
ABSTRACT
Introduction Several case reports or small series have suggested a possible link between mRNA COVID vaccines and the subsequent development of myocarditis and pericarditis. This study is a prospective collection and review of all cases with a myocarditis/pericarditis diagnosis over a 2-month period at an academic medical center.
Methods Prospective case series from 1st June 2021 until 31st July 2021. Patients were identified by admission and discharge diagnoses which included myocarditis or pericarditis. Inclusion criteria: in receipt of mRNA vaccine within one month prior to presentation; The CMR protocol included cine imaging, native T1 and T2 mapping, late gadolinium enhancement and post contrast T1 mapping. All CMR studies were read in consensus by two experienced readers. Diagnosis was based on clinical presentation, ECG/echo findings and serial troponins and was confirmed in each case by CMR. Incidence was estimated from total doses of mRNA vaccine administered in the Ottawa region for the matching time-period. This data was obtained from the Public Health Agency of Ottawa.
Results 32 patients were identified over the period of interest. Eighteen patients were diagnosed with myocarditis; 12 with myopericarditis; and 2 with pericarditis alone. The median age was 33 years (18-65 years). The sex ratio was 2 females to 29 males. In 5 cases, symptoms developed after only a single dose of mRNA vaccine. In 27 patients, symptoms developed after their second dose of. Median time between vaccine dose and symptoms was 1.5 days (1-26 days). Chest pain was the commonest symptom, but many others were reported. Non-syncopal non-sustained ventricular tachycardia was seen in only a single case. Median LV ejection fraction (EF) was 57% (44-66%). Nine patients had an LVEF below the normal threshold of 55%. Incidence of myopericarditis overall was approximately 10 cases for every 10,000 inoculations.
Summary and Conclusions This is the largest series in the literature to clearly relate the temporal relationship between mRNA COVID vaccination, symptoms and CMR findings. In most patients, symptom onset began within the first few days after vaccination with corresponding abnormalities in biomarkers and on ECG. Cardiac MRI confirmed acute myocardial and pericardial changes with the presence of edema demonstrated with both tissue mapping and late gadolinium enhancement. Symptoms settled quickly with standard therapy and patients were discharged within a few days. No major adverse cardiac events and no significant arrythmias were noted during inpatient stay. Further follow up will be required to ascertain the longer-term outcomes of this patient group.
Introduction
At the end of May 2021, the World Health Organization (WHO) vaccine safety committee issued a statement of interest regarding reported cases of myocardial and/or pericardial inflammation occurring in patients subsequent to vaccination with COVID-19 mRNA vaccines(1). This followed a small number of reported cases from Israel and the United States(2–4). Data analyses in the US confirmed that the observed number of cases exceeded the expected number of cases in the 16-24 year-old age group. Cases appeared to be mainly in males and to develop shortly after the 2nd dose had been administered(5).
Although the Public Health Agency of Canada did not, initially, report higher rates of myocarditis compared to background historical trends, clinicians in our health region were aware of the phenomenon. A local task force was convened by Ottawa region cardiologists based at the 4 main admitting hospitals - and a decision taken to centralize admissions and investigations for post-vaccine inflammation at the University of Ottawa Heart Institute. This paper is a prospective case series describing clinical and cardiac MRI (CMR) findings over the first 2 months of this process.
Methods
Case selection
This was a prospective case series of all patients presenting to a single academic center with a suspected diagnosis of post vaccine myocarditis or pericarditis. The electronic health record was used to identify all patients with a compatible admission diagnosis between 1st June until 31st July 2021. All patients underwent echo, CMR and daily ECGs and Troponin. Dates and types of mRNA vaccine were recorded for each subject. Modified Lake Louise criteria(6) were used to make a diagnosis of myocarditis. Typical clinical and imaging findings were used to formulate a diagnosis of pericarditis.
Image acquisition
Cardiac MRI (CMR) was performed on a 1.5T unit (Siemens Aera, Siemens Healthineers, Erlangen, Germany) according to standardized protocols(7). The protocol included a) short axis steady state free precession (SSFP) cine imaging in short axis (slice thickness 8mm, gap 2mm) from base to apex; b) inline motion corrected native T1 and T2 maps in the short axis at basal, mid and apical levels as well as in the 3 and 4 chamber positions; c) dynamic resting perfusion; d) post contrast axial T1-VIBE images; e) post contrast SSFP single slice 2, 3 and 4 chamber cine imaging; f) single shot and segmented inversion recovery gradient echo late gadolinium enhancement (LGE) images 10 min-15 min after single-dose (0.1 mmol/kg) of macrocyclic Gadobutrol (Gadavist, Bayer Healthcare LLC); and g) post contrast T1 maps to match the native T1 slices.
Image processing
All CMR studies were reviewed and processed offline (cvi42, Circle Cardiovascular Imaging, Calgary). Ventricular volumes, mass and function were measured in conventional fashion. T1 and T2 maps were analyzed visually, with the aid of pixel-probing to determine absolute values. Formal segmental analysis was not performed, because of the issue of volume averaging small amounts of abnormal myocardium with large amounts of normal myocardium, thus risking a false negative report. Studies were reviewed by two experienced certified cardiologists or radiologists and a consensus sought on one of 4 possible final diagnoses: a) no evidence of myocardial or pericardial inflammation; b) myocarditis present; c) pericarditis present; d) myopericarditis present.
Public Health Data (Ottawa Region)
We collated data on all vaccinations performed in the Ottawa area relevant to the study period, provided by Public Health Ottawa. Data are publicly available for download at: https://open.ottawa.ca. We recorded all vaccinations given in the Ottawa area between 1st June and 31st July 2021. These data were used to provide a denominator to calculate incidence of myopericarditis.
Institutional Review Board (IRB)
This was an IRB-approved HIPPA/PHIPPA compliant study. The need for informed consent was waived by the IRB.
Results
Thirty-two patients were assessed over the study period (Table 1). and The median age was 33 years, 29 males, 3 females. Twenty-seven patients developed symptoms after their second vaccine dose, while 5 patients had received only a single dose at the time of presentation. Every patient had received at least one dose of an mRNA vaccine. The most common combination was Pfizer/Moderna followed by Moderna/Moderna. Only 2 patients received Astra Zeneca vaccine (both as the initial dose followed by a Moderna 2nd dose).
Clinical presentation
Time from last vaccination to presentation with symptoms was a median of 1.5 days (Table 1). A variety of symptoms were reported, with the commonest being chest pain, breathlessness, fever and chills (Figure 1). All patients were hemodynamically stable; no patient had an audible friction rub.

Initial investigations
Twenty-two patients had an abnormal ECG at presentation with the commonest abnormalities being diffuse ST segment elevation (STE) with PR depression (9 patients) and STE with T wave inversion (3 patients). Ten patients had a normal ECG at presentation. Biomarkers such as troponin, NTpro-BNP, CRP and ESR were uniformly mildly elevated at the time of presentation, although declined quickly during admission. No cases of COVID-19 were identified by PCR.
Cohort as a proportion of all COVID-19 doses of mRNA vaccine administered locally over the same timeframe
There were 15,997 doses of Moderna vaccine, and 16,382 doses of Pfizer vaccine administered over the study period, for a total of 32,379 doses. Note that these numbers represent a mixture of first and second doses. Therefore, if our cohort captured all cases in the Ottawa area, then the incidence of myocarditis would be 0.1% of all vaccine doses (32 cases/32,379 doses x 100), or 10 cases of myocarditis for every 10,000 doses of vaccine. The numbers by vaccine type are: 7 cases of myocarditis after a most recent dose of Pfizer vaccine compared to 16,382 doses administered, for an incidence of 0.04% or 4 cases per 10,000 inoculations. 25 cases of myocarditis occurred after a most recent dose of Moderna vaccine, compared to 15,997 doses administered, for an incidence of 0.16% or 16 cases of myocarditis per 10,000 inoculations. In the same time-period, 587 dose of Astra Zeneca vaccine were administered. We did not encounter any cases of myopericarditis where this vaccine was the proximate inoculate prior to symptomatic presentation.
In-hospital course
Thirty out of 32 patients were admitted to the hospital for observation with continuous telemetry and analgesia; 2 patients were followed closely as outpatients. Patients were discharged after resolution of symptoms and clear trend for Troponin improvement. Median hospital stay was 4 days. Since a distinction between pure myocarditis versus myopericarditis was not initially possible, most patients were empirically treated initially with high dose aspirin and colchicine, and symptoms resolved quickly in all cases. No patient required steroid or other immunosuppressive therapy. Two patients were in a stable atrial arrhythmia at presentation – one with pre-existing paroxysmal atrial flutter and the other with non-sustained atrial tachycardia which converted spontaneously. One patient experienced a single 11-beat run of asymptomatic self-terminating ventricular tachycardia during admission, but there were no other significant rhythm disturbances.
Imaging findings
No myocardial abnormalities were detected by in-patient echocardiography. Three patients had detectable pericardial effusion (1 trivial, 1 small, 1 moderate). On CMR isolated myocarditis was the commonest abnormality (18 patients), followed by myopericarditis (10 patients). The 2 patients with isolated pericarditis had normal myocardial appearances. All areas of the LV myocardium were affected, although the basal inferolateral wall was particularly commonly involved (Figures 2-4). One patient with isolated pericarditis had suggestion of early constriction with septal flattening, during deep inspiration, on real time cine imaging (Figure 5). No patient developed heart failure symptoms although just under one third of the cohort had mild LV dysfunction with an LVEF < 55% at CMR. Significant LV dysfunction was not seen however, with the lowest EF value being 44%.
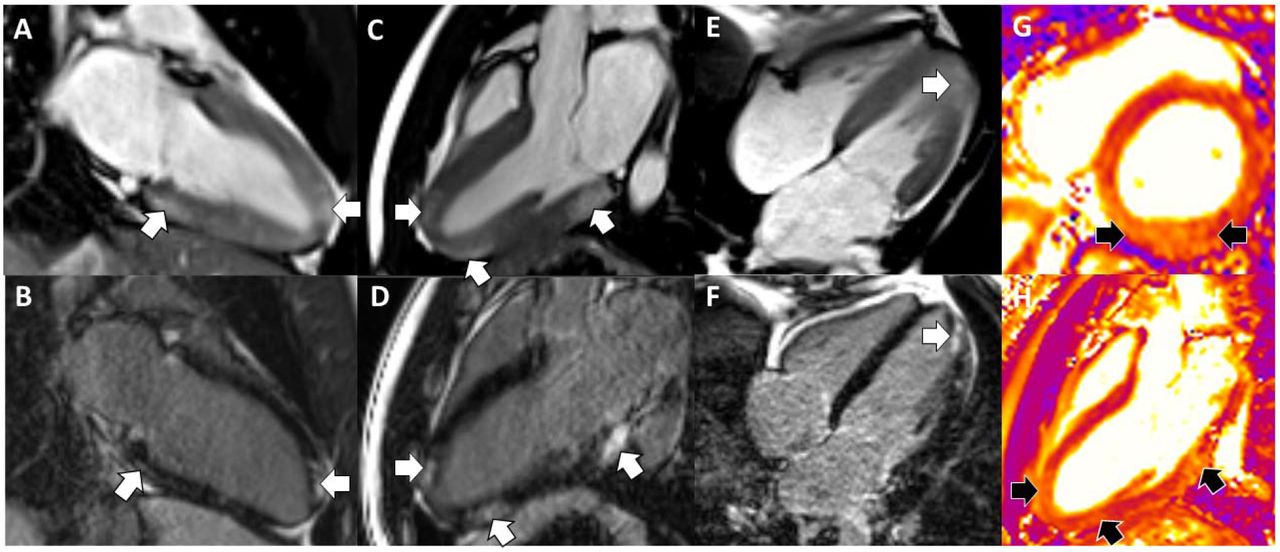
Matching pairs of post-contrast SSFP cine images (A,C,E) with accompanying LGE images (B, D, F) demonstrate multifocal areas of enhancement (white arrows), at several sites within the left ventricle. Native T2 maps (G, H) confirm the presence of edema (black arrows) at corresponding sites, indicative of an acute inflammatory response, with T2 values in excess of 70 milliseconds.

SSFP post contrast cine images (A), LGE images (B) and native T2 map (C) all show multifocal areas of edema (black arrows) and enhancement (white arrows) along the full length of the inferolateral wall.

SSFP (A, D), LGE (B, E) and native T2 maps (C, F) images demonstrate extensive edema (black arrows) and enhancement (white arrows) through the left ventricular myocardium. At presentation, the patient had a mildly reduced ejection fraction of 45%.
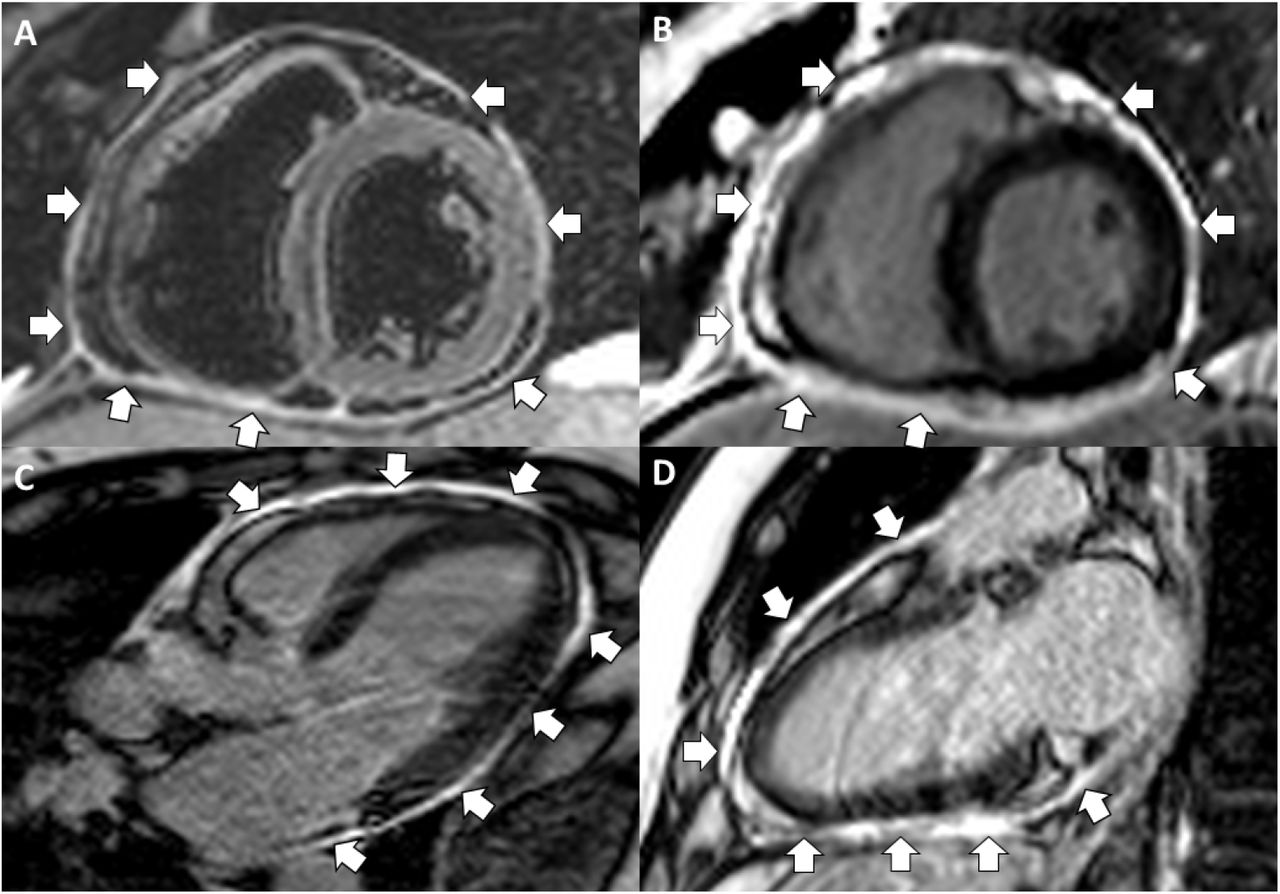
T2 weighted adiabatic inversion recovery images (A) reveal circumferential pericardial thickening with increased water signal (arrows). Late gadolinium enhancement images (B-D) demonstrate intense contrast enhancement (arrows). This patient also had evidence of mild septal flattening with inspiration, suggestive of early constrictive physiology.
Outcomes
Median in-patient length of stay was 4 days, with all patients asymptomatic at the time of discharge. There have been no re-admissions to date. Subsequent outpatient follow-up has not identified concerns, although repeat CMR - to ensure full resolution of tissue abnormalities - is outstanding in all our subjects.
Discussion
We report on 32 cases of consecutively presenting CMR-confirmed case myocarditis/pericarditis to an academic medical center following vaccination with one of two available COVID-19 mRNA vaccines. We believe that this is the largest series of patients with myocarditis (alone or myopericarditis) to date and the largest to report CMR findings, as well as the first report from Canada. The strengths of our series include central admission to the only cardiology center for a wide catchment area in a socialized health care system. As well as a clearly defined investigation protocol which included CMR imaging with tissue mapping in all cases. Our cases demonstrate a tight temporal association between receipt of mRNA vaccine and subsequent development of symptoms in a relatively short time frame afterwards. CMR was able to identify tissue level involvement in every case. Short term outcomes were good, with no clinically significant arrythmias in our cohort, despite mildly depressed LV function in one third of cases. There were no readmissions or deaths.
Myopericarditis is a recognized complication associated with numerous vaccines, in the United States accounting for 0.1% of all adverse reactions collected by the vaccine adverse effect reporting system (VAERS)(8). These reports, collected between 1990-2018, reveal that 79% of cases were in males and occurred mostly within 2 weeks of vaccination. An initial report from Israel in April 2021 highlighted an apparent sequential relationship between receipt of COVID-19 mRNA vaccine and myocarditis, most occurring in otherwise previously healthy young men and occurring with an incidence 5-25 times the usual background rate(9). The precise mechanism remains obscure and theories include a direct trophic effect of virus (though there are no reports of viral isolates from endomyocardial biopsy), and an exaggerated host immune response invoking both cytotoxic T cells in tandem with cytokine storm(10), despite engineered nucleoside modification designed to minimize this(11). As a result, both the Food and Drug Administration in the US, and the Public Health Agency of Canada have moved to add warning labels to Pfizer and Moderna mRNA vaccines highlighting the risk of inflammatory heart disease(12,13).
The true incidence of inflammatory heart disease following mRNA vaccine remains uncertain. A recent report from 40 hospitals in the same medical system and with a common electronic health record collated all cases of myopericarditis and compared to the underlying vaccination rate in the region(14), They estimated an incidence of 1 case of myocarditis in 100,000 vaccinations – and, separately, 1.8 cases of pericarditis per 100,000 vaccinations. That our data should suggest a tenfold higher incidence seems surprising. However, it is important to understand that the report of Diaz et al was essentially based upon the collection of administrative health data and not upon the direct investigation of patients with a protocolized approach, as we used in our study. For example, their case definition of myocarditis is not reported and whether a reference standard such as CMR was used to confirm a clinical suspicion is not discussed. Lack of direct myocardial assessment risks under-recognition of cases. The authors themselves raise this as a limitation of their study. Data from the Center for Disease Control (CDC) also report a lower incidence than that in our study. Using myocarditis cases reported to VAERS with onset within 7 days after dose 2 of an mRNA vaccine, crude reporting rates (i.e., using confirmed and unconfirmed cases) per million second dose recipients were calculated using national COVID-19 vaccine administration data as of June 11, 2021. The highest reporting rates were among males aged 12-17 years and those aged 18-24 years (62.8 and 50.5 reported myocarditis cases per million second doses of mRNA COVID-19 vaccine administered, respectively). We were not able to break down the denominator of all vaccinations in the Ottawa area by age. Therefore, although our patients were largely in the vulnerable 18-30 age category, our denominator included the full adult age spectrum. As such it is possible that the numbers, we quote are an underestimate of incidence for the 18-30 age group itself. In support of this, is the initial report from Israel of a 1 in 3000 to 1 in 6000 incidence of myocarditis following vaccination in young adults(9).
Most reports have emphasized mild illness and brief in-hospital stay – and this was our experience also. However, one of the larger cohorts to date described the need for heart failure treatment in 40% of its myocarditis patients (despite an absence of prior heart failure episodes) and intensive care in 10%(14). That report also demonstrated a clear uptrend in admission for both myocarditis and pericarditis, compared with data for the two prior years. A limitation of that work was the lack of any reported imaging (echo or CMR) and therefore some uncertainty regarding the accuracy of the final diagnosis. Although we did not encounter clinical heart failure, our series identifies a higher proportion of patients with abnormal LVEF than most other studies. This is most likely because decrements in function were generally mild and difficult to recognize by echo, but apparent when CMR was used in every case as it was here.
It is unclear whether prior COVID-19 infection (which may also cause myocarditis(15)), ‘primes’ the immune system for a more aggressive response following vaccination. Most reported cases had no prior COVID infection (true also in our series), although the report by Shaw et al of 4 patients included 2 with a definite prior COVID-19 diagnosis(16). Arrhythmia appears rare, even though ventricular arrhythmias were observed frequently in patients with COVID-19 and cardiac injury(17). Despite this only one case of paroxysmal VT was reported in the BNT162b2 (BioNTech Pfizer) vaccine trial(18), and only a single paroxysmal episode was seen in 1 patient in our cohort, who remained asymptomatic.
Where CMR was done in prior reports, the overwhelming diagnosis was that of myocarditis. Our cohort included many more cases which we interpreted as myopericarditis and this was generally in patients in whom there was clear edema and enhancement of pericardium overlying a myocarditic segment – in other words pericardial inflammation was an epiphenomenon of myocardial inflammation; this was also demonstrated in the case series from Starekova et al(19). True isolated diffuse pericarditis was rare in the literature and in our own cohort.
Study limitations
We acknowledge that association does not, by itself, provide evidence of causation - although the tight temporal coupling between vaccination and symptom onset represents a strong causal signal, also described in other reports. We do not yet have more than immediate short term outcome data. We quote calculated incidences of myocarditis per 10,000 inoculations but recognize that the public health data is imperfect and did not allow for distinction between first and second doses. We acknowledge that - despite central referral - our capture of cases may have been incomplete. Finally, we did not routinely test for other causes of myocarditis, as prior data suggested this would have been low yield(20).
Conclusion
Myocarditis appears to be an unpredictable and relatively infrequent side effect following vaccination with COVID-19 mRNA vaccines, is most common in younger males and appears to be self-limiting with supportive therapy. This is relevant to the ongoing public debate regarding proposals for vaccination of children under the age of 16, in whom the balance of benefit and risk may be more finely balanced(21). Our findings may also contribute to the debate regarding booster vaccine doses in those with prior documented myocarditis episodes. Ongoing monitoring using large scale national reporting systems is essential for both the prevalence and relevance of post-vaccine myocarditis to be truly understood.
Data Availability
Data is available from the corresponding author under reasonable request.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}