
Abstract
Background and Objectives While most maintenance dialysis patients exhibit initial seroresponse to vaccination, concerns remain regarding the durability of this antibody response. This study evaluated immunity over time.
Design, setting, participants, and measurements This retrospective cohort study included maintenance dialysis patients from a midsize national dialysis provider who received a complete SARS-CoV-2 vaccine series and had at least one antibody titer checked after full vaccination. Immunoglobulin G spike antibodies (SAb-IgG) titers were assessed monthly with routine labs beginning after full vaccination and followed over time; the semiquantitative SAb-IgG titer reported a range between 0 and ≥ 20 U/L. Descriptive analyses compared trends over time by prior history of COVID-19 and type of vaccine received. Time-to-event analyses were conducted for the outcome of loss of seroresponse (SAb-IgG < 1 U/L or development of COVID-19). Cox proportional hazards regression was used to adjust for additional clinical characteristics of interest.
Results Among 1898 maintenance dialysis patients, 1567 (84%) had no prior history of COVID-19. Patients without a history of COVID-19 had declining titers over time. Among 441 BNT162b2/Pfizer recipients, median [IQR] SAb-IgG titer declined from 20 [5.99-20] U/L in month 1 to 1.30 [0.15-3.59] U/L by month 6. Among 779 mRNA-1273/Moderna recipients, median [IQR] SAb-IgG titer declined from 20 [20-20] in month 1 to 6.20 [1.74-20] by month 6. The 347 Ad26.COV2.S/Janssen recipients had a lower titer response than mRNA vaccine recipients over all time periods. In time-to-event analyses, Ad26.COV2.S/Janssen and mRNA-1273/Moderna recipients had the shortest and longest time to loss of seroresponse, respectively. The maximum titer reached in the first two months after full vaccination was predictive of the durability of the SAb-IgG seroresponse; patients with SAb-IgG titer 1-19.99 U/L were more likely to have loss of seroresponse compared to patients with SAb-IgG titer ≥ 20 U/L (HR 23.9 [95% CI: 16.1-35.5]).
Conclusions Vaccine-induced seroresponse wanes over time among maintenance dialysis patients across vaccine types. Early titers after full vaccination predict the durability of seroresponse.
Introduction
As of September 2021, the COVID-19 pandemic has claimed over 4.5 million lives worldwide, with more than 600,000 deaths in the United States.1 The three vaccines currently authorized for use by the Food and Drug Administration, either with approval or emergency use authorization, are all highly effective at preventing death and serious illness in the general population.2–4
Concerns about the robustness of the vaccine-induced immune response in vulnerable populations5–7 have prompted the Centers for Disease Control and Prevention (CDC) to recommend an additional dose for immunocompromised patients,8 while concerns about the durability of response have prompted discussion of booster doses of vaccine.9 The implications for patients receiving maintenance dialysis remain unclear at this time. Early studies have shown that the majority of maintenance dialysis patients generate an appropriate initial seroresponse to mRNA vaccines, although at a lower rate than the general population.10–17 Given that maintenance dialysis patients have an attenuated response to other vaccines, with extensive data on additional or booster doses for hepatitis B vaccination,18 similar concerns exist that potential uremia-associated immunocompromise may impact the response to SARS-CoV-2 vaccines. A small study in 76 dialysis patients demonstrated antibody decline in 75% of patients, with almost 20% becoming seronegative by 4 months.19 In the general population, waning immunity has been linked to increased breakthrough cases.20,21 Given the very high risk for poor outcomes associated with COVID-19 in maintenance dialysis patients, as well as their limited ability to physically distance, obtaining and maintaining immunity is of critical importance.22,23 We therefore conducted a retrospective multicenter study to assess the intermediate duration of vaccine-induced seroresponse among maintenance dialysis patients. Expanding on an earlier publication,11 we report here the seroresponse trends over time.
Methods
Dialysis Clinic, Inc. (DCI) is a national not-for-profit provider that cares for more than 15,000 patients at 260 outpatient dialysis clinics across 29 states. Since January 2021, DCI physicians have had available an antibody monitoring protocol for patients, activated by physician order upon documentation of receipt of a SARS-CoV-2 vaccine, regardless of the vaccine type or place of administration. Like the existing hepatitis B vaccine protocol, the SARS-CoV-2 vaccine protocol documents seroresponse to vaccination by measuring antibody titers as part of the monthly blood draws. Immunoglobulin G spike antibodies (SAb-IgG) against the receptor-binding domain of the S1 subunit of SARS-CoV-2 spike antigen were measured using the chemiluminescent assay ADVIA Centaur® XP/XPT COV2G, which received emergency use authorization in July 2020.24 This semi-quantitative assay has a range between 0 and ≥ 20 U/L; per manufacturer specifications, SAb-IgG titer ≥ 1 U/L represents detectable antibodies, likely signifying seroresponse.24
Demographic and clinical data, vaccination dates, and SAb-IgG titer results were obtained from the DCI electronic health record. Patients were included if they had received a complete vaccine series of one vaccine type without additional doses. Patients were excluded from analysis if they were less than 18 years of age or did not have at least one antibody titer assessment 14 days or more after completion of a vaccine series (hereafter termed “fully vaccinated” in accordance with current CDC guidelines25). Baseline characteristics were assessed at the time of full vaccination. Prior COVID-19 was defined by a positive SARS-CoV-2 PCR test at any time before the date of full vaccination or SAb-IgG titer ≥ 1 U/L before or within 10 days after the first vaccine dose (representing likely prior undiagnosed COVID-19, as suggested by prior studies2,26). Positive SARS-CoV-2 tests were captured regardless of whether the patient was assessed in the dialysis clinic, at a testing center, or at a hospital. Analyses were stratified by prior COVID-19 status.
In analyses, SAb-IgG titers were grouped by the month of assessment relative to the date of full vaccination (month 1, 2, etc). Primary descriptive analyses compared titers by vaccine type over time. To assess whether initial vaccine response predicted sustained response, secondary descriptive analyses compared trends over time, stratifying by the maximum titer attained during the first two months following full vaccination (“maximum initial titer”). Handling of missing and duplicate values is described in the Supplemental Methods.
To better characterize antibody levels over time, time-to-event analysis was used to assess for the outcome of antibody titer <1 U/L or development of COVID-19, defined as having a positive SARS-CoV-2 test. Sensitivity analyses were conducted for the outcome of antibody titer <2 U/L or development of COVID-19, using a threshold suggested by DCI Lab’s internal validation methods.11 Of note, all DCI patients are screened for COVID-19 symptoms and recent exposure upon arrival to the dialysis facility for each treatment, followed by SARS-CoV-2 testing if they screen positive. Patients were censored at death, transplantation, or last available titer assessment. Results were compared by vaccine type and by maximum initial titer in descriptive analyses. Multivariable Cox proportional hazards regression was used to associate patients’ clinical characteristics with the outcome.
This study was reviewed and approved by the WCG IRB Work Order 1-1456342-1. Statistical analyses were performed using R v4.0.2.
Results
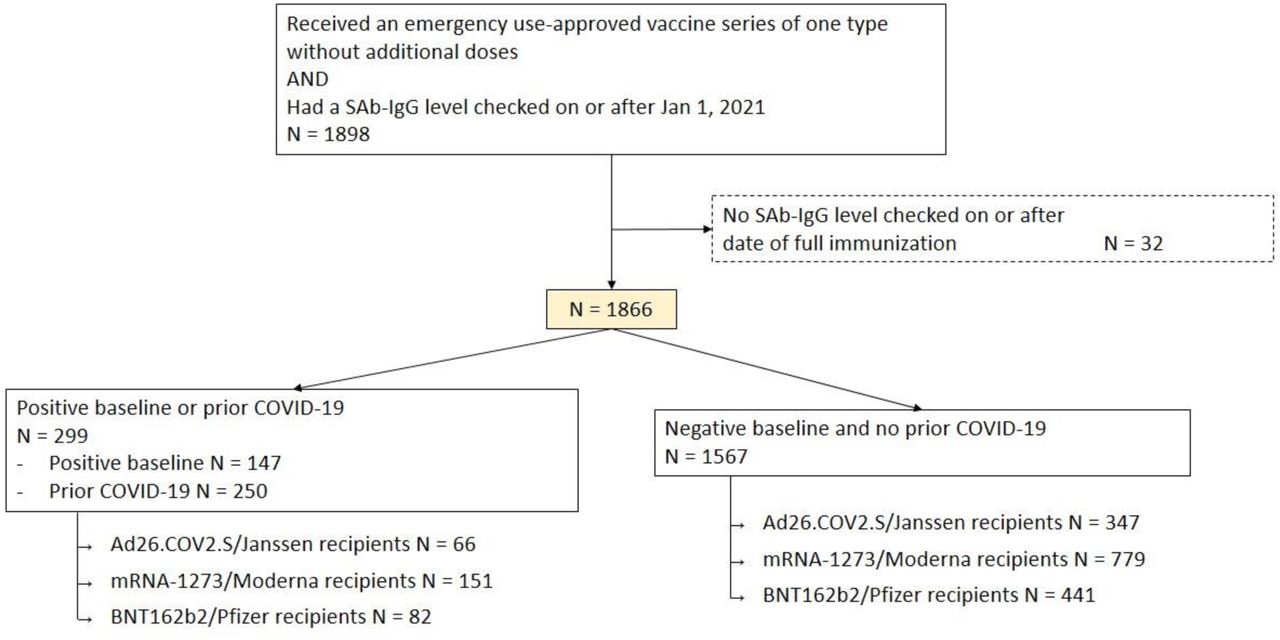
Among DCI patients, 1898 adults received a full SARS-CoV-2 vaccine series and had at least one SAb-IgG titer assessment after January 1, 2021, with 1866 patients having SAb-IgG assessment following full vaccination (Figure 1). Of these, 1084 (58.1%) were male, 437 (23.4%) were African-American, 298 (16.0%) were Hispanic, and the average age was 63.9 ± 13.7 (SD); 299 (16.0%) had a history of COVID-19 based on either early positive SAb-IgG levels or prior positive testing. BNT162b2/Pfizer recipients tended to be older and have longer follow-up, while Ad26.COV2.S/Janssen recipients tended to be of Black race or non-Hispanic ethnicity. Among the 1567 patients without a history of COVID-19, a higher proportion of mRNA-1273/Moderna recipients were receiving peritoneal dialysis compared to BNT162b2/Pfizer and Ad26.COV2.S/Janssen recipients (Table 1).
Baseline defined by SAb-IgG titer > 1 before or within 10 days after first dose of vaccine
Prior COVID-19 defined as positive SARS-CoV-2 test before full immunity (at 14 days after completion of a vaccine series)
Patients without a history of COVID-19 who received mRNA vaccine had declining SAb-IgG titers over time (Figure 2A). Among BNT162b2/Pfizer recipients, median [IQR, N number of data values] antibody titer was 20 [5.99-20, N of 339] U/L in month 1, with a reduction to 2.69 [0.70-9.38, N of 337] by month 4 and 1.30 [0.15-3.59, N of 174] U/L by month 6. Among mRNA-1273/Moderna recipients, median [IQR, N number of data values] SAb-IgG titer declined from 20 [20-20, N of 646] in month 1 to 20 [4.03-20, N of 604] by month 4 and to 6.20 [1.74-20, N of 85] by month 6. Over all time periods, Ad26.COV2.S/Janssen recipients had median [IQR] SAb-IgG titer of less than 1 U/L, without significant change over time. Among patients with a history of COVID-19, more than 75% of mRNA vaccine recipients maintained antibody titer at the upper limit of the assay’s detection (20 U/L) through month 6; this is true also of Janssen vaccine recipients through month 5 (with 6-month data limited by the number of participants with follow-up to this time point) (Figure 2B).
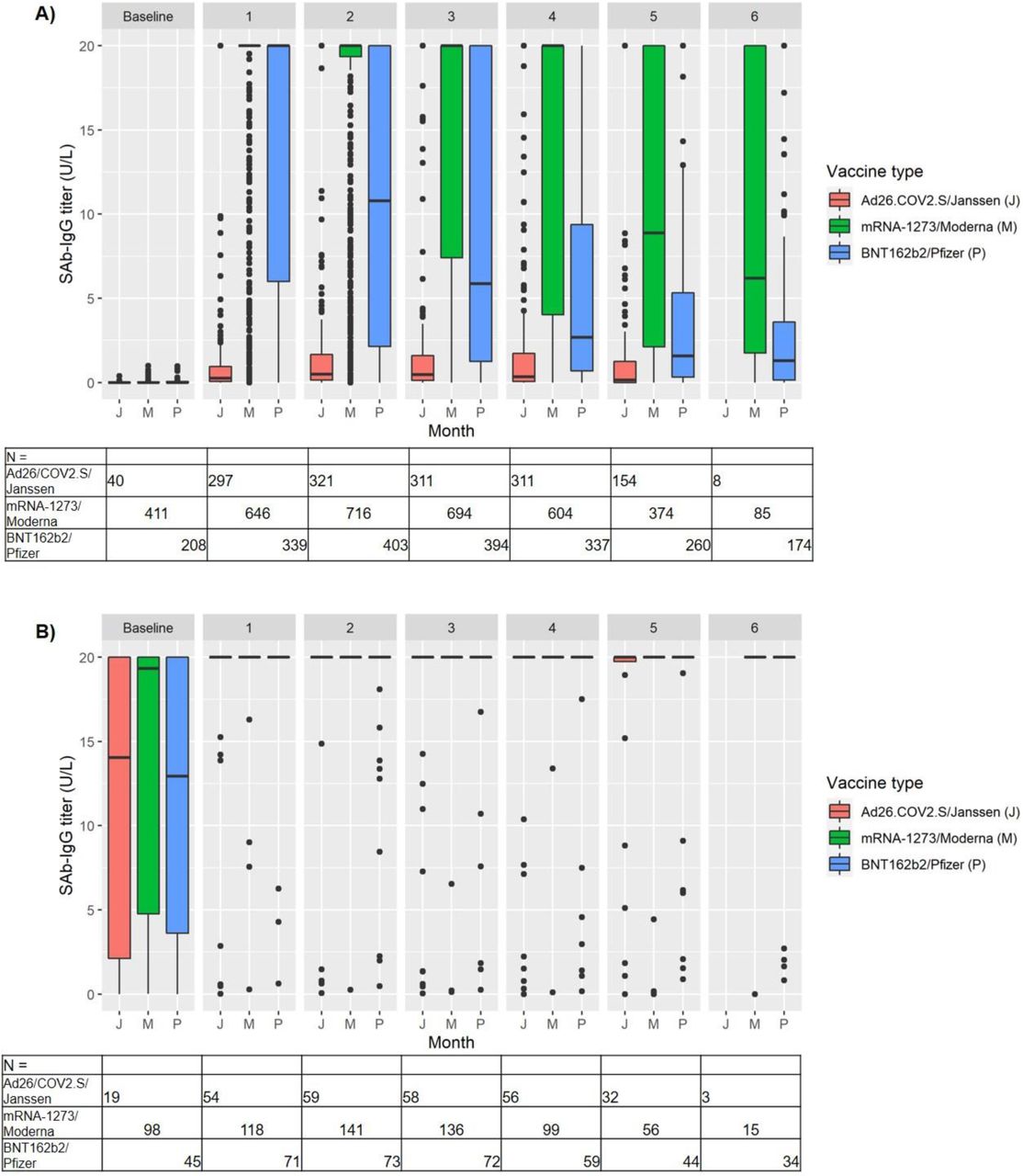
A) Patients without prior COVID-19
B) Patients with prior COVID-19
The tables of N show the number of titers for each month, by vaccine type.
Data are not shown for groups with N < 10
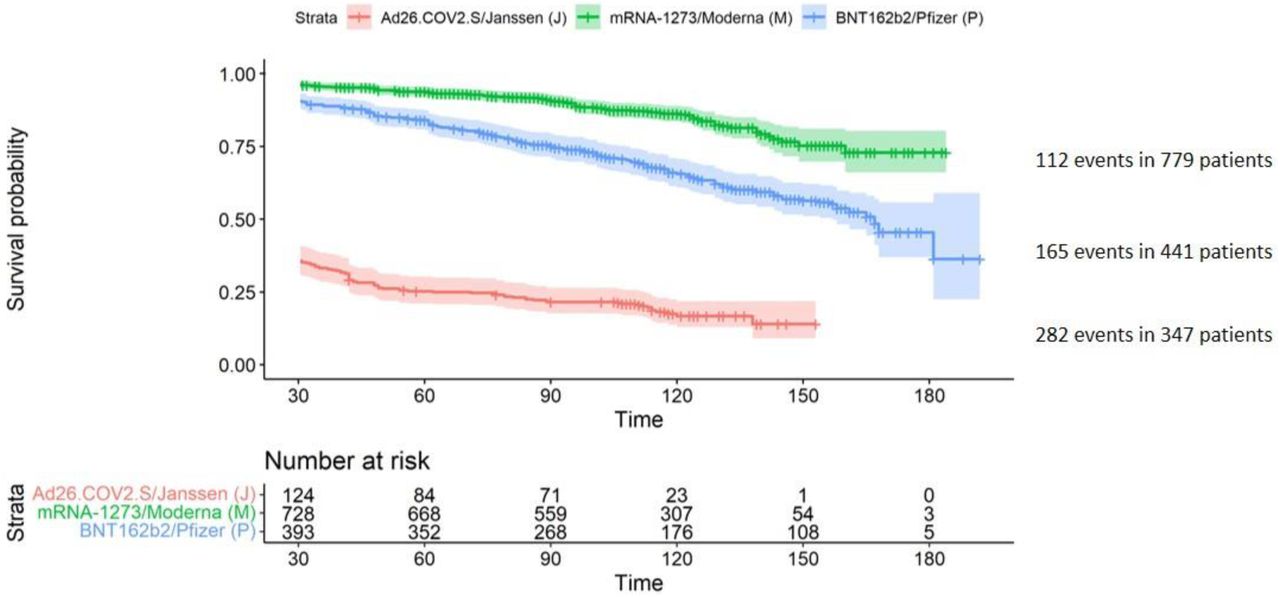
Among the 1567 patients without a history of COVID-19, 559 developed SAb-IgG titer < 1 U/L or were diagnosed with COVID-19 (556 and 3 patients, respectively). Time-to-event analysis showed a difference by vaccine type, with Ad26COV2.S/Janssen recipients having the shortest time to SAb-IgG < 1 U/L while mRNA-1273/Moderna recipients had more durable SAb-IgG titer levels (Figure 3). At month 4, 67.5% of Janssen, 32.1% of Pfizer and 12.3% of Moderna recipients had SAb-IgG titers less than 1 U/L; at month 6, 43.9% of Pfizer and 14.1% of Moderna recipients had SAb-IgG titers less than 1 U/L (as noted, 6-month data on Janssen recipients is limited by the number of participants with follow-up to this time point). Sensitivity analysis using the threshold of SAb-IgG titer <2 instead showed more events occurring, as expected, but the differences by vaccine type remained (Supplemental Figure S1).

Data are shown beginning at Day 30, at which time all patients have had at least one opportunity for assessment of the outcome of Ab titer < 1 U/L via monthly labs. Patients were censored at death, transplantation, or last available titer assessment.
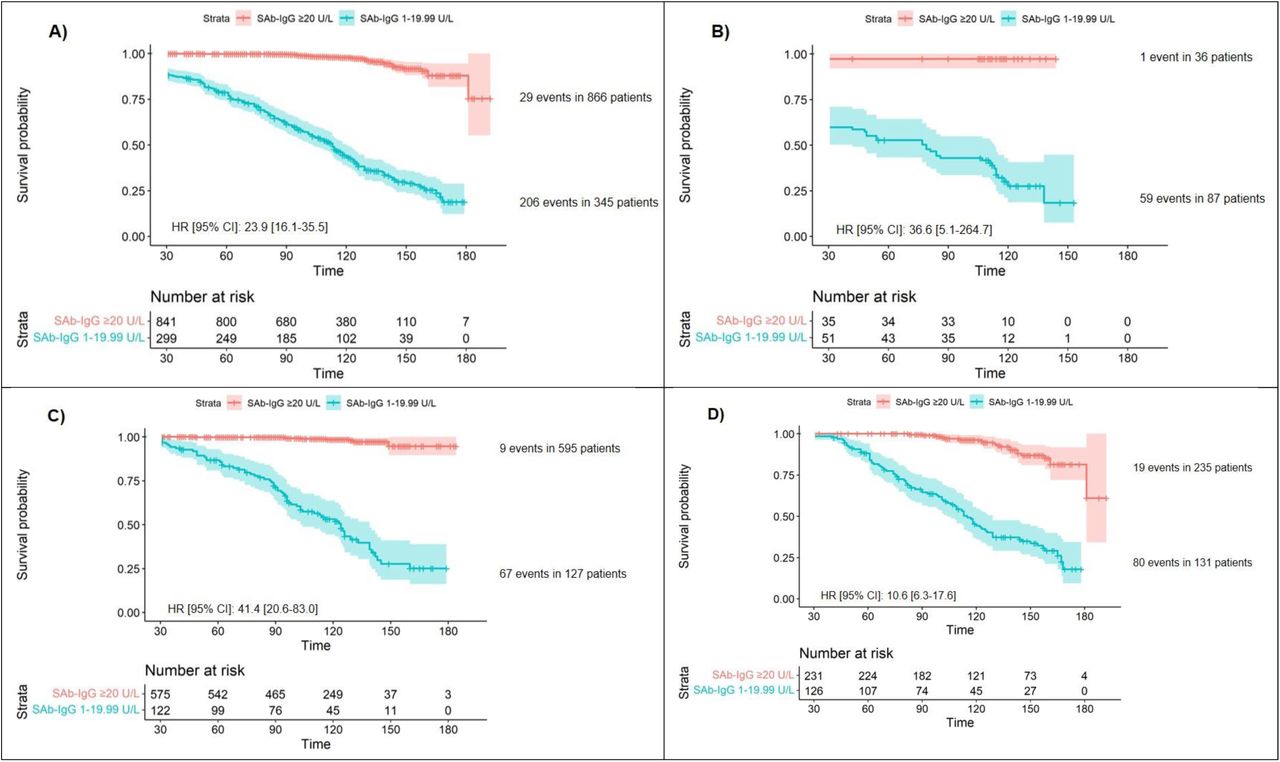
To assess whether initial seroresponse predicts sustained response, patients were then grouped by maximum titer measured during the first two months following full vaccination: 866, 345, and 302 patients had maximum initial titer of ≥ 20, 1 to 19.99, and less than 1 U/L, respectively, while 54 patients did not have a titer assessed during the first two months of full immunity and were excluded from this analysis. Black race, non-Hispanic ethnicity, and use of immunomodulating medications were more likely to be associated with a maximum initial titer of less than 1. Moderna recipients were more likely to have a maximum initial titer of 20 U/L or higher, and Janssen recipients were more likely to have a maximum initial titer of less than 1 U/L (Table 2).
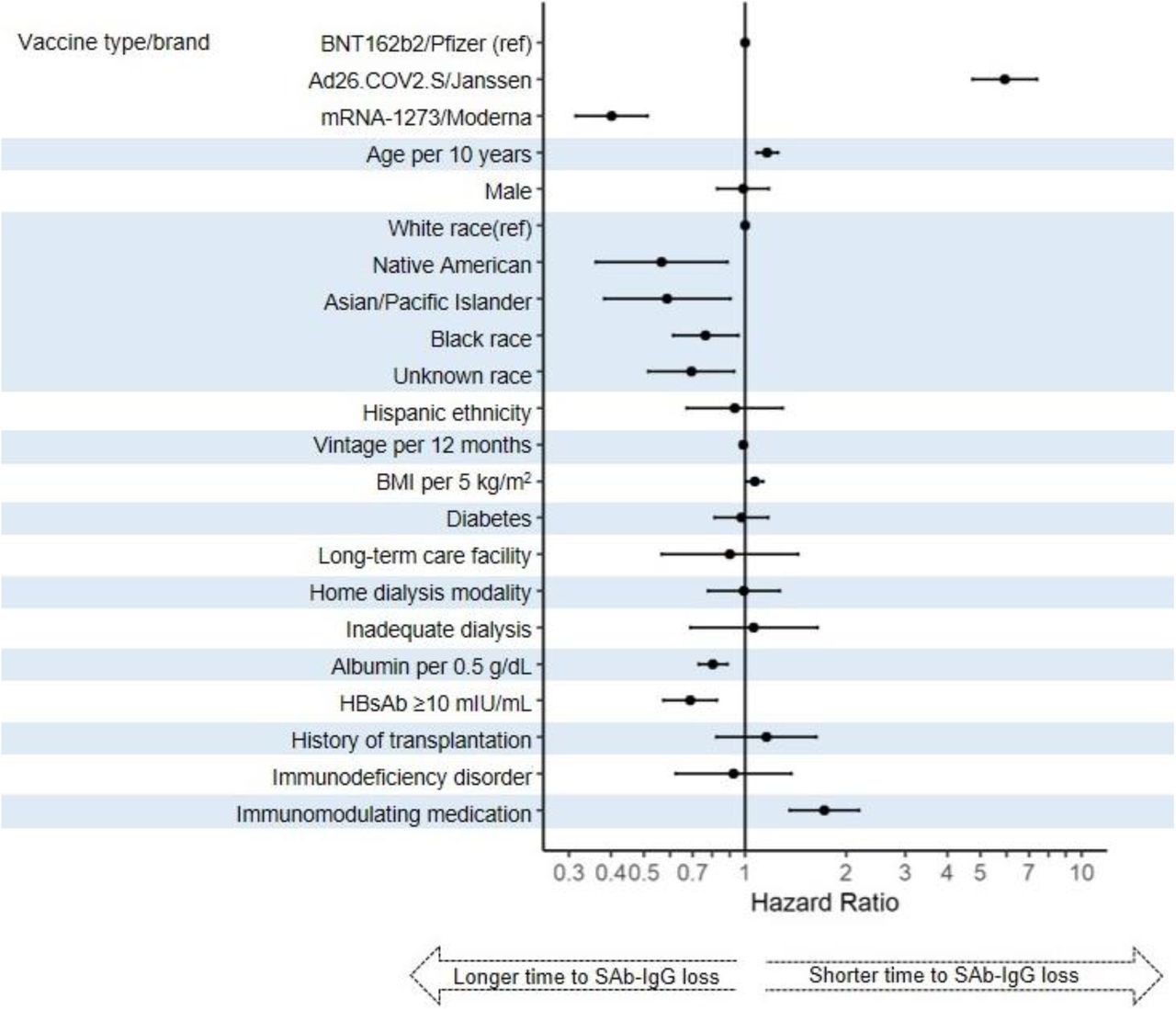
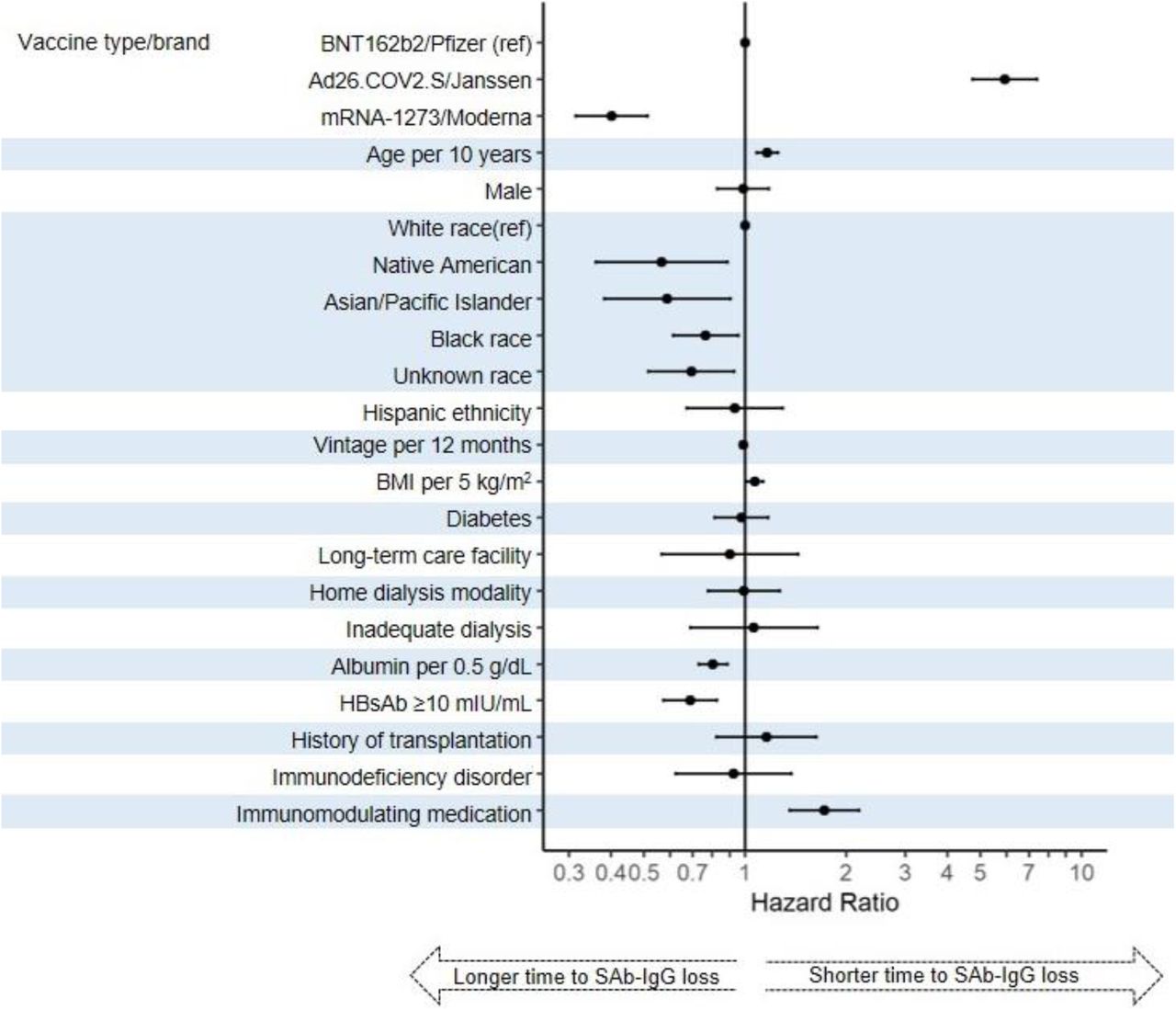
In time-to-event analysis, those who had a maximum initial titer ≥ 20 U/L were less likely to develop the outcome of titer less than 1 U/L or COVID-19 compared to those with a maximum initial titer from 1 to 19.99 U/L. This difference persisted even among recipients of the same vaccine type (Figures 4A-D) and in sensitivity analyses for the outcome of titer less than 2 U/L (with corresponding change in strata thresholds, Supplemental Figures S2A-D). In multivariate Cox proportional hazards regression, in addition to differences by vaccine type, older age, White race, higher body mass index, lower albumin, lack of hepatitis B seroimmunity, and use of immunomodulating medications were associated with shorter time to loss of seroresponse (Figure 5). In sensitivity analyses, body mass index was no longer associated with loss of seroresponse; other findings were similar (Supplemental Figure S3).
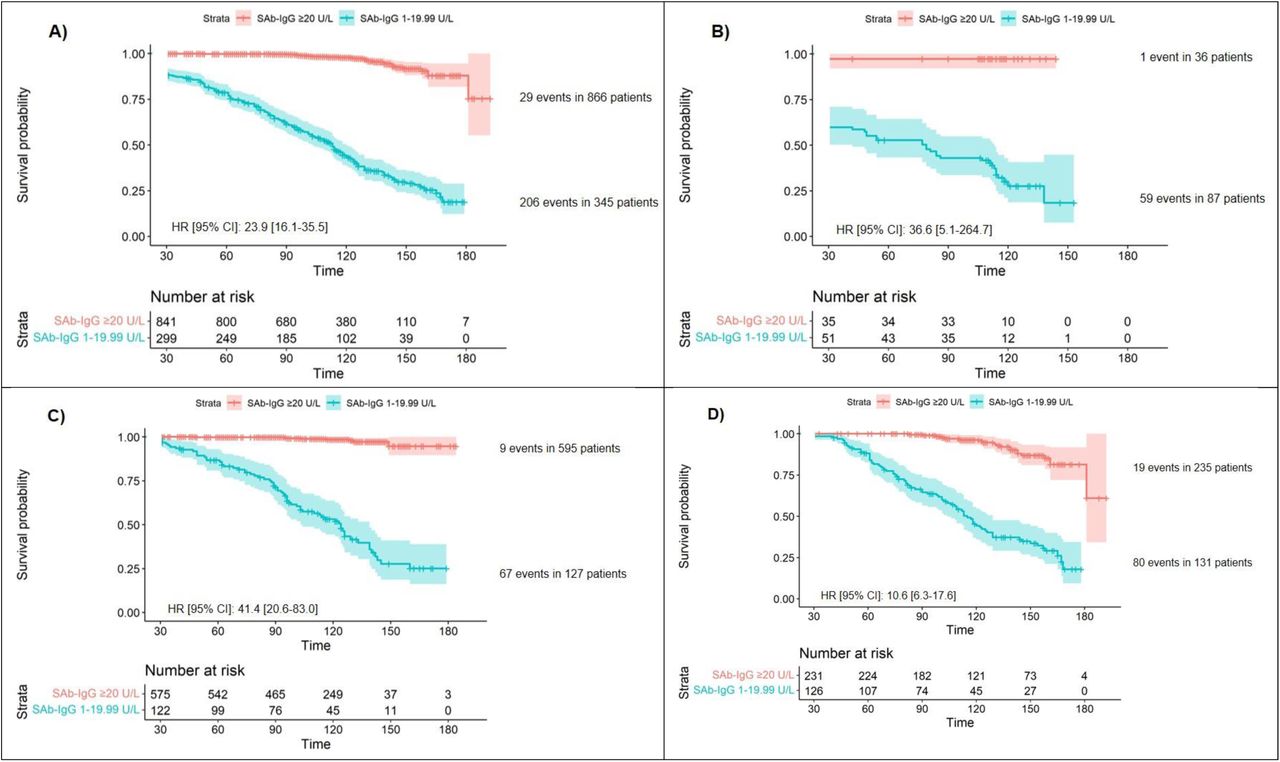
Data are shown beginning at Day 30, at which time all patients have had at least one opportunity for assessment of the outcome of SAb-IgG titer < 1 U/L via monthly labs. Patients were censored at death, transplantation, or last available titer assessment. Patients with maximum initial SAb-IgG titer are not shown since, given our definition of maximum initial titer, all had experienced the outcome by the end of month 2.
A) All patients
B) Ad26.COV2.S/Janssen recipients only
C) mRNA-1273/Moderna recipients only
D) BNT162b2/Pfizer recipients only
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Inadequate dialysis defined by hemodialysis dose spKt/V<1.2 or peritoneal dialysis dose weekly Kt/V<1.7 HBsAb ≥10 mIU/mL signifies hepatitis B seroimmunity
Discussion
Among a national population of maintenance dialysis patients in the United States, mRNA vaccines elicited greater seroresponse than the Ad26.COV2.S/Janssen vaccine, but antibody titers against the SARS-CoV-2 spike protein waned substantially over the first six months following full vaccination among patients without a prior history of COVID-19. Furthermore, the robustness of the initial antibody response appears to predict the rapidity of subsequent waning of antibody levels. Other predictors of the duration of seroresponse largely reflect patients’ immune health.
As of August 13, 2021, the CDC recommends a third dose of mRNA vaccine for those with moderate to severe immunocompromise.8 The inclusion of maintenance dialysis patients within this classification is non-specific and depends upon the medical judgment of the treating clinician. Critically, initial studies suggest that vaccine-induced immunity among maintenance dialysis patients immediately following receipt of a vaccine series was intermediate, with somewhat lesser response than among the general population but a greater response than among patients receiving immunosuppression for transplantation or other indications.10–17 Our data provide longitudinal evidence of immunity waning fairly rapidly over time, contrasting somewhat with SAb-IgG titers measured over time in healthy adults.27–30 These data estimate that, even following current vaccination standards, about half of maintenance dialysis patients will have suboptimal vaccine-induced protection in the fall of 2021, a time of projected high community prevalence of COVID-19.31,32 While the antibody level needed for protection from disease has not been definitively determined, a general correlation between seroimmunity and protection from disease has been observed.33 Additionally, individuals with seroimmunity may be less likely to transmit the virus, providing protection to other vulnerable patients in mandatory congregate healthcare settings.34,35 Similar data on waning immunity prompted officials in France to recommend an additional vaccine dose to maintenance dialysis patients in April 2021, with some early evidence of subsequent strengthened immunity in several small studies.26,36–38
There may be a role for wider routine monitoring of SAb-IgG titers for maintenance dialysis patients. Seroimmunity to hepatitis B is currently monitored through such a protocol, and, due to this population’s regular and frequent contact with the medical system, routine testing and administration of additional doses would not be logistically difficult. In particular, the peak response in the first two months of full immunity indicates one’s likely course and could be used to anticipate the timing of loss of seroimmunity.30 Of note, the CDC currently does not recommend using COVID-19 antibody testing to guide clinical decision-making.39
This study represents a real-world, geographically diverse, multi-center population of maintenance dialysis patients in the United States, in whom prior risk of COVID-19 morbidity and mortality has been documented.23,40 We acknowledge this study’s limitations. As with all observational studies, confounding variables may affect interpretation of results. In particular, data for months 5 and 6 primarily reflect patients who received their doses vaccine early (e.g. January and February of 2021) with a moderately higher proportion of BNT162b2/Pfizer vaccine recipients, and these patients may be frailer at baseline. In addition, we did not correlate antibody titers with breakthrough infection, an issue which remains complex and controversial.
In conclusion, immunity to SARS-CoV-2 vaccines, as indicated by SAb-IgG titers, wanes over time in maintenance dialysis patients without a prior history of COVID-19. In the setting of SARS-CoV-2 variants of concern, the impact of waning titers on breakthrough infections needs to be monitored closely. The current CDC recommendation to provide a third vaccine dose based on clinical assessment for immune compromise is an important consideration for the maintenance dialysis population. A large proportion of maintenance dialysis patients have suboptimal response to the currently recommended vaccine regimens. Therefore, additional doses of vaccine should be considered for this vulnerable population, whether routinely or, with further investigation, potentially guided by protective correlates such as antibody response.
Footnotes
Support: This report was supported by Dialysis Clinic, Inc. CMH receives support from ASN KidneyCure’s Ben J. Lipps Research fellowship. CMH’s funder had no role in study design, data collection, reporting, or the decision to submit.
Financial Disclosure: Mr. Aweh, Dr. Manley, Mr. Ladik, Ms. Frament, Dr. Johnson and Dr. Lacson Jr are all employees of DCI, where Dr. Johnson is Vice Chair of the Board. Dr. Weiner, Dr. Miskulin, Dr. Agyropoulos, Dr. Abreo, Dr. Chin, Dr. Gladish, and Dr. Salman receive salary support to their institution from DCI.
References




Subject Area
Reviews and Context
0
Comment
0
TRIP Peer Reviews
0
Community Reviews
0
Automated Services
24
Blogs/Media
Author Videos