
Summary
SARS-CoV-2 infection causes a wide spectrum of disease severity. Immune changes associated with severe disease include pro-inflammatory cytokine production and expansion of immature myeloid populations. The relative importance of the immunological changes in driving progression to severe disease remain poorly understood.
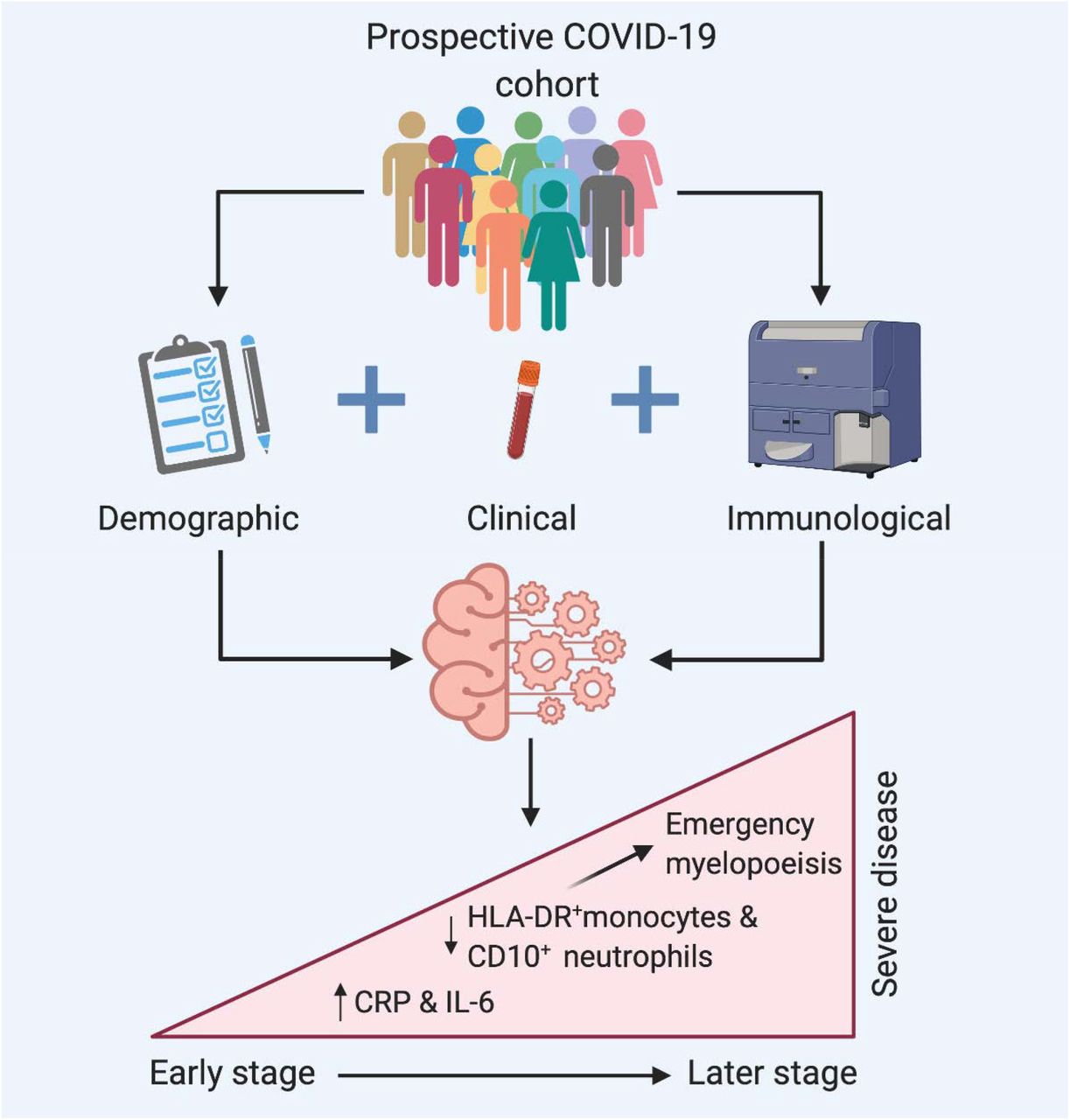
We aimed to identify and rank clinical and immunological features associated with progression to severe COVID-19. We sought to use tests available in an on-site diagnostic hospital laboratory to identify an immunological signature for severe disease development which could be detected prior to peak severity thereby allowing initiation of therapeutic interventions. We used univariate and multivariate analysis, including unbiased machine learning, to investigate the relationships between clinical and demographic characteristics, inflammatory markers, and leukocyte immunophenotypes with progression to severe disease in 108 patients and to rank these in importance. A combination of four features (elevated levels of interleukin-6 and C-reactive protein, coupled with reduced monocyte HLA-DR expression and reduced neutrophil CD10 expression), were strongly predictive of severe disease with an average prediction score of 0.925.
Highlights
Severe COVID-19 can be predicted by a combination of emergency myelopoiesis (CD10-neutrophils and HLA DR-monocytes) and inflammation (raised IL-6 and CRP)
These changes can be identified from tests carried out prior to peak illness severity in a diagnostic laboratory
This predictive model was derived from a cohort of patients with a wide range of ages, frailty and COVID-19 severity

{kind=link}
Competing Interest Statement
The authors have declared no competing interest.
Funding Statement
L.T. has been awarded the Irish Clinical Academic Training (ICAT) Programme, supported by the Wellcome Trust and the Health Research Board (Grant Number 203930/B/16/Z), the Health Service Executive, National Doctors Training and Planning and the Health and Social Care, Research and Development Division, Northern Ireland. R.M.M. has been awarded a Science Foundation Ireland (SFI) Investigator Award (15/IA/3041). N.C. and C.N.C. are part-funded by an SFI grant, Grant Code 20/SPP/3685.
Author Declarations
I confirm all relevant ethical guidelines have been followed, and any necessary IRB and/or ethics committee approvals have been obtained.
Yes
The details of the IRB/oversight body that provided approval or exemption for the research described are given below:
Ethical approval was granted by the Tallaght University Hospital / St. James's Hospital Joint Research Ethics Committee (reference REC 2020-03).
All necessary patient/participant consent has been obtained and the appropriate institutional forms have been archived.
Yes
I understand that all clinical trials and any other prospective interventional studies must be registered with an ICMJE-approved registry, such as ClinicalTrials.gov. I confirm that any such study reported in the manuscript has been registered and the trial registration ID is provided (note: if posting a prospective study registered retrospectively, please provide a statement in the trial ID field explaining why the study was not registered in advance).
Yes
I have followed all appropriate research reporting guidelines and uploaded the relevant EQUATOR Network research reporting checklist(s) and other pertinent material as supplementary files, if applicable.
Yes
Footnotes
CNC and NC are joint senior authors on this paper.
STAR COVID Bioresource
Data Availability
All relevant data is included in the manuscript. Further queries can be addressed to the corresponding author.



