
ABSTRACT
Introduction Indomethacin, a non-steroidal anti-inflammatory drug (NSAID), has been presented as a broad-spectrum antiviral agent. This randomised clinical trial in a hospital setting evaluated the efficacy and safety of this drug in RT-PCR-positive coronavirus disease 2019 (COVID-19) patients.
Materials & Methods A total of 210 RT-PCR-positive COVID-19 patients, who provided consent were allotted, to control or case arm, based on block randomisation. The control arm received standard of care comprising paracetamol, ivermectin, and other adjuvant therapies. The patient in the case arm received indomethacin instead of paracetamol, with other medications retained. The primary endpoint was the development of hypoxia/desaturation with SpO2 ≤ 93, while time to become afebrile and time for cough and myalgia resolution were the secondary endpoints.
Results The results of 210 patients were available, with 102 and 108 patients in the indomethacin and paracetamol arms, respectively. We monitored patient profiles along with everyday clinical parameters. Blood chemistry at the time of admission and discharge was assessed.
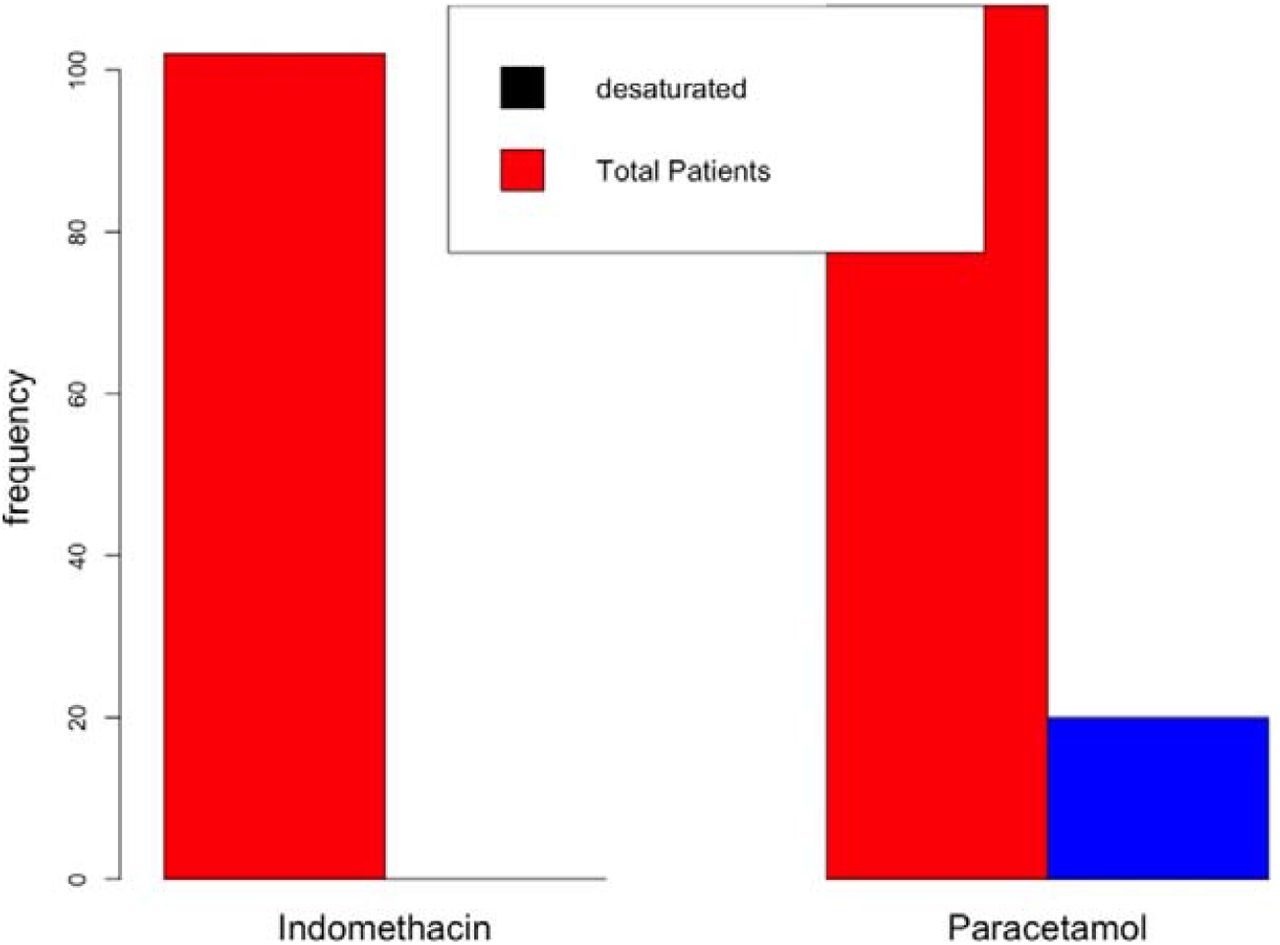
As no one in either of the arms required high-flow oxygen, desaturation with SpO2 level of 93 and below was an important goal. In the indomethacin group, none of the 102 patients developed desaturation. On the other hand, 20 of the 108 patients in the paracetamol arm developed desaturation. Patients who received indomethacin also experienced more rapid symptomatic relief than those in the paracetamol arm, with most symptoms disappearing in half the time. 56 patients out of 108 in the paracetamol arm had fever on the seventh day, while no patient in the indomethacin group had fever. Either arm did not report any adverse event. The fourteenth-day follow-up revealed that the paracetamol arm patients had faced several discomforts, including myalgia, joint pain, and tiredness; indomethacin arm patients mostly complained only of tiredness.
Conclusion Indomethacin is a safe and effective drug for treating patients with mild and moderate Covid-19.
1. Introduction
SARS-Cov-2, a member of the coronavirus family, has been ravaging the world for the past 18 months. Although an effective treatment has eluded the medical community, there have been several registered trials on finding new or repurposed drugs. Several studies have discussed the mechanism of the virus-host interaction and possible treatments [1] but a safe and effective treatment for the disease is yet to emerge. Drug repurposing seems to be an immediate solution and various drugs have been suggested for COVID-19 treatment [2, 3].
The drugs required to combat the pathogen may fall into one or more of the following categories: antivirals, anti-inflammatory agents, and supporting therapies [4, 5]. According to V’Kovski, [1] the antiviral action can be based on the stages of viral-host interactions. These include attachment and virus neutralisation, host protease inhibitors that stop the entry of the virus, viral protease inhibitors, viral RdRp inhibitors, and viral maturation inhibitors. Frediansyah et al. [6] enumerated the possible antiviral solutions at various stages of interactions. The role of cathepsin L in cleavage of the S protein complex and subsequent release of virus genome is well documented. Inhibiting cathepsin L inhibits the entry of SARS-Cov-2 by 76% [7].
Pro-inflammatory cytokine production is natural during immune response. The elimination of virus-infected cells is an important step in disease control. If this step, which naturally follows virus entry and replication, is defective or prolonged, it can result in a cytokine storm,[8] an uncontrolled release of pro-inflammatory cytokines. Several interleukins are involved in a cytokine storm, the foremost being interleukin 6 (IL-6), IL-1,[8] and IL -17 [9]. IL-17 also seems to have a role as the interaction partner of SARS-Cov-2. Anti-inflammatory drugs targeting the production of these interleukins are important for COVID-19 treatment.
1.1 Indomethacin as a Drug for SARS-Cov-2
Amici et al. [10] were the first to identify the antiviral activity of indomethacin. They recorded the antiviral activities of indomethacin against SARS-Cov-1 in vitro. Xu et al. [11] presented evidence of its antiviral activity against SARS-Cov-2. Their investigations covered the antiviral effect of indomethacin in vitro, cellulo, corona-infected canine models. They also stated that indomethacin does not reduce infectivity, binding, or entry into target cells. This conclusion is based on the results of Amici et al. [10] for SARS-Cov-1, although computer models have indicated otherwise [12]. Downregulation of ACE2 and TMPRSS2 is important to reduce infectivity. Using an open-source code, Gene2Drug, Napolitano et al.,[12] showed in a computer model that indomethacin downregulates ACE2 by suppressing the genes in the ACE2 pathway. Raghav et al. [13] depicted the role of indomethacin in inhibiting cathepsin L activity required for fusion. Interestingly, any other non-steroidal anti-inflammatory drugs [13] did not project this quality.
Non-Structural Protein7 (Nsp7), along with Nsp12, is important for RNA synthesis, as highlighted by Frediansyah et al. [6], Gordan et al. [9] recognised that prostaglandin E synthase 2 (PGES-2) is an “interactor” with Nsp7, and indomethacin inhibits PGES-2. Hence, indomethacin is an important candidate for blocking RNA synthesis. Amici et al. [10] reported of this block of RNA synthesis. Amici et.al [14] also demonstrated that protein kinase R (PKR) activation by indomethacin results in inhibition of virus protein translation. This follows the work of Brunelli et al. [15], where the role of indomethacin in activating PKR directly has been demonstrated.
Several publications [16, 17] have highlighted the importance of preventing inflammation in Covid-19 patients. Indomethacin downregulates IL-6 by inhibiting the synthesis of PGES-2 [18]. Indomethacin has been successful in preventing cytokine reactions in kidney transplant patients receiving OKT3 therapy [19, 20].
Rajan et al. [21] conducted one of the first indomethacin trials. Using the data from an open-label single-arm data for indomethacin, they showed the effect of indomethacin as a treatment option by matching propensity score with retrospectively collected data on paracetamol. Gordon et al. [9] showed by retrospective data analysis that indomethacin markedly reduces the need for hospitalisation. Two studies [22, 23] have shown the effectiveness of indomethacin in treating a small number of SARS-Cov-2 patients with severe comorbidities. However, these were small case series, and a larger controlled trial is required to validate these findings.
2 Materials & Methods
Panimalar Medical College, Chennai, India, was included in this trial. We recruited RT-PCR positive Covid-19 patients using block randomisation parallel group protocol [24] for efficacy and safety of indomethacin after obtaining Ethics Committee clearance and after an informed consent from the patients. The patients were apprised of the trial and the background before obtaining the informed consent which were made available in English and the vernacular language.
2.1 Ethics Approval
The trial was approved by the “Panimalar Medical College Hospital & Research Institute - Institutional Human Ethics Committee with a CDSCO Registration Number : ECR/1399/INST/2020. The approval Number for the trial is PMCH&RI/IHEC/2021/051
2.2 Trial Details
We registered the trial with Clinical Trial Registry of India (CTRI/2021/05/033544) of the ICMR. In this open label study, randomised sequence generated were handed over to the coordinators at the medical college for recruitment.
Indomethacin replaced paracetamol and was given along with the hospital standard care, which included doxycycline and ivermectin. However, other studies have shown that ivermectin may not be effective in treating Covid-19 patients [25]. We also added a proton pump inhibitor along with indomethacin. The drugs and their dosage are listed in Table 1.
Drug chart
The primary goal in this study was desaturation and requirement of oxygen. The secondary outcome was symptomatic relief. Safety profile of indomethacin was also monitored as a secondary outcome. We recruited 300 patients who had symptoms for about three days or less, based on a block randomisation protocol at a 1:1 ratio. All care were taken to conceal the allocation of patients from the treating physicians. They were not involved either in randomisation or the allocation. The results presented here are for 210 patients; 102 in the indomethacin arm and 108 in the paracetamol arm. A flow chart is given in Fig. 1.

Flow diagram for the recruitment of the patients
The inclusion criteria for patients are as follows:
2.2.1 Inclusion and Exclusion Criteria of Patients
Inclusion
Age between 20 and 90 years
RT-PCR Positive
Hospitalised patients
The case criteria for the study:
Normal Kidney Function Test (KFT)
Normal Liver Function Test (LFT)
Oxygen saturation – 94 or more
Exclusion
Hypersensitivity/Allergy to Drugs
Gastritis
Recent heart attack
Severe asthma
Acute kidney injury
Patients on immunosuppressants
Pregnant & lactating mothers
Indomethacin allergy
The following investigations were conducted on admission: CT scan of the lungs, LFT, RFT, liver function test, kidney function test, C-reactive protein (CRP), and D-dimer. We repeated blood chemistry on discharge and monitored the well-being of patients for 14 days. We also monitored the patients for oxygen saturation, fever, cough, and myalgia for seven days at the hospital. Patients were deemed symptomatically recovered if the temperature dropped below 99 0F for two days and cough reduced to score 1 on a one-to-ten scale (1: no cough; 2-3: cough sometimes; 4-6: coughing with the ability to do things; 7-8 persistent cough; 9-10: great deal of discomfort).
3.0 Results
We recruited patients based on random number generation. Patient profiles are shown in Fig. 2 and Table 2.

Profile of the recruited patients
The profile of the recruited patients
The age profile and gender-wise enumeration match closely in both groups. The temperature on admission had a marginal bias, being higher for patients in the indomethacin group. In addition, more patients in the indomethacin group had severe cough (above Scale 7). The co-morbidity distribution was similar.
To understand the impact of the sample size, we assumed the response rate for paracetamol and indomethacin to be 0.8 and 0.965 respectively. The sample size was calculated using R with an alpha value of 0.05. The marginal power was of 0.8 [26]. The sample size worked out to be 100. Post-hoc calculations based on actual results yielded a marginal power of 0.99.
3.1. Efficacy of Indomethacin
Symptomatic relief is very important for the psychological and physiological well-being of patients. We monitored the number of days to become afebrile, days for reduction of cough, and relief from myalgia. The results are presented in Fig. 3a for afebrile, Fig. 3b for number of days for cough reduction, Fig. 3c for cough reduction with a higher score on admission, Fig. 3d with lower cough score on admission and Fig. 3e for myalgia reduction.

Days for becoming afebrile

Number of days for cough reduction

Number of days for cough reduction with a score of 7 or higher on admission

Number of days for cough reduction with a score from 2 to 6 on admission

Number of days for myalgia reduction
Median (dark line) and interquartile ranges are shown as boxes. The symptomatic recovery from fever and cough in terms of median values are given in Table 3. Two points are significant from the table and figure. Symptomatic relief with indomethacin takes only half the time compared to paracetamol. Additionally, the IQR, a measure of statistical dispersion, is very small with indomethacin compared to that of paracetamol. This is significant because the action of indomethacin is almost independent of the condition of patient on admission. The p-values in the figure indicates statistical significance.
Symptomatic relief due to various treatments
The key question is the number of patients desaturating (SpO2 ≤ 93) in both arms. The patients were admitted with a median SpO2 of 95 (IQR = 1) and SpO2 of 96 (IQR = 1) in the indomethacin arm and paracetamol arm, respectively, with a minimum SpO2 of 94. Out of 108 patients, 20 desaturated in the paracetamol arm, while none desaturated in the indomethacin arm. Any patient did not require high-flow oxygen; prone position and occasional low-flow oxygen was enough. In the indomethacin arm, saturation improved in one or two doses. The results are presented in Fig. 4.

Number of patients desaturated
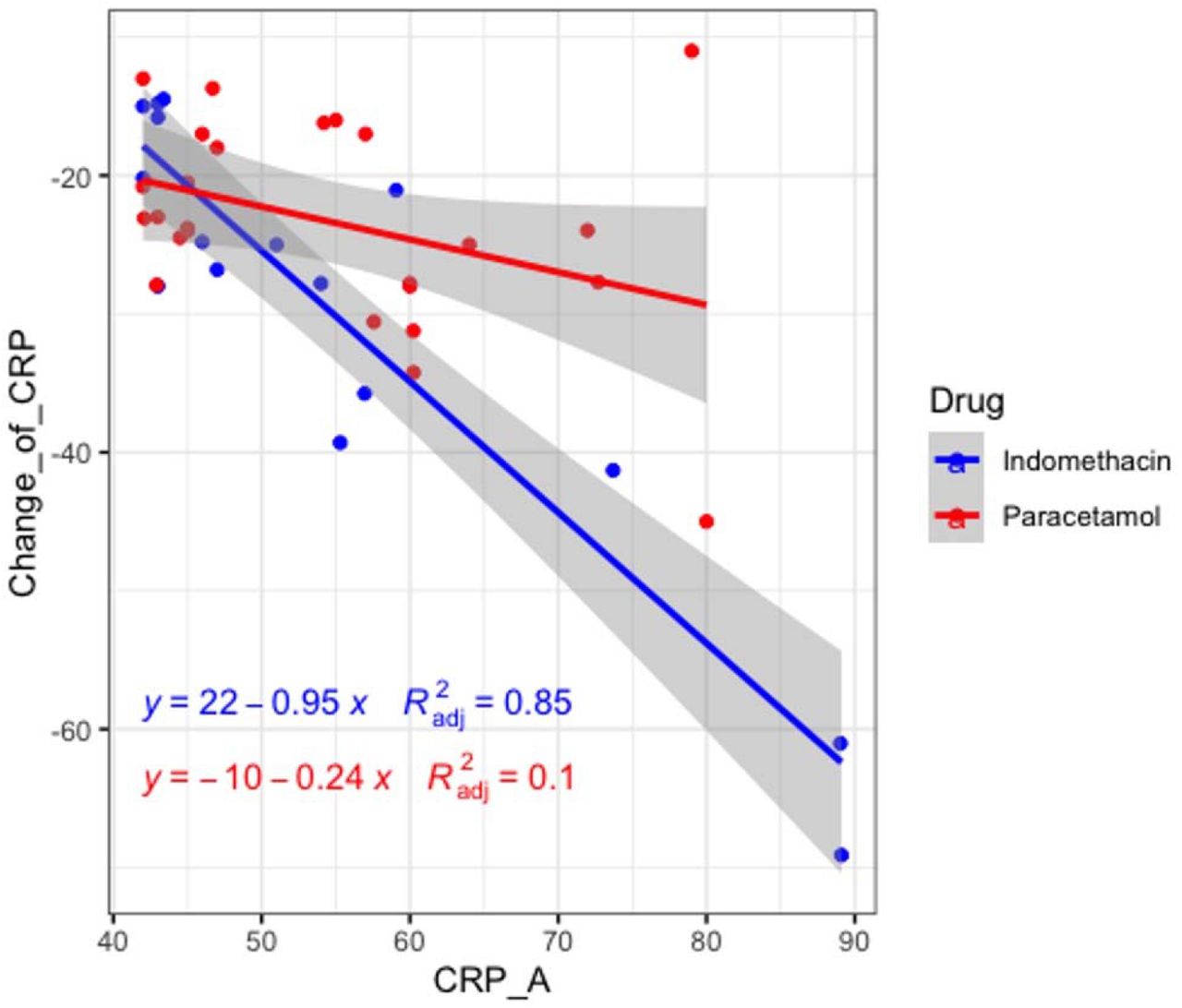
CRP is a well-known inflammatory marker, implicating Covid-19 as a severe disease. According to Liu et al.,[16] a CRP score greater than 41.8 may lead to a severe disease. Fig. 5 shows the relationship between CRP level on admission and decrease in CRP level on the seventh day. Fig. 6 shows the relationship between CRP on admission with a value greater than 41 and a reduction in CRP. Although the information in Fig.5 is available in Fig. 5, the separation provides clarity of data.

CRP on admission vs change in CRP at discharge

Relationship between CRP on admission (> 41) and change in CRP at discharge
60 patients took RT-PCR tests on the seventh day. The results are presented in Fig. 7. As can be seen from the figure, more patients became RT-PCR negative on the seventh day in the indomethacin arm although the p-value was 0.42.

RT-PCR-negative patients at the end of the seventh day
The patients were followed-up on the fourteenth day through telephonic enquiry. The results of patient feedback are summarised in Table 4. It should be noted that many patients had more than one ailment and, hence, the numbers did not add up to the total.
Fourteenth-day feedback of the patients.
3.2. Safety Profile of Indomethacin
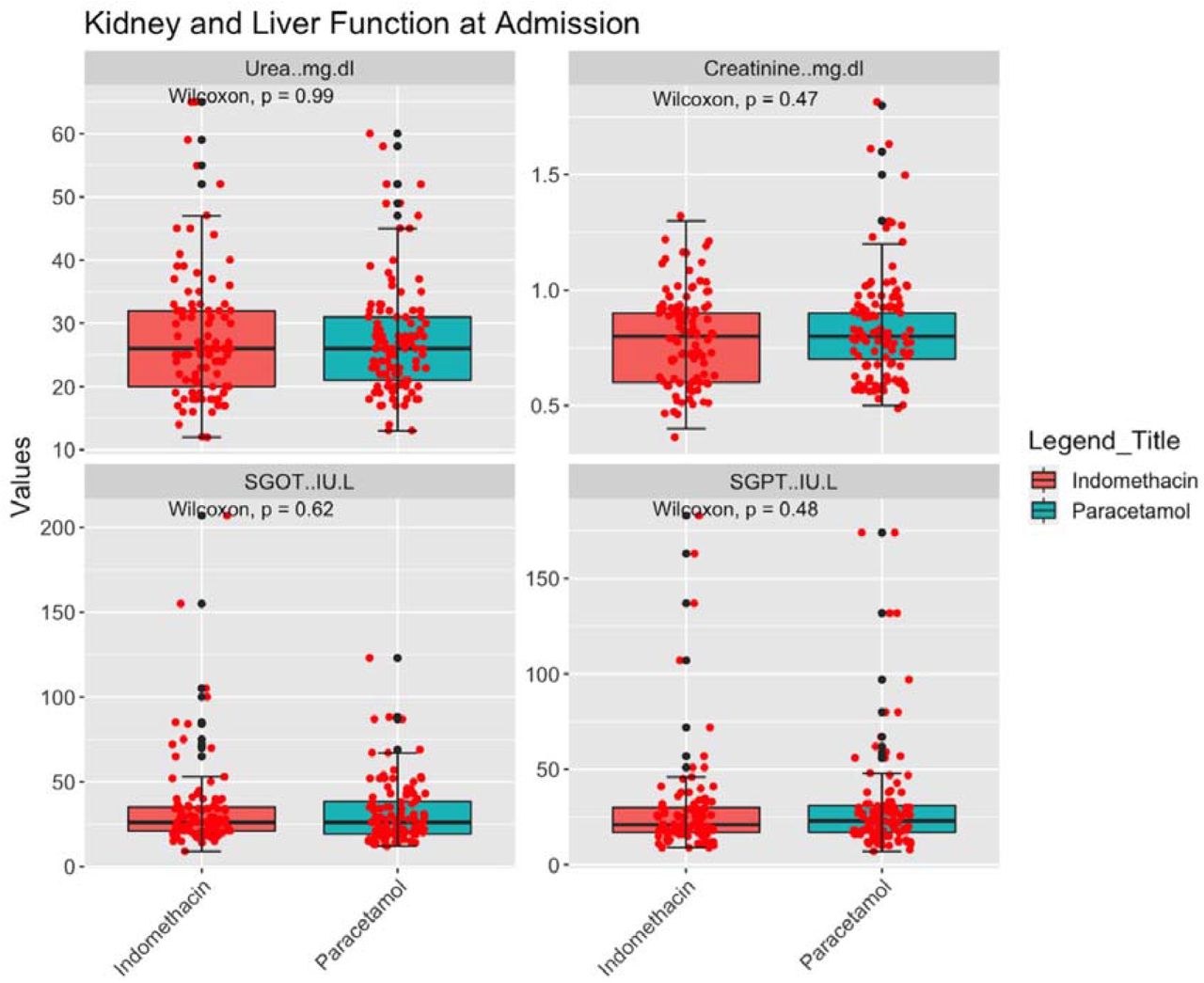
Indomethacin was approved in 1965. However, there have been concerns regarding its safety [27]. The number of prescriptions for indomethacin were 2.16 million [28] in 2018, in the US alone. Patients were tested for serum urea and creatinine, SGOT and SGPT before and after the treatment, and the results are shown in Fig. 8 and Fig. 9.

Kidney and liver function tests at admission

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kidney and liver function tests at discharge
Fig. 8 and Fig. 9 show statistical similarity between both arms. Neither the liver nor kidney function deteriorated after treatment in either arm. Patients or attending physicians did not report any other side effects.
4.0 Discussion
The primary aim of the study was to understand the efficacy of indomethacin in preventing desaturation (SpO2 ≤ 93) and deterioration in mild and moderate Covid-19 patients and compare this with a paracetamol-based arm. The secondary aim was to evaluate symptomatic relief in indomethacin patients compared to paracetamol patients. The results are striking: Indomethacin arm patients did not develop desaturation, while nearly 20 per cent of the paracetamol arm patients developed desaturation. When the SpO2 level dips below 93, we managed the patient with either low-flow oxygen or by placing them in prone position to enhance breathing. Any patient in this study did not show further deterioration. Notably, SpO2 improved just after one or two doses in the indomethacin arm. Patients with a marginal SpO2 level of 94 showed an improvement. At the end of the seventh day, 13 patients in the paracetamol arm were at a SpO2 level of 94. In the indomethacin arm, only two patients had SpO2 levels of 94, while 97 of the 102 patients had a higher SpO2 level, higher than 97. In the paracetamol arm only 51 patients (out of 108 patients) had a SpO2 level higher than 97.
Symptomatic relief was even more salient. The median time for becoming afebrile was three and seven days in the indomethacin and paracetamol arm, respectively. The median time for cough reduction was four days and seven days in the indomethacin and paracetamol arm, respectively. 59 out of 108 patients in the paracetamol arm had fever on the seventh day while any of the indomethacin arm patients did not have fever. 49 of 75 patients taking paracetamol took seven or more days to recover from cough; only nine out of 70 patients in the indomethacin arm took seven days or more to recover and they were at level 2 in the ordinal scale. No patient in the indomethacin arm required continuation of indomethacin after the five-day regimen. On the other hand, patients who were not afebrile after the treatment regimen of five days in the paracetamol arm were continued with the paracetamol at the discretion of the treating physician. One of the most important conclusions came from analysing the IQR. Fig. 3a and 3b show a very thin IQR band for fever and cough reduction in indomethacin patients, along with a small error bar, compared to paracetamol patients. This clearly shows that indomethacin is independent of the patient profile. A marginally broader IQR brand in myalgia may indicate the subjective nature of relief.
The results are similar to our earlier study on propensity score matching [21]. In that study, the median time for becoming afebrile, cough reduction, and myalgia relief in the indomethacin arm was four, three, and four days, respectively. However, the median in the paracetamol arm was seven and eight and 6.5 days, respectively.
We monitored CRP on admission and discharge. Indomethacin is very effective in reducing CRP in patients with higher CRP levels on admission (> 41 mg/L). The R2 value for indomethacin (0.85) was much higher compared to paracetamol (0.1). Thus, we can conclude that the consistency of indomethacin in reducing inflammation is very high.
A fourteen-day follow-up further revealed the efficacy of the drug. In the indomethacin arm, nearly 50% patients had fully recovered compared to 28% in the paracetamol arm. Patients who took indomethacin complained of tiredness. Many of these patients had returned to work. Only 14 % of the patients had Myalgia while 10% complained of joint pain. On the other hand, in the paracetamol arm, the recovery was slower with 47% complaining of myalgia, 48% of tiredness, 39% of joint pain and 33% complaining of other ailments.
Alkotaji et.al. [29] had hypothesised the importance of indomethacin in reducing cough and myalgia through its inhibitive action on bradykinin and the mechanism and ill-effects of bradykinin are well documented. The theory proposed in this study explains the difference in symptomatic relief between the two groups.
We had hypothesised that early symptomatic relief is important for recovery and prevents desaturation. 17 of the 20 patients who desaturated had fever beyond seven days and eleven had cough beyond seven days. The fourteenth-day state of the patients also reflected this.
The viral load reduction was better for indomethacin. However, the difference was not significant. Seven days may be too early for an RT-PCR test.
4.1. Limitation of the Study
The limitation of the study is that indomethacin was administered with standard care and not as a stand-alone treatment. With this result, indomethacin may be tried as a stand-alone treatment. This is not a double blinded study. The trial involved only hospitalised patients and not under home isolation.
5.0. Conclusions
The use of indomethacin alongside standard treatment protocol in hospitalised Covid-19 patients was associated with marked symptomatic relief and improved oxygen saturation level. We did not observe any adverse effects.
Data Availability
All data are available and can be obtained with ethics committee clearance
Conflict of Interest
We have read and understood BMJ policy on declaration of interests and declare that we have no competing interests.
Funding
Funding for this study was provided by Mr. Kris Gopalakrishnan, Alumnus of the Indian Institute of Technology Madras. He is also the Chairman of Axilor Ventures. He did not participate in the study in anyway.
Contributors
Rajan Ravichandran : Conceptualised the study, analysed the data, revised the paper
Surapaneni Krishna Mohan : Monitored the data collection for the whole trial.
Suresh Kumar Sukumaran : Monitored the data collection for the trial and is the guarantor of the data
Devakumar Kamaraj : monitored data collection for the whole trial
Sumetha Suga Daivasuga : In charge of all tests in the trial
Samson Oliver Abraham Samuel Ravi : collected samples and conducted tests
Sivakumar Vijayaraghavalu : Initiated the collaborative project, designed data collection tools, revised the paper
Ramarathnam Krishna Kumar : wrote the statistical analysis plan, analysed the data, drafted and revised the paper.
Acknowledgement
The authors acknowledge the generous funding for this study by Mr. Kris Gopalakrishnan, Alumnus, Indian Institute of Technology Madras.
The authors acknowledge the help of Mr. Kumar and Ms. Jeniffer in assisting the smooth conduction of the trial
Footnotes
The paper has been rewritten fro better clarity
References



