
Abstract
To allow a return to a pre-COVID-19 lifestyle, virtually every country has initiated a vaccination program to mitigate severe disease burden and control transmission; over 3.6 billion vaccine doses have been administered as of July 2021. However, it remains to be seen whether herd immunity will be within reach of these programs, especially as more transmissible SARS-CoV-2 variants continue to emerge. To address this question, we developed a data-driven model of SARS-CoV-2 transmission for Shanghai, China, a population with low prior immunity from natural infection. We found that extending the vaccination program to individuals aged 3-17 years plays a key role to reach herd immunity for the original SARS-CoV-2 lineages. With a vaccine efficacy 74% against infection, vaccine-induced herd immunity would require coverages of 93% or higher. Herd immunity for new variants, such as Alpha or Delta, can only be achieved with more efficacious vaccines and coverages above 80-90%. A continuation of the current pace of vaccination in China would reach 72% coverage by September 2021; although this program would fail to reach herd immunity it would reduce deaths by 95-100% in case of an outbreak. Efforts should be taken to increase population’s confidence and willingness to be vaccinated and to guarantee highly efficacious vaccines against more transmissible variants of concern.
Introduction
The first-wave of novel coronavirus disease 2019 (COVID-19) in China subsided quickly after the implementation of strict containment measures and travel restrictions starting in March 2020 1. As of July 21, 2021, the COVID-19 pandemic has caused over 191 million reported cases and 4.1 million deaths globally 2. The pandemic is far from over, as SARS-CoV-2 has undergone some significant mutations and a number of variants have become widespread due to increased transmissibility and/or immune escape characteristics – e.g., variants Alpha 3-5, Beta 6, Gamma 7, and Delta 8. After the original COVID-19 wave in early 2020, China has experienced several minor local outbreaks 9, including one detected in June 2021 in Guangdong Province caused by imported cases of Delta variant from India 10. To control this pandemic, a large share of the world needs to have immunity to SARS-CoV-2.
Effective vaccines against COVID-19 represent the most viable option to suppress SARS-CoV-2 transmission globally. The effectiveness of vaccination programs depends on several key factors, including vaccine supply, willingness to receive the vaccine, vaccine efficacy, and the age groups targeted by the vaccination effort. In China, home of about 1.4 billion people (∼18% of the world population), 1.5 billion doses have been administered as of July 20, 2021 11. This figure corresponds to 52.7% of the whole population and 68.6% of the target population (i.e., individuals aged 18 years and above). However, it remains to be seen if and when the vaccine coverage may reach a level sufficient to achieve herd immunity. Countries around the globe are facing the same question.
The classical herd immunity level is defined as 1-1/R0, where R0 is the basic reproduction number – the average number of infections generated by a typical infectious individual in a fully susceptible population 12. For a vaccine with efficacy VE that gives life-long protection, the level of herd immunity required to stop transmission is (1-1/R0)/VE. However, this estimate is an oversimplification of a complex phenomenon as it ignores the heterogeneities of actual human population (e.g., social mixing patterns, age-specific susceptibility to infection) 13,14 as well as of vaccination (e.g., lifelong immunity, sterilizing vaccine). To overcome this limitation, here we integrate contact survey data collected in Shanghai, China 15 as well as official demographic statistics of the Shanghai population, and develop an age-structured stochastic model to simulate SARS-CoV-2 transmission triggered by case importation (Fig.S1 in SI Appendix). We then use this model to evaluate whether herd immunity is achievable or not via mass vaccination and to explore the way forward to achieve suppression of SARS-CoV-2 transmission.
Results
Modeling SARS-CoV-2 transmission and vaccination
In the susceptible-infectious-removed SIR transmission model, we account for Shanghai-specific age structure, heterogeneous mixing patterns by age, and heterogeneous susceptibility to infection by age. The number of symptomatic cases, hospitalizations, ICU admissions, and deaths are then derived from estimated number of infections. A qualitative model description is reported in the Methods section, a summary of model parameters, and data sources is reported in SI Appendix Table S1. The model allows the explicit simulation of the vaccination strategy currently used in China: random distribution of vaccines to adults aged 18+ years (strategy 1). Two of the SARS-CoV-2 vaccines (i.e., CoronaVac and BBIBP-Corv) used in China have been licensed for children aged 3 to 17 years 16; however, as of July 21, 2021 children are not included among the target population for vaccination. To explore the contribution of vaccinating children aged 3-17 years to achieving herd immunity, we test two alternative strategies: i) same as strategy 1, but extended to individuals aged 3+ years starting from September 1, 2021 (strategy 2); ii) random distribution of vaccines to individuals aged 3+ years since the start of vaccination programs (strategy 3).
All individuals with vaccine contraindications or pregnant women (2.15% of the population) are excluded from the target population of the focus vaccination programs (see Sec. 4 of SI Appendix for details). The vaccine schedule requires two doses and VE is set at 73.5% against infection, in line with clinical trial data 17. In the baseline scenario, we assume that forty infected individuals 18 are introduced in the population on September 1, 2021, and R0=2.5 in the absence of interventions, as estimated for the historical SARS-CoV-2 lineage in China 19-22. This is an optimistic scenario for SARS-CoV-2 transmission in 2021; however we also present simulations corresponding to highly transmissible variants currently circulating globally, with R0 up to 6. We do not assume any social distancing in the main scenario, although we run sensitivity analyses with different levels of non-pharmaceutical interventions (NPIs).
The proportion of the population immune from natural infection is considered near 0% at the start of simulations. The number of vaccine doses administered per day (vaccination capacity) exponentially increases and is capped at 1.22% of the population (see Sec. 5 of SI Appendix for details). As of September 1, 2021, the projected vaccination coverage is 71.2% of the population (Fig.1A-C).
Baseline scenario
By forward simulating one year and assuming no vaccine hesitancy, continued vaccination efforts lead to a final coverage of 97.6% of the target population, which corresponds to 86.4% of the total population for strategy 1 and 95.6% for strategies 2 and 3 (Fig. 1A-C). Under any scenario, the mean incidence of newly infected individuals never reaches 20 over 10,000 residents (Fig. 1D-F). We estimated the impact of vaccination on reproduction number by using the next-generation matrix approach 23 (see Sec. 2-3 of SI Appendix for details). We estimated that the effective reproduction number at the time the infection is seeded (Re) is still well above the epidemic threshold, namely 1.72 (95%CI: 1.37-2.13), 1.73 (95%CI: 1.44-2.06), and 1.18 (95%CI: 1.17-1.19) for strategy 1-3, respectively. These estimates suggest that the vaccine coverage on September 1, 2021 is not enough to prevent onward transmission, regardless of the vaccination strategy. Re is estimated to cross the epidemic threshold (i.e., 1) on January 22, 2022, October 6, 2021 and September 16, 2021 for strategy 1, 2, and 3, respectively (Fig. 1G-I). Compared with strategy 1, with an infection attack rate of 5.54% (95%CI: 2.35-7.78%), strategy 2 and 3 are associated with infection attack rates lower than 4 per 100,000 (Fig.1J-L).

A Age-specific vaccine coverage over time for strategy 1. Vaccination program is assumed to be initiated on November 30, 2020 (i.e., the time that the vaccine doses administrated was first officially reported in China). The dotted lines correspond the start of epidemic. The inserted table shows the age-specific coverage for the two key time points (the start of epidemic (i.e., September 1, 2021), and the time that the coverage keeps constant (i.e., September 24), respectively). The line corresponds to the mean value, while the shaded area represents 95% quantile intervals (CI). B As A, but for strategy 2. C As A, but for strategy 3. D Daily incidence of new SARS-CoV-2 infections per 10,000 individuals for strategy 1 (mean and 95% CI). E As D, but for strategy 2. F As D, but for strategy 3. G Effective reproduction number Re over time (mean and 95% CI), as estimated using the Next-Generation matrix method from the time series of susceptible individuals for strategy 1. The shaded area in gray indicates the epidemic threshold Re =1. The numbers around the x-axis indicate when Re cross this threshold (i.e., January 22) for strategy 1. H As G, but for strategy 2. I As G, but for strategy 3. J Proportion of immune population due to either natural infection or vaccination over time for strategy 1. K As J, but for strategy 2. L As J, but for strategy 3.
Although vaccine-induced immunity is not enough to prevent viral circulation, all the scenarios considered are associated with substantial mitigation of COVID-19 burden. We estimate the infection attack rate for the three vaccination strategies to decrease by more than 90% with respect to a reference scenario with no interventions, with cumulative infection attack rates in the range of 554 to 0.12 per 10,000 individuals. Strategy 2-3 achieve the highest reduction (close to 100%) thanks to the inclusion of the age group 3-17 years in the target population of the vaccination program (Fig. 2A-B). Similar reductions are obtained also for other metrics of COVID-19 burden (e.g., hospitalized cases, individuals requiring an ICU; see Fig. S3 in SI Appendix). Nearly no difference in the reduction of overall number of deaths is observed among the three strategies (reduction close to 100%), with cumulative number of deaths no larger than 1 per 10,000 individuals. This pattern is explained by the substantially lower case fatality ratio in individuals 0-17 years (0.51%) compared to other age groups (Fig. 2C-D) 24.

A Cumulative number of infections per 10,000 individuals after 1 simulated year for reference scenario and three vaccination strategies (mean and 95% CI). Reference scenario indicates no vaccination and no NPIs with R0=2.5 at the beginning of transmission. Infections consist of unvaccinated and vaccinated individuals. The bar corresponds to the mean value, while the vertical line represents 95% quantile intervals. B Reduction in infections (mean and 95% CI) with respect to the reference scenario in different age groups and the total population. The reduction is defined as the estimated number of infections after 1 year since the introduction of the initial infected individuals under reference scenario minus the one under the vaccination strategy, relative to the estimated number under reference scenario. The 95% CI of the reduction may cross 0 as the burden between reference scenario and vaccination scenario is approximately the same in some simulations. We thus trimmed the lower limit of 95% CI at 0 through the manuscript. C As A, but for cumulative number of deaths. D As B, but for reduction in deaths.
These results were based on the assumption of an “all-or-nothing” vaccine (i.e., a vaccinated individual will either develop full protection with probability given by the vaccine efficacy or zero protection). To test the robustness of our findings to this assumption, we also tested a “leaky” vaccine (i.e., the susceptibility to infection of any vaccinated individual is reduced by a factor equal to the vaccine efficacy 25) and we obtained very consistent results with respect to the baseline analysis (Fig. S4 in SI Appendix). Moreover, the obtained results are confirmed when the initial number of seeds is varied in the range from 10 to 100 (Fig. S5 in SI Appendix), and when equal susceptibility to infection by age is assumed (Fig. S6 in SI Appendix). Finally, we also conducted a counterfactual analysis where we assume that a part of the population was already immune before the start of the vaccination campaign (similar to the situation in Western countries). Under this assumption, we found that a 10% initial immunity proportion would lead to Re below the epidemic threshold for strategy 3 before September 1, the start date of the simulations (Fig. S7 in SI Appendix).
As regard the parameters regulating the vaccination process, we found that the (overall) vaccine efficacy has the largest impact, followed by the vaccine efficacy of individuals aged 3-17 and 60+ relative to individuals aged 18-59 years (Fig. S8 and S9 in SI Appendix). On the other hand, the time between vaccination and maximum protection and the time interval between the first and second dose have a more moderate impact on the overall effectiveness of the analyzed vaccination strategies (Fig. S10 and S11 in SI Appendix).
Scenario 1: Delaying the start of the epidemic
The findings presented thus far suggest that herd immunity cannot be built through vaccination by September 1, 2021. Next, we test to what extent the start of a new epidemic wave needs to be delayed (e.g., by keeping strict restriction for international travels) to allow the immunity to build up in the population, potentially reaching herd immunity levels. According to the daily vaccine capacity used in the baseline scenario (based on the history of daily vaccination capacity data up to May 23, 2021), we estimate that Re remains above the epidemic threshold for strategy 1 even if the epidemic is delayed to November 1, 2021 (Fig. 3A and Fig. S12 in SI Appendix). However, simulation results show that for strategy 2 and 3 it is possible to decrease Re below the epidemic threshold when the epidemic start is delayed until after November 1, 2021-at that time, the vaccination coverage is estimated to reach 95.6%. In addition, in this case, strategies 2 and 3 lead to a higher reduction of the infection attack rate with respect to the scenario with no intervention (less than 0.4 per 100,000 individuals for an epidemic starting on November 1, 2021 - Fig. 3B-C). The estimated cumulative number of deaths is estimated to be reduced by more than 95% (Fig. S13 in SI Appendix).

A Estimated effective reproduction number (Re, mean and 95% CI) as a function of vaccine coverage at the time the infection is seeded (i.e., September 1, October 1 and November 1). Colors refer to the scenario of delaying the start of the epidemic to different date. The shaded area in gray indicates the herd immunity threshold Re =1. B Cumulative number of infections per 10,000 individuals after 1 simulated year for reference scenario and three vaccination strategies (mean and 95% CI). Reference scenario indicates no vaccination and no NPIs with R0=2.5 at the beginning of transmission. C Reduction in infections (mean and 95% CI) with respect to the reference scenario. D As A, but for the scenario of adopting different intensity of NPIs,  . E As B, but for the scenario of adopting different intensity of NPIs. F As C, but for the scenario of adopting different intensity of NPIs.
. E As B, but for the scenario of adopting different intensity of NPIs. F As C, but for the scenario of adopting different intensity of NPIs.
Scenario 2: Adopting NPIs in case of a new outbreak
The results presented so far suggest that herd immunity is not achievable at any time point without targeting also individuals 17 years old or younger (strategy 1). Adopting NPIs as a response to an epidemic outbreak can lower the transmission potential of the virus. It is thus worth investigating the synergetic effect of vaccination programs combined with NPIs of different intensity. It is important to note that we do not explicitly model every single measure to limit transmission (e.g., case isolation, contact tracing, wearing masks, social distancing, improved hygiene). These measures are implicit as concerted strategies that result in a decreased reproduction number. We define the value of the reproduction number in a fully susceptible population and under a certain level of NPIs as  . We explored
. We explored  in the range 1.1-2.3.
in the range 1.1-2.3.
The reproduction number on September 1, 2021 for strategy 1 and 2 can be reduced to below the epidemic threshold when  only, while strategy 3 can lead to a drastic decrease in Re, reaching herd immunity when
only, while strategy 3 can lead to a drastic decrease in Re, reaching herd immunity when  (Fig. 3D). By forward vaccinating and simulating 1 year of epidemic, substantial infections could be reduced thanks to the synergetic effect of vaccination and NPIs (Fig. 3E-F), with a reduction of more than 95% of deaths as compared with no intervention scenario (Fig. S15 in SI Appendix).
(Fig. 3D). By forward vaccinating and simulating 1 year of epidemic, substantial infections could be reduced thanks to the synergetic effect of vaccination and NPIs (Fig. 3E-F), with a reduction of more than 95% of deaths as compared with no intervention scenario (Fig. S15 in SI Appendix).
Scenario 3: Delaying the start of the epidemic and adopting NPIs
To further improve the potential for vaccination-induced herd immunity against the SARS-CoV-2 and reduce COVID-19 burden, here we tested the combination of the two scenarios mentioned above: delaying the start of the epidemic and adopting NPIs of different level of intensity in response to a new outbreak.
Should an epidemic start in mid-September 2021, herd immunity would be achievable only for strategy 3 (Fig. 4C). If the epidemic is further delayed to October 2021 and moderate NPIs are adopted, strategy 2 can succeed in blocking transmission (Fig. 4B). In the case of strategy 1 (i.e., the vaccination policy excluding underage individuals), strict NPIs should be adopted to prevent a major epidemic wave (Fig. 4A and Fig. S16-17 in SI Appendix).

A Estimated effective reproduction number (Re) as a function of  and epidemic start date for strategy 1. The bold line in black indicates the herd immunity threshold Re =1. B As A, but for strategy 2. C As A, but for strategy 3.
and epidemic start date for strategy 1. The bold line in black indicates the herd immunity threshold Re =1. B As A, but for strategy 2. C As A, but for strategy 3.
Herd immunity threshold
We explored the vaccination-induced herd immunity threshold in the absence of transmission by estimating Re under different fixed vaccine coverage. We estimated that Re decreases below 1.0 only for strategy 2 and 3 (Fig. 5A). The estimated herd immunity threshold under these two strategies is 92.8% and 80.8%, respectively, which suggests that level of immunity needed to lead the effective reproduction number below the epidemic threshold is lower if vaccination is extended to individuals aged 3-17 years early on. In particular, we estimated that for strategy 2 the required immunity level (92.8%) could be reached on October 5, 2021 (Fig.5B).
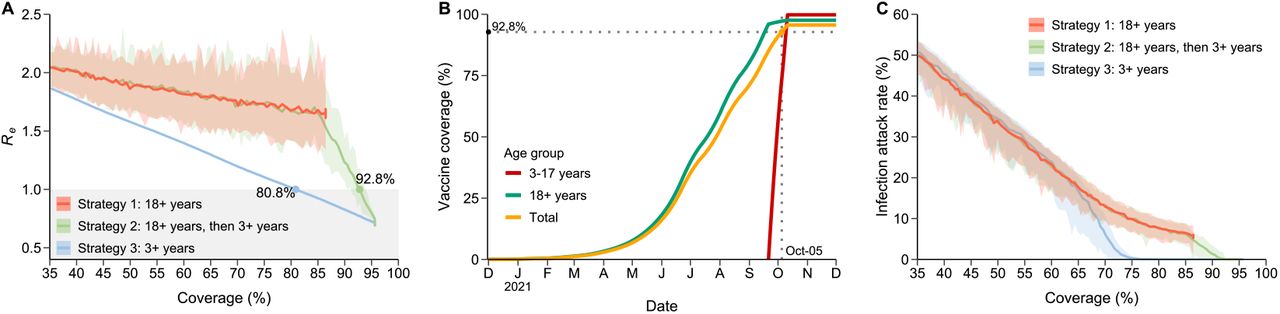
A Estimated effective reproduction number (Re, mean and 95% CI) as a function of vaccine coverage in the absence of transmission. Colors refer to three vaccination strategies. The shaded area in gray indicates the herd immunity threshold Re =1. The numbers around the line indicate where Re cross this threshold. B Age-specific vaccine coverage over time for strategy 2 in the absence of transmission. The crossed point of two dotted lines corresponds to the time the coverage reached the herd immunity threshold. C The infection attack rate after 1 simulated year as a function of vaccine coverage. The transmission is simulated with the initial vaccine coverage and there is no longer vaccination after the infection is seeded.
We also estimated the infection attack rate under different vaccination coverages under the assumption that vaccination stops at the time the epidemic is seeded. This purely hypothetical scenario shows that when the adult population (18+ years of age) is vaccinated (strategy 1), despite a fairly high estimated reproduction number (1.68), the estimated infection attack rate is relatively low (5.94%) (Fig. 5A and 5C). In fact, given the age-targeted vaccination program and the lack of natural immunity, the susceptible population is mostly concentrated in the young population. The high number of contacts in younger age groups, combined with the high vaccination coverage in the rest of the population, lead to a fairly high reproduction number but, at the same time, the infections are focused on a small segment of the population only (young individuals) and thus the overall infection attack rate remains fairly low.
The effectiveness of age-targeted vaccination strategies depend on the age-mixing patterns of the population 26. To test the robustness of our findings, we tested an alternative contact matrix for China 27 and we found consistent results (Fig. S18-19 in SI Appendix). In addition, to explore to what extent vaccine efficacy affects the herd immunity threshold, we estimate Re by increasing the efficacy against infection to 85% and 95%. Our results show that, although Re decreases, the results for strategy 1 and 2 are rather consistent with those obtained in the main analysis (Fig. S20 in SI Appendix). In contrast, for strategy 3 the threshold is estimated to be substantially lower 63.0% in the case of a 95% efficacious vaccine (Fig. S20 in SI Appendix).
SARS-CoV-2 variants
Given the global epidemiological situation of COVID-19 as of July 2021, it is likely that, should a major epidemic wave start to unfold in China, it will be caused by a SARS-CoV-2 variant. Four SARS-CoV-2 variants of concern (Alpha, Beta, Gamma, and Delta) are considered in our analysis, each of which is characterized by a specific transmissibility (Tab. S2 in SI Appendix). Moreover, given the uncertainty surrounding the estimates of vaccine efficacy against them, we explored VE in the range 60-100%.
Our results show that, for any of these four variants, herd immunity is unattainable for a vaccine with 73.5% efficacy as in the baseline scenario, even in the extreme case where the vaccine coverage is 100% (Fig. 6). Vaccine-induced herd immunity may only be achievable with higher VE and high coverage. For example, for a vaccine with 90% efficacy against the Alpha variant, more than 83% of the population would need to be vaccinated to reach herd immunity (Fig. 6). Similarly, for a vaccine 90% efficacious against Delta, herd immunity would require more than 92% of the population vaccinated (Fig. 6).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
A for Alpha strain with R0=4.0. B As A, but for Beta strain with R0=3.8. C As A, but for Gamma strain with R0=5.0. D As A, but for Delta strain with R0=6.0. The bold line in black indicates the herd immunity threshold Re =1. Re is estimated in the scenario that all individuals are eligible to vaccination and vaccinated 2 doses before the epidemic starts.
Discussion
Our study evaluates the feasibility of reaching herd immunity against SARS-CoV-2 through vaccination, considering heterogeneity in population age structure, age-specific contact patterns, vaccine efficacy, as well as biological characteristics of the historical SARS-CoV-2 lineages and variants. Our findings show the key role of extending the vaccination program to school-aged children in order to reach herd immunity. Considering the vaccination capacity in China in July 2021, an expansion of vaccination program to the population aged 3 years or more would achieve herd immunity against the original SARS-CoV-2 lineage by September, 2021. However, herd immunity is unlikely to be reached against new variants of concern. If we consider the transmissibility of the Delta variant, herd immunity would require vaccination of 87.5% of the whole population with a highly efficacious vaccine against infection (95% efficacy, which does not exist yet). The adoption of NPIs could prevent the spread of a major epidemic wave even when the herd immunity level is not reached, but such an option obviously entails social and economic costs. Further, all strategies considered in this study would mitigate the overwhelming majority of deaths.
Our study explored if and when vaccination-induced herd immunity can be reached in China. Under the hypotheses that the circulating strain has the same transmissibility as historical lineages and that the vaccination campaign will not slow down due to vaccine hesitancy, for a strategy targeting adults first, followed by individuals aged 3-17 years (strategy 2), herd immunity could be reached as early as mid-October 2021. However, should the vaccination program target individuals aged 18 years or more only (strategy 1), herd immunity seems to remain an unreachable target given that about 14% of the Chinese population would be excluded from the program (either because of age or other forms of non-eligibility). This finding is consistent with a previous study reporting that herd immunity may only be possible if the vaccination program is extended to children 28. Nonetheless, it is important to remark that the effectiveness of the vaccination program is impacted both by the natural immunity accumulated in the population (which is close to 0 in China as of July 2021) and the age structure of the population. In fact, in populations with a lower proportion of children, herd immunity may be achievable through vaccination of adults only.
Our findings point to the importance of adopting NPIs and/or self-precautionary measures until herd immunity is reached, or the burden of the epidemic becomes manageable. These measures can either help delay the seeding of the infection (e.g., strict border control measures) or, should an epidemic start to unfold, to mitigate its burden (e.g., social distancing, contact tracing, testing, wearing masks, hygiene practices, limiting contacts). However, questions remain about which NPIs need to be implement, their intensity, and timing. Future studies are needed to address these questions.
A key role to determine whether herd immunity can be reached is played by the willingness-to-vaccine of the population. According to previous surveys on COVID-19 vaccine hesitancy, vaccine acceptance in China was estimated to vary between 60.4% and 91.3% for general population aged 18 years and above 29-32, and may be even lower for older adults 32 and healthcare workers 33. Similar estimates were obtained for several other countries including the UK (71.5%) 34 and the US (75.4%) 34. Given these levels of vaccine hesitancy, achieving high levels of coverage may remain an elusive target. Efforts to increase population’s confidence and willingness to be vaccinated will thus be of paramount importance to allow a return to a pre-COVID-19 lifestyle. Our study shows that the spread of new more transmissible (and possibly also more lethal 35-42) variants substantially increases herd immunity thresholds to level that may not be feasible in any population, so that mitigation strategies become much more relevant.
Previous studies have estimated the herd immunity threshold either through natural infection or vaccination under the assumption of an homogenously mixed population 28,43-46, but heterogeneity in contact structure, age structure of the population, susceptibility to infection by age, and order in which individuals are vaccinated are all key factors shaping the herd immunity level 14,47,48 The developed model is based on social mixing patterns estimated for the Shanghai population 15 and on China-specific data on COVID-19 epidemiology (population immunity, hospitalization rates 24, case fatality ratio 24, etc.). Nevertheless, the introduced modeling framework is flexible and can be tailored to other countries We tested a scenario close to the situation in the USA, where initial fraction of naturally immune population is set to 22% 49 and a BNT162b2/Pfizer vaccine with 95% VE 50 is considered. The results show that the initial (natural) immunity level in the population and the use of a more efficacious vaccine may theoretically ease the path towards reaching herd immunity (Fig. S21 in SI Appendix), although the spread of the Delta variant may counterbalance these effects making it virtually impossible to reach herd immunity. Moreover, vaccination hesitancy may jeopardize the vaccination effort in the US and other Western countries as well.
This study is prone to the limitations pertaining to modeling exercises. First, VE for children have not been estimated for the vaccines in use in China; therefore, we have assumed the same VE as in adults based on immunogenicity studies 51. Given such a lack of field evidence, we have conducted a sensitivity analysis where a lower vaccine efficacy is assumed for children. The overall conclusions of the study do not change. Still, further data on age-specific vaccine efficacy could help refine the obtained estimates.
Second, we assumed that immunity induced either from infection or vaccination lasts more than the time horizon considered in the simulations (i.e., 1 year). There are both evidence from laboratory studies and the field suggesting that the protection lasts several months 52-54. Despite these preliminary pieces of evidence, the duration of the immunity remains a research area of paramount importance and intrinsically linked to viral evolution. It is also possible that waning immunity will continue to provide protection against severe disease but only partial against infection or transmission, which affects the herd immunity threshold. Overall, the duration and quality of immunity will determine the periodicity of COVID-19 outbreaks globally 55,56.
Third, in the baseline scenario, we referred to an inactivated SARS-CoV-2 vaccine (BBIBP-CorV) taken to be 73.5% efficacious against infection 17. However, several other vaccines (including CoronaVac, WBIP-CorV, Ad5 nCoV, and ZF2001) are licensed and have been used in China 57-60. We varied vaccine efficacy in the range 60%-84% in sensitivity analyses. The main conclusion about the need to extend the vaccination campaign to children is unaltered.
In conclusion, based on the current evidence, reaching vaccine-induced herd immunity in a population with little/no natural immunity is challenging. Key steps will be the authorization of COVID-19 vaccines for children and minimize vaccine hesitancy. These, together with highly efficacious vaccines, will be even more crucial given the global spread of SARS-CoV-2 variants with higher transmission potential than the historical lineages. Importantly, even if herd immunity is unlikely to be reached, vaccination will still dramatically reduce COVID-19 burden.
Methods
SARS-CoV-2 transmission and vaccination model
We built a compartmental model of SRAS-CoV-2 transmission and vaccination, based on an age-structured stochastic SIR scheme, accounting for heterogeneous contact patterns by age as estimated in Shanghai 15 and heterogeneous susceptibility to infection by age as estimated using contact tracing data in Hunan province of China 61. In the model, the population is divided into three epidemiological categories: susceptible, infectious, and removed, stratified by 17 age groups. Susceptible individuals can become infectious after contact with an infectious individual according to the age-specific force of infection. The rate at which contacts occur is determined by the mixing patterns of each age group. The average generation time was set to 7 days 61. We consider a basic reproductive number (R0) of 2.5 according to estimates for the historical SARS-CoV-2 lineages in China 19-21,62. Higher values (in the range 3.8-6) are used when other variants of concern are modeled 35-42. Simulations are initiated with 40 infectious individuals, corresponding to the number of cases first detected in a local outbreak in Beijing on June 11, 2020 63.
We consider a 2-dose vaccine, that only susceptible individuals are eligible for vaccination (we recall that natural immunity is close to 0 in China as of July 2021), and that the duration of vaccine-induced immunity lasts longer than the time horizon considered in this study (i.e., 1 year). Details about the model are reported in Sec. 1 of SI Appendix.
Baseline vaccination scenario
As the baseline scenario, we considered the following assumptions:
Epidemic start: An epidemic is assumed to be triggered by forty SARS-CoV-2 infections on September 1, 2021; vaccines have been rolling out in China since November 30, 2020 64.
Vaccination strategy: We test three different vaccination strategies:
Strategy 1—random distribution of vaccines to adults aged 18+ years
Strategy 2—same as strategy 1, but the vaccination is extended to individuals aged 3+ years starting from September 1, 2021
Strategy 3—random distribution of vaccines to individuals aged 3+ years since the start of the vaccination program.
Note that in all scenarios, we consider that a fraction of the population (about 2% - Sec. 4 of SI Appendix) is not eligible to receive the vaccine (e.g., pregnant women, individuals with allergies or other conditions preventing them to safely receive the vaccine).
Vaccine capacity: We simulated the daily vaccine administration capacity based on the vaccine capacity data throughout the entire vaccination campaign in China 65. We found that the daily vaccine administration capacity exponentially increased during the initial phase of the campaign before stabilizing at 294,234 doses per day on June 2, 2021 for the Shanghai population (about 24 million individuals; details are reported in Sec. 5 of SI Appendix).
Vaccine efficacy (VE): There are three types of COVID-19 vaccines currently used in China: inactivated, recombinant protein subunit, and adenovirus-vectored vaccines. Their VE was estimated to vary from 65% to 84%, except for the one tested in Brazil (VE=50%) where Gamma variant was dominant at the time of the trial 66-71. We assume 73.5% VE against infection for a two-dose schedule (with a 21-day interval) 17 and explore 60%-84% VE as sensitivity analysis. We also test a two-dose schedule with a 14-day interval. In addition, COVID-19 vaccines may not be equally effective across age groups in preventing infection or disease. To understand the impact of this assumption, we also tested a relative VE of 50% and 75% for individuals aged 3-17 and 60+ years as compared to VE for individuals aged 18-59 years.
Vaccine action: We considered two ways in which VE could be below 100%: an “all-or-nothing” vaccine (baseline analysis), in which the vaccine provides full protection to a fraction VE of individuals who are vaccinated and no protection to the remaining 1-VE vaccinated individual. The second option we considered is a “leaky” vaccine in which all vaccinated individuals have a certain level of protection to the infection corresponding to VE.
Initial immunity: As of July 2021, there is essentially no population immunity from natural infection in China 72. For the sake of generalizability of results to other countries with ongoing transmission, we have explored a scenario where 30% of the population has initial natural immunity 49.
Susceptibility to infection by age: Children under 15 years of age were estimated to have a lower susceptibility to SARS-CoV-2 infection as compared to adults (i.e., individuals aged 15 to 64 years), while individuals aged 65+ years had the highest susceptibility to infection 61.
Immunity duration: We let the transmission model run for one year, assuming a life-long protection from natural infection or vaccination.
Comprehensive sensitivity analyses to evaluate the impact of the baseline assumptions on our results are carried out as well (Tab. S1 in SI Appendix).
Alternative vaccination scenarios
We test three alternative scenarios to explore the potential for vaccination-induced herd immunity, where: i) epidemic start is delayed from September 1, 2021 to October 1, 2021, and November 1, 2021; ii) the initial reproduction number varies between 1.1 and 2.3 to account for different intensity of NPIs  ; iii) combinations of scenarios i and ii.
; iii) combinations of scenarios i and ii.
SARS-CoV-2 variants
Multiple SARS-CoV-2 variants have been documented globally, four of which are of particular concern: Alpha, Beta, Gamma, and Delta 73. These variants are estimated to have higher transmissibility 3,6,8,42 and possibly an increased mortality 74,75. To assess the potential for herd immunity in this context, we consider a R0 in the range 3.8-6 (Tab. S2 in SI Appendix).
Data analysis
For each scenario, 100 stochastic simulations were performed. The output of these simulations determined the distribution of the number of infections. We then analyzed model outcome to estimate the number of symptomatic infections, hospitalizations, ICU admissions, and deaths by accounting for the transition probability between different endpoints (Tab. S1 in SI Appendix). For vaccinated individuals, the estimates of disease burden also account for estimates of vaccine efficacy against different clinical endpoints (e.g., symptomatic case, hospitalization, ICU admission, death). Details are reported in Sec. 1 in SI Appendix. We defined 95% credible intervals as quantiles 0.025 and 0.975 of the estimated distributions.
We used the next-generation matrix approach to estimate the reproduction number, Re. Herd immunity is considered as achievable when Re <1. Details are reported in Sec. 2-3 in SI Appendix.
Data Availability
The availability of all data can be addressed to the correspondence author.
End notes
Author Contributions
H.Y. conceived and designed the study. H.Y. and M.A. supervised the study. M.A. designed the model. H.L. developed the model. H.L., J.Z., J.C., J.Y., X.D. analyzed the model outputs. H.L., C.P., X.D, and Z.C. prepared the tables and figures. H.L. and J.Z. prepared the first draft of the manuscript. W.Z. and Q.W. participated in data collection. X.C and Z.C. updated the relative literatures. H.Y., M.A. W.Z. and C. V. revised the content critically. All authors contributed to review and revision and approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Declaration of interests
H.Y. has received research funding from Sanofi Pasteur, GlaxoSmithKline, Yichang HEC Changjiang Pharmaceutical Company, and Shanghai Roche Pharmaceutical Company. M.A. has received research funding from Seqirus. None of those research funding is related to COVID-19. All other authors report no competing interests.
Disclaimer
This article does not necessarily represent the views of the NIH or the US government.
Acknowledgments
The study was supported by grants from the National Science Fund for Distinguished Young Scholars (No. 81525023), European Union Grant 874850 MOOD (MOOD 000), and the National Institute for Health Research (NIHR) (grant no. 16/137/109) using UK aid from the UK Government to support global health research. We also acknowledge grant from Shanghai Key Laboratory of Infectious Diseases and Biosafety Emergency Response (20dz2260100). The views expressed in this publication are those of the author(s) and not necessarily those of the NIHR or the UK Department of Health and Social Care.
Reference



