
Abstract
The neuropeptide oxytocin (OXT) can modulate social cognition by facilitating attention towards social cues and may be a potential therapeutic intervention for social attention impairment in disorders such as autism. Intranasal administration of OXT is widely used to examine its functional effects in both adults and children. However, we have recently shown that administration orally as a lingual spray also modulates neural responses to emotional faces and is potentially better tolerated for therapeutic use. Here, we therefore examined if 24IU OXT administered orally is also effective in facilitating social attention. In a randomized, placebo-controlled, pharmacological study we used a validated emotional anti-saccade eye-tracking paradigm to explore effects of oral OXT on bottom-up and top-down attention processing in 80 healthy male subjects. Our findings showed in terms of top-down attention, oral OXT increased both errors and response latencies for all social stimuli (angry, fearful, happy, sad and neutral emotion faces) but not non-social stimuli (oval shape) in the anti-saccade condition. Comparison with our previous intranasal OXT study using the same task paradigm revealed both routes have a similar effect on increasing anti-saccade errors. However, compared with intranasal OXT, oral OXT significantly decreased error rates for social stimuli in the pro-saccade condition, indicative of increased bottom-up attention processing. Additionally, OXT administration both either route produced an anxiolytic effect evidenced by reduced state anxiety scores. Together, these findings suggest that orally administered OXT has a similar effect on top-down social attention control and anxiety as intranasal administration but more potently influences bottom-up control.
1. Introduction
The neuropeptide oxytocin (OXT) is an important modulator of social cognition in both animal models and humans (Kendrick, 2000, 2017; Quintana et al., 2021) and has been proposed as a therapeutic intervention in disorders with social dysfunction. In particular, treatment with exogenous OXT has been considered in autism spectrum disorder (ASD) with associations between altered OXT function and receptor genotypes reported in numerous studies (Feldman et al, 2014; LoParo & Waldman, 2015; Zhang et al., 2016). While several clinical trials with chronic intranasal OXT treatment have reported some improvements in social responsivity in children with ASD (Parker et al., 2017; Yatawara et al., 2016) the therapeutic effects are still relatively modest. There is also an ongoing debate in the field as to how OXT administered intranasally may be producing functional effects and whether the amount and frequency of doses or route of administration might influence outcomes.
The great majority of studies investigating the functional effects of acute or chronic OXT treatment in both clinical and preclinical contexts have used an intranasal administration route. This has been largely guided by studies reporting that the blood-brain barrier (BBB) is relatively impermeable to OXT and that when given intranasally OXT can directly enter into the brain via the olfactory and trigeminal nerves (Lee et al., 2020; Quintana et al., 2021; Yeomans et al., 2021). However, there is increasing support for the possibility that increased peripheral concentrations of OXT may additionally, or alternatively, produce functional effects by crossing the BBB after binding to RAGE (receptors for advanced glycation end products, Yamamoto & Higashida, 2020; Yamamoto et al., 2019) and/or via acting on peripheral receptors in the heart or gastrointestinal system to increase vagally-mediated stimulation of the brain (Carter, 2014; Zheng & Kendrick, 2021). Indeed, intranasally administered OXT could potentially also act via these two peripheral routes since it increases concentrations in the blood and can also enter the gastrointestinal system by being swallowed after some of the dose drips down into the mouth cavity. A number of animal model studies have indicated that similar functional effects of OXT can occur following direct administration into the brain or given intraperitoneally. In humans, two initial studies in ASD patients reported some positive effects of intravenously administered OXT (Hollander et al., 2003, 2007) although other subsequent studies have reported both negative (Quintana et al., 2016) and positive (Martins et al., 2020) effects of intravenous OXT on brain activity. Most recently we have investigated whether using an oral (lingual) route in humans can produce functional effects since this can both produce increased OXT concentrations in blood and gastrointestinal system but without any possibility of direct entry into the brain (De Groot et al., 1995; Kou et al., 2021). Importantly, from a potential therapeutic standpoint, especially in children, an oral route of chronic administration is likely to be much better tolerated than either nasal sprays or intravenous infusions. The initial results obtained have been encouraging, demonstrating that oral OXT enhanced responses in the brain reward system and amygdala to emotional faces compared to intranasal application. By contrast, no effects were found in the brain reward system and the amygdala showed a significant reduction in response to emotional faces after intranasal OXT treatment (Kou et al., 2021). Furthermore, effects of oral OXT on putamen responses to happy faces were positively associated with increased plasma concentrations of OXT. Oral administration of OXT has also been shown to produce neural and behavioral effects in rodents (Maejima et al., 2020; Tabbaa & Hammock, 2020). However, going forward, it is important to investigate whether orally administered OXT can also have beneficial functional effects on other aspects of social cognition.
Autism is characterized by marked deficits in social attention (Fletcher-Watson et al., 2009; Fujioka et al., 2020; Kou et al., 2019) and a number of studies have demonstrated that intranasal administered OXT treatment can improve attention to social cues in both healthy (Ellenbogen et al., 2012; Kendrick et al., 2017; Le et al., 2020, 2021; Xu et al., 2019; Yao et al., 2018) and clinical populations (Guastella et al., 2010; Huang et al., 2021; Yamasue et al., 2020). In the context of its possible therapeutic use it is therefore important to establish whether orally administered OXT can also enhance attention towards social cues.
Against this background, the present study aimed to explore the effect of oral OXT on social attention including both top-down and bottom-up attention control to social cues using a validated emotional anti-saccade task which we have employed to examine the effect of intranasal OXT in a previous study (Xu et al., 2019). The emotional anti-saccade task includes five emotional faces (sad, angry, fearful, happy, and neutral) as social stimuli and oval shapes as non-social stimuli. Participants are either instructed to look towards the stimuli (pro-saccade) or look away to the side opposite to them (anti-saccade) in this task. During the pro-saccade condition participants focus on the target automatically which involves “bottom-up” attention control while during the anti-saccade condition they need to inhibit reflexive orienting towards stimuli and therefore implement “top-down” attention control (Munoz & Everling, 2004). Results from our previous study found that intranasal OXT selectively reduced subjects’ ability to engage top-down attention control to look away from socially salient stimuli and therefore increased anti-saccade errors (Xu et al., 2019). We also found that intranasal OXT decreased post-task state anxiety in line with previous studies showing its anxiolytic effects (Kou et al., 2020; Neumann & Landgraf, 2012). Therefore, in the current study we used the same task to examine if oral OXT produces similar or different effects on social attention processing and state anxiety compared to intranasal OXT (Xu et al., 2019). Moreover, previous studies have demonstrated effects of state anxiety on attention control with respect to both anti-saccade and pro-saccade conditions (Cornwell et al., 2012; Myles et al., 2020), and so it was also important to investigate oral OXT’s effects from this standpoint.
In order to compare the effects of orally and intranasally administered OXT findings from the current 24IU oral dose study were further compared with those from our previous intranasal study where subjects received the same OXT dose (Xu et al., 2019; pre-registered randomized controlled trial under NCT03486925). This comparison between the routes of administration provided a way to help address the important question of whether the effects of OXT in increasing attention towards social stimuli necessitate its direct entry into the brain since it cannot do this via an oral administration route. Given increasing evidence for the involvement of peripheral changes in OXT concentrations following exogenous treatment we hypothesized that orally administered OXT would also produce effects on top-down attentional control when social stimuli were used. We additionally hypothesized that oral OXT would produce similar decreases in state anxiety.
2. Methods
2.1. Participants
80 healthy right-handed male subjects (age: Mean ± SEM = 22.65 ± 0.23) were recruited in the current study and provided written informed consent. The sample size was based on our previous intranasal arginine vasopressin study and achieves > 80% power (Zhuang et al., 2021). Only male subjects were included in this study to match our previous intranasal OXT study (Xu et al., 2019). All subjects were instructed to abstain from consuming alcohol and caffeine during the 24 hours before experiment. In the placebo-controlled between-subject design experiment, subjects were randomly assigned to receive 24 International Units (IU) of oxytocin (n = 40, age: Mean ± SEM = 22.43 ± 0.28) or placebo (n = 40, age: Mean ± SEM = 22.88 ± 0.36; details see Supplementary Material Figure S1 for consolidated standards of reporting trials (CONSORT) flow chart) via oral (lingual) spray. The current study was approved by the local ethics committee of University of Electronic Science and Technology of China (UESTC) and pre-registered at clinical trials.gov (ClinicalTrials.gov ID: NCT04493515) and all experimental procedures were in accordance with the latest version of the Declaration of Helsinki. All subjects voluntarily signed the written informed consent.
2.2. Experimental procedure
To control for potential confounders between different treatment groups subjects were asked to complete validated questionnaires in Chinese before drug treatment including Positive and Negative Affect Schedule (PANAS, Watson et al., 1988), State-Trait Anxiety Inventory (SAI-TAI, Spielberger, 1983) and other scales measuring depression, autism, childhood experience, cognition and emotion regulation (details see Supplementary Material). No significant differences were found between OXT and PLC groups in these questionnaire scores (all ps ≥ 0.08, see Supplementary Material Table S1). Next, subjects were randomly assigned to receive OXT (Sichuan Meike Pharmaceutical Co. Ltd) or PLC (identical spray with same ingredients but without OXT) administration orally 45 min before the anti-saccade task. They were instructed to self-administer alternately 3 puffs on the tongue and 3 puffs under the tongue (1 puff 0.1 ml, interspaced by 30s). After each spray subjects were required not to swallow until the next puff so that OXT could have more time to be absorbed by the lingual blood vessels. After the whole experiment subjects were asked to guess which treatment they had received and the accuracy of their answers was not significantly better than chance (χ2 = 0.98, p = 0.32). Additionally, to examine potential treatment and task effects on mood and state anxiety, subjects completed the PANAS and SAI before OXT or PLC treatment and after all experimental tasks.
2.3. Experimental paradigm
The present study used a validated emotional anti-saccade paradigm (Chen et al, 2014; Xu et al., 2019) including five social emotional faces (angry, fearful, happy, sad and neutral) from 4 female and 4 male actors and eight non-social slightly varying oval shapes. To avoid any possible carry-over effects of emotional stimuli, the non-emotional blocks (2 blocks: one anti- and one pro-saccade block) including 48 trials per block were always at the beginning of the task and then followed by the emotional blocks (12 blocks: 6 anti- and 6 pro-saccade blocks) including 40 trials per block. All blocks and trials in each block were presented randomly.
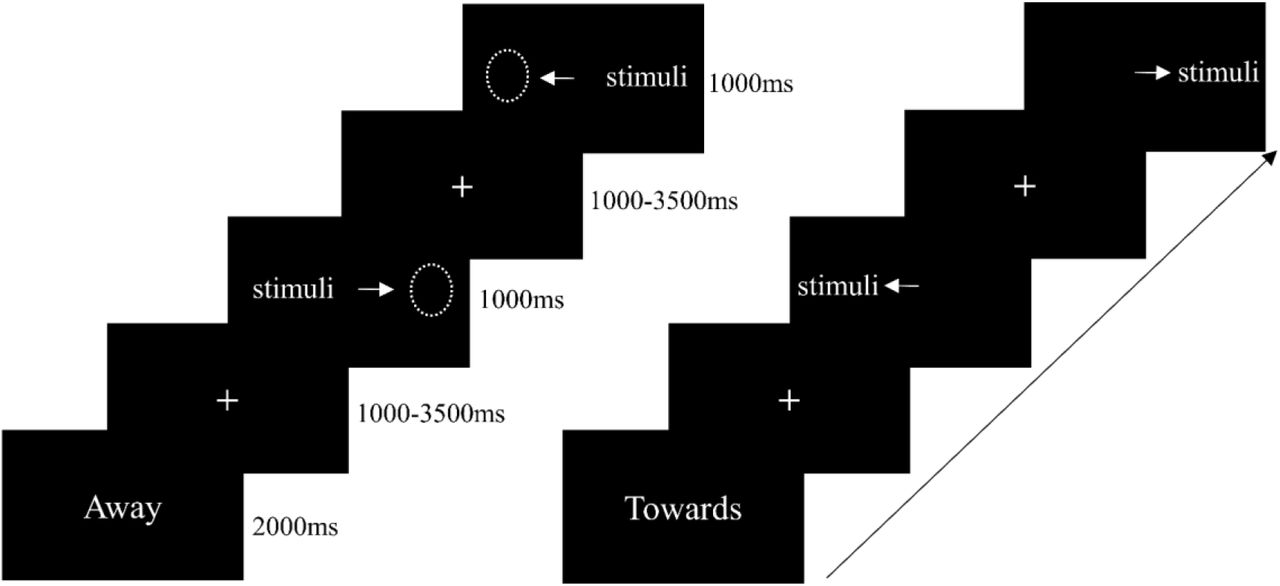
Each block began with a 2000 ms cue word “Towards” or “Away”. After the cue, a jittered fixation appeared in the center of the monitor with a mean duration of 1500 ms (time range:1000-3500 ms) and subjects were asked to fixate on it. Next, the stimulus was presented on the left or right side of screen for 1000 ms. Subjects were required to look towards the stimulus in the “Towards” blocks (pro-saccade condition) and look away from the the stimulus in the “Away” blocks (anti-saccade condition) as accurately and quickly as they could (Figure 1). The whole task took approximately 35 minutes with a short rest between blocks.
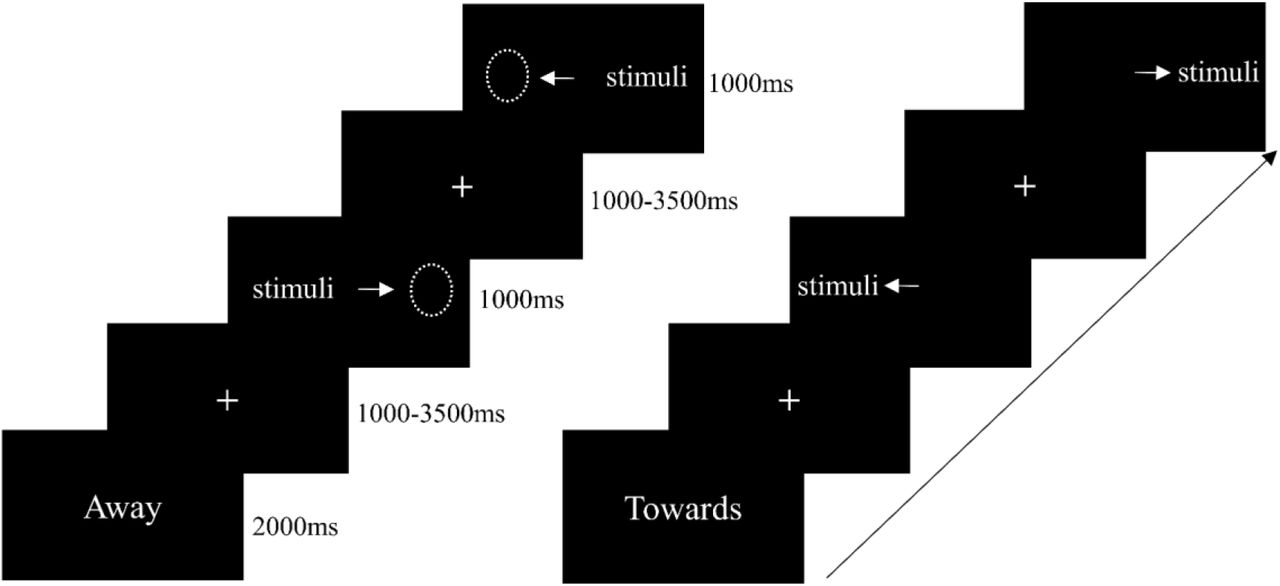
Timing set for anti-saccade condition (left) and pro-saccade condition (right) in the emotional anti-saccade task.
2.4 Eye movement recording and processing
Eye movement data were recorded in the monocular mode (right eye) using an EyeLink 1000 Plus system (SR Research, Ottawa, Canada, 2000 Hz sampling rate) with a screen resolution of 1024*768. To fix the standard position and distance from the screen, a chin rest was set 57 cm away from the monitor. At the beginning of each block a 9-point calibration was performed to ensure eye-tracking data quality.
The raw eye movement data was preprocessed and exported by the EyeLink DataViewer 3.1 (SR Research Mississauga, Ontario, Canada). In line with previous studies, trials with latencies less than 70 ms or more than 700 ms and saccade velocity lower than 30°/sec were discarded (García-Blanco et al, 2013; Xu et al., 2019). Data from 10 subjects were excluded from the final statistical analysis including 5 subjects who failed to complete the whole experiment due to technical errors, 3 subjects who failed to pass the calibration and 2 subjects whose more than 25% of trials were excluded (Reinholdt-Dunne et al., 2012). There was no significant difference in percentage of excluded trials for the remaining subjects between OXT (n = 35) and PLC groups (n = 35, PLC: Mean ± SEM = 7.96% ± 0.85, OXT: Mean ± SEM = 9.37% ± 0.83, t = 1.18, p = 0.24). Finally, the mean error rate and latency of correct saccade trials during both anti- and pro-saccade conditions were calculated and served as primary behavioral indexes. An error was defined as subjects making their first saccade in the opposite direction to the one they had been instructed to do.
2.5. Statistical analyses
To determine the social effects of oral OXT on attention control, treatment (OXT/PLC) * condition (social/non-social) * task (pro-/anti-saccade) mixed ANOVAs were conducted on both latency and error rate. To explore the emotion-specific effects of oral OXT on attention processing, we further conducted treatment (OXT/PLC) * task (pro-/anti-saccade) * stimuli (angry/sad/fearful/happy/neutral/shape) mixed ANOVAs on latency and error rate.
Next, to compare the effects of oral and intranasal OXT on attention control, treatment (intranasal OXT/oral OXT/PLC) * task (anti-/pro-saccade) * condition (social/non-social) mixed ANOVAs on latency and error rate were performed. Additionally, to determine the emotion-specific effects of OXT via different routes on attention processing, treatment (intranasal OXT/ oral OXT/PLC) * task (anti-/pro-saccade) * stimuli (angry/sad/fearful/happy/neutral/shape) mixed ANOVAs on latency and error rate were conducted. Furthermore, to control non-treatment related variables the two PLC groups from the current and our previous intranasal study were compared with respect to social- and emotion-specific effects on attention control (see Supplementary Material). The comparison study was pre-registered at clinical trials.gov (ClinicalTrials.gov ID: NCT04815395). Appropriate Bonferroni-corrected comparisons were employed to disentangle significant main and interaction effects.
3. Results
3.1. Effects of oral OXT on saccade error rates
The treatment (OXT/PLC) * condition (social/non-social) * task (pro-/anti-saccade) mixed ANOVA on error rate showed a significant main effect of treatment (F1, 68 = 6.38, p = 0.014, ηp2 = 0.09), reflected by higher overall error rates after OXT compared to PLC treatment (PLC: Mean ± SEM = 5.52% ± 0.90, OXT: Mean ± SEM = 8.72% ± 0.90, Cohen’s d = 0.63, see Figure 2A and 2B). In addition, a significant interaction effect between treatment and task was observed (F1, 68 = 8.12, p = 0.006, ηp2 = 0.11) with post-hoc Bonferroni-corrected comparisons showing that compared to PLC treatment, OXT increased error rates in the anti-saccade but not pro-saccade condition (anti: PLC: Mean ± SEM = 9.45% ± 1.56, OXT: Mean ± SEM = 15.48% ± 1.56, p = 0.008, Cohen’s d = 0.65; pro: PLC: Mean ± SEM = 1.59% ± 0.41, OXT: Mean ± SEM = 1.95% ± 0.41, p = 0.53). We also found a significant main effect of condition (F1, 68 = 17.54, p < 0.001, ηp2 = 0.21) and task (F1, 68 =115.45, p < 0.001, ηp2 = 0.63), reflected by higher error rates for social compared to non-social stimuli (social: Mean ± SEM = 8.24% ± 0.68, non-social: Mean ± SEM = 6.00% ± 0.70), and higher error rates during anti-saccade compared to pro-saccade condition (anti: Mean ± SEM = 12.47% ± 1.10, pro: Mean ± SEM = 1.77% ± 0.29). Additionally, a significant interaction between condition and task was observed (F1, 68 = 13.01, p < 0.001, ηp2 = 0.16). Post-hoc Bonferroni-corrected comparisons found increased error rates for social compared to non-social stimuli during anti-saccade rather than pro-saccade condition (anti: social: Mean ± SEM = 14.77% ± 1.27, non-social: Mean ± SEM = 10.16% ± 1.21, p < 0.001; pro: social: Mean ± SEM = 1.71% ± 0.23, non-social: Mean ± SEM = 1.84% ± 0.43, p = 0.73). This is in line with our previous findings (Xu et al., 2019) and suggests social stimuli and task modulate error rates. However, no other treatment related interaction effects were observed (all ps ≥ 0.34).

Oral OXT’s effect on error rates and latencies. (A) Oral OXT increased error rates for both social and non-social stimuli in the anti-saccade condition, however (B) A treatment * condition interaction showed that error rates for social emotional faces were significantly higher than shapes in the anti-saccade condition (effect sizes: angry: Cohen’s d = 0.62, sad: d = 0.52, fearful: d = 0.72, happy: d = 0.64, neutral: d = 0.54). (C) Saccade latency for social and non-social stimuli in pro- and anti-saccade condition after oral OXT and PLC treatment. (D) A treatment * condition interaction showed that latencies for social emotional faces were significantly increased for faces but not shapes in the anti-saccade condition (angry: Cohen’s d = 0.64, sad: d = 0.60, fearful: d = 0.62, happy: d = 0.53, neutral: d = 0.67). Latencies for social emotional faces were significantly faster than for shapes in the pro-saccade condition. *, ** and *** denote significant post-hoc treatment effects at pBonferroni < 0.05, pBonferroni < 0.01 and pBonferroni < 0.001 respectively.
The treatment (OXT/PLC) * task (pro-/anti-saccade) * stimuli (angry/sad/fearful/ happy/neutral/shape) mixed ANOVA on error rate did not find a significant interaction treatment * task * stimuli interaction (F5, 340 = 0.80, p = 0.51) indicating that there were no significant emotion specific effects of OXT.
3.2. Effects of oral OXT on saccade response latency
To examine the effect of oral OXT on saccade response latency, the treatment (OXT/PLC) * condition (social/non-social) * task (pro-/anti-saccade) mixed ANOVA was conducted. Results showed a significant three-way interaction between treatment, condition and task (F1, 68 = 6.19, p = 0.015, ηp2 = 0.08). Post-hoc Bonferroni-corrected tests revealed that compared to PLC treatment, oral OXT increased latencies for social but not non-social stimuli during the anti-saccade condition (social, PLC: Mean ± SEM = 263.84 ± 4.18 ms, OXT: Mean ± SEM = 279.87 ± 4.18 ms, p = 0.009, Cohen’s d = 0.65; non-social, PLC: Mean ± SEM = 267.56 ± 4.45 ms, OXT: Mean ± SEM = 278.15 ± 4.45 ms, p = 0.10, Figure 2C). Effect sizes for individual stimuli were: angry: Cohen’s d = 0.64, sad: d = 0.60, fearful: d = 0.62, happy: d = 0.53, neutral: d = 0.67 but not for shapes p = 0.10 (Figure 2D). In line with our previous intranasal study (Xu et al., 2019), we found a significant main effect of condition (F1, 68 = 124.21, p < 0.001, ηp2 = 0.65) and task (F1, 68 = 979.00, p < 0.001, ηp2 = 0.94), with faster latencies for social compared to non-social stimuli (social: Mean ± SEM = 223.72 ± 2.20 ms, non-social: Mean ± SEM = 238.22 ± 2.51 ms) and increased anti-saccade latencies compared to pro-saccade (anti: Mean ± SEM = 272.36 ± 2.92 ms, pro: Mean ± SEM = 189.58 ± 2.29 ms). Additionally, a significant interaction between condition and task was observed (F1, 68 = 128.08, p < 0.001, ηp2 = 0.65), with post-hoc Bonferroni-corrected comparisons showing faster latencies for social compared to non-social stimuli during pro-saccade (social: Mean ± SEM = 175.58 ± 2.20 ms, non-social: Mean ± SEM = 203.58 ± 2.68 ms, p < 0.001) but not anti-saccade condition (social: Mean ± SEM = 271.86 ± 2.96 ms, non-social: Mean ± SEM = 272.86 ± 3.15 ms, p = 0.58).
The treatment (OXT/PLC) * task (pro-/anti-saccade) * stimuli (angry/sad/fearful/happy/neutral/shape) mixed ANOVA was conducted to explore emotion-specific effect of OXT on response latency. While there was a significant three-way interaction effect between treatment, task and stimuli (F5, 340 = 2.50, p = 0.047, ηp2 = 0.04), a post-hoc Bonferroni-corrected comparison did not reveal any differences between specific face emotions.
3.3. Effects of oral OXT on state anxiety
Paired t-tests were conducted on pre- and post-task SAI scores to examine treatment effect on state anxiety measured by SAI. Results showed that SAI scores were significantly decreased in the oral OXT group (pre: Mean ± SEM = 40.00 ± 2.00, post: Mean ± SEM = 36.46 ± 1.73, p = 0.027, Cohen’s d = 0.32) but not PLC group (pre: Mean ± SEM = 40.51 ± 1.53, post: Mean ± SEM = 39.63 ± 1.50, p = 0.38).
Additionally, to examine oral OXT’s effect on the association between state anxiety (pre- and post-task SAI) and attention control (pro- and anti-saccade error rates), Pearson correlations with multiple comparison correction were conducted. However, no significant correlations were observed either in the oral OXT (all ps ≥ 0.079; pre-SAI, pro: r = -0.15, p = 0.399, anti: r = -0.06, p = 0.715; post-SAI: pro: r = -0.18, p = 0.307, anti: r = -0.30, p = 0.079) or in the PLC groups (all ps ≥ 0.333; pre-SAI, pro: r = -0.05, p = 0.785, anti: r = -0.01, p = 0.958; post-SAI: pro: r = -0.17, p = 0.333, anti: r = -0.06, p = 0.719).
3.4. Comparisons between the effects of intranasal and oral OXT on attention control
For error rate, the treatment (intranasal OXT/oral OXT/PLC) * task (pro-/anti-saccade) * condition (social/non-social) mixed ANOVA found a marginally significant interaction between treatment, task and condition (F2, 100 = 2.79, p = 0.066, ηp2 = 0.05). Direct comparison between intranasal and oral OXT using exploratory post-hoc Bonferroni-corrected tests showed that compared to intranasal OXT, oral OXT decreased error rates for social stimuli during the pro-saccade (oral: Mean ± SEM = 1.75% ± 0.45; intranasal: Mean ± SEM = 3.61% ± 0.47, p = 0.016, Cohen’s d = 0.63, Figure 3A) but not anti-saccade condition (oral: Mean ± SEM = 18.28% ± 1.90; intranasal: Mean ± SEM = 21.43% ± 1.96, p = 0.75).

{kind=link}
{kind=link}
{kind=link}
(A) The comparison between intranasal and oral OXT’s effect on social attention processing, with higher error rates for social stimuli during pro-saccade condition after intranasal OXT compared to oral OXT treatment. (B) Pro-saccade error rates for emotional faces and oval shapes in intranasal and oral OXT group, with reduced error rates for sad and neutral faces after oral OXT compared to intranasal OXT. * denotes significant post-hoc difference at pBonferroni < 0.05.
Furthermore, the treatment (intranasal OXT/oral OXT/PLC) * task (pro-/anti-saccade) * stimuli (angry/sad/fearful/happy/neutral/shape) mixed ANOVA on error rate was performed to explore the emotion-specific effect of OXT via different routes. Results found a significant three-way interaction between stimuli, task and treatment (F10, 500 = 2.02, p = 0.05, ηp2 = 0.04), with decreased error rates for sad and neutral faces after oral OXT compared to intranasal OXT during the pro-saccade condition in the further post-hoc Bonferroni-corrected comparisons (pro: sad: oral: Mean ± SEM = 1.75% ± 0.67; intranasal: Mean ± SEM = 4.48% ± 0.69, p = 0.017, Cohen’s d = 0.59; neutral: oral: Mean ± SEM = 1.83% ± 0.47; intranasal: Mean ± SEM = 3.74% ± 0.48, p = 0.016, Cohen’s d = 0.69, Figure 3B; anti: all ps > 0.08). However, mixed ANOVAs on response latency showed no significant differences between the effects of intranasal and oral OXT on social (all ps > 0.99) or non-social (all ps > 0.94) attention processing.
To further examine the non-significant hypothesis that oral and intranasal OXT have similar effects on top-down attentional control, Bayesian analysis was conducted using JASP (version 0.14.1.0, https://jasp-stats.org). A Bayesian independent-sample t test was performed on the anti-saccade error rates in the oral and intranasal OXT groups. A Bayes factor (BF01 = 3.62) was observed, suggesting that the null hypothesis for the differences between oral and intranasal OXT was moderately fitted relative to alternative model (Jeffreys, 1998). A similar Bayesian analysis on saccade latencies only revealed an anecdotal fit however (BF01 = 2.78).
3.5. Comparison between the effects of oral and intranasal OXT on state anxiety
To compare the effects of intranasal and oral OXT on state anxiety, the group (intranasal OXT/oral OXT/PLC) * SAI (pre-/post-test) mixed ANOVA was conducted on SAI scores. However, neither the interaction effect (F2, 100 = 1.19, p = 0.31) nor the main effect of group was significant (F2, 100 = 2.00, p = 0.14). The further exploratory post-hoc with Bonferroni correction showed that post-task SAI scores were significantly decreased following both oral and intranasal OXT (oral: p = 0.009, intranasal: p = 0.02) but not PLC (p = 0.51).
To further explore whether oral and intranasal OXT have similar anxiolytic effects, the non-significant hypothesis was examined using a Bayesian independent-sample t test on the changes of SAI scores (post-minus pre-task SAI scores) via the oral and intranasal route. Results showed a Bayes factor (BF01 = 3.97), indicating that the non-significant differences between oral and intranasal OXT group were moderately fitted in the present data (Jeffreys, 1998).
4. Discussion
Overall the current pharmacological study using an emotional anti-saccade eye tracking paradigm revealed that orally administered OXT increased error rates and response latencies for the anti-saccade condition across all emotional expressions (angry, sad, fearful, happy and neutral faces) was similar to findings we have previously reported for intranasally administered OXT (Xu et al., 2019). This demonstrates that OXT administered via both routes biases top-down attention processing towards social stimuli. Oral OXT also reduced state anxiety scores in a similar manner to intranasal OXT suggesting a similar anxiolytic effect produced via both routes. However, an additional comparison for the effects of OXT on pro-saccade error rates for social stimuli, indicative of bottom up attentional processing, revealed a significantly greater effect of oral compared to intranasal administration.
Our findings showing faster pro-saccade latencies and increased anti-saccade error rates for social compared to non-social stimuli is in line with previous findings reporting social valence modulated attentional processing and also validates the anti-saccade paradigm we used (Salvia et al, 2020; Xu et al., 2019). However, although previous studies showed effects of state anxiety on both bottom-up and top-down attention control (Cornwell et al., 2012; Myles et al., 2020), we did not found significant associations between state anxiety and attention control in the current paradigm. This may be due to the fact that subjects in previous studies had high trait anxiety and a non-social/non-emotional anti-saccade task was employed.
The main finding in the present study demonstrates that orally administered OXT produced similar effects to intranasal OXT on top-down social attention in terms of both increased anti-saccade errors and longer saccade response times during presentation of social stimuli. In terms of increased anti-saccade errors there was however also a main treatment effect indicating that oral OXT influenced top-down attention processing during presentation of both social and non-social stimuli although the effect was significantly stronger for social stimuli. Both routes of administration also significantly reduced state anxiety in this paradigm and Bayes factors >3 were found for analyses of anti-saccade errors and state anxiety, indicating moderate evidence for the null model of the non-significant difference between orally and intranasally administered OXT’s effect on top-down both social attention processing and anxiety relative to the alternative model (Jeffreys, 1998). Importantly, a previous study has demonstrated that orally administered OXT can enhance neural responses to emotional faces in the putamen in the reward system which are associated with increased concentrations of the peptide in blood (Kou et al., 2021). Other studies have also reported that the effects of OXT on putamen activation is strongly associated with social salience processing (Hu et al., 2015; Zhao et al., 2019). Overall these findings support the potential for an oral OXT administration route to be considered for therapeutic use in ASD or other disorders with social dysfunction.
In contrast to the similarity between the effects of oral and intranasal OXT on top-down attentional processing we found evidence for a significantly greater effect of oral OXT in reducing pro-saccade errors, indicating a stronger influence on bottom-up processing compared to intranasal administration. Automatic, bottom-up mediated, attention may particularly involve amygdala projections to the salience network and frontal executive processing regions (Comte et al., 2016) and in this respect it is interesting to note that while intranasal OXT administration strengthens effective connectivity from frontal and salience networks to the amygdala (i.e. top-down control) it has no effect on the strength of functional connections from the amygdala (Jiang et al., 2021). Following intranasal OXT in male subjects amygdala responses to emotional faces are also reduced whereas following oral administration they are increased (Kou et al., 2021). Thus, intriguingly, the route of OXT administration may have differential effects on bottom-up but not top-down social attention processing via different modulatory effects on amygdala responses and functional connectivity.
In terms of the ongoing debate concerning how intranasally administered OXT may act to modulate neural and behavioral functions, our findings provide further support for the importance of increased OXT concentrations in the peripheral vascular system and/or gastrointestinal system producing neural changes either via RAGE-mediated transport across the BBB or via vagal stimulation. While this does not rule out additional contributions of direct entry of OXT into the brain via the olfactory and trigeminal nerves following intranasal administration, it provides increased support for this not being the only route. Interestingly however, the current findings together with those of our previous study (Kou et al., 2021) and from another group (Martins et al., 2020) raise the possibility that there may be important administration route-dependent functional effects which need further exploration and may ultimately influence therapeutic intervention strategy. Plasma concentration changes following 24IU oral administration of OXT are significantly smaller than those found after intranasal administration (Kou et al., 2021) raising the possibility that route-dependent functional effects may be influenced by the dose. Thus, at this stage it is possible that there may be interactions between OXT dose (both concentration and frequency) and route of administration which determine functional effects.
The effects of oral administration of OXT on both top-down and bottom up attention processing are similar to those we have previously reported after intranasal administration of vasopressin (Zhuang et al., 2021). This suggests that both peptides have facilitatory effects on social attention and that both may act to enhance the salience of social stimuli as has been proposed for OXT (Shamay-Tsoory & Abu-Akel, 2016). Findings, may also help to explain why both peptides have been shown to improve social responsivity in children with autism (Parker et al., 2017, 2019; Yatawara et al., 2016). There is the possibility of cross-talk between receptors since both peptides can stimulate each other’s receptors to some extent (Neumann & Landgraf, 2012). However, with at least a 10-fold reduction in affinity for the other peptide’s receptors it seems more likely that both produce enhanced social attention via acting on their own receptors.
There are several limitations which should be acknowledged in the current study. First, only male subjects were included in the present study to be in line with the intranasal OXT study (Xu et al., 2019). Some previous studies in rodents have reported sex-specific behavioral and neural effects of peripherally administered OXT (Dumais et al, 2017; Tabbaa & Hammock, 2020) and some studies in humans with intranasal OXT administration have also reported sex-dependent effects (Gao et al., 2016; Luo et al., 2017), although not for social attention paradigms. However, future studies will be needed to explore oral OXT’s effect on attention control in both male and female subjects. Second, in line with previous studies, oval shapes served as non-social stimuli but are less complex than emotional faces. Future studies could consider using objects or natural scenes as non-social control stimuli to match the complexity of faces. Third, given that the PANAS and SAI questionnaires were only measured prior to oral treatment and post-task, it cannot be determined whether the observed anxiolytic effect in oral OXT group was due to OXT treatment per se or a combination of treatment and task.
In summary, the current study using a validated emotional anti-saccade paradigm which can measure treatment effects on both top-down and bottom-up attentional processing revealed that oral OXT selectively modulated social but not non-social stimuli. Comparison of the effects of oral OXT with those we have previously reported for intranasal OXT revealed that while both had similar effects on top-down attention and state anxiety, orally administered OXT additionally modulated bottom-up attention. Overall, these findings suggest that some key functional effects of exogenous OXT administration involve an influence on the brain via the peptide being transported from the blood across the BBB and/or via vagally mediated effects. The findings also suggest that OXT administered via an oral route may be useful in a therapeutic context, particularly for children where intranasal administration may be less well tolerated.
Data Availability
The data in the manuscript could be accessible from authors on the request
Declaration of conflicting interests
The authors declared no conflicts of interest with their research, authorship or the publication of this article.
Author contributions
Qian Zhuang: Formal analysis; Investigation; Writing-original draft. Xiaoxiao Zheng: Formal analysis; Investigation. Shuxia Yao: Conceptualization. Weihua Zhao: Project administration. Benjamin Becker: Supervision; Validation. Xiaolei Xu: Formal analysis; Supervision; Validation. Keith M. Kendrick: Conceptualization; Funding acquisition; Project administration; Resources; Supervision; Validation; Writing review & editing.
Acknowledgements
This work was supported by the National Natural Science Foundation of China (grant numbers 31530032 – KMK and 91632117 - BB), Key Technological Projects of Guangdong Province (grant number 2018B030335001 – KMK).
Footnotes
No. 2006, Xiyuan Ave., West Hi-Tech Zone, Chengdu, Sichuan 611731, China. Phone: +86-28-61830811; Fax: +86-28-61830811
References



