
Abstract
The SARS-CoV-2 Delta variant and its sublineages (B.1.617.2, AY.1, AY.2, AY.3; [1]) can cause high viral loads, are highly transmissible, and contain mutations that confer partial immune escape [2,3]. Using PCR threshold cycle (Ct) data from a single large contract laboratory, we show that individuals in Wisconsin, USA had similar viral loads in nasal swabs, irrespective of vaccine status, during a time of high and increasing prevalence of the Delta variant. Infectious SARS-CoV-2 was isolated from 51 of 55 specimens (93%) with Ct <25 from both vaccinated and unvaccinated persons, indicating that most individuals with Ct values in this range (Wilson 95% CI 83%-97%) shed infectious virus regardless of vaccine status. Notably, 68% of individuals infected despite vaccination tested positive with Ct <25, including at least 8 who were asymptomatic at the time of testing. Our data substantiate the idea that vaccinated individuals who become infected with the Delta variant may have the potential to transmit SARS-CoV-2 to others. Vaccinated individuals should continue to wear face coverings in indoor and congregate settings, while also being tested for SARS-CoV-2 if they are exposed or experience COVID-like symptoms.
Main text
We analyzed respiratory specimens from 719 individuals collected between 29 June 2021 and 31 July 2021. Delta and its sublineages accounted for 69% of all Wisconsin sequences in GISAID in the week beginning 27 June 2021; this proportion increased to 95% for the week ending 24 July, the most recent date for which data are available [4]. We recovered viral genome sequences from 122 of the specimens analyzed in this report; 110 of 122 (90%) belonged to Delta lineages. The high and increasing prevalence of Delta-lineage viruses during the study period, and high proportion of Delta-lineage viruses among our sequenced samples, together suggest that most infections in our dataset were caused by Delta, though this cannot be directly confirmed.
We defined fully vaccinated individuals as those who received a final vaccine dose at least 2 weeks prior to testing positive. Of the 719 individuals, vaccination status at the time of testing was available in the Wisconsin Immunization Registry and Wisconsin Electronic Disease Surveillance System for 322 (293 vaccinated and 29 unvaccinated), while self-reported vaccination status was available for the remaining 397 (18 vaccinated and 379 unvaccinated). We compared Ct values in specimens from these fully vaccinated and unvaccinated individuals at the time of testing (Figure 1). We detected no significant differences in Ct values by vaccination status. Notably, 212 of 311 (68%) of individuals with infection despite full vaccination had extremely low Ct values <25, consistent with high viral loads.

Distributions of SARS-CoV-2 PCR cycle threshold (Ct) values at the time of testing do not differ by vaccination status. N1 PCR Ct values for SARS-CoV-2-positive specimens grouped by vaccination status. Boxplots represent mean N1 Ct values +/- one standard deviation. P-values were calculated by comparing mean Ct values between the groups by Welch two-sample t-test.
While a given Ct value cannot be used to infer infectiousness, previous studies suggested that infectious SARS-CoV-2 can frequently be recovered from specimens with Ct values of 25-30 or lower [5]. To determine whether high viral loads might indicate the presence of infectious SARS-CoV-2, we attempted to culture infectious virus from a subset of 55 specimens with Ct values <25 (Figure 2). Infectious SARS-CoV-2 was isolated from 14 of 16 specimens (88%) from unvaccinated individuals and 37 of 39 specimens (95%) from vaccinated people, suggesting that Ct <25 is frequently associated with the capacity to shed infectious SARS-CoV-2, even in fully vaccinated persons.
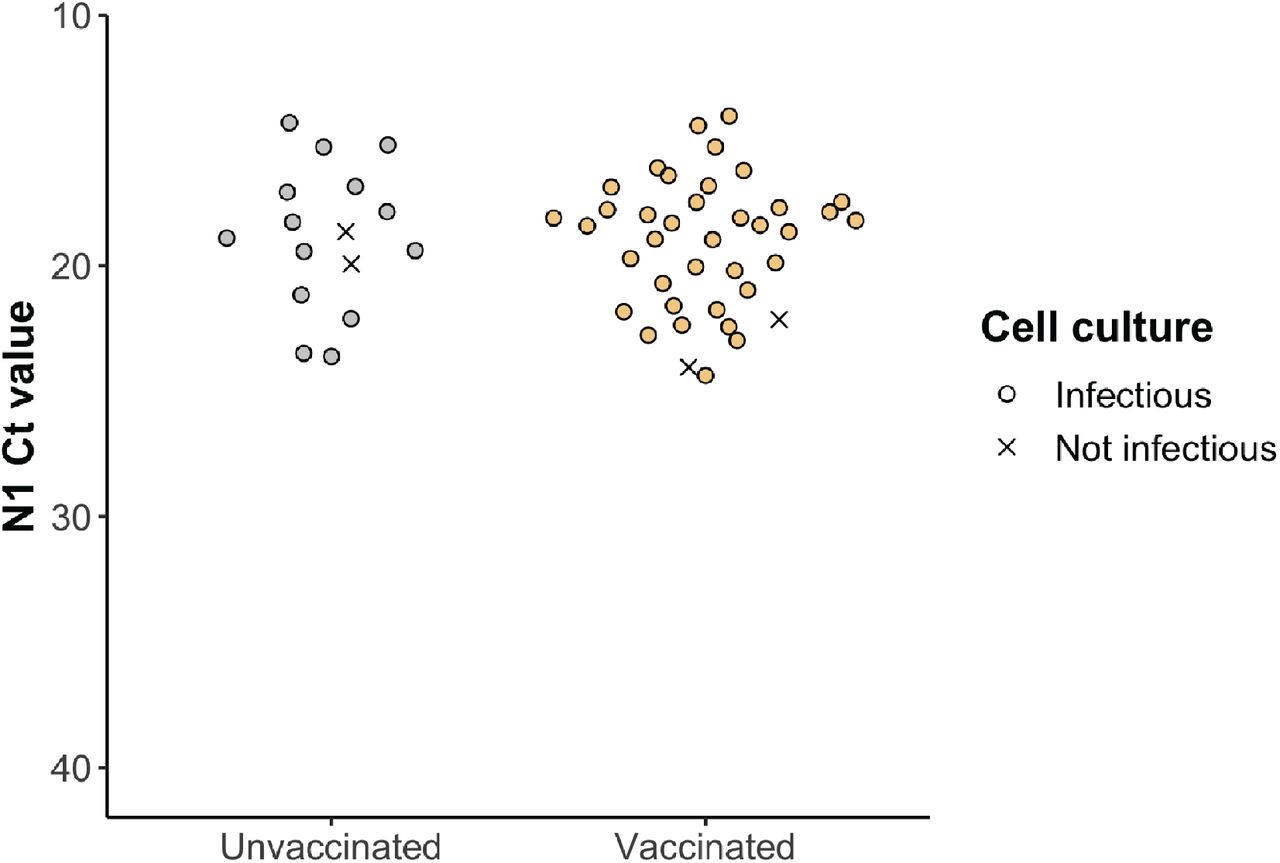
Infectious virus detected in nasal swab specimens from unvaccinated and fully vaccinated cases with Ct values < 25. Infectiousness was determined by the presence of cytopathic effects (CPE) after 5 days of replication in Vero E6 TMPRSS2 cells. Specimens with visually apparent CPE under a light microscope are represented by filled circles, and specimens without apparent CPE are represented by ‘X’.
Data on symptom status were available from 516 of the 719 individuals evaluated here, so we further compared Ct values in test-positive specimens according to vaccination and symptom status (Figure 3A). For symptomatic cases, there was no significant difference in the time elapsed between symptom onset and testing for vaccinated vs. unvaccinated individuals (two-sample K-S test, p=0.49; Figure 3B). Full vaccination did not affect Ct values observed in infected individuals, either with or without symptoms, at the time of testing. Among those for whom symptom status is known, 252 of 276 individuals who were not fully vaccinated (91%) reported symptoms at the time of testing, while 228 of 240 people who were fully vaccinated (95%) reported symptoms. Among individuals who were asymptomatic at the time of testing, Ct values <25 were detected in 7 of 24 unvaccinated individuals (29%; CI: 13-51%) and in 8 of 12 individuals who were infected despite being fully vaccinated (67%; CI: 35-90%). Infectious virus was detected in the sole specimen tested from an asymptomatic fully vaccinated individual. Although the number of asymptomatic individuals sampled is small, these results indicate that some individuals who are infected despite vaccination can have high viral loads and shed infectious virus even while being asymptomatic. Additional virus isolation data are needed to determine the frequency of infectious virus shedding in asymptomatic cases.

{kind=link}
{kind=link}
{kind=link}
Symptom status does not affect distributions of SARS-CoV-2 PCR cycle threshold (Ct) values at the time of testing in vaccinated vs. unvaccinated persons. A) N1 Ct values for SARS-CoV-2-positive specimens grouped by vaccination status for symptomatic, asymptomatic, and unknown symptom status cases. Boxplots represent mean N1 Ct values +/- one standard deviation. P-values were calculated by comparing mean Ct values between groups by Welch two-sample t-tests. B) Density distributions of unvaccinated and vaccinated specimen collection dates by day since symptom onset. Day 0 on the x-axis denotes self-reported day of symptom onset. Negative values for days indicate specimen collection prior to symptom onset. Symptom onset data were available for n=249 unvaccinated cases and n=222 vaccinated cases.
Our findings are consistent with other recent reports detecting high virus loads in some individuals infected despite vaccination in England [6] and Singapore [7]. Our detection of infectious virus in 93% of samples with Ct <25 indicates that high viral loads are consistent with the potential to transmit SARS-CoV-2, regardless of the individual’s vaccination status. Notably, transmission of Delta from vaccinated healthcare workers to their household contacts was recently documented in an investigation of a hospital-associated outbreak in Finland [8]. An outbreak in Barnstable County, MA associated with large gatherings also involved a substantial proportion of fully vaccinated individuals [9]. The co-circulation of viruses belonging to Pango lineages B.1.617.2, AY.2, and AY.3, as well as the broad geographic distribution of our specimens, indicate that the infections analyzed here are not associated with any single large outbreak, and that Delta-lineage SARS-CoV-2 can achieve high viral loads consistent with transmissibility in fully vaccinated individuals across a range of exposure settings. Taken together, these studies indicate that individuals infected with Delta variants despite vaccination have the capacity to transmit infection to others.
Our study has at least three important limitations. First, we have only one specimen from most individuals, and therefore we cannot know the trajectory of viral loads at the time of testing. Indeed, a study of Delta infection dynamics suggests that viral loads decline more rapidly in vaccinated vs. unvaccinated individuals, as one might expect [7]. However, that study also indicates that viral loads in vaccinated and unvaccinated individuals remain similarly high for 5-6 days after illness onset, before declining more rapidly in vaccinated people. In our study, 91% of specimens from symptomatic cases were collected from 0-6 days after illness onset and the timing of tests relative to illness onset did not differ by vaccination status. These observations suggest that the Ct value comparisons in our study are likely not biased by the time of testing. A second limitation is that there may be differences in the populations of vaccinated and unvaccinated persons seeking testing that bias our results. Vaccinated individuals may not perceive a high risk of COVID-19 disease, and may be less likely to seek testing than unvaccinated people. It is difficult to determine from our data whether vaccinated and unvaccinated people experienced symptoms of similar severity. Thus, we cannot determine the extent to which our sampling failed to detect asymptomatic or paucisymptomatic infections. Such mild infections may be more frequent among vaccinated than unvaccinated individuals infected with Delta.
Consistent with this, a recent report from England detected a substantially greater proportion of low-positive tests with Ct values between 35 and 40 in vaccinated individuals than in the unvaccinated [6]. Importantly, our study was not designed to estimate the rate of infection despite vaccination, but rather to determine whether individuals infected despite vaccination could have high viral loads consistent with the potential to transmit SARS-CoV-2. Finally, there is inherent variability in PCR Ct values due to specimen variability that can be impacted by collection technique and other variables outside of our control.
The finding of high SARS-CoV-2 viral loads and replication-competent virus in vaccinated individuals has important implications for risk assessment and mitigation. The impact of Delta variants on vaccine effectiveness is currently being evaluated (see, e.g., [10]). Risk disinhibition may lead vaccinated people to increase behaviors that expose them to SARS-CoV-2 infection, and individuals who are infected despite vaccination could serve as sources of onward transmission to others. Vaccinated individuals, particularly those who may have high levels of community or occupational exposure to SARS-CoV-2, should be encouraged to continue frequent testing, especially when symptomatic, to limit community spread. Continued adherence to non-pharmaceutical interventions, such as masking and distancing, will remain important for both vaccinated and unvaccinated individuals because we cannot predict which vaccinated individuals will experience infections with high viral loads. While vaccines continue to provide outstanding protection against severe disease and mortality, the durability of this protection cannot be reliably predicted. Therefore, it is essential for public health policy to encourage vaccination while also planning for contingencies, including diminished long-term protection.
Data Availability
Data and processing workflows are available at https://go.wisc.edu/p22l16. To protect potentially personally identifiable information, the publicly available dataset contains only PCR Ct values, vaccine status, symptom status, and days from symptom onset to testing for each specimen.
Conflict of interest
The authors declare no conflicting interests.
Ethics statement
Per the University of Wisconsin-Madison IRB, this project qualifies as public health surveillance activities as defined in the Common Rule, 45 CFR 46.102(l)(2). As such, the project is not deemed to be research regulated under the Common Rule and therefore, does not require University of Wisconsin-Madison IRB review and oversight.
Data availability
Data and processing workflows are available at https://go.wisc.edu/p22l16. To protect potentially personally identifiable information, the publicly available dataset contains only PCR Ct values, vaccine status, symptom status, and days from symptom onset to testing for each specimen.
Acknowledgments
We would like to acknowledge the local health departments in Wisconsin who referred samples for SARS-CoV-2 testing. We gratefully acknowledge Shelby O’Connor and Hannah Segaloff for critical review of the manuscript and helpful discussion. We also acknowledge all Exact Sciences employees who contributed to sample testing. This work was supported by Centers for Disease Control and Prevention contracts 75D30120C09870 and 75D30121C11060 to D.H.O and T.C.F. The authors are also members of the Upper Midwest Regional Accelerator for Genomic Surveillance funded by the Rockefeller Foundation.
Footnotes
The key changes in this revision are: - Inclusion of more individuals dating to 31 July 2021 - Addition of verified vaccine statuses of some samples from official public health registries - Addition of virus culture data from samples with a PCR Ct < 25 - Addition of information on testing timing - Removal of Pango lineages and GISAID identifiers since we are now using an expanded dataset where delta was even more prevalent in Wisconsin



