
ABSTRACT
Background There are no standardized reporting systems or assessments specific to residents of retirement homes in North America. As such, little is known about these older adults as a distinct population. We created a new population-level cohort of residents of retirement homes and examined their health service rates relative to other older adult populations.
Methods We conducted a population-based retrospective cohort study in Ontario, Canada in 2018. The postal codes of all licensed retirement homes (n = 757) were classified and linked to individual-level health system administrative data to derive a cohort of residents of retirement homes. A generalized linear model with a gamma distribution and log link function was used to model rates of emergency department visits, hospitalizations, alternate levels of care (ALC) days, primary care visits, and specialist physician visits.
Results Residents of retirement homes comprised two percent of the older adult population in Ontario (n = 54,773; 2.3%). After adjustment for relevant characteristics, residents of retirement homes had 10 times the rate of emergency department visits (Relative Rate [RR] 10.02, 95% Confidence Interval [CI] 9.83 to 10.21), 20 times the rate of hospitalizations (RR 20.43, 95% CI 20.08 to 20.78), and 44 times the rate ALC days (RR 43.91, 95% CI 43.28 to 44.54) compared to community-dwelling older adults.
Interpretation Residents of retirement homes are a distinct older adult population with high rates of hospital-based care. Our findings contribute to policy debates about the provision of health care in privately operated congregate care settings for older adults.
INTRODUCTION
Retirement homes are private, congregate living environments that deliver supportive care to adults who are 65 years of age and older (1,2). Retirement homes are often marketed to provide a lifestyle and community, and these homes provide a range of assisted living care services (e.g., meals, administration of medication, nursing services, etc.) on a cost recovery basis (2). These homes predominately operate on a private, for-profit business model, and the room, board, and services are purchased by residents and/or their family or friend caregivers (1,2).
Retirement homes are referred to as assisted living facilities in other North American jurisdictions. The legislative and regulatory operating requirements for these homes vary (3); Ontario is the only jurisdiction to regulate and license retirement homes through an independent, not-for-profit regulator (i.e., Retirement Homes Regulatory Authority [RHRA]) (2). There are more than 700 licensed retirement homes in Ontario that can house over 70,000 older adults, which is comparable to the number of beds in the long-term care home sector (1,2,4). Unlike long-term care homes where the validated Resident Assessment Instrument Minimum Data Set (RAI-MDS) is used, there are no standardized assessments specific to residents of retirement homes (5). The absence of standardized assessments that are periodically conducted on residents of retirement homes, coupled with the privately financed nature of the sector, presents unique challenges to identify these older adults using health system administrative data and understand their health service use relative to other older adult populations.
While there is a body of research describing the assisted living sector and residents of assisted living facilities in the United States (6–12), the Canadian literature requires a more in-depth investigation. Canadian studies have investigated transitions to a long-term care home, risk of hospitalization among those who live with dementia, and events and health conditions associated with the transition to a congregate care setting for older adults (13–17). To date, no population- or provincial-level cohort of residents of retirement homes in Canada has been created to define the retirement home and assisted living sector, describe the characteristics and health service use of older adults who purchase these services, and position the sector in the gradient of care services and housing needs for older adults. In this study, we create a new population-level cohort of residents of retirement homes and examine their health service rates relative to other older adult populations (i.e., residents of long-term care homes, home care recipients in the community, and community-dwelling older adults) in Ontario, Canada.
METHODS
Study Design and Setting
We conducted a population-based retrospective cohort study using linked, individual-level health system administrative data in 2018 in Ontario, Canada at ICES. ICES is an independent, non-profit research institute whose legal status under Ontario’s health information privacy law allows it to collect and analyze health care and demographic data, without consent, for health system evaluation and improvement. The use of the data in this project is authorized under section 45 of Ontario’s Personal Health Information Protection Act (PHIPA) and does not require review by a Research Ethics Board. We followed the REporting of studies Conducted using Observational Routinely-collected health Data (RECORD) statement guideline (Supplemental Table 1) (18).
Data
The RHRA shared their public register of licensed retirement homes, which contains historical data on the license of the home, resident and suite capacities, provision of regulated care services, and full postal address. There were 757 licensed retirement homes in 2018 (Supplemental Table 2). We verified and visualized the postal code of each licensed retirement home through a variety of sources (i.e., Canada Post, Statistics Canada, and Google Maps). Building off research that examined the feasibility of using postal codes to identify residents of retirement homes (19), we used a modified taxonomy to classify the postal code of each licensed retirement home as unique, or not unique, to the retirement home. We imported the RHRA’s public register and our classified postal code data on licensed retirement homes to ICES. The health system administrative datasets used are listed and described in Supplemental Table 3. These datasets were linked using unique encoded identifiers and analyzed at ICES.
Identification of Residents of Retirement Homes
We identified adults who were 65 years of age of and older and had a postal code that ever matched to a licensed retirement home with a unique postal code classification in 2018 (Figure 1). There were substantially more adults who were 65 years of age and older and had a postal code that matched to a licensed retirement home with a not unique postal code classification than beds in licensed retirement homes. We limited our identification of residents of retirement homes with not unique postal codes to those who received home care services in a retirement home, as the receipt of home care services specified whether the services were provided in a retirement home. We defined the index date as when the adults’ postal code matched to the postal code of a licensed retirement home; we terminated follow-up when the adult transitioned to a long-term care home, complex continuing care facility, or died.

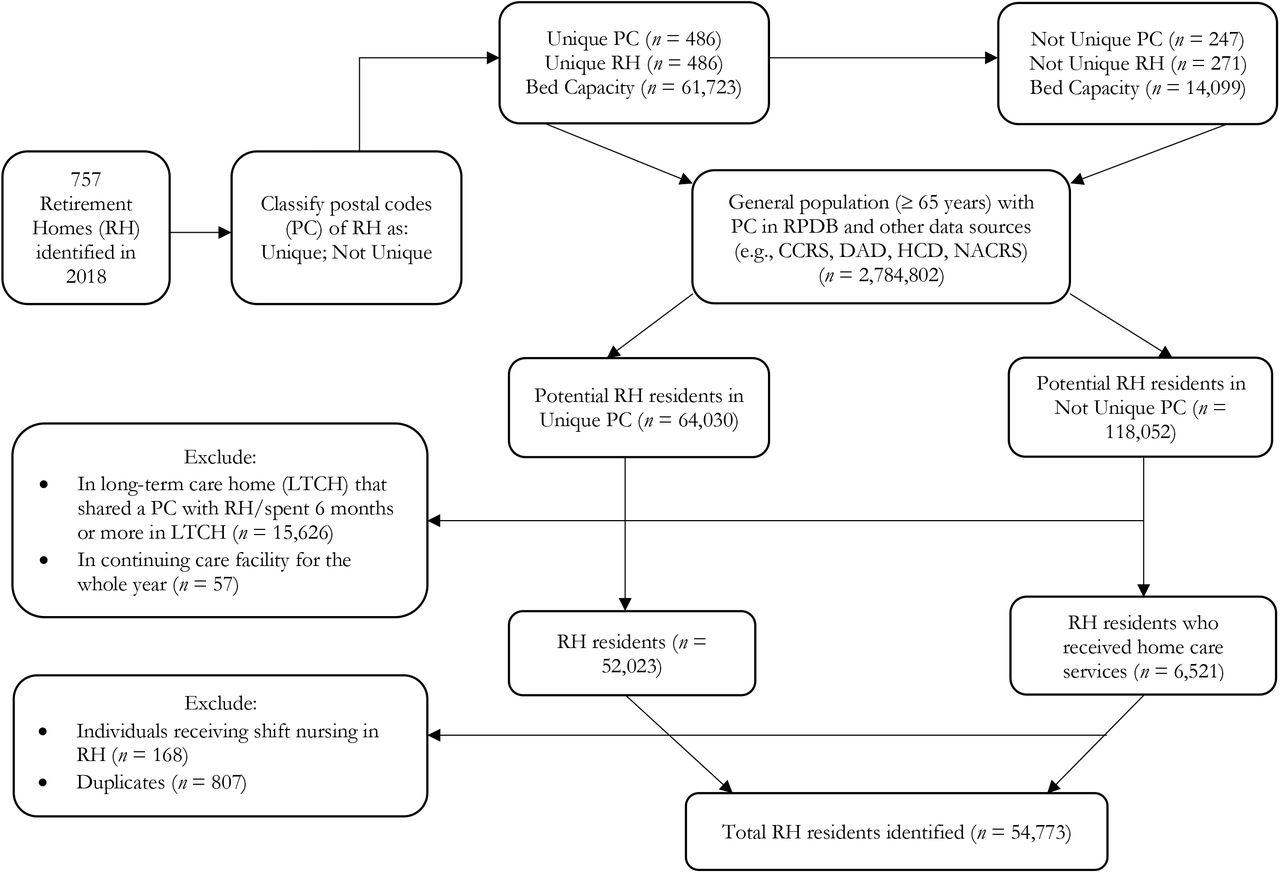{kind=link}
We excluded adults who were institutionalized in a long-term care home that was co-located with a retirement home and adults who resided in a long-term care home for more than half of 2018 (i.e., six months plus one day) (n = 15,626). Adults who resided in a continuing care facility for the whole year in 2018 were excluded (n = 57). We also excluded adults who received shift nursing in retirement homes (n = 168), as these individuals were temporarily housed in the retirement home through convalescent government programs, and so these individuals were not true residents of retirement homes. We excluded duplicate adults who moved from one retirement home to another during the year (n = 807). According to the RHRA’s register, there were 75,822 beds in all licensed retirement homes in 2018, and our approach identified a cohort of 54,733 residents of retirement homes (n = 54,733; 72.2%).
Identification of Other Older Adult Populations
For comparison purposes, we identified residents of long-term care homes, older adults who received home care services in the community, and community-dwelling adults who were 65 years of age and older in 2018. Residents of long-term care homes were identified by their inclusion in the Continuing Care Reporting System (n = 96,528). Adults who received home care services in their community were differentiated from residents of retirement homes by their postal code that never matched to a postal code associated with a licensed retirement home (n = 290,245). Community-dwelling adults were defined as those who were 65 years of age and older and never met any of the above criteria (n = 1,967,612). We defined the index date as when the adult met the criteria to be categorized as one of the mutually exclusive older adult populations in 2018; we terminated follow-up when the adult met the criteria to be categorized as a different older adult population or died.
Measures
The outcomes of interest were annual rates of emergency department visits, hospitalizations, alternate levels of care (ALC) days, primary care visits, and specialist physician visits. These rates were standardized at the level of the individual (i.e., from index to end of follow-up). Emergency department visits were defined as any care received in an emergency department. Hospitalizations were defined as any hospitalization. ALC days were obtained from the Discharge Abstract Database.
Primary care visits among residents of retirement homes, home care recipients in the community, and community-dwelling older adults were defined as any billing by a family or community medicine physician to the universal health insurance plan where the location of the visit occurred in an office, home, or via the telephone. Primary care visits among residents of long-term care homes were similarly defined in accordance with the Monthly Management System and included a long-term care home as the visit location. Specialist physician visits were defined as any physician billing whose speciality was not family or community medicine to the universal health insurance plan. All individuals could only have one primary care and/or specialist physician visit per physician per day.
Sociodemographic (i.e., age and sex) and community characteristics (i.e., urban location, neighborhood income quintile, Ontario Marginalization Index) were obtained at the index date. Clinical comorbidities were also obtained at the index date from physician-diagnosed billing codes to the universal health insurance plan in Ontario, ICD-9 or ICD-10 diagnosis codes, and validated ICES-derived cohorts (20–27).
Statistical Analysis
Counts and proportions were calculated for categorical sociodemographic, community, and clinical variables; means and standard deviations were calculated for continuous, normally distributed sociodemographic variables, and medians and interquartile ranges were calculated for continuous, not normally distributed sociodemographic variables. A generalized linear model with a gamma distribution and log link function was used to model the standardized health service rates among the different older adult populations, and community-dwelling older adults were used as the reference population. The gamma distribution and log link function is appropriate to model dispersed rates and/or costs in dollars (28). Crude and adjusted relative rates and 95% confidence intervals were calculated from exponentiated beta coefficients. All statistical tests were two-tailed, and the level of statistical significance was P < .05. Variance inflation factors were calculated to assess for multicollinearity. A sex-stratified subgroup analysis was conducted. Dataset processing and statistical analyses were conducted in SAS Enterprise 9.4 (Cary, NC, USA).
RESULTS
Residents of retirement homes comprised two percent of adults aged 65 and older in Ontario in 2018 (n = 54,773; 2.3%). More than two thirds of residents of retirement homes were female (n = 37,768; 69.0%), and residents of retirement homes had a mean age of 87.7 years (Table 1). Hypertension (n = 47,212; 86.2%), osteoarthritis (n = 36,978; 67.5%), mood disorders (n = 35,000; 63.9%) and dementia (n = 20,651; 37.7%) were the most prevalent clinical comorbidities among residents of retirement homes. More than 90% of all residents of retirement homes resided in urban communities (n = 50,650; 92.5%).
Sociodemographic Characteristics and Clinical Comorbidities Among Residents of Retirement Homes, Residents of Long-Term Care Homes, Home Care Recipients in the Community, and Community-Dwelling Older Adults in 2018 (n = 2,419,158)
The crude and sex-stratified health service rates are described in Supplemental Table 4. After adjustment for sociodemographic characteristics and clinical comorbidities at index, residents of retirement homes had 10 times the rate of emergency department visits (Relative Rate [RR] 10.02, 95% Confidence Interval [CI], 9.83 to 10.21), 20 times the rate of hospitalizations (RR 20.43, 95% CI 20.08 to 20.78), 44 times the rate of ALC days (RR 43.91, 95% CI 43.28 to 44.54), and nearly twice the rate of primary care (RR 1.99, 95% CI 1.97 to 2.02) and specialist physician visits (RR 1.62, 95% CI 1.59 to 1.65), compared to community-dwelling older adults (Table 2). Male residents of retirement homes had higher rates of emergency department visits, hospitalizations, and ALC days than female residents of retirement homes, but similar rates of primary care and specialist physician visits (Table 3). Adjusted beta coefficients and standard errors are available in Supplementary Tables 5 and 6.
Annual, Standardized Health Service Rates Among Residents of Retirement Homes, Residents of Long-Term Care Homes, and Home Care Recipients in the Community in 2018
Sex-Stratified Subgroup Analysis of Annual, Standardized Health Service Rates Among Residents of Retirement Homes, Residents of Long-Term Care Homes, and Home Care Recipients in the Community in 2018
INTERPRETATION
Residents of retirement homes had the highest rates of emergency department visits, hospitalizations, and ALC days relative to the other older adult populations in Ontario, Canada in 2018. These older adults purchase health care services from their retirement home to support independent living, yet we found they consume more publicly funded hospital-based care and have lower rates of primary care and specialist physician visits. Our findings contribute to on-going policy debates about privately financed and delivered health care, and the provision of health care in privately operated congregate care settings for older adults, in jurisdictions that provide universal health insurance to its citizens (29,30).
The variation in legislative and operating requirements for retirement homes has been shown to affect rates of hospital-based use among these residents (31,32). Previous studies found residents of retirement homes have substantially higher rates of emergency department visits and hospitalizations compared to community-dwelling older adults and residents of long-term care homes (11,33). Our findings align with the literature and may suggest residents of retirement homes have higher needs for care compared to other older adult populations.
Residents of retirement homes had the highest rates of ALC days relative to the other older adult populations in our study, which suggests the needs of some residents may exceed the capacity of their home to provide the level and scope of care needed. Moreover, some of these residents may not be able to afford additional care from their retirement home, as rates for heavy care in Ontario can exceed $6,000 per month (34). Nearly half of the residents of retirement homes lived in middle- and low-income neighborhoods. The costs for heavy care are likely out of reach for many of these older adults (35–37), which underscores the need for equitable policies that support health and housing for older adults.
Residents of retirement homes had lower rates of primary care and specialist physician visits relative to home care recipients who lived in the community. Residents of long-term care homes receive primary care through the Monthly Management System, but no similar model exists for retirement homes. Our findings suggest the implementation and expansion of similar medical models of care in retirement homes may be an important intervention to promote continuity of care and reduce rates of hospital-based care among this population.
Retirement home and assisted living markets in North America are rapidly expanding to accommodate the varying preferences of older adults for housing, health, and social care (2,5– 7,35,38). The growth and availability of beds in retirement homes and assisted living facilities outpaces that of long-term care homes (2,38), and this growth is likely attributed to fewer legislative and regulatory requirements than long-term care homes. The increased supply of retirement homes may suggest that retirement homes are a substitute for a long-term care home (7,38), which suggests that retirement homes are an important link in the continuum of care settings for older adults and should be subject to similar regulatory oversight.
There are limitations to our study. We conducted a secondary analysis of health system administrative data; as such, there is the possibility of misclassification bias and residual confounding could influence our results and interpretation. We were unable to identify residents of retirement homes who did not receive home care services in licensed retirement homes with not unique postal codes. We were also unable to determine the occupancy of each retirement home, as the RHRA does not require operators to disclose this statistic as a condition for licensing (2). As the occupancy of each retirement home is unknown, the size of our cohort of residents of retirement homes may reflect the actual population size.
Residents of retirement home are a unique older adult population in Ontario, Canada. Future research should examine with more granularity the reasons why residents of retirement homes visited emergency departments and/or were hospitalized to understand their needs for hospital-based care that may not be met in their retirement home.
Data Availability
The dataset from this study is held securely in coded form at ICES. While data sharing agreements prohibit ICES from making the data set publicly available, access may be granted to those who meet pre-specified criteria for confidential access, available at www.ices.on.ca/DAS. The full data set creation plan and underlying analytic code are available from the corresponding author upon request, understanding that the programs may rely upon coding templates or macros that are unique to ICES.
SUPPLEMENTARY MATERIAL
RECORD Checklist
Characteristics of Licensed Retirement Homes in 2018 (n = 757)
Descriptions of the Health System Administrative Databases
Annual, Standardized Health Service Rates Among Residents of Retirement Homes, Residents of Long-Term Care Homes, and Home Care Recipients in the Community in 2018
Adjusted Beta Coefficients (Standard Errors) from Annual, Standardized Health Service Rates Among Residents of Retirement Homes, Residents of Long-Term Care Homes, and Home Care Recipients in the Community in 2018
Sex-Stratified Subgroup Analysis Adjusted Beta Coefficients (Standard Errors) from Annual, Standardized Health Service Rates Among Residents of Retirement Homes, Residents of Long-Term Care Homes, and Home Care Recipients in the Community in 2018
ACKNOWLEDGMENTS
This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health (MOH) and the Ministry of Long-Term Care (MLTC). Parts of this material are based on data and/or information compiled and provided by CIHI. The analyses, conclusions, opinions, and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred. We extend our gratitude to Paul Pham, Adriane Castellino, and Chloe Ma at the Retirement Homes Regulatory Authority for sharing the registry of licensed retirement homes.
Footnotes
Funding: This work was supported partially by Schlegel Chair in Clinical Epidemiology in Aging at McMaster University, as well as the Ontario Ministry of Health System Research Fund (2017-01097).
Competing Interests: We have no competing interests, financial or otherwise, to disclose.
REFERENCES



