
Abstract
SARS-CoV-2 inactivated vaccines have shown remarkable efficacy in clinical trials, especially in reducing severe illness and casualty. However, the waning of humoral immunity over time has raised concern over the durability of immune memory following vaccination. Thus, we conducted a non-randomized trial among the healthcare professionals (HCWs) to investigate the long-term sustainability of SARS-CoV-2-specific B cells and T cells stimulated by inactivated vaccine and the potential need for a third booster dose for the HCWs. Although neutralizing antibodies elicited by the standard two-dose vaccination schedule dropped from a peak of 31.2 AU/ml to 9.2 AU/ml 5 months after the second vaccination, spike-specific memory B and T cells were still detectable, forming the basis for a quick recall response. As expected, the faded humoral immune response was vigorously elevated to 66.8 AU/ml by 7.2 folds 1 week after the third dose along with abundant spike-specific circulating follicular helper T cells in parallel. Meanwhile, spike-specific CD4+ and CD8+ T cells were also robustly elevated by 5.9 and 2.7 folds respectively. Robust expansion of memory pools by the third dose potentiated greater durability of protective immune responses. Another key finding in this trial was that HCWs with low serological response to 2 doses were not truly “no responders” but fully equipped with immune memory that could be quickly recalled by a third dose even 5 months after the second vaccination. Collectively, these data provide insights into the generation of long-term immunological memory by the inactivated vaccine, which has implications for future booster strategies that the frontline HCWs, individuals with low serological response to 2 dose of vaccine and immune compromised patients could benefit from a third dose of inactivated vaccine.
Introduction
The coronavirus disease 2019 (COVID-19), caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), continues to spread across the globe currently1, 2. The pandemic has brought profound casualties of human life and socioeconomic issues. The establishment of herd immunity by effective and sustainable vaccines represents the best strategy to prevent COVID-19. The rapid spreading of COVID-19 has urged the governments to authorize the emergent use of vaccines against SARS-CoV-23–5.
The presence of neutralizing antibodies (NAbs) against SARS-CoV-2 is an indicator of protective immunity after vaccination or infection6, 7. NAbs capable of blocking the interaction between the spike protein and its receptor angiotensin converting enzyme 2 (ACE2) are particularly important for protection from COVID-198. Therefore, inducing potent NAbs and long-lasting memory B cells are the primary goal of SARS-CoV-2 vaccines. Two doses of mRNA or inactivated vaccines are capable of inducing potent neutralizing antibody responses 3, 9, 10. Our previous study further demonstrated that inactivated vaccines elicited SARS-CoV-2 specific memory B cells11, which is important for a rapid and robust recall of protective responses against viral infection. However, little is known how long can these immune responses sustain. A rapid decline of neutralizing antibodies has been observed among infected healthcare workers (HCWs)12. Neutralizing antibodies also waned over time after the second dose of BNT162b2 or ChAdOx113, which indicates weakened protection from SARS-CoV-2 infection. In addition, the rapid emergence of novel SARS-CoV-2 variants of concern dampens the efficacy of SARS-CoV-2 vaccines, since vaccine-induced antibodies were always less effective in neutralizing emerging variants of concern (VOCs)14. Moreover, cross-reactive antibodies decayed even faster than antibodies against wild-type strain15.
Besides humoral immune responses, T cells also play a pivotal role in coordinating the adaptive immune responses and as effectors against viral infection. In some cases, patients with inherited or treatment-induced B cell deficiency were able to recover from COVID-1916, 17, suggesting a potential role of cellular responses in fighting against SARS-CoV-2 infection. Induction of CD8+ T cell responses was documented in both SARS-CoV-2 infection and vaccination18, 19. On the other hand, rapid induction of CD4+ T cells is associated with coordinated humoral and cellular response to a SARS-CoV-2 mRNA vaccine20. SARS-CoV-2 specific circulating TFH (cTFH) cells, whose counterparts in lymph nodes reinforce B cell differentiation and humoral response21, correlated with neutralizing antibody levels in convalescent COVID-19 patients22, 23.
Nevertheless, T cell responses induced by inactivated vaccines are much less well characterized than humoral immunity. One previous study revealed that the inactivated vaccine could elicit T cells response after 2 dose vaccination24, but the phenotype and sustainability of antigen-specific CD4+ and CD8+ T cells remained unclear yet.
In this study, we sought to investigate the sustainability of immune memory stimulated by the inactivated vaccine and profile humoral and cellular responses to a third dose among HCWs. Although NAbs declined substantially, SARS-CoV-2-specific memory B, CD4+, and CD8+ T cells persisted in the peripheral blood 5 months after the second vaccination, even in participants who were seronegative after 2 doses of the inactivated vaccines. The third vaccination robustly recalled both humoral and cellular immune responses in all participants.
Materials and methods
Human subjects
In this study, we conducted a non-randomized trial and recruited participants from a prospective cohort at the First Affiliated Hospital of Sun Yat-sen University (FAH-SYSU) in Guangzhou, China. As we described previously11, 63 HCWs received the inactivated SARS-CoV-2 vaccine BBIBP-CorV (BBIBP-CorV, Sinopharm, Beijing) in the morning (9am-11am) or afternoon (15pm-17pm) on day (d) 0 and d28, respectively. Fifty of the 63 HCWs were volunteered to receive a third booster shot of the inactivated vaccine 6 months after the prime vaccination (d180). They were assigned to the morning or afternoon group as to their previous vaccinating time accordingly. Demographic characteristics of the HCWs were summarized in S. Table 1. Blood samples were collected on d180 before the booster dose and d187, d194 and d208 after the booster dose. Convalescent patients who had recovered from SARS-CoV-2 infection were recruited as the positive control (S Table 2). All studies were approved by the Institutional Review Board of FAH-SYSU and written consent was obtained from all participants. The prospective cohort and the trial were registered to Chinese Clinical Trial Registry (ChiCTR2100042222 and ChiCTR2100048665).
Cell isolation
Blood samples were collected into the heparinized tubes and processed right after sample collection. Peripheral blood mononuclear cells (PBMCs) were isolated using density-gradient centrifugation. Briefly, blood samples were diluted with PBS at 1:1 ratio and loaded on top of Lymphoprep™ (StemCell) in the Falcon tubes. The falcon tubes were then centrifuged at 1500 rpm for 30 mins. The medium layer was collected and washed with PBS twice. PBMCs were cryopreserved in Bambanker (StemCell) immediately.
SARS-CoV-2 neutralizing antibodies measurement
A one-step competitive immunoassay was used to detect the serum concentration of neutralizing antibodies (NAbs) for SARS-CoV-2 in the sera through Chemiluminescent immunoassay using iFlash 2019-nCoV NAb kit (YHLO Biotech Co, Ltd). As for this assay, receptor binding domain (RBD) of the SARS-CoV-2 was coated on magnetic beads. Acridinium ester-labeled ACE2 was designed to compete with SARS-CoV-2 NAbs in the sera for the RBD. SARS-CoV-2 NAb titers were calculated by an iFlash3000 Chemiluminescence Immunoassay Analyzer (YHLO Biotech Co, Ltd). The surrogate neutralization assay detects antibodies that are able to compete with the binding of the extracellular domain of the SARS-CoV-2 receptor ACE2 to a recombinant RBD of the SARS-CoV-2 S1 protein coated on the microparticles, which indicates the neutralization activity of sera as tested before25. Neutralizing activity is determined in arbitrary units (AU) and the cut-off is 10 AU/ml.
Ex vivo ELISpot assay
IFN-γ ELISpot assays were performed as described previously26. Briefly, 100 μl of the coating antibody (15 μg/ml, MabTech, #3420-3-250) was added to the well of ELISpot plate (MabTech) and incubated overnight at 4°C. The peptide pool of SARS-CoV-2 spike protein (MabTech, #3630-1) was added to 300,000 PBMCs per test at a final concentration of 2 g/ml for 24 μh.
Unstimulated cells were used as negative control while anti-CD3/CD28 dynabeads (Thermo Fisher) stimulated cells were set as the positive control. Plates were incubated with IFN-γ detection antibody (1μg/ml, MabTech, #3420-6-250), followed by Avidin-HRP (1μg/ml, Vector, #A-2004-5) and visualized using the ACE substrate. Antigen-specific T cell responses were quantified by subtracting the number of spots in unstimulated cells from the peptide stimulated cells.
SARS-CoV-2-specific B cell ELISpot was performed as previously described27. Briefly, ELISpot plates were coated with 10ug/ml recombinant RBD protein (Sino Biological, #40592-VNAH-100) and 8ug/ml spike protein (Sino Biological, #40589-V08B1) overnight at 4°C. To optimize the human IgG B cell ELISpot assay, PBMCs were cultured with a mixture of R848 (1 μ ml, Tocris, #4536/10) and IL-2 (20 ng/ml, PeproTech, #200-02-10) for 3 days to secrete a detectable amount of antibody28, 29. After pre-stimulation, cells were washed extensively to remove secreted antibodies. 500,000 PBMCs were added to the coated plates and incubated for 18 h at 37°C with 5% CO2. The following day, cells were removed and plates were incubated with Biotin-anti-Human IgG (1μg/ml, Jackson ImmunoResearch, #709-065-098).
Plates were then incubated with Avidin-HRP followed by visualization with ACE substrate. ELISpot plates were analyzed using an ELISpot counter (Cellular Technologies Ltd). Results were expressed as spot-forming units (s.f.u.) per 106 PBMCs. Responses were considered positive if the results were at least three times the mean of the negative control wells and >25 s.f.u. per 106 PBMCs. Data were excluded when negative control wells had >30 s.f.u. per 106 PBMCs or positive control wells (anti-CD3/CD28 dynabeads) were negative.
Activation-induced markers (AIM) T cell assay
PBMCs were cultured in RPMI 1640 supplemented with 10% FBS and 1% penicillin and streptomycin (Thermo Fisher) at 37 °C overnight. The cells were then cultured with or without the peptide pool of SARS-CoV-2 spike protein (2 μg/mL) for 12 h. An equal concentration of DMSO in PBS was used as the negative control. Antigen-specific T cells were measured as a percentage of AIM+ (OX40+CD137+) for CD4+ T or (CD69+CD137+) for CD8+ T cells after stimulation of PBMCs with the peptide pool of spike protein26. After the stimulation, cells were first stained with Zombie Red for dead cell exclusion. Cells were then stained with anti-CD3-Pacific blue, anti-CD4-BV510, anti-CD8-Percp, anti-CD69-Super Bright 436, anti-CD134 (OX40)-BV605 and anti-CD137-(4-1BB)-PE antibodies for antigen-specific T cell analysis. As for phenotype analysis of SARS-CoV-2-specific T cells, cells were further labeled with anti-CCR7-APC/cy7, anti-CD45RA-BV650, anti-CXCR5-BV711 and anti-PD-1-PE/cy7 antibodies. All FACS antibodies were from Biolegend. Stimulation with anti-CD3/CD28 dynabeads was included as positive controls. Any sample with a low response to anti-CD3/CD28 stimulation was excluded as a quality control for the samples. Data were acquired by flow cytometry.
Detection of SARS-CoV-2-specific memory B cells
SARS-CoV-2-specific memory B cells were detected as we described previously11. First, biotinylated antigens were multimerized with fluorescence labeled streptavidin individually. Recombinant spike protein (R&D, #BT10549-050) was mixed with BV510-streptavidin (BioLegend) at 10:1 ratio and BV785-streptavidin (BioLegend) at 18:1 ratio at 4°C for 1h. Recombinant RBD protein (R&D, #BT10500-050) was mixed with BV421-streptavidin (BioLegend) at 20:1 ratio at 4°C for 1h. The antigen probes prepared above were then mixed in 50mM free d-biotin (Macklin) in PBS to ensure minimal cross-reactivity. PBMCs were thawed and let to rest at 37°C with 5% CO2 for 2h and stained with Zombie Red (BioLegend) in PBS at room temperature for 20min. Cells were then stained with 50 μl of antigen probe cocktail containing 100 ng of spike and 50 ng of RBD at 4°C for 30 min. Cells were washed with PBS and then stained with the following antibody cocktail: anti-CD3-Pacific Blue™, anti-CD19-PE-CY7, anti-CD27-AF700, anti-IgD-FITC, anti-CD38-BV650, anti-IgM-BV605, anti-IgG-AF647, anti-IgA-PE all from BioLegend at 1:100 dilution. Samples were acquired by flow cytometry.
Flow cytometry
All flow cytometry samples were analyzed using cryopreserved cells which were thawed and suspended in RPMI 1640 media supplemented with 2% FBS. All samples were analyzed by flow cytometry with CytekTM AURORA. FlowJo (Tree Star, USA) software was used for FACS data analysis. Details of antibodies used in this study are listed in S.Table. 3.
ELISA-based antibody-antigen distribution analysis
SARS-CoV-2 proteins were purchased from Sino Biological (Beijing, China). 40ng/well of SARS-CoV-2 spike (40589-V08B1), spike S1 subunit (40591-V08H), spike NTD (40591-V49H), spike S2 subunit (40590-V08B), RBD (40592-V08H), RBD T478K (40592-V08H91), nucleocapsid (40588-V08B) and envelope (40609-V10E3) were coated on the 96-well ELISA plate (655061, Greiner Bio-one) overnight at 4 ℃, respectively. Plates were washed by PBS supplemented with 0.05% Tween-20 (PBST) three times, followed by blocking with 5%BSA in PBST for 1 hour at room temperature. Human serum was diluted 20-fold for the first well and 4-fold serial diluted for subsequent wells in 5%BSA in PBST, and 100 μl/well was subjected to the coated ELISA plated for the incubation at 4℃ overnight.
Plates were washed 3 times by PBST, processed to 100 μl/well goat HRP conjugated anti-human IgG antibody (2040-05, SouthernBiotech) at 1:3000 dilution in PBST for staining in 30 minutes at room temperature. Plates were washed five times with PBST. 100 μl/well 3,3,5,5-Tetramethylbenzidine substrate (P0209, Beyotime) was added to each well for 15 minutes reaction, and stopped by adding 50μ well stopping buffer (C1058, Solarbio). OD450nm absorbance was measured by Varioskan Lux Microplate Reader (Thermo Fisher).
Statistical analysis
Statistical analysis was performed using Prism 5.0. Comparisons were assessed using Wilcoxon rank sum test, Student’s t-test, paired Student’s t-test or One-way ANOVA followed by Bonferroni’s multiple comparison post-test as appropriate. P values < 0.05 were considered as statistically significant.
Results
Neutralizing antibody response is enhanced by a third dose of inactivated SARS-CoV-2 vaccine BBIBP-CorV
To investigate the immune response and the subsequent duration of immune protection by the inactivated SARS-CoV-2 vaccine BBIBP-CorV, we conducted a non-randomized trial and recruited HCWs from a prospective cohort. Fifty HCWs from this cohort were volunteered to participate in this non-randomized trial. They were assigned to receive a third dose of the inactivated vaccine 6 months after the primary vaccination (Fig. 1A). No severe side effects related to vaccination were recorded during the trial (S. Table 1). Among the 50 participants, 36 of them were tested negative for neutralizing activities by Chemiluminescent immunoassay 6 months after the primary vaccination. Nine HCWs who were seronegative on d56 after two doses of vaccine remained to be negative and 27 of the positive HCWs turned negative. Of the 9 negative HCWs, 7 of them were from the afternoon group and 2 were from the morning group. The average concentration of NAbs dropped by 70% from d56 to d180 (Fig. 1B). Consistent with our previous study11, stronger NAbs was maintained in the morning vaccination group when compared to the afternoon group after 6 months.

(A) Protocol of the prospective cohort and the non-randomized trial. Healthcare workers (HCWs) were recruited from a perspective cohort who received two doses of an inactivated vaccine either in the morning (n=25) or afternoon (n=25) on day d 0 and d28. They were assigned to morning or afternoon vaccination to receive a third dose of the inactivated vaccine on day 180 according to their previous vaccinating time. Blood samples were collected on different time points d0 (T1), d14 (T2), d21 (T3), d28 (T4), d56 (T5), d180 (T6), d187 (T7), d194 (T8) and d208 (T9). (B-E) Neutralizing antibodies (NAbs) against SARS-CoV-2 in the serum of each volunteer was measured by Chemifluorescence Assay longitudinally. The concentration of NAbs in the sera at different time points was summarized and shown in the box plot (B). The longitudinal changes of NAbs in the sera before and after the third dose of vaccination (C). NAbs concentrations in the sera from the morning or afternoon group at different time points before and after the third dose of vaccine. Data were summarized and shown as dot plot (D). NAbs concentrations in the sera of female or male at different time points before and after the third dose of vaccination were summarized and shown as dot plot (E). Medians of the data were shown. **p<0.01, ****p<0.0001. Comparisons were done by Wilcoxon rank sum test. Ns: not significant.
Blood samples were collected from multiple time points before and after the third dose of vaccine longitudinally and NAbs was measured by Chemiluminescent immunoassay. We found that serological response was induced within 1 week after the boost dose. The concentration of NAbs was increased by 7.2 folds from 9.3 AU/ml on d180 to 66.9 AU/ml on d187. The concentration of NAbs continued to rise and reach the peak by 10.6 folds at around 2 weeks after the booster shot (Fig. 1C). The enhanced neutralizing antibody response was still observed at the early response after the third dose. There was a trend that the morning group benefited more from the vaccination. The difference between the two groups diminished over time (Fig. 1D). However, we did not observe different levels of NAbs between female and male (Fig. 1E).
To further profile the antibody spectrum induced by the inactivated vaccin, we measured antibodies against SARS-CoV-2 nucleocapsid, spike, spike S1, spike S2, RBD, spike N terminal domain (NTD) and envelope in the serum samples from d194 by ELISA. Supprisingly, antibodies against against these SARS-CoV-2 structure proteins were detected in all of the HCWs (S. Fig. 1). In addition to spike-targeted antibodies, inactivated vaccine is capable of inducing a broad specturm of antibodies against SARS-CoV-2 and might provide greater protection than expected.
SARS-CoV-2 specific memory B cell response is robustly induced by a third dose of inactivated vaccine BBIBP-CorV
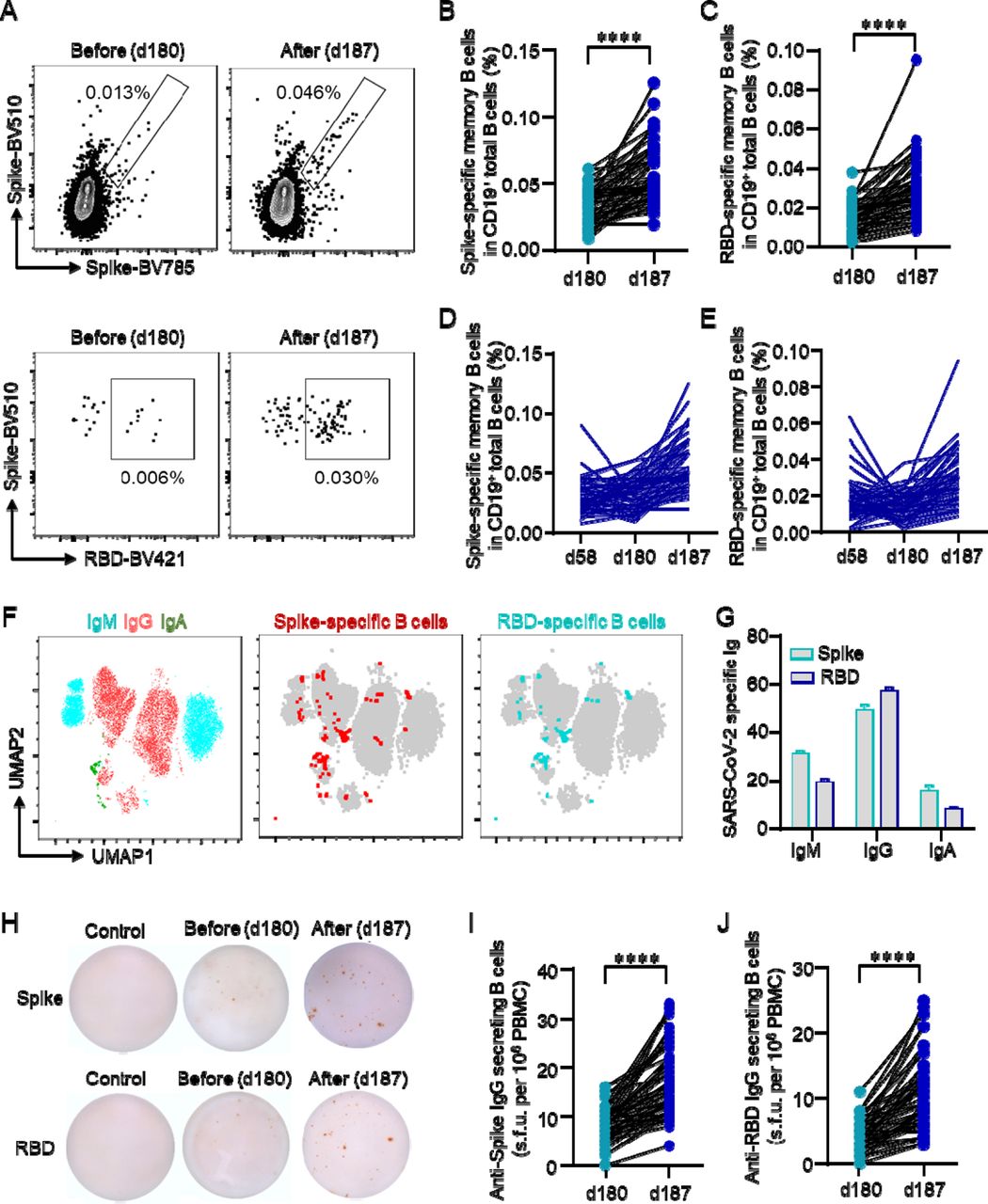
Antigen-specific memory B cells play an important role in the recall response upon reinfection or boost by vaccination. To study the durability of SARS-CoV-2-specific memory B cells and their response to the booster vaccine, we first measured spike- and RBD-specific B cells by flow cytometry. We found that spike- and RBD-specific memory B cells were detected 6 months after vaccination. The percentages of spike- and RBD-specific memory B cells were increased by 1.7 and 2 folds respectively by the third dose of vaccine (Fig. 2A-2C). As compared to data on d56, there was a decreasing trend for the percentage SARS-CoV-2-specific memory B cells over time. However, the percentage viral specific memory B cells were largely maintained on d180 (Fig. 2D, 2E). As for the spike- and RBD-specific memory B cells, the majority of the cells could be mapped into IgG+ or IgM+ B cells. IgA+ B cells accounted for a minimal percentage of these SARS-CoV-2-specific memory B cells (Fig. 2F, 2G). Spike- or RBD-specific memory B cells were further detected by ELISpot and similar results were found. The third dose inactivated vaccine boosted spike- or RBD-specific memory B cells from 8 u.f.c/106 PBMCs to 17 u.f.c/106 PBMCs and 4 u.f.c/106 PBMCs to 10.7 u.f.c/106 PBMCs respectively as by ELISpot (Fig. 2H-2J). As we phenotyping the total B cell population by flow cytometry, we found that percentage of total and naïve B cells were not affected by the third dose of vaccine. Double negative (IgD-CD27-) B cells were increased. However, IgG+ B cells remained unchanged after the booster dose (S. Fig. 2, 3).

Study was carried out as in Fig. 1. (A) Recombinant spike or receptor binding domain (RBD) proteins were used to label SARS-CoV-2-specific BCR. Data were acquired by flow cytometry. Representative FACS plots for spike- or RBD-specific BCR were shown. (B, C) Percentages of spike- or RBD-specific memory B cells among total B cells were summarized and shown as line graph. (D, E) Longitudinal changes of spike- or RBD-specific memory B cells as measured by flow cytometry. (F) IgG+, IgA+ and IgM+ B cells were measured by flow cytometry. UMAP plot demonstrated the distribution of spike- and RBD-specific memory B cells in IgG+, IgA+ and IgM+ B cells. (G) Distribution of spike- and RBD-specific immunoglobulins (Ig). (H) PBMCs were incubated in spike- or RBD-coated ELISpot 96-well plates for 18 h. Anti-spike or anti-RBD IgG-secreting B cells were measured by ELISpot. Representative ELISpot images were shown. (I, J) Numbers of anti-spike or anti-RBD IgG-secreting B cells in 106 PBMCs. ****p<0.0001. Comparisons were done by Student’s paired-T test.
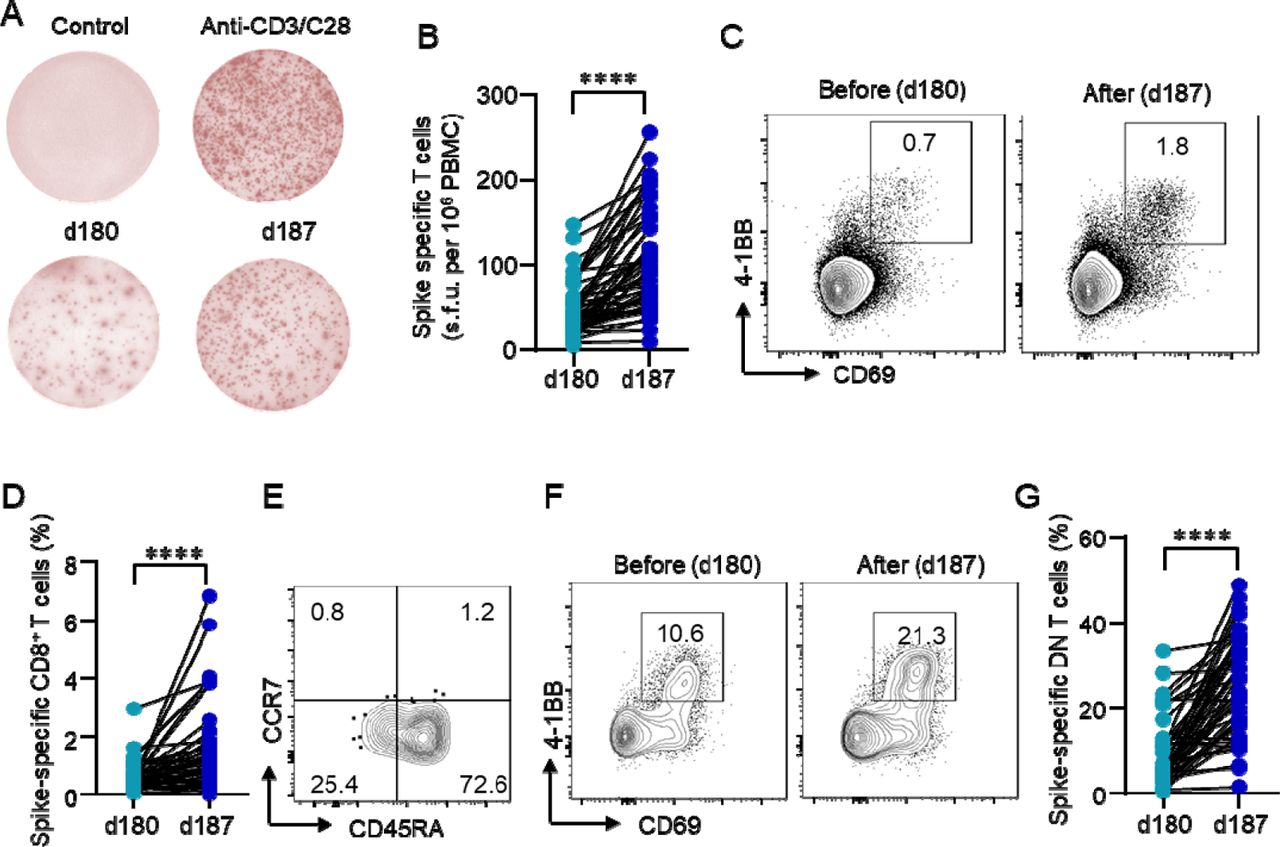
A PBMCs were stimulated with or without the spike peptide pool (2 μg/ml). Anti-CD3/CD28 dynabeads were used as positive control. IFN-γ producing T cells were detected by ELISpot after 24 h incubation. Representative images of ELISpot wells were shown. (B) The number of IFN-γ-producing T cells was quantified by calculating the spot-forming units (s.f.u.). Data were shown as line graph. (C-G) PBMCs were stimulated with spike peptide pool (2 g/ml) for 12 h. Activation-induced markers (AIM) CD69 μ and 4-1BB were measured by flow by flow cytometry. (C, D) Representative FACS plots showing the SARS-CoV-2-specific AIM+ CD8+ T cells. Percentages of AIM+ CD8+ T cells were summarized. (E) The distribution of AIM+ CD8+ T cells across TN (CD45RA+CCR7+), TEM (CD45RA-CCR7-), TCM (CD45RA-CCR7+), TERMA (CD45RA+CCR7-). (F, G) Activation of CD3+CD4-CD8- T cells as stimulated by spike peptide pool was quantified for the expression of CD69 and 4-1BB. ****p<0.0001. Comparisons were done by Student’s paired-T test.
The cellular response is boosted by a third dose of inactivated SARS-CoV-2 vaccine BBIBP-CorV
Although there was a short report showing T cell responses to SARS-CoV-2 antigens after 2 doses of the inactivated vaccine24, it is not clear how long they sustain. Blood samples were acquired from the participants 6 months after the primary vaccination and cellular response was first measured by IFN-γ ELISpot using the spike peptide pool. As expected, antigen-specific T cells were recorded in all of the participants, although low frequencies were detected in some of the participants. However, the SARS-CoV-2-specific CD8+ T cells could be potentially underestimated for the use of the spike peptide pool alone. T cell response was enhanced by a third dose vaccine by 2.3 folds as measured by ELISpot (Fig. 3A, 3B). Further, SARS-CoV-2-specific CD8+ T cells (CD69+4-1BB+) were robustly primed following the booster shot 2.7 folds (Fig. 3C, 3D). Phenotypic markers indicated that the majority of the SARS-CoV-2-specific memory CD8+ T cells were CD45RA+CCR7- terminally differentiated effector memory cells (TEMRA). CD45RA-CCR7- effector memory T cells (TEM) accounted for only one-fourth of the total antigen-specific CD8+ T cells (Fig. 3E), which is similar to that from recovered COVID-19 patients26. However, the subsets of total CD8+ T cells were not affected (S.Fig. 4, 5). We also detected SARS-CoV-2-specific CD3+CD4-CD8- T cells in inactivated SARS-CoV-2 vaccinated individuals, which were further induced to a greater extent when compared to CD8+ T cells by the booster shot (Fig. 3F, 3G). The induction of CD3+CD4-CD8- T cells might be correlated with vaccine efficacy30.

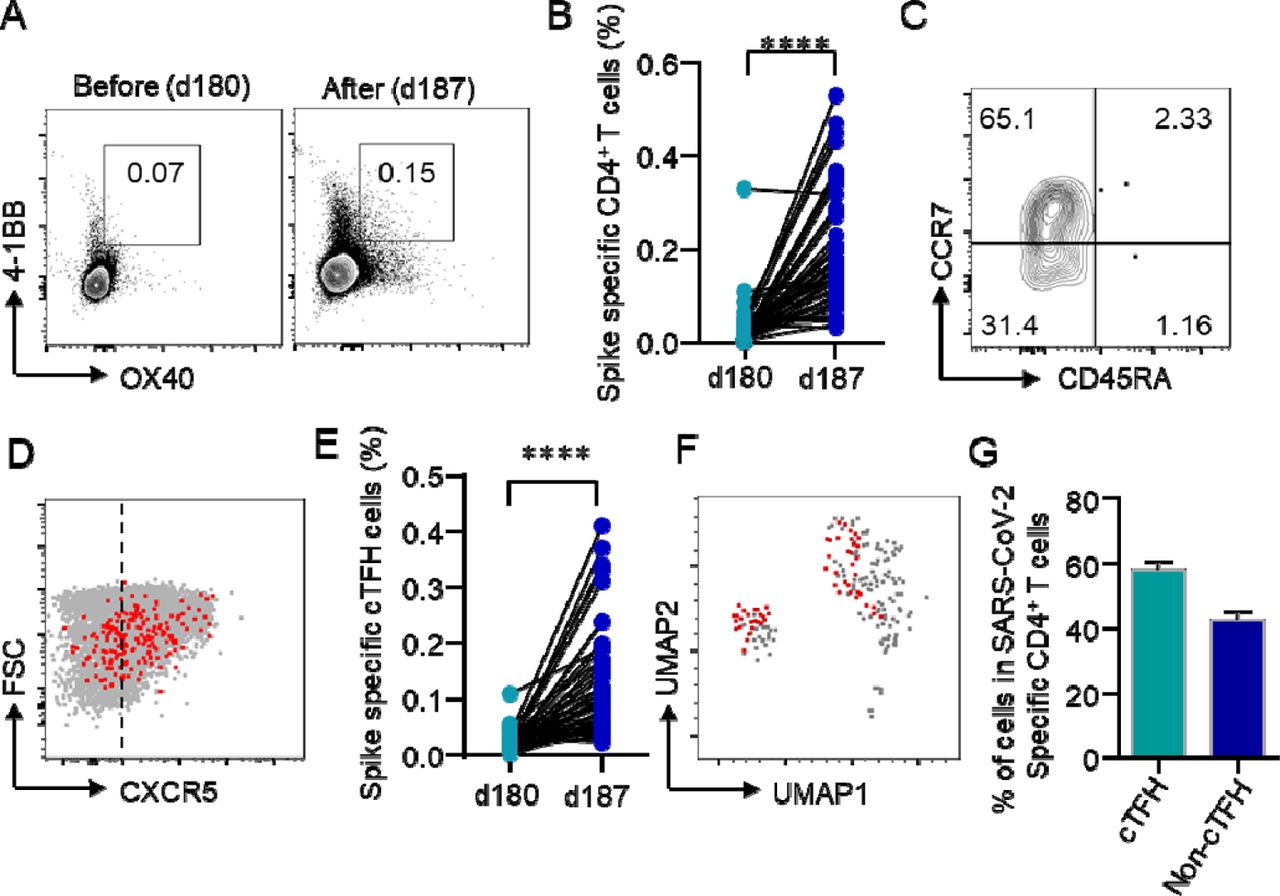
(A, B) Activation-induced markers (AIM) OX40 and 4-1BB in CD4+ T cells were detected flow cytometry after incubation PBMCs with spike peptide pool (1μg/ml) for 12 h. AIM+ CD4+ T cells were quantified by summarizing the percentages of AIM+ CD4+ T cells in the PBMCs. (C) The distribution of AIM+ CD4+ T cells across TN (CD45RA+CCR7+), TEM (CD45RA-CCR7-), TCM (CD45RA-CCR7+), TERMA (CD45RA+CCR7-). (D) Expression of CXCR5 among AIM+ CD4+ T cells was measured by flow cytometry. Representative FACS plot showed CXCR5 expression in AIM+ CD4+ T cells. (E) Percentage of circulation follicular helper T cells (cTFH) in total CD4+ T cells were summarized. (F) UMAP plot showed the distribution of cTFH cells among AIM+ CD4+ T cells. (G) Percentage of cTFH cells in AIM+ CD4+ T cells. ****p<0.0001. Caparisons were done by Student’s paired-T test.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Neutralizing antibodies (NAbs) in the sera were measured as in Fig. 1. The concentration of NAbs was analyzed longitudinally at different time points before and after the third dose of vaccination. The red arrow indicates the timing of the third dose vaccination. (B) Comparison of NAbs response to the third dose of the inactivated vaccine between previous negative and positive serological response to two doses. (C-J) Blood samples were collected on day (d) 180, d187, d194, d201 and analyzed longitudinally. (C) Spike-specific BCR was detected by flow cytometry. (D) Spike- or RBD-specific BCR was measured by ELISpot after incubation of PBMCs with spike- or RBD-coated plates for 18 h. Anti-spike and anti-RBD IgG-secreting B cells were quantified and summarized in E and F. (G) IFN-γ producing T cells were detected by ELISpot. PBMCs were incubated with spike peptide pool at 2 μg for 24 h and spot-forming unites (s.f.u) were quantified. (H-J) Spike-specific CD8+, CD4+ and circulating follicular T cells (cTFH) were measured by flow cytometry after incubating cells with spike peptide pool at 2 μg/ml for 12 h. Activation of CD8+ T cells (CD69+4-1BB+), CD4+ T cells (OX40+4-1BB+), and cTFH cells (CXCR5+OX40+4-1BB+) were summarized. *p<0.05, **p<0.01, ****p<0.0001. Comparisons were done by Wilcoxon rank sum test in B and One-way ANOVA corrected for multiple comparison in C, E-J. ns: not significant
SARS-CoV-2-specific CD4+ T cells are enhanced by a third dose of inactivated SARS-CoV-2 vaccine BBIBP-CorV
There is limited knowledge regarding the induction of SARS-CoV-2-specific CD4+ T cells by the inactivated vaccine. We detected SARS-CoV-2-specific CD4+ T cells by stimulated cells with the spike peptide pool and measured the activated CD4+ T cells (OX40+4-1BB+) by flow cytometry. Spike-specific CD4+ T cells were detected at a low level on d180 before the booster shot. The third dose induced the expansion of SARS-CoV-2-specific CD4+ T cells by 5.9 folds rapidly within 1 week (Fig. 4A, 4B). Phenotypic analysis showed that the majority of the SARS-CoV-2-specific CD4+ T cells were CD45RA-CCR7+ TCM and CD45RA-CCR7- TEM, which was different from that of SARS-CoV-2-specific CD8+ T cells (Fig. 4C). Among spike-specific CD4+ T cells, 57.7% of the cells were CXCR5+ cTFH cells (Fig. 4D-4G), indicating an important role of TFH cells in the induction of immune protection by inactivated vaccination. Among total CD4+ T cells, we observed the slightly decreased TN cells, with increased TEM and TCM cells in the peripheral blood (S. Fig. 4, 5).
A third dose of inactivated SARS-CoV-2 vaccine BBIBP-CorV boosts immune responses in individuals with negative serologic response to 2 doses
The weakened or negative serological response has been noted in immune-compromised individuals after vaccination or SARS-CoV-2 infection. The third dose of mRNA vaccine could help to enhance immune responses in these patients31, 32. Consistent with these studies, we found that NAb was detected in all of the 9 participants with a negative serological response after 2 doses of vaccine. The level of NAb in all of the 9 participants increased rapidly within 1 week and reach the peak 2 weeks after the booster shot (Fig. 5A). However, the serological response was boosted to a less extent when compared to the participants with seropositive response to 2 doses of vaccine (Fig. 5B). Surprisingly, SARS-CoV-2-specific memory B cells were detected in these seronegative individuals 6 months after the primary vaccination, which was expanded by the third dose of vaccine (Fig. 5C). To further explore SARS-CoV-2-specific memory B cell and T cell response to the third dose of vaccine, we collected longitudinal PBMCs samples from each individual from 4 time points: baseline, 1 week post the booster shot, 2 weeks post booster shot and 4 weeks post booster shot. In consistent with the NAb data, Spike- or RBD-specific memory B cells were detected at a low level by ELISpot using recombinant spike and RBD proteins. The number of anti-spike and anti-RBD IgG-producing B cells were increased within 1 week and continue to rise up to a less extent 2 weeks after the booster shot (Fig. 5D-5F).
Next, we were to investigate T cell responses to the booster dose in seronegative individuals after 2 doses of vaccine. Interestingly, spike-specific T cells were detected even before the third dose of vaccine as measured by ELISpot. The third dose of vaccine enhanced SARS-CoV-2-specific T cell response consistently (Fig. 5G). The induction of SARS-CoV-2-specific CD4+ and CD8+ T cells by the third dose of vaccine was further confirmed by measuring AIM+ T cells (OX40+4-1BB+ for CD4+ T cells and CD69+4-1BB+ for CD8+ T cells) by flow cytometry. Both spike-specific CD4+ T cells and CD8+ T cells were expanded by the third dose of vaccine (Fig. 5H, 5I). We also observed the expansion of SARS-CoV-2-specific cTFH cells by the third dose of vaccine (Fig. 5J). Taken together, a third dose of inactivated SARS-CoV-2 vaccine could induce detected B cell and T cell response in individuals with negative serological response to 2 doses of vaccine.
Discussion
In this study, we investigated the duration of B cell and T cell immunity and their response to a third dose of the inactivated SARS-CoV-2 vaccine BBIBP-CorV in a non-randomized trial. Data in this study showed that neutralizing antibodies gradually decreased after the second dose of vaccine during the 6-month observation. SARS-CoV-2-specific B cells and T cells were detected and persisted in the peripheral blood 6 months after the primary vaccination. Both humoral and cellular responses were induced by the third dose of inactivated SARS-CoV-2 vaccine robustly and rapidly. The generation of SARS-CoV-2-specific B cells and T cells by the inactivated vaccine could be key for developing durable protection, as has been shown in mRNA vaccine and other settings33, 34. Another key observation in this study was the induction of antigen-specific B cell and T cell response in HCWs with low serological response to 2 doses of inactivation vaccines.
The neutralizing antibody titers have been noted to decay following vaccination or SARS-CoV-2 infection35–37. However, HCWs who have recovered from COVID-19 show a substantially lower risk of reinfection with SARS-CoV-238. The study shows that the number of RBD-specific memory B cells remain relatively stable between 6 and 12 months after SARS-CoV-2 infection and BCR repertoire expand markedly in these recovered COVID-19 patients after mRNA vaccination39. Consistently, spike- and RBD–specific memory B cells can still be detected all the COVID-19 convalescent patients up to 13 months after infection as shown in this study (S. Figure 6). It is also worth noted that SARS-CoV-2 infection induces long-lived plasma cells in the bone marrow of individuals who have recovered from COVID-19. SARS-CoV-2 mRNA vaccines induce sustained immune memory and long-term protecting effects33, 40, 41. As for inactivated vaccines, the levels of NAbs wane over time, which is in accordance with our data in this study.
Recently, a third dose of inactivated vaccine CoronaVac elicited a rapid and long-lasting recall antibody response with the capability of neutralizing several VOCs42. The rapid and strong secondary response by the inactivated vaccine represents a characteristic secondary immune response, which demonstrates the establishment of long-term immune memory within these participants. Our further data confirms that SARS-CoV-2-specific memory B cells persisted 6 months later the primary vaccination and expanded substantially by the third dose of vaccine. The secondary immune response is one of the most important features of immune memory as stimulated by vaccination, which is characterized by a faster and stronger immune response by memory B cells or plasma cells43. Despite the waning of antibodies, the generation of SARS-CoV-2-specific memory B cells could mediate recall response in future infection and provide protecting immunity. As has been observed in recovered COVID-19 patients, long-lived bone marrow spike-binding plasma cells are quiescent27, which explains the declining antibodies over time. Nonetheless, further investigation should be carried out on how waning immunity could affect protection against COVID-19.
SARS-CoV-2-specific CD4+ and CD8+ T cells in convalescent COVID-19 patients could be long-lasting up to 13 months as have been documented in this study (S. Fig. 7). SARS-CoV-2-specific CD4+ and CD8+ T cells induced by BBIBP-CorV were detected in all the HCWs who received 2 doses of vaccine, and that last up to 6 months at a minimum period in this study. In accordance with previous data from mRNA vaccine20, SARS-CoV-2-specific CD4+ T cells induced by inactivated vaccine falled into central and effector memory subsets mostly. While the majority of SARS-CoV-2-specific CD8+ T cells were TEMRA cells. For the expression of CCR7, the central memory T cells are homing to the secondary lymphoid organs and may play a key role in the secondary response in future infection or booster vaccination. Effector memory T cells are circulating in between blood and peripheral tissues and may provide prompt immune response upon infection44, 45. For the emergence of VOCs of SARS-CoV-2, there is growing concern over vaccine efficacy. T cells from COVID-19 convalescents and in recipients of mRNA vaccine can recognize peptide epitopes distributed throughout the SARS-CoV-2 spike protein and the total reactivity against SARS-CoV-2 variants of B.1.1.7, B.1.351, P.1, and CAL.20C lineages are mostly maintained in terms of magnitude and frequency of response46. SARS-CoV-2-specific T cells from convalescent COVID-19 patients or vaccinated individuals direct target the conserved epitopes between prototype and VOCs47, 48. Thus SARS-CoV-2-specific T cells by vaccination are likely to be less affected by antibody escapes mutations in variants. A study has shown that mRNA vaccine-induced SARS-CoV-2 specific T cells were qualitatively similar to that following SARS-CoV-2 infection20. We found that SARS-CoV-2-specific T cells by inactivated vaccine expanded robustly after the third booster dose. The induction of SARS-CoV-2-specific memory T cell subsets with the capacity of long-term duration by inactivated vaccine supports the idea that T cell responses could be long-lived and contribute to future immune protection.
Another key finding in this study was that the induction of SARS-CoV-2-specific cTFH cells by the inactivated vaccine. Our previous study has demonstrated the mobilization of cTFH cells after the first dose of inactivated vaccination11. For the relatively late development of humoral response by the inactivated vaccines, early response of cTFH cells could contribute to the early protection of vaccination when antibody level was still low3,49. cTFH cells have been associated with humoral response in COVID-19 patients or vaccination individuals20, 23. Data in this study further confirmed that the induction of cTFH cells by the inactivated vaccine correlated with humoral response closely.
Low seroconversion rates to mRNA vaccination have been reported in solid transplant recipients50. The applications of immune suppressants or B cell-targeted therapies could also hamper serological response to vaccination51, 52. Recently, data show that antibody response was enhanced in kidney transplant recipients with minimal serologic response to 2 doses by a third dose of mRNA vaccine31. In this study, we found that a third dose of inactivated vaccine could induce a strong antibody response in those seronegative individuals after two doses of vaccine within 1 week. The booster shot also induced the expansion of SARS-CoV-2-specific memory B cells and T cells. HCWs with low serological response to 2 doses were not truly “no responders” but fully equipped with immune memory that could be quickly recalled by a third dose. These data provide evidence for those who to receive a booster shot after two doses of vaccination.
Data from this study point to the immunological benefits of a third dose of inactivated vaccine and highlight the important role of SARS-CoV-2-specific memory B cells in future infection and vaccination. In concern with the potential decayed humoral immunity over time after vaccination and the emergence of VOCs, the induction of SARS-CoV-2-specific memory B cells and T cells could represent key factors of long-term protective immunity against SARS-CoV-2 infection. With continued high global incidence, and potential for more transmissible SARS-CoV-2 variants, data on longer-term vaccine efficacy and antibody dynamics are needed for clarifying the necessity of further booster doses. HCWs and frontline staff, who face high exposure rates and dangers from SARS-CoV-2 and are in anticipation of a potential need for booster shots. Immune compromised patients or individuals with low response rates to 2 doses of vaccine could benefit from a third dose of vaccine. Nevertheless, it is important to note that further studies are needed to demonstrate the clinical relevant of these immunological responses by inactivated vaccination.
Author Contributions
HX, HZ and JW supervised the study. YL, QZeng, CD, MLi, LL and DL contributed equally to the study. HX, HZ, JW and YL conceived and designed the study. YL, DL, JM and RM recruited participants in the trial and collected blood samples. QZeng, CD, MLi and LL performed the experiments and collected data. QZeng and QZhou performed statistical analysis. HZ, YL, QZeng, CD, MLi, LL and DL drafted the report. HX, JW, SP and MLiu made critical revision on the manuscript. All authors contributed to the interpretation of data. All authors approved the final version before submission.
Conflict interests
The authors have no conflicts of interest to disclose.
Acknowledgment
The work is supported by The Talent Program of the First Affiliated Hospital, Sun Yat-sen University (Y70311) and The Hundred Talent Program of Sun Yat-sen Univetsity (Y61229).
Reference



