
Abstract
SARS-CoV-2 variant B.1.617.2 (delta) is associated with higher viral loads [1] and increased transmissibility relative to other variants, as well as partial escape from polyclonal and monoclonal antibodies [2]. The emergence of the delta variant has been associated with increasing case counts and test-positivity rates, indicative of rapid community spread. Since early July 2021, SARS-CoV-2 cases in the United States have increased coincident with delta SARS-CoV-2 becoming the predominant lineage nationwide [3]. Understanding how and why the virus is spreading in settings where there is high vaccine coverage has important public health implications. It is particularly important to assess whether vaccinated individuals who become infected can transmit SARS-CoV-2 to others. In Wisconsin, a large local contract laboratory provides SARS-CoV-2 testing for multiple local health departments, providing a single standard source of data using the same assay to measure virus burdens in test-positive cases. This includes providing high-volume testing in Dane County, a county with extremely high vaccine coverage. These PCR-based tests provide semi-quantitative information about the viral load, or amount of SARS-CoV-2 RNA, in respiratory specimens. Here we use this viral load data to compare the amount of SARS-CoV-2 present in test-positive specimens from people who self-report their vaccine status and date of final immunization, during a period in which the delta variant became the predominant circulating variant in Wisconsin. We find no difference in viral loads when comparing unvaccinated individuals to those who have vaccine “breakthrough” infections. Furthermore, individuals with vaccine breakthrough infections frequently test positive with viral loads consistent with the ability to shed infectious viruses. Our results, while preliminary, suggest that if vaccinated individuals become infected with the delta variant, they may be sources of SARS-CoV-2 transmission to others.
Main text
The term “vaccine protection” can have several meanings, and is not always clearly defined (reviewed in [4]). Ideally, vaccination would provide “sterilizing immunity,” completely preventing virus replication in vaccinated individuals. Intramuscularly delivered vaccines against respiratory viruses are not necessarily expected to provide this level of protection, however [5]. Current SARS-CoV-2 vaccines are thought to provide rapid immune control of virus replication, protecting vaccinated people against symptomatic disease, severe disease, and/or death, with varying levels of effectiveness. We might therefore expect vaccination to limit the magnitude of virus shedding in vaccinated individuals who become infected (i.e., in breakthrough infections). Lowering virus load could diminish both the severity of disease and the potential for onward transmission of SARS-CoV-2 from a vaccinated individual.
To determine whether vaccination reduces virus load in the setting of SARS-CoV-2 vaccine breakthrough, we compared the threshold cycle (Ct) value in test-positive specimens collected between 28 June 2021 and 24 July 2021 from 83 individuals in Dane County, Wisconsin, which has one of the highest rates of vaccination among populous counties in the United States [6] and high rates of testing per capita. Self-reported vaccine status and dates of final vaccine were used to stratify this cohort into two groups: fully vaccinated (i.e., two weeks after final self-reported vaccine dose; n=32) and those who had not received any vaccine (n=51; Figure 1A). Though Ct values do not provide absolute virus quantification, they provide a convenient proxy for estimated viral loads. Notably, all Ct values in our dataset were generated by the same contract laboratory using the same protocol, eliminating a potential source of variability.

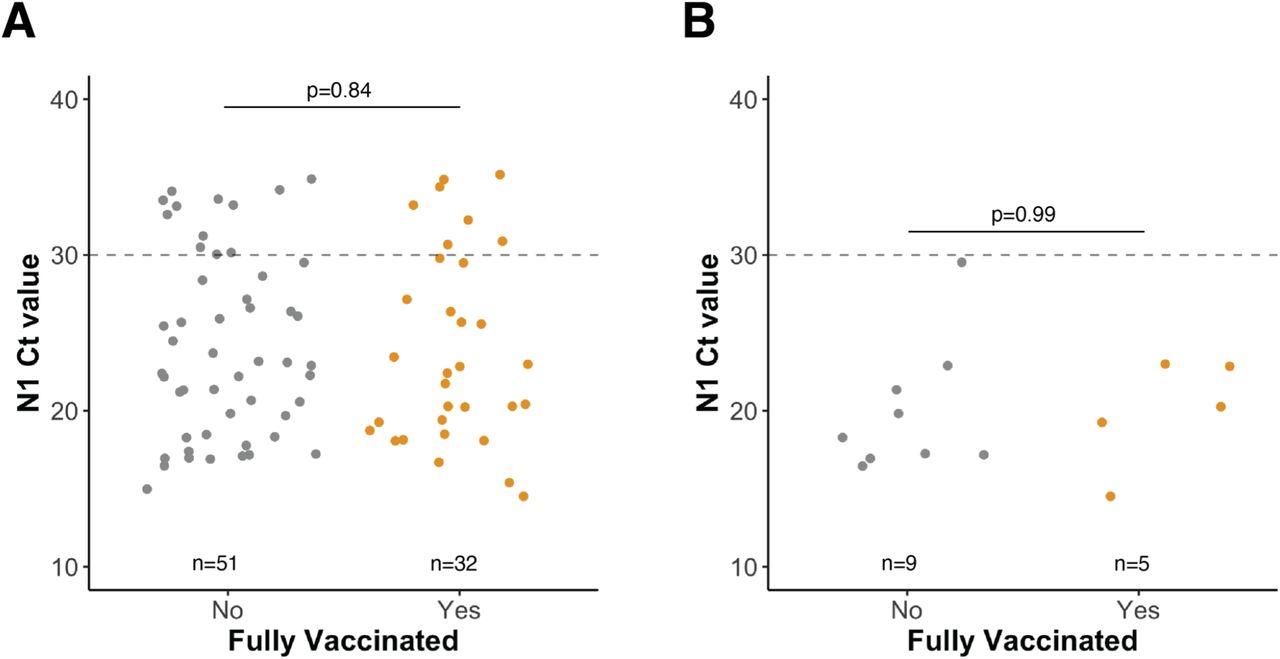
Viral loads for Dane County specimens are independent of vaccination status. A) N1 threshold cycle (Ct) values for SARS-CoV-2-positive specimens grouped by vaccination status. B) N1 Ct values for SARS-CoV-2-positive specimens confirmed to be delta variants by sequencing. In A and B, the horizontal dashed line represents the threshold for consistent recovery of infectious virus as well as our Ct cut-off for sequencing specimens. Sequence data were available only for specimens collected on or before 16 July 2021, not all samples had a Ct < 30, and not all samples with a Ct < 30 sequenced successfully, accounting for the relatively low number of delta confirmed sequences. P-values were calculated by comparing mean Ct values between groups by Welch two sample t-tests. Data from the Dane County cohort are shown.
We detected no significant differences in Ct values between fully vaccinated and unvaccinated individuals. Previous studies have suggested that Ct values of ∼30 or lower are consistent with the recovery of infectious virus in biological specimens, an indication of potential contagiousness [7–9]. Figure 1B shows the same analysis, restricted to samples in which the presence of the delta variant was confirmed by sequencing. We generated sequence data from 16 of these specimens; 14 of 16 (88%) belonged to the delta lineage (Supplemental Figure 1). Thus, we cannot confirm the virus lineages of the majority of cases, although the high prevalence of delta variants in the sequenced specimens suggests many, if not most, are delta.
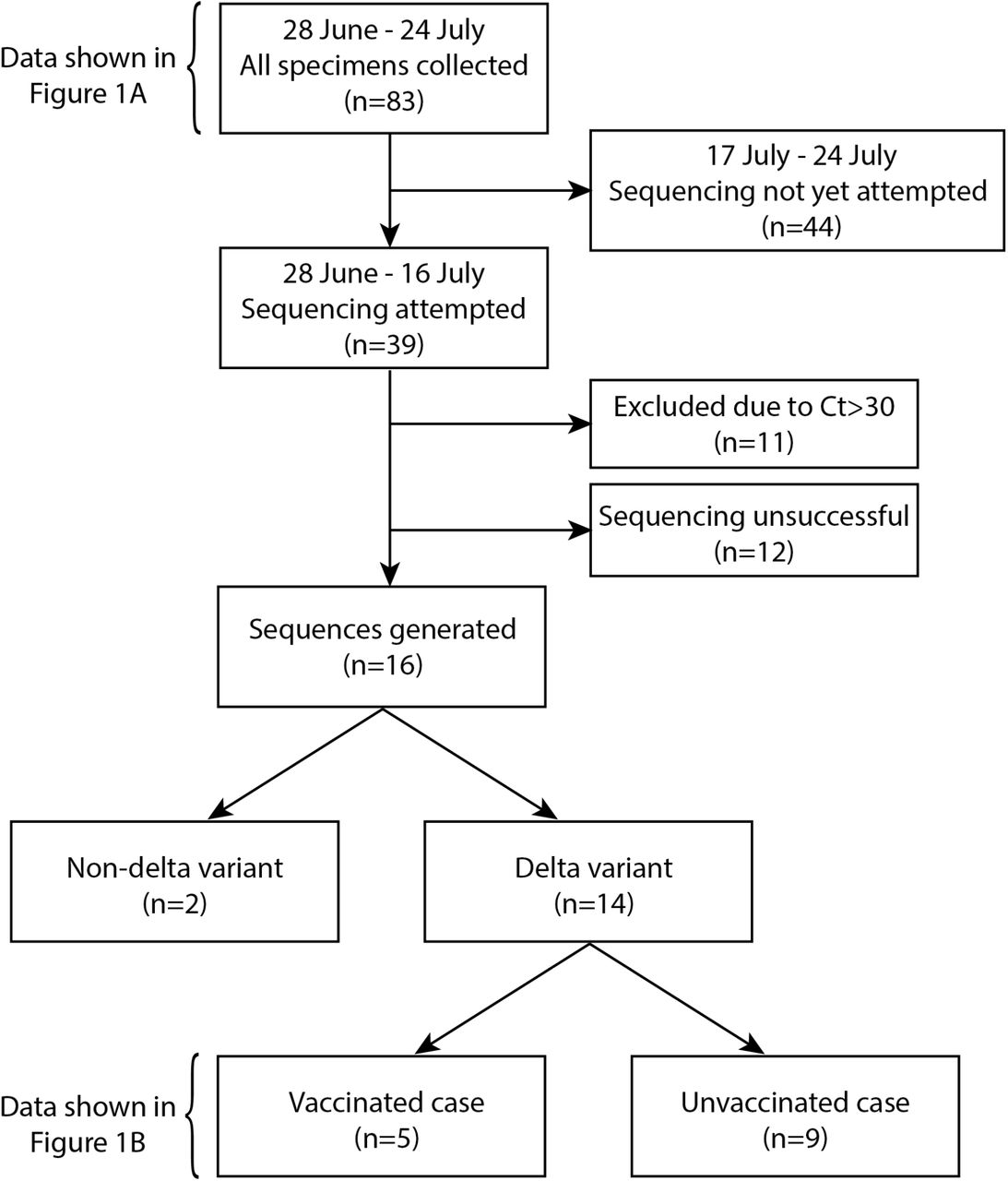
Inclusion/exclusion workflow for sequencing of Dane County specimens in this study.
We then expanded the analysis to include 208 additional samples from other Wisconsin counties that are tested by the same commercial laboratory. Considering all 291 samples from all counties (Supplemental Figure 2), there were 79 infections among individuals who were fully vaccinated (Figure 2A). Sixty-six of these 79 (84%) had Ct values ≤30, while 177 of 212 (83%) unvaccinated individuals had viral loads in this range. Moreover, 26 of 79 (33%) of fully vaccinated individuals with breakthrough infections had extremely low Ct values <20, consistent with very high viral loads. Taken together, these data suggest that a substantial proportion of individuals with SARS-CoV-2 vaccine breakthrough infections during our study period have levels of SARS-CoV-2 RNA in nasal secretions that are consistent with the ability to transmit the virus to others.

Inclusion/exclusion workflow for sequencing of all Wisconsin specimens in this study, including specimens collected in Dane County.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Viral loads for the expanded Wisconsin cohort, including Dane County, are independent of vaccination status. A) N1 cycle threshold (Ct) values for SARS-CoV-2-positive specimens grouped by vaccination status. Specimens were collected from 11 Wisconsin counties. B) N1 Ct values for SARS-CoV-2-positive specimens were confirmed to be delta variants by sequencing. In A and B, the horizontal dashed line represents the threshold for consistent recovery of infectious virus as well as our Ct cut-off for sequencing specimens. Sequence data were available only for specimens collected on or before 16 July 2021, not all samples with a Ct < 30 were sequenced successfully, and not all were delta, accounting for the relatively low number of delta confirmed sequences. P-values were calculated by comparing mean Ct values between groups by Welch two-sample t-tests. Data from the expanded Wisconsin cohort, including Dane County, are shown.
Sequence data were available for 50 of 291 specimens. 42 of these (84%) were of the delta lineage (Figure 2B), in keeping with other genomic surveillance data indicating that delta was the predominant SARS-CoV-2 lineage in Wisconsin in July 2021 [10]. The high prevalence of delta variants across all sequenced specimens during our study period again suggests that a majority of the unsequenced infections are also caused by delta variants, though this cannot be confirmed.
These findings will need to be substantiated in larger cohorts and are subject to sources of potential data skew that could limit generalizability. Dane County accounts for 29% (83/291) of cases reported here. Vaccination rates in this county are much higher than the US national average (49.4% of the US population and 67.4% of the Dane County population is fully vaccinated). Testing is also more common in Dane County, with 3.08 tests per person compared to a US average of 1.48 tests per person. This high vaccination rate and high rate of testing enable us to ascertain a relatively high proportion of breakthrough infections, but it also means that circumstances that are unique to this county could confound the data. It is difficult currently to distinguish among potential mechanisms of vaccine breakthrough. A recent preprint suggests that the effectiveness of the Pfizer vaccine against symptomatic disease may wane slightly with time since vaccination [11], but it is difficult to determine whether this represents waning levels of vaccine-induced immunity, increasing circulation of variants like delta with partial immune escape, and/or bias in the timing of vaccination, i.e. the possibility that the earliest groups to be vaccinated are enriched for individuals who are likely to have less robust immune responses to vaccination. It is also difficult to determine the rate of asymptomatic or paucisymptomatic breakthrough infections and to ascertain whether viral loads in such cases are as high as those in symptomatic breakthrough infections. The “true” proportion of breakthrough infections with high viral loads would require comprehensive, frequent surveillance testing of vaccinated populations to identify these individuals.
There may also be differences in viral dynamics with the delta variant that confound the interpretation of these results. With only one specimen per individual, collected at an arbitrary timepoint following infection, we cannot know the trajectory of viral loads at the time each “snapshot” was taken. Others have speculated that delta infections may involve a shorter eclipse phase before the onset of symptoms than with previous variants; this could motivate testing earlier during infection than has been the case with non-delta variants. We also cannot know from these data whether vaccination shortens the duration of high-level virus shedding, reducing the likelihood of onward transmission.
Nonetheless, the finding of high SARS-CoV-2 viral loads in vaccinated individuals has important implications for risk assessment and mitigation. Emerging data suggest that circulation of delta may be associated with reduced vaccine effectiveness against any symptomatic disease, but protection against severe disease and death is still robust [12]. However, risk disinhibition may lead vaccinated people to increase behaviors that expose them to SARS-CoV-2 infection, and individuals with breakthrough infections could serve as sources of onward transmission to others. Policies that create a dichotomy between vaccination and routine testing should be re-evaluated. Vaccinated individuals, particularly those who may have high levels of community or occupational exposure to SARS-CoV-2, should be encouraged to continue frequent testing, especially when symptomatic, to limit community spread. Continued adherence to non-pharmaceutical interventions, such as masking and distancing, will remain important for both vaccinated and unvaccinated individuals because we cannot predict which vaccinated individuals will experience breakthrough infections with high viral loads. This somewhat unexpected finding also underscores the uncertainty about the long-term performance of SARS-CoV-2 vaccines. While vaccines continue to provide outstanding protection against severe disease and mortality, the durability of this protection cannot be reliably predicted. Therefore, it is essential for public health policy to encourage vaccination while also planning for contingencies, including diminished long-term protection.
Vaccination status for cases in Dane County, Wisconsin from 28 June 2021 to 24 July 2021.
Vaccination status for cases in eleven Wisconsin counties, including Dane County, from 28 June 2021 to 24 July 2021.
Data Availability
Data and processing workflows are available at https://go.wisc.edu/p22l16. To protect potentially personally identifiable information, county of residence and sampling dates are redacted from the publicly available data.
Conflict of interest
The authors declare no conflicting interests.
Ethics statement
Per the University of Wisconsin-Madison IRB, this project qualifies as public health surveillance activities as defined in the Common Rule, 45 CFR 46.102(l)(2). As such, the project is not deemed to be research regulated under the Common Rule and therefore, does not require University of Wisconsin-Madison IRB review and oversight.
Data availability
Data and processing workflows are available at https://go.wisc.edu/p22l16. To protect potentially personally identifiable information, sample collection dates and county of residence are redacted from the publicly available dataset.
Acknowledgments
We would like to acknowledge the local health departments in Wisconsin who referred samples for SARS-CoV-2 testing and the Wisconsin Department of Health Services for facilitating the sequencing of residual test-positive samples. We gratefully acknowledge Ryan Westergaard, Kelsey Florek, Allen Bateman, and Shelby O’Connor for critical review of the manuscript and helpful discussion. We also acknowledge all Exact Sciences employees who contributed to sample testing. This work was supported by Centers for Disease Control and Prevention contracts 75D30120C09870 and 75D30121C11060 to D.H.O and T.C.F. The authors are also members of the Upper Midwest Regional Accelerator for Genomic Surveillance funded by the Rockefeller Foundation.



