
Abstract
We tested whether COVID-19 incidence and hospitalization rates were inversely related to vaccination coverage among the 112 most populous counties in the United States, each with a population exceeding 600,000, and together with a combined total population of 147 million persons. We measured vaccination coverage as the percent of the total population fully vaccinated as of July 15, 2021, with the exception of 11 Texas counties, where the cutoff date was July 14, 2021. We measured COVID-19 incidence as the number of confirmed cases per 100,000 population during the 14-day period ending August 12, 2021. We measured hospitalization rates as the number of confirmed COVID-19 admissions per 100,000 population during the same 14-day period. COVID-19 incidence was significantly higher among counties in the lower half of the distribution of vaccination coverage (incidence 543.8 per 100,000 among 56 counties with mean coverage 42.61%) than among counties in the upper half of the distribution of coverage (incidence 280.7 per 100,000 among 56 counties with mean coverage 57.37%, p < 0.0001). Hospital admissions were also significantly higher among counties in the lower half of the distribution (55.37 per 100,000) than in the upper half of the distribution (20.48 per 100,000, p < 0.0001). In log-linear regression models, a 10-percentage-point increase in vaccination coverage was associated with a 28.3% decrease in COVID-19 incidence (95% confidence interval, 16.8 - 39.7%), a 44.9 percent decrease in the rate of COVID-19 hospitalization (95% CI, 28.8 - 61.0%), and a 16.6% decrease in COVID-19 hospitalizations per 100 cases (95% CI, 8.4 - 24.8%). Higher vaccination coverage is associated not only with significantly lower COVID-19 incidence, but also significantly less severe cases of the disease.
Introduction
Several observers have noted that the recent Delta variant-driven surge in COVID-19 cases in the U.S. has been concentrated in places with relatively low vaccination rates.1-3 Still others have pointed to the emergence of Delta-associated hot spots in highly vaccinated parts of the country.4 Here, we tested whether COVID-19 incidence and hospitalization rates during the two weeks ending August 12 were inversely related to the percentage of the population fully vaccinated by mid-July 2021. To avoid comparing small rural counties with large urban centers, we concentrated on the 112 largest counties, each with a population over 600,000, and together with a combined total population of 147 million persons.
Data and Methods
Data
Our data derive principally from the COVID-19 Community Profile Report maintained at healthdata.gov.5 The Counties tab in the spreadsheet for 8/12/2021 gave the incidence of COVID-19 cases per 100,000 during the most recent and the previous 7-day periods, from which we calculated the 14-day cumulative incidence. The spreadsheets for 8/5/2021 and 8/12/2021 gave the numbers of confirmed COVID-19 hospitalizations for the two previous 7-day periods, from which we computed county-specific 14-day hospital admission rates per 100,000. We also computed the number of COVID-19 hospital admissions per 100 cases, which we defined as 100 times the hospital admission rate divided by the incidence rate.
We similarly relied on the Counties tab in the spreadsheet for 7/15/2021 to extract the county-specific percentage of the population fully vaccinated as of that date. Since vaccination coverage for Texas was omitted from the Community Profile Report, we supplemented our database with state-specific data compiled by the Democrat and Chronicle as of 7/14/21.6
These sources taken together provided us with one independent variable – the vaccination coverage in each county as of mid-July – and three dependent variables – 14-day COVID-19 incidence, 14-day COVID-19 hospital admission rates, and COVID-19 hospital admissions per 100 cases – in each county for the period ending August 12.
Statistical Methods
We divided our study sample of 112 counties into 56 counties in the lower half and 56 counts in the upper half of the distribution of vaccination coverage. We then computed the means for each of the three dependent variables in both the lower and upper halves and then relied on the t-test based upon unequal variances to assess differences in group means.
We then conducted a cross-sectional regression analysis of the sample of 112 counties, where each county constituted a distinct observation. We employed ordinary least squares to estimate the parameters (α, β) of the log-linear model log Y = α + β X, where Y is the dependent variable of interest in each county (that is, COVID-19 incidence, COVID-19 hospitalization rate, or the hospitalization-case ratio) and X represents the corresponding vaccination coverage in that county. In our results below, we report these estimates as Model 1. We also estimated the same log-linear model by population-weighted least squares (reported as Model 2). We further estimated the model log Y = α + β X + μFL + μTX, where μFL and μTX, respectively, are binary parameters indicating whether the county was one of the 10 located in Florida or one of the 11 located in Texas (Model 3).
Results
The median vaccination coverage across all 112 counties was 49.95 percent. Thus, the lower half of the distribution consisted of 56 counties with a vaccination coverage below 49.95 percent, while the upper half consisted of 56 counties with a vaccination coverage equal to at least 49.95 percent. Table 1 gives the mean values of the independent variable and the three dependent variables for the lower and upper halves of the sample. The mean coverage of the lower half of the distribution was 42.61 percent, while the mean coverage of the upper half was 57.37 percent. The mean COVID-19 incidence per 100,000 was 543.8 per 100,000 in the lower half and 280.6 per 100,000 in the upper half (p < 0.0001 in a t-test of group means with unequal variances). The mean COVID-19 hospital admission rate per 100,000 was 55.37 in lower half and 20.48 in the upper half (p < 0.0001). The mean number of COVID-19 hospital admissions per 100 cases was 8.96 in the lower half and 7.06 in the upper half (p = 0.0037).
Table 1 below demonstrates significant absolute differences between the lower and upper halves in COVID-19 incidence, COVID-19 hospital admission rates, and the number of COVID-19 hospital admissions per 100 cases. What’s more, the relative difference in hospital admissions (55.37 / 20.48 = 2.70) is considerably greater than the relative difference in case incidence (543.8 / 280.6 = 1.94), a finding that points to a marked increase in case severity among low-coverage counties. This conclusion is supported by the significant difference between the two halves in the admission-case ratio.
Fig. 1 above displays a two-way scatterplot of COVID-19 incidence versus vaccination coverage in each of the 112 counties. While there is substantial scatter, an inverse relationship is nonetheless evident. The most populous counties in Florida – including Miami-Date, Palm Beach, Hillsborough (home to Tampa), Broward (home to Fort Lauderdale), Orange (home to Orlando), Duval (home to Jacksonville), and others – display notable clustering that suggests a shared determinant. This clustering is not as evident for Texas. While the data points for the interior counties of Bexar County (home to San Antonio) and Harris County (home to Houston) appear relatively close to each other, the cyan data point for the border county of El Paso TX, is situated at the bottom of the plot of Fig. 1.
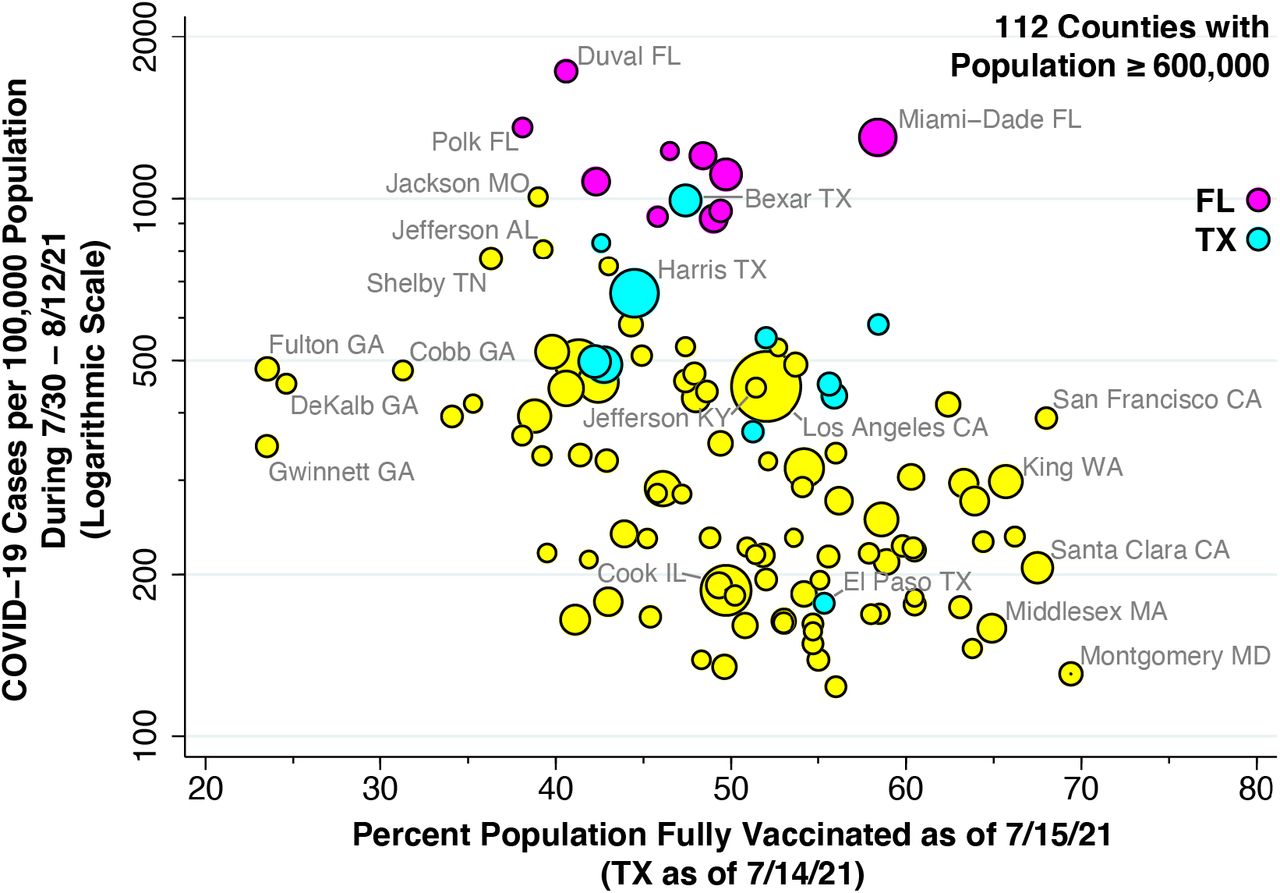
COVID-19 incidence is measured on a logarithmic scale as confirmed cases per 100,000 population. Vaccination coverage is measured as percent of population fully vaccinated. Vaccination coverage data for 11 Texas counties as of 7/14/2021. Florida counties highlighted in magenta. Texas counties highlighted in cyan. Size of data point proportional to county population.
Fig. 2 above plots hospital admission rates versus vaccination coverage. Again, an inverse relationship is evident. At one extreme, we observe low-vaccination, high-hospitalization counties such as Fulton County, GA (home to Atlanta) and Jefferson County, AL (home to Birmingham). At the other end, we observe high-vaccination, low-hospitalization counties such as Montgomery County, MD (home to Rockville and Bethesda), Middlesex County, MA (home to Cambridge), and King County, WA (home to Seattle).

Hospital admission rate is measured on a logarithmic scale as admissions for confirmed cases of COVID-19 per 100,000 population. Vaccination coverage is measured as percent of population fully vaccinated. Vaccination coverage data for 11 Texas counties as of 7/14/2021. Florida counties highlighted in magenta. Texas counties highlighted in cyan. Size of data point proportional to county population.
Fig. 3 below plots hospital admissions per 100 cases in relation to vaccination coverage. While Miami-Dade County appeared to be an outlier in Figs. 1 and 2, with high incidence and hospitalization rates, Fig. 3 shows that its hospitalization-to-case ratio, an indicator of case severity, is in line with its 58.4 percent vaccination coverage.

{kind=link}
{kind=link}
{kind=link}
COVID-19 hospital admissions per 100 cases is measured on a logarithmic scale as 100 times the ratio of the COVID-19 hospital admissions rate to the COVID-19 incidence rate. Vaccination coverage is measured as percent of population fully vaccinated. Vaccination coverage data for 11 Texas counties as of 7/14/2021. Florida counties highlighted in magenta. Texas counties highlighted in cyan. Size of data point proportional to county population.
Table 2 above provides our regression results for each of the three dependent variables. The estimated value of β = –0.0283 in the top panel means that a 10-percentage-point increase in vaccination coverage was associated with a 28.3% decrease in COVID-19 incidence (95% confidence interval, 16.8 – 39.7%). The estimated value of β = –0.0449 in the top panel means that a 10-percentage-point increase in vaccination coverage was associated with a 44.9% decrease in COVID-19 hospital admission rates (95% CI, 28.8 – 61.0%), while the estimated value of β = –0.0166 in the bottom panel means that the same 10-percentage-point increase in vaccination coverage was associate with a 16.6% decrease in COVID-19 hospitalizations per 100 cases (95% CI, 8.4 – 24.8%). The fact that the estimate of β displayed in the bottom panel equals the difference in the estimates of β derived from the other two panels is a direct consequence of our log-linear regression specification.
The column corresponding to Model 2 in Table 2 shows insignificant changes in the estimated values of β when we ran a population-weighted regression rather than ordinary least squares. The results in the column corresponding to Model 3 demonstrate that the estimates of β remained significant even when we included indicator variables for Florida and Texas.
Discussion
The most critical limitation of the current study is that the COVID-19 Community Profile Report, maintained at healthdata.gov,5 does not provide a detailed breakdown of our county-specific data by age group. While numerous demographic and environmental factors could have contributed to the substantial scatter seen in Figs. 1 through 3, including county-specific differences in racial and ethnic distribution as well as population density, nonetheless age-specific differences are likely to have figured most prominently. It is also possible that differences in public policies, including prohibition of mandates on vaccination and mask-wearing in schools and workplaces in certain states, may have been contributing factors.7 Still, the persistence of clearly detectable differences between low- and high-vaccination counties – even with the low R2 statistics seen in the regression results in Table 2 – points to an important, identifiable deterrent effect of vaccinations on disease spread.
A recent case report suggests that the Delta variant is more likely to cause breakthrough infections in fully vaccinated individuals, who may harbor sufficient concentrations of virus in the nasopharynx to transmit their infections to others.8 Another report finds a recent diminution in the effectiveness of mRNA vaccines in preventing infection among nursing home residents.9 Our results here do not bear directly on the existence or extent of such a phenomenon. But they do suggest that the phenomenon is not sufficiently important on a large scale to completely attenuate the inverse relationship between COVID-19 incidence and vaccination coverage seen here. What’s more, even if some fully vaccinated individuals can still transmit their infections, our findings offer indirect but concrete evidence that vaccination substantially reduces disease severity. Such a conclusion is supported by a recent report of trends in COVID-19 infections and hospitalizations among vaccinated and unvaccinated persons in New York state.10
Data Availability
The sources of data for this study are publicly accessible via the Internet at the URLs cited in the reference section. We have posted our data analyses at the Open Science Framework (OSF) in a project entitled 112-County COVID-19 Incidence-Vaccination Study (https://osf.io/wtb6j/).
Competing Interests Declaration
The author has no competing interests to declare.
Funding Declaration
The author has no funding sources to declare.
Human Subjects Declaration
This study relies exclusively on anonymized, publicly available data that contain no individual identifiers.
Data Availability Statement
The sources of data for this study are publicly accessible via the Internet at the URLs cited in the reference section. We have posted our data analyses at the Open Science Framework (OSF) in a project entitled 112-County COVID-19 Incidence-Vaccination Study (https://osf.io/wtb6j/).
Acknowledgments
This article represents the sole opinion of its author and does not necessarily represent the opinions of the Massachusetts Institute of Technology, Eisner Health, or any other organization or individual.
Footnotes
* Email: jeffrey{at}mit.edu
The Abstract and Methods now note that the total combined population of the 112 study counties was 147 million. Typos are corrected in the Abstract. Additional references are added to the Discussion.



