comparable to the multiple different dosing regimens described in case reports with a few exceptions.2,3,8,9 For example, the lowest dose described in our data started at 0.125 mg of buprenorphine. Hammig et al. (2016) describe one of the lowest starting doses of buprenorphine at 0.2 mg of buprenorphine, although their microdosing method was developed to avoid withdrawal during an abstinence period rather than avoiding POW among people with history of fentanyl use.2 For the regimens we found that specified the time duration of microdosing initiation, the range was from 5-8 days, comparable to existing medical literature.2,3,8 While Klaire et al. (2019) describe a strategy for an in-hospital rapid uptitration of buprenorphine in 3 days, the largest study of outpatient treatment by Moe et al. (2020), employed a 7 day incremental uptitration initiated in the emergency department.8,9 While there is insufficient evidence to recommend a specific dosing regimen, these experiences should encourage clinicians who treat OUD to take a patient symptom guided approach. Currently a randomized control trial has been proposed to compare a rapid micro-induction of buprenorphine versus a standard buprenorphine induction in Vancouver, Canada.21
We also found additional evidence of increasing amounts of fentanyl in the opioid supply. The dramatic increase in posts mentioning fentanyl starting in 2016 is corroborated by reports of increases in fentanyl related overdose fatalities starting in 2015 and continuing today.10,22-24 While forensic toxicologic data of post-mortem samples may lag behind actual changes in the opioid supply, particularly if laboratories are not testing for illicitly manufactured fentanyl analogs, social medial may offer an opportunity to proactively surveil the drug supply based on the experiences that people with OUD voluntarily share.11,24,25
Because of its emphasis on anonymity coupled with its relatively recent rise in popularity, Reddit affords researchers the opportunity to explore unexpected effects of the changing opioid supply that might not be apparent at the individual patient level.11 In our study, an association was observed between the increasing number of posts about fentanyl and the number of posts about POW. This association adds to a small body of evidence that buprenorphine initiation might present unexpected challenges in the era of fentanyl. The observation that fentanyl use could be associated with POW with standard buprenorphine initiation was also reported in a case series by Antoine et al. (2021) that included four patients who primarily used fentanyl, two of whom developed POW after a standard induction protocol and two who did not develop POW with a microdosing protocol.3 When reviewing individual posts, we found that many discussed personal experiences with POW and associated that with fentanyl being present in the drug supply. Additionally, many posts included in-depth discussions about fentanyl and buprenorphine pharmacology, as the posters attempted to identify the causes of their experiences. Some posts cited peer-reviewed research, but many included information that was incorrect or misleading.
In this study, we found that the median time from last fentanyl use to buprenorphine initiation among people who experienced POW was 40 hours. This suggests that many patients are potentially at risk of POW after much longer periods of abstinence than the 12-24 hours recommended with conventional buprenorphine induction in non-fentanyl using populations.2,9 A qualitative study by Silverstein et al. (2019). of participants with OUD in the Dayton, Ohio region described multiple instances of participants who used fentanyl becoming frustrated at buprenorphine for causing POW, making them less likely to engage in buprenorphine therapy.10 Participants described experiencing POW up to 72 hours from last opioid use, which is consistent with the range of posts we found (figure 3).10 In our time interval analysis, we found that people who used fentanyl experienced POW after a statistically significant longer abstinence period compared to people who used heroin. Interestingly, there were many more posts in the fentanyl group compared to the heroin group, which may reflect an increased incidence of developing POW in this group or a higher prevalence of fentanyl use among Reddit users. Similar to the Silverstein et al. (2019) study, we found posts describing similar strategies to address POW such as waiting longer before starting buprenorphine, using adjuncts such as kratom, or switching to alternatives like methadone.3,10 Further research should characterize the toxicokinetics of fentanyl in people with OUD, as this has important clinical implications for clinicians treating these patients in an algorithmic approach to buprenorphine induction.
There are several limitations to this study. Reddit users have been reported to be majority male, younger, and non-Hispanic white, compared to the general population of the United States, and may not reflect a representative sample of people with OUD.17 Additionally a temporal association between increased posts about fentanyl and POW could be related to various other factors such as temporal changes in how OUD is being treated or increasing usage of buprenorphine over other medications to treat OUD. Additionally, people who experience negative outcomes could be more likely to post about them on social media, exaggerating the risk of POW with standard induction regimens of buprenorphine. Another limitation to this study is that the geographic locations of posts were not available to evaluate if the locations of the people making these posts corresponded to areas of high fentanyl prevalence. Prior work has found that automated NLP methods can characterize aspects such as sentiment and geolocation on social media sites like Twitter, but they are less well described for Reddit.26
5. CONCLUSION
This study found that Reddit discussions about POW increased in a similar timeframe as Reddit posts about fentanyl. Posts related to POW discussed the experiences of people with OUD and several themes emerged that are of importance to clinicians who treat these patients. Many posts discussed strategies to avoid POW with buprenorphine inductions. Taking adjuncts such as kratom, benzodiazepines, or loperamide was a strategy mentioned to help prolong their period of abstinence before taking buprenorphine. A subset of posts described microdosing, or the Bernese method, as a strategy to avoid POW. While this strategy of buprenorphine induction is only described in a few case reports and has not become a mainstream medical practice, posts on Reddit suggest that people with OUD are experimenting and searching for these strategies to initiate buprenorphine without having to experience an abstinence period or risk POW. The challenges of initiating buprenorphine need to be evaluated in the context of the prevalence of fentanyl in the drug supply so that clinicians can optimize treatment initiation with buprenorphine.
Data Availability
Raw data can be downloaded (while it is public) directly from the Reddit API.
FUNDING
Research reported in this publication was supported by the National Institute on Drug Abuse (NIDA) of the National Institutes of Health (NIH) under award number R01DA046619. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
CONFLICT OF INTEREST
None declared.
Footnotes
(abeed@dbmi{at}emory.edu)
(whitney.hogg{at}emory.edu)
(jennifer.love{at}mountsinai.org)
(Nicole.O'Donnell{at}pennmedicine.upenn.edu)
(Lewis.Nelson{at}Rutgers.edu)
(Jeanmarie.Perrone{at}pennmedicine.upenn.edu)
REFERENCES



