
Abstract
Objectives To determine whether COVID-19 efficacy varies with clinical risk category and to investigate risk factors for severe COVID-19 in those who have received two doses of vaccine.
Design Matched case-control study (REACT-SCOT).
Setting Population of Scotland from 1 December 2020 to 19 August 2021.
Main outcome measure Severe COVID-19, defined as cases with entry to critical care or fatal outcome.
Results Efficacy against severe COVID-19 of two doses of vaccine was 93% (95 percent CI 90% to 95%) in those without designated risk conditions, 89% (95 percent CI 85% to 92%) in those with moderate risk conditions, but only 66% (95 percent CI 52% to 76%) in those designated as clinically extremely vulnerable (CEV) and eligible for shielding. Of the 330 cases of severe COVID-19 in double-vaccinated individuals, 47% had moderate risk conditions and 41% were CEV. In the double-vaccinated CEV group, the rate ratio for severe disease (with no risk condition as reference category) was highest in solid organ transplants at 98 (95% CI 29 to 332) but even in this subgroup the absolute risk of severe COVID-19 was low (14 cases in 16079 person-months of follow-up).
Conclusions Two doses of vaccine protect against severe COVID-19 in CEV individuals but the residual risk in double-vaccinated individuals remains far higher in those who are CEV than in those who are not. These results suggest that any policy of offering booster doses to doubly-vaccinated individuals should focus initially on the clinically vulnerable, and lay a basis for determining eligibility for passive immunization to protect those at highest risk.
Introduction
The REACT-SCOT matched case-control study was established by Public Health Scotland at the beginning of the epidemic to investigate risk factors for severe COVID-19 (1). Using this framework, we have reported on the relation of severe COVID-19 to risk conditions including those designated as clinically extremely vulnerable (CEV) and therefore eligible for the shielding programme in Scotland (1–3). We have previously reported a comparison of the efficacy of vaccination against severe COVID-19 between CEV people and those with moderate risk conditions or no risk conditions, based on data up to 16 March 2021 (4). At this time few individuals had received a second dose of vaccine, but since then most CEV individuals have received two doses. This report updates and extends the earlier analyses, with the following objectives:
To determine whether vaccine efficacy varies with risk category and CEV status now that more data, including exposure to two doses of vaccine, are available and now that the Delta variant is the dominant variant in Scotland.
To investigate risk factors for severe or hospitalised COVID-19 in those who have received two doses of vaccine.
Methods
We used the REACT-SCOT study to take advantage of data linkages already established. The design has been described in detail previously (1). In brief, for every incident case of COVID-19 in the population ten controls matched for one-year age, sex and primary care practice and alive on the day of presentation of the case that they were matched to were selected using the Community Health Index database. COVID-19 cases are those with a positive nucleic acid test, or a hospital admission or death with COVID-19 ICD-10 codes. The REACT-SCOT case-control dataset is refreshed regularly and is linked to the vaccination database and to the regularly updated dataset of all individuals deemed eligible for the shielding programme. Though the data extract included cases presenting up to 2 September 2021, the analyses reported here are restricted to cases and controls presenting from 1 December 2020 to 19 August 2021, ensuring follow-up for at least 14 days after presentation date to allow cases to be classified as severe or hospitalised.
Classification of risk categories
As previously (1), to minimise ascertainment bias we pre-specified the primary outcome measure as severe COVID-19, defined as diagnosed cases with entry to critical care within 28 days of presentation or fatal outcome (any death within 28 days of a positive test or any death for which COVID-19 was coded as underlying cause). Cases and controls were classified into three broad risk categories: no risk condition; at least one of the moderate risk conditions designated by public health agencies (1); or eligible for shielding (3). For further analyses, the shielding category was subdivided as described previously into six categories: solid organ transplant, specific cancers, severe respiratory conditions, other rare conditions, on immunosuppressants, and additional conditions (3). This corresponds to the list used by Public Health Scotland (5), after combining the small numbers in the group “pregnant with heart disease with the”other conditions” category. For additional analyses the category “specific cancers” was split to allocate cancers of blood-forming organs (ICD-10 codes C81-C88, C90-C96) to a separate category.
Statistical analysis
The matched design controls for age, sex, general practice and calendar time to single day. Covariates included in the models were those that have been previously identified as strong predictors of severe disease in this population: care home residence, number of adults in household, number of non-cardiovascular drug classes dispensed and recent hospital stay (1–3). For care home residents the number of of adults in the household was coded as 1 to ensure that these two variables are not confounded. The number of non-cardiovascular drug classes was calculated as the number of distinct BNF subparagraph codes for which a prescription was dispensed between 15 and 240 days before presentation date. The number of hospital diagnoses was calculated as the number of distinct ICD-10 chapters represented at least once in hospital discharge records between 25 days and 5 years before presentation date. Recent hospital stay was defined as any in-patient stay from 5 to 14 days before presentation date.
Vaccination status was coded as the number of doses administered at least 14 days before presentation date. Vaccine doses administered less than 14 days before presentation date were ignored. The effect of vaccination in each of the clinical vulnerability categories was estimated in a conditional logistic regression model specifying effects βR2, …, βRJ for the log rate ratio associated with risk categories 2 to J (βR1 = 0 for the reference category J = 1), and nested effects βV 1, …, βV J for the log rate ratio associated with vaccination in each of the J risk categories. With this incidence density sampling design, the conditional odds ratio is the rate ratio. The efficacy of vaccination is 1 minus the rate ratio. The unconditional odds ratios calculated from frequency tables of the vaccination status of cases and controls in each risk group cannot be used to estimate rate ratios (6,7).
Cohort analysis of the shielding list
The case-control study estimates only rate ratios. To investigate how the absolute rates of severe disease in those listed as clinically extremely vulnerable have changed with the vaccination programme rollout, we also undertook a cohort analysis of all individuals who had ever been on the shielding list. A Poisson regression model was fitted to the cohort formatted with one observation per 28-day person-time interval, and individuals censored at first diagnosis of COVID-19. Event status was defined as severe COVID-19 presenting within the person-time interval, and the covariates were sex, baseline age, and shielding eligibility group. The baseline hazard rate was modelled as a natural spline function of calendar time with 6 degrees of freedom. To allow comparison with how the rates of all diagnosed cases varied with calendar time, a similar model was fitted with event status defined as any diagnosed case.
Results
Relation of vaccine efficacy to risk conditions
As shown in Table 1 from 1 December 2020 to 19 August 2021 there were 5168 cases of severe COVID-19 in the total population of Scotland of whom 27% had no designated risk condition, 52% had a moderate risk condition and 21% were CEV. The distributions in cases and controls of other risk factors included as covariates in the models are shown for completeness. Overall 84% of severe cases arising in this period were not yet vaccinated. Table S1 shows the same tabulation with case definition broadened to include all 17121 hospitalised cases and their matched controls.
Numbers of cases of severe COVID-19 and matched controls, by risk group and vaccine product
Table 2 shows rate ratios associated with 1 and 2 vaccine doses (with 0 doses as reference category) in each of the three broad risk categories from the conditional logistic regression model. The model included risk categories (no risk conditions as reference category), care home residence, number of adults in household, number of drug classes and recent hospital stay as covariates. The rate ratio associated with two doses of vaccine was 0.07 (95% CI 0.05 to 0.10) in those without risk conditions, 0.11 (95% CI to 0.15) in those with moderate risk conditions, and 0.34 (95% CI 0.24 to 0.48) in the CEV group. On the scale of efficacy, these estimates are equivalent to 93% (95 percent CI 90% to 95%) in those without risk conditions, 89% (95 percent CI 85% to 92%) in those with moderate risk conditions, and 66% (95 percent CI 52% to 76%) in the CEV group. Table S2 shows the same model with case definition broadened to include all hospitalised cases and their matched controls: the efficacy of 2 doses against hospitalisation also was lower at 67% (95 percent CI 61% to 72%) in the CEV than in the other two risk categories. The difference in vaccine efficacy between the CEV group and the other two risk categories was not explained by differences in time since second dose; the relation of vaccine efficacy to calendar time and time since second dose will be reported separately.
Rate ratios for severe COVID-19 within risk groups associated with vaccine dose: unvaccinated as reference category
Table 3 shows rate ratios associated with vaccination by risk group with the CEV group subdivided into six categories. Rate ratios were higher (and thus efficacy was lower) in all shielding eligibility subgroups than in those without risk conditions or with moderate risk conditions, but the confidence intervals were too wide for comparisons of efficacy between CEV subgroups. Within the “Specific cancers” group, efficacy of two doses did not differ between those with blood cancers and those with other types of cancer but the confidence intervals were wide. Table S3 shows rate ratios for the first and second dose with the case definition broadened to include all hospitalised cases and their matched controls. In this table the highest rate ratio (lowest efficacy) is in solid organ transplant recipients but again the confidence intervals are too wide for comparisons of efficacy between CEV subgroups.
Rate ratios for severe COVID-19 associated with vaccine dose within clinically extremely vulnerable subgroups/2, 1
We examined whether there was any difference in efficacy by class of vaccine and whether any such differences varied by risk category. Table 4 shows rate ratios associated with 1 and 2 doses of each class of vaccine (with 0 doses as reference category) in each of the three broad risk categories. Table S4 shows the same model with case definition broadened to include all hospitalised cases and their matched controls. Although the confidence intervals for the rate ratios associated with 1 or 2 doses of each vaccine product in the CEV group are wide, it is clear that for both classes of vaccine product the efficacy of 2 doses is lower in the CEV group than in those with moderate risk conditions or no risk conditions. Efficacy of two doses against severe COVID-19 in the CEV group did not differ between the AstraZeneca vaccine (63% (95 percent CI 46% to 75%)) and the mRNA vaccines (72% (95 percent CI 51% to 84%)).
Rate ratios for severe COVID-19 within risk groups: vaccine dose and product encoded as categoric variable with unvaccinated as reference category
Risk factors for severe COVID-19 in the double-vaccinated
Table 5 shows risk factors for severe COVID-19 in cases and controls who had received 2 doses of vaccine at least 14 days before presentation date. Table S5 shows the same analysis with case definition broadened to include hospitalized cases and matched controls who had received 2 doses of vaccine. Only 13% of double-vaccinated severe cases had no designated risk condition: 44% had at least one moderate risk condition and 43% were eligible for shielding. Of the variables that we have previously reported as risk factors for severe COVID-19 in the general population, care home residence and socioeconomic deprivation were not associated with severe disease in the double-vaccinated. In this group the risk factors for severe disease were designated risk conditions, other indicators of co-morbidity including numbers of hospital diagnoses and drug classes prescribed and transmission-related factors including number of adults in household and recent hospital stay. A risk score for hospitalised or fatal COVID-19 in the double-vaccinated calculated from the multivariable conditional logistic regression model in Table S5 was able to distinguish severe cases from noncases with a C-statistic of 0.8. Among the CEV groups, the highest rate ratio for severe disease was solid organ transplant recipients: with no risk conditions as reference category, the unadjusted rate ratio associated with receipt of a solid organ transplant among the double-vaccinated was 98 (95% CI 29 to 332) for severe disease and 40.8 (95% CI 21.0 to 79.5) for hospitalisation.
Risk factors for severe COVID-19 in those who had received 2 doses of vaccine at least 14 days before
Shielding cohort
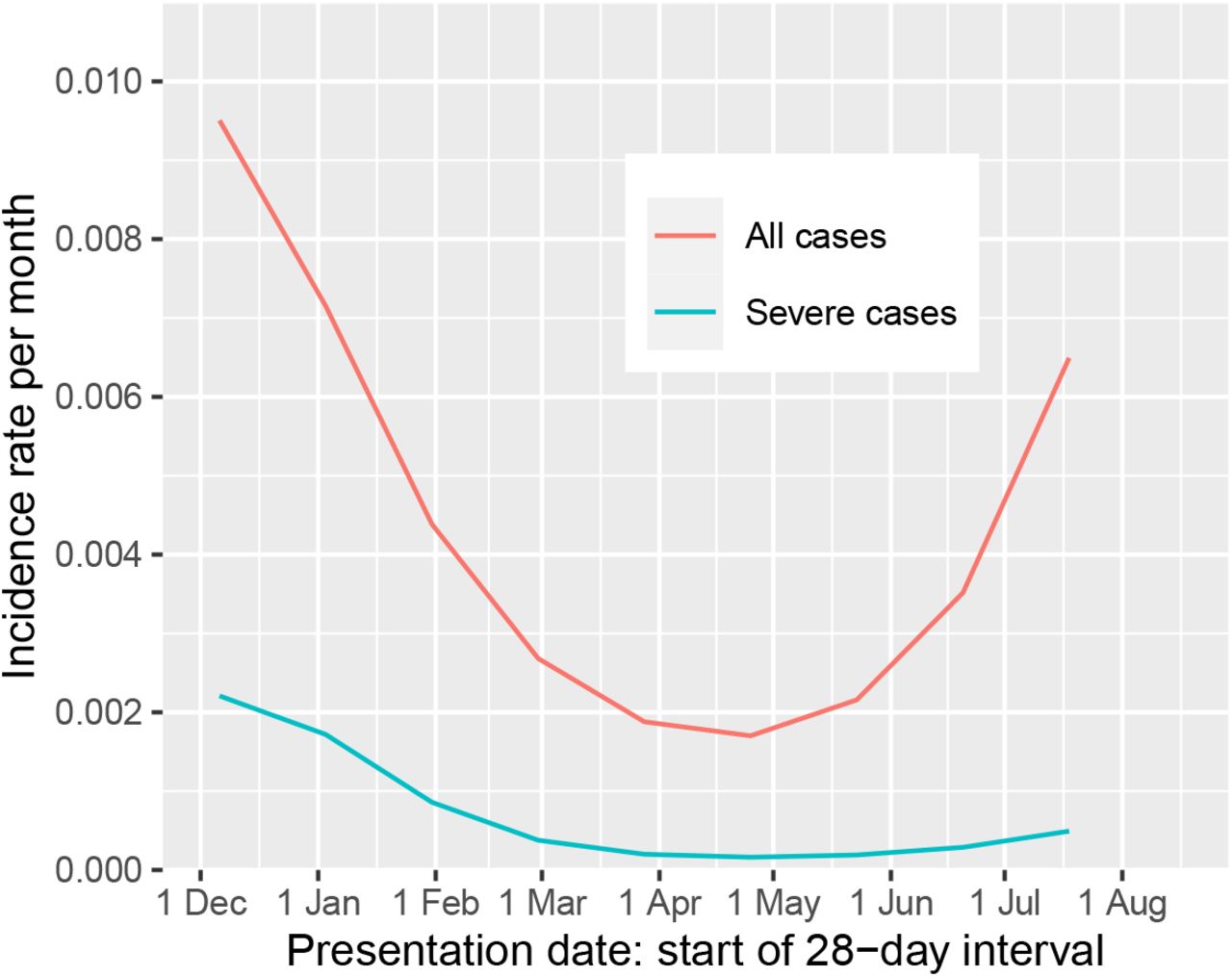
By the date of the latest extract of the shielding list in July 2021, 8230 (4%) of the 202510 individuals who had ever been on the shielding list had been diagnosed with COVID-19, and 18893 (9%) had been removed from the list for other reasons. Fig 1 shows the fitted incidence per month of any diagnosis and of severe cases in Poisson regression models fitted to the entire cohort. The incidence of any diagnosed COVID-19 in the shielding cohort fell from 1 December to a nadir in late April. Despite the incidence of any diagnosed COVID-19 rising steeply from 1 May onwards, the incidence of severe COVID-19 rose only slightly.

{kind=link}
Fitted values for monthly incidence of any case and severe case in the shielding cohort, based on Poisson regression with spline terms for calendar time
Table S6 shows the incidence of severe COVID-19 in double-vaccinated CEV individuals, by subgroup. In the highest risk group – solid organ transplant recipients – the incidence was 0.9 per 1000 per month (14 cases in 16079 person-months of follow-up).
Discussion
Statement of principal findings
Although the efficacy of two doses of vaccine against severe COVID-19 in those without risk conditions remains around 90%, it is now clear that efficacy in clinically extremely vulnerable individuals is somewhat lower at 66%. On the scale of absolute risk reduction, a reduction by two-thirds of fivefold elevated risk in unvaccinated CEV individuals is of course greater than a reduction of baseline risk by nine-tenths.
Among double-vaccinated individuals, those who have designated risk conditions or are CEV account for 88% of severe cases and 77% of hospitalised cases.
In comparison with double-vaccinated individuals of the same age and sex without risk conditions, double-vaccinated CEV individuals remain at relatively high risk of severe disease or hospitalisation. For solid organ transplant recipients the rate ratio is of the order of 100-fold for severe disease, but even in this group the absolute risk of severe disease in the double-vaccinated is less than 1 in 1000 per month.
Strengths and limitations
Strengths of this study are the elimination of calendar time effects by the matched case-control design, the comprehensive linkage to e-health records and the focus on severe cases as main outcome measure. Hospitalised cases may include some test-positive individuals whose admission or continued stay in hospital was for another underlying diagnosis: this in turn may lead to underestimation of vaccine efficacy against COVID-19, especially in risk groups with comorbidities. Such misclassification is less likely to occur with the narrow definition of severe COVID-19 used in the REACT-SCOT study.
Even in this large cohort, the numbers of severe cases in some CEV subgroups are too small for vaccine efficacy against severe disease to be estimated accurately within these subgroups. Another limitation is that as most immunosuppressants and drugs for cancer are prescribed only in hospital and where prescribing records are not held in electronic form, we cannot study the relation of risk to different classes of immunosuppressant drugs. The national shielding list does not hold information about drug therapy or diagnoses other than the seven broad categories listed as CEV.
Relation to other studies
A recent report based on primary care data examined vaccine efficacy against symptomatic COVID-19 for which a medical consultation was recorded (8). For those who had been advised to shield, the efficacy after two doses of any vaccine was estimated as 87% (based on combining the age-stratified estimates). However without regular scheduled testing, estimation of vaccine efficacy against infection detected by testing is subject to ascertainment bias, and this problem is not entirely overcome by restricting to symptomatic cases or by test-negative case-control designs. This ascertainment bias is much less when the outcomes under study are severe or hospitalised disease.
Policy implications
CEV individuals should be advised that whilst the vaccines offer considerable protection residual risk remains relatively high in the CEV, and that they need to balance the adverse consequences of prolenged shielding against the ongoing risk of COVID-19. These results also support the policy of offering vaccination at a lower age threshold to those who share a household with a CEV individual. As in the general population, two doses are more effective than one in CEV individuals. It is thus plausible that an additional dose might give more protection to double-vaccinated individuals in this group; a risk score could be constructed to allow optimal targeting. For solid organ transplant recipients, passive immunization therapies may be an option now that they have been licensed in the UK for prevention in “those who have a medical condition making them unlikely to respond to or be protected by vaccination”. (9).
Data Availability
The component datasets used here are available via the Public Benefits and Privacy Panel for Health and Social Care at https://www.informationgovernance.scot.nhs.uk/pbpphsc/ for researchers who meet the criteria for access to confidential data. All source code used for derivation of variables, statistical analysis and generation of this manuscript is available on https://github.com/pmckeigue/covid-scotland_public.
Declarations
Public and Patient Involvement statement
This study was conducted under approvals from the Public Benefit and Privacy Panel for Health and Social Care which includes public and patient representatives.
Ethics approval
This study was performed within Public Health Scotland as part of its statutory duty to monitor and investigate public health problems. Under the UK Policy Framework for Health and Social Care Research set out by the NHS Health Research Authority, this does not fall within the definition of research and ethical review was therefore not required. Individual consent is not required for Public Health Scotland staff to process personal data to perform specific tasks in the public interest that fall within its statutory role. The statutory basis for this is set out in Public Health Scotland’s privacy notice.
Transparency declaration
PM as the manuscript’s guarantor affirms: that the manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as originally planned and registered have been explained. This manuscript has been generated directly from the source data by a reproducible research pipeline.
Funding
No specific funding was received for this study.
Data Availability
The component datasets used here are available via the Public Benefits and Privacy Panel for Health and Social Care at https://www.informationgovernance.scot.nhs.uk/pbpphsc/ for researchers who meet the criteria for access to confidential data. All source code used for derivation of variables, statistical analysis and generation of this manuscript is available on https://github.com/pmckeigue/covid-scotland_public.
Competing interest
All authors have completed and submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest.
Supplementary Material
Numbers of cases of hospitalized or fatal COVID-19 and matched controls, by risk group and vaccine product
Rate ratios for hopitalised or fatal COVID-19 within risk groups associated with vaccine dose: unvaccinated as reference category
Rate ratios for hospitalised or fatal COVID-19 associated with vaccine dose within clinically extremely vulnerable subgroups, with unvaccinated as reference category
Rate ratios for hospitalized or fatal COVID-19 within risk groups associated with vaccine dose by product within risk groups, with unvaccinated as reference category
Risk factors for hospitalised or fatal COVID-19 in those who had received 2 doses of vaccine at least 14 days before
Incidence of severe COVID-19 in clinically extremely vulnerable individuals who had received 2 doses of vaccine at least 14 days before, by risk subgroup
Acknowledgements
We thank Jen Bishop, Ciara Gribben and David Caldwell for undertaking the linkage analysis within Public Health Scotland,



