
Abstract
Importance COVID-19 vaccine hesitancy has become a leading barrier to increasing the US vaccination rate.
Objective To evaluate time trends in COVID-19 vaccine intent during the US vaccine rollout, and identify key factors related to and self-reported reasons for COVID-19 vaccine hesitancy in May 2021.
Design, Participants and Setting A COVID-19 survey was offered to US adult Facebook users in several languages yielding 5,088,772 qualifying responses from January 6 to May 31, 2021. Data was aggregated by month. Survey weights matched the sample to the age, gender, and state profile of the US population.
Exposure Demographics, geographic factors, political/COVID-19 environment, health status, beliefs, and behaviors.
Main Outcome Measures “If a vaccine to prevent COVID-19 were offered to you today, would you choose to get vaccinated.” Hesitant was defined as responding, probably or definitely would not choose to get vaccinated (versus probably or definitely would, or already vaccinated).
Results COVID-19 vaccine hesitancy decreased by one-third from 25.4% (95%CI, 25.3, 25.5) in January to 16.6% (95%CI, 16.4, 16.7) in May, with relatively large decreases among participants with Black, Pacific Islander or Hispanic race/ethnicity and ≤high school education. Independent risk factors for vaccine hesitancy in May (N=525,644) included younger age, non-Asian race, <4 year college degree, living in a more rural county, living in a county with higher Trump vote share in the 2020 election, lack of worry about COVID-19, working outside the home, never intentionally avoiding contact with others, and no past-year flu vaccine. Differences in hesitancy by race/ethnicity varied by age (e.g., Black adults more hesitant than White adults <35 years old, but less hesitant among adults ≥45 years old), and vice versa. Almost half of vaccine hesitant respondents reported fear of side effects (49.2% [95%CI, 48.7, 49.7]) and not trusting the COVID-19 vaccine (48.4% [95%CI, 48.0, 48.9]); over one-third reported not trusting the government, not needing the vaccine, and waiting to see if safe. Reasons differed by degree of vaccine intent and by race/ethnicity.
Conclusion COVID-19 vaccine hesitancy varied by demographics, geography, beliefs, and behaviors, indicating a need for a range of messaging and policy options to target high-hesitancy groups.
Introduction
On December 11, 20201, the Federal Drug Administration (FDA) granted the first Emergency Use Authorization of a COVID-19 vaccine2. By March 2021, 3 COVID-19 vaccines had been authorized in the US3, and the president announced procurement of enough doses for every adult to be vaccinated by the end of May 20214. By May 2021, vaccine eligibility was expanded to everyone covered under the FDA authorizations (initially ≥16 years old, expanded to ≥12 years old on May 105), and efforts to increase vaccine access to underserved populations were underway6,7. However, COVID-19 vaccine hesitancy (i.e., a refusal or reluctance to be vaccinated) slowed vaccination uptake8. By July 2021, vaccine hesitancy was widely perceived by the public as prolonging the pandemic; on August 1, it was the subject of a New York Times front-page story9, and was center-stage to disease control discussions as a fourth COVID-19 surge filled hospitals across parts of the US10,11.
A longitudinal study of US adults (N=7,420) by Daly et al. reported an overall decrease in COVID-19 vaccine hesitancy from 46.0% in October 2020 to 35.2% in March 2021, with larger decreases in adults with Black and Hispanic versus White race/ethnicity12, thereby reducing but not eliminating the racial disparity in COVID-19 vaccine hesitancy. However, how COVID-19 vaccine hesitancy has changed up through the time of adult universal eligibility, overall and among subgroups, as well as reasons for hesitancy at the time of universal eligibility deserves further study.
Among a massive sample of US adults, we report COVID-19 vaccine uptake and intent by month, January-May, 2021, and evaluate time trends by race/ethnicity, education, US region and political environment. For May, the prevalence of COVID-19 vaccine hesitancy is reported by demographics, geographic factors, political/COVID-19 environment, health status, beliefs and behaviors, and associations between each potential risk factor with hesitancy is estimated with and without adjustment for potential confounders. Lastly, we identify the most common reasons for COVID-19 vaccine hesitancy by level of COVID-19 vaccine intent and race/ethnicity.
Methods
Sampling and Weighting
Since April 2020, the Delphi Group at Carnegie Mellon University (CMU) has been conducting a national COVID-19 Trends and Impact Survey (CTIS)13 in collaboration with Facebook Data for Good. Each month, CTIS is offered to a random sample, stratified by geographic region, of ≈100 million US residents from the Facebook Active User Base who use one of the supported languages (English [American and British], Spanish [Spain and Latin American], French, Brazilian Portuguese, Vietnamese, and simplified Chinese). The offer to participate is shown with a link to the survey at the top of users’ Facebook News Feed, from once a month to once every six months, depending on their geographic strata, with the intent to yield ≈1.1 million responders monthly, which allows for evaluation of local trends. When individuals click through the link, an anonymized unique identifier is generated. CMU returns the unique IDs to Facebook, which creates weights that account for the sampling design and non-response; these weights are then post-stratified to match the US general population by age, gender, and state14. The design ensures CMU researchers do not see user names or profile information, and Facebook does not see survey microdata. The CMU Institutional Review Board approved the survey protocol and instrument (STUDY2020_00000162).
Study sample
The survey has been updated (via edits to existing questions as well as removal and addition of questions) periodically since its inception. The same version of the vaccine uptake and intent questions were offered to all potential respondents from January 6 to May, 19, 2021, and to approximately 15% of potential respondents from May 20-31. This study is limited to responses from these offers (5,088,772 survey responses from participants who completed the survey at least once January 6 to May 31, 2021). Data was aggregated by month to evaluate time trends in COVID-19 vaccine uptake and intent. There may be repeat respondents across months; however, respondents cannot be linked longitudinally, so data was treated as repeat cross-sectional surveys. To be included in the analysis sample, participants had to complete the questions on vaccine uptake and intent, and report a gender other than “prefer to self-describe.” This exclusion was made after discovering that the majority of fill-in responses for self-described gender were political/discriminatory statements or otherwise questionable answers (e.g. Apache Helicopter or Unicorn), and that as a group, those who selected self-described gender (<1% of the sample) had a high frequency of uncommon responses (e.g., Hispanic ethnicity [41.4%], the oldest age group [23.2% ≥75 years] and highest education level [28.1% Doctorate]), suggesting the survey was not completed in good faith.
We used the most recent month’s data (May 2021) to assess how demographics, geographic factors, political/COVID-19 environment, health status, beliefs and behaviors relate to COVID-19 vaccine hesitancy. In May 2021, 66,138,989 Facebook users were offered the survey used in this analysis, of whom 562,572 completed at least part of the survey (criteria for screening), and 529,658 answered the questions on vaccine uptake and intent. After excluding self-described gender, the May analysis sample included 525,644 respondents. Applying the same criteria, the January, February, March, and April samples had 1,195,650; 1,142,195; 1,209,536; and 1,015,747 participants, respectively (see eTable 1 for study flow by month).
Measures
The survey questions and response sets utilized in this report are provided in the eAppendix. Vaccination questions were adapted from CDC-sponsored questions developed for two household panel surveys15 and shared with us prior to launch. The answer set for reasons for vaccine hesitancy, which appears to be a distinct phenomenon from general vaccine hesitancy, was also expanded through a review of media reports and brainstorming sessions among survey methodologists. We categorized participants as vaccine hesitant if they answered that they probably or definitely would not choose to get vaccinated “if a vaccine to prevent COVID-19 were offered to you today” (versus probably or definitely would choose to get vaccinated or were already vaccinated). Those who had already received a COVID-19 vaccine were coded as not hesitant to ensure a consistent study population, as access to vaccinations varied by state and month in the studied timeframe.
The question on gender was developed for this survey; other demographic questions (age, race, ethnicity, education, employment status) were adapted from existing surveys: race and ethnicity from the 2020 Census16, age categories match the 10-year blocks reported by the American Community Survey (ACS)17, and education categories were adapted from ACS18. Participants who reported Hispanic ethnicity were categorized by ethnicity. Non-Hispanic participants were categorized by their race; non-Hispanic participants who reported more than one race were categorized as multi-racial. Participants who did not select one of the named races were categorized as missing. The “less than high school” and “high school graduate or equivalent” categories were combined as “≤high school.” Likewise, “some college” and “2 year degree” were combined as “some college.”
County-level variables were created using participants reported zip code: US region (i.e., Census Bureau statistical region19, dividing West into Mountain and Pacific); urban-rural level of metropolitan statistical area classification20; and several political/COVID-19 environment indicators: quartile of county COVID-19 death rate in the previous month (April 2021)21, quartile of county Trump vote share in the 2020 presidential election (calculated as percent voted for Trump minus percent voted for Biden out of total votes within a county; not available for Alaska)22 and state governor’s political party (not available for US territories)23.
Questions related to health status, beliefs and behaviors included ever having tested positive for COVID-19, ever diagnosed with specific health conditions (asthma, autoimmune disorder, cancer, chronic obstructive pulmonary disease, diabetes type 1, diabetes type 2, heart disease, high blood pressure, kidney disease, and weakened/compromised immune system), the extent of worry about self or family becoming seriously ill from COVID-19, living with someone age 65 years or older, past-year flu vaccination, and the extent of intentionally avoiding contact with others. Participants were categorized as having no health conditions or at least one health condition. Additionally, participants were categorized as having high blood pressure only, each of the other health conditions with or without high blood pressure, or “multiple conditions,” defined as at least two conditions excluding high blood pressure, which was relatively common and has limited support as a risk-factor for COVID-1924.
Statistical analysis
All estimates were generated using survey weights25. We calculated percentages of COVID-19 vaccine intent by month, as well as first-last month differences, for the full sample and by race/ethnicity, education, US region, and county Trump support. We limited the race/ethnicity comparison to adults 18-34 years due to an interaction between race/ethnicity and age (reported below with May data), and because hesitancy is higher among younger versus older adults.
Among the May sample, we calculated percentages of COVID-19 vaccine hesitancy by all covariates and used a series of weighted Poisson regression models to estimate the risk ratios (RR) for vaccine hesitancy for each variable. To enable model fitting with an interaction term for age and race, where age data was missing but race/ethnicity was available, race/ethnicity was recoded to missing in the May sample. This affected 70 Hispanics, 262 Whites, 46 Blacks, 13 Asians, 15 Native Americans, 1 Pacific Islanders, and 30 multi-racial respondents (0.08% of our sample). Adjusted risk ratios (aRR) were estimated from a single Poisson regression model including all covariates and an interaction term for age group and race/ethnicity. In a second multivariable model, a simplified health conditions variable (none, at least one, described above) was replaced with the version specifying specific conditions to estimate aRR by health condition. Among hesitant participants we calculated percentages of each reason for hesitancy by 3 levels of vaccine intent (definitely no, probably no, and probably yes), and by race/ethnicity. For all parameters, 95% confidence intervals (CI) were calculated using robust standard errors.12 Analyses were conducted in R (Version 4.0.2, R Core Team, Vienna, Austria).
Results
Participant characteristics
Excluding missing responses, weighted May participants had a median age range of 55-64 years; 45.7% identified as male, 53.2% female, 1.1% nonbinary; 16.4% were Hispanic, 69.1 % White, 6.5% Black, 3.6% Asian, 0.8% Native American, 0.24% Pacific Islander, and 3.3% were multi-racial; 22.5% had ≤high school education; 41.0% ≥four-year college degree. Over half (56.0%) worked for pay; 42.9% worked outside the home. Demographics were similar January through April (data not shown).
COVID-19 vaccine receipt and intent over time
Hesitancy decreased each month, with a one-third decrease from 25.4% (95%CI 25.3,25.5) in January to 16.6% (95% CI, 16.4,16.7) in May, 2021. There was a bigger decrease in percentage points in the response “probably not” (−7.1%[95% CI -7.2, -6.9]) versus “definitely not” (−1.8% [95% CI -1.9, -1.7]) (Figure 1; eTable 2).
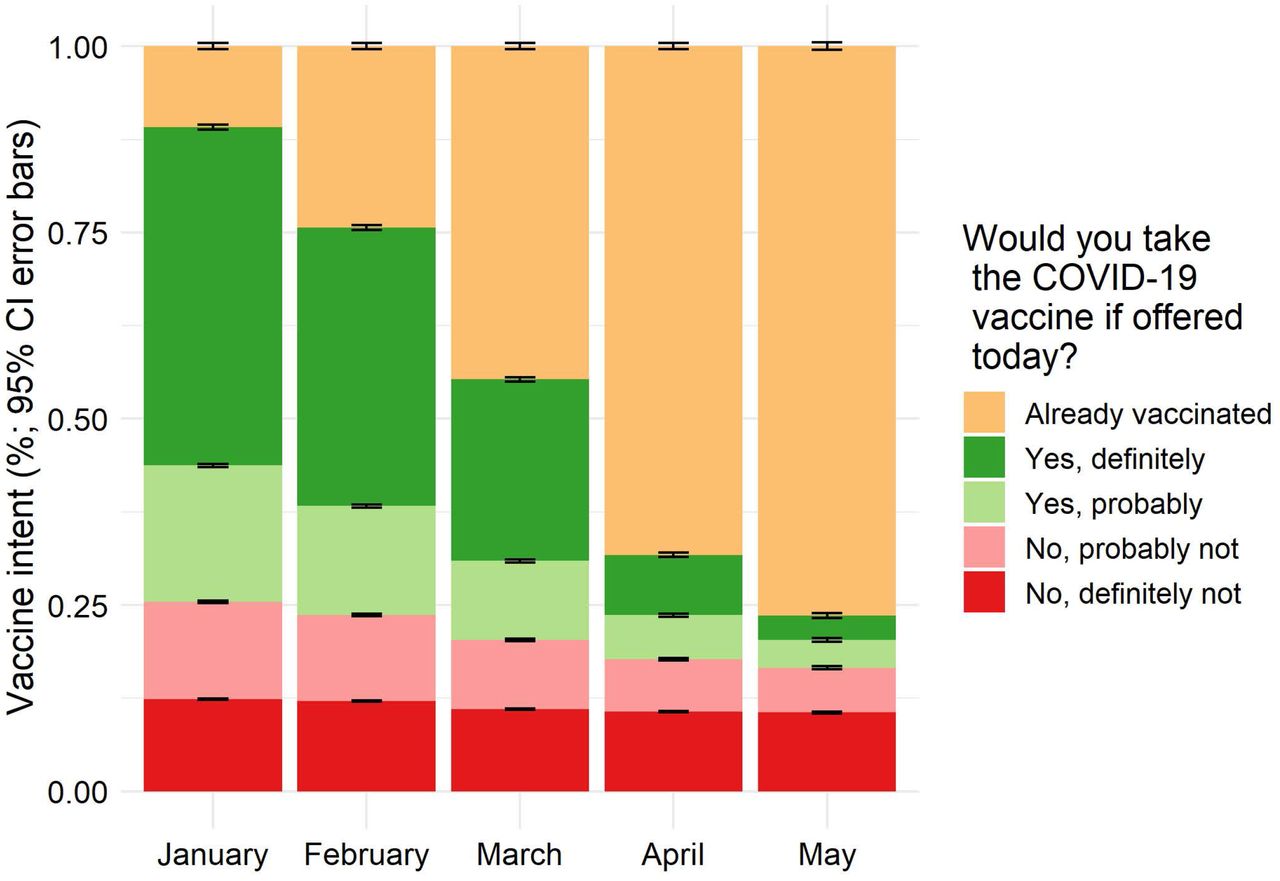
COVID-19 vaccine receipt and intent among US adults by month (January-May, 2021) Vaccine hesitancy decreased among adults each month from January to May, mostly due to a decrease in the response, “probably not” (−7.1 percentage points (%) [95% CI -7.2, -6.9]) versus “definitely not” (−1.8 % [95% CI -1.9, -1.7]).
Per Figure 2, from January to May the gap in percent hesitant between race/ethnicity groups among younger adults (panel A) and education levels among all respondents (panel B) decreased, with the biggest decreases among two of the three most hesitant race/ethnicity groups (e.g., Black and Pacific Islander but not Native American) and the two most hesitant education groups (≤high school and some college education) in January. Hesitancy appeared relatively constant among those with a professional degree (e.g. MD, JD) or Doctorate. Decreases in percent hesitant over time were fairly similar across US regions (panel C), with a slightly smaller decrease in the Mountain region and slightly larger decrease in the South. The gap in percent hesitant by Trump vote share increased slightly from January to May, with the highest quartile, which was the most hesitant group, having the smallest decrease (panel D). Supporting data is provided in eTable 3.

COVID-19 vaccine hesitancy by race/ethnicity (ages 18-34 yearsa), education level, US region and county Trump vote share in the 2020 presidential election among US adults by month (January-May, 2021)
Between January and May, the gap in percent hesitant between race/ethnicity groups among adults 18-34 years (panel A) and education levels among all ages (panel B) decreased, with the biggest decreases among the most hesitant groups (e.g., Black race and ≤high school education, respectively). Changes in percent hesitant over time were fairly similar across US regions (panel C); however, there was a slightly smaller decrease in the Mountain region and slightly larger decrease in the South versus other regions. The gap in percent hesitant by county political environment, quantified in quartiles of percent Trump vote share in the 2020 presidential election, increased slightly between January and May, with the most hesitant group (highest quartile) having the smallest decrease (panel D).
Factors related to COVID-19 vaccine hesitancy
Hesitancy in May, 2021 is reported by participant demographics and geographic factors in Table 1 (N=525,644). Although hesitancy was lower in females versus males (RR 0.79, 95% CI 0.78, 0.81), with adjustment for covariates (i.e., variables reported in Tables 1 and 2), female gender was associated with higher hesitancy (aRR 1.12, 95%CI 1.10, 1.14). Non-binary adults had similar hesitancy to males (RR 1.10, 95%CI, 0.97, 1.22; aRR 0.99, 95%CI 0.88, 1.10).
COVID-19 vaccine hesitancy in May 2021 by demographics among US adults (N=525,644)
COVID-19 vaccine hesitancy in May 2021 by political/ COVID-19 environment, health status, beliefs and behaviors among US adults (N=525,644)
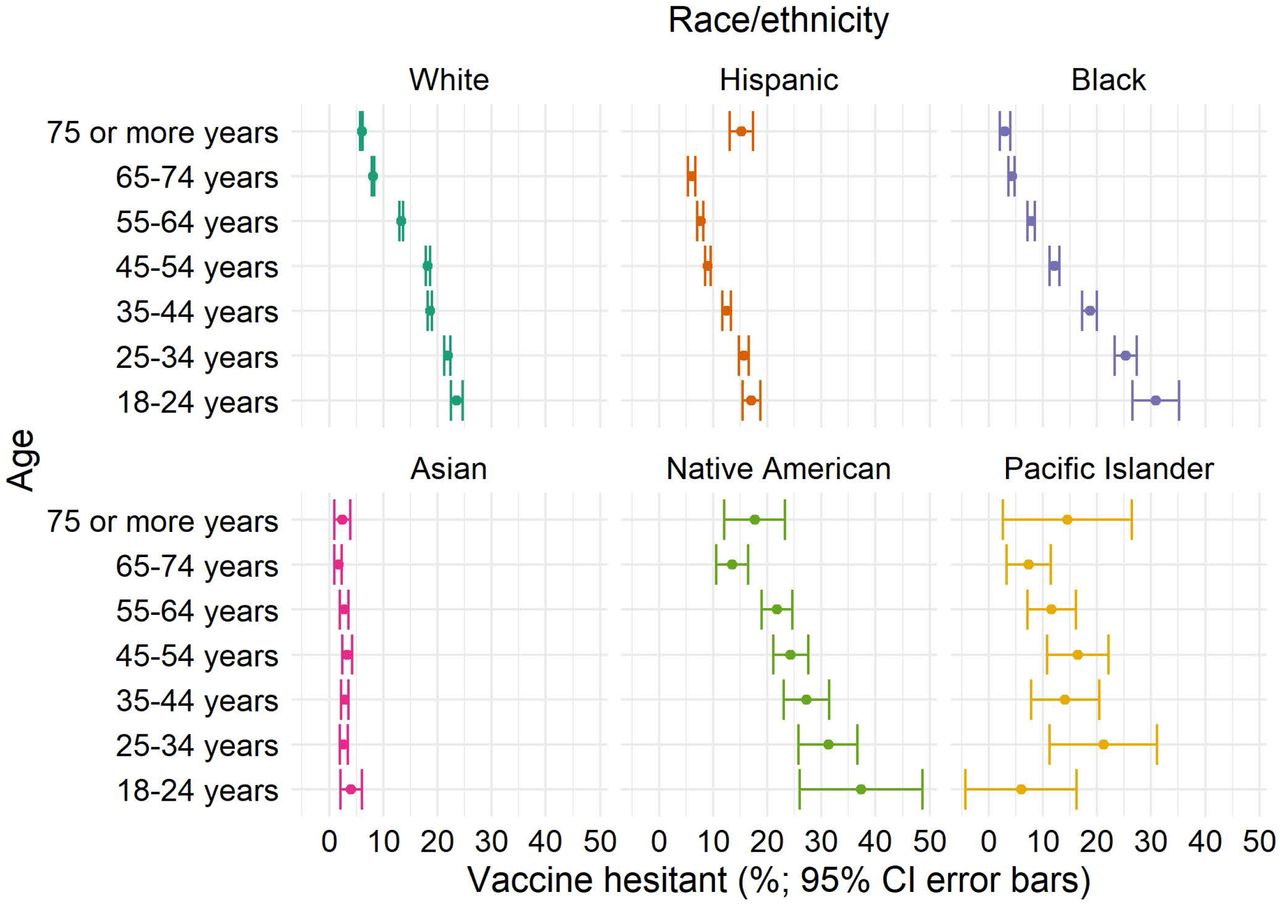
In general, younger age and non-Asian race (particularly multi-racial and Native American), were related to greater hesitancy. However, an interaction was observed between age and race/ethnicity categories (Figure 3). Differences in hesitancy by age were more pronounced in Blacks and less pronounced in Asians and Whites. Differences in hesitancy by race/ethnicity were more pronounced in younger adults and adults ≥75 years. Furthermore, for some comparisons, the direction of the difference differed by age. For example, for Blacks versus Whites, the RR of hesitancy was 1.31 (95%CI, 1.12, 1.51) in 18-24 year olds, versus 0.50 (95%CI, 0.34, 0.67) in ≥75 year olds. eTables 4 and 5 provide RRs for age groups stratified by race/ethnicity groups and vice versa, with and without adjustment for all covariates. Age and race/ethnicity differences were generally attenuated in the full multivariable model but still present.

{kind=link}
{kind=link}
{kind=link}
COVID-19 vaccine hesitancy by age group, stratified by race/ethnicity, among US adults, May 2021
Differences in hesitancy by age (e.g., 18-24 year-olds versus 65-74 year-olds) were more pronounced in Blacks (RR=7.26 [95%CI, 5.92, 8.61]) versus Whites (RR=2.89 [95% CI 2.75, 3.04]) or other race/ethnicity groups. Asians had hesitancy <5% hesitancy in all age groups. Differences in hesitancy by race/ethnicity were more pronounced in younger adults and adults ≥75 years.
The association between hesitancy and education level followed a U-shaped curve with the lowest hesitancy among those with a master’s degree, followed by those with a 4 year college degree, then a professional degree, and a doctorate. The highest hesitancy was among those with ≤high school education or some college (RR=1.89 [95%CI 1.84, 1.94] and 1.67 [95%CI 1.62, 1.71], respectively, versus a 4 year college degree). Additional demographic risk factors for hesitancy included working outside the home (RR=2.44 [95%CI 2.35, 2.53]) or not working for pay (RR=1.50 [95% CI: 1.44, 1.55]) versus working at home; living in the South (RR=1.62 95%CI 1.56, 1.67]), Midwest (RR=1.51 [95%CI 1.47, 1.56]) or Mountain (RR=1.50 [95%CI 1.44, 1.57]) versus the Pacific US region; and in a less urban county (e.g., RR=2.36 [95 CI, 2.28, 2.44] for non-core versus large central metro). Associations were attenuated with adjustment (Table 1).
COVID-19 vaccine hesitancy is reported by indicators of political/COVID-19 environment, health status, and beliefs and behaviors in Table 2. Risk factors for hesitancy were living in a state with Republican versus Democratic governor (RR=1.34 [95%CI 1.32, 1.36]), living in a county with higher Trump support (e.g., RR=2.57 [95%CI 2.50, 2.65] for highest versus lowest quartile), living in a county with a lower April COVID-19 death rate (e.g., RR=0.70 [95%CI 0.68, 0.73] for highest versus lowest quartile), history of a positive COVID-19 test versus no history (RR=1.26 [95%CI 1.23, 1.29]), not having versus having a high-risk health condition (RR=1.41 [95%CI 1.38, 1.43]), less worry about self or immediate family becoming seriously ill from COVID-19 (e.g., RR=3.66 [3.58, 3.74] for not worried at all versus worried), not having versus having received a past-year flu vaccine (RR=4.97 [95%CI 4.85, 5.08]), and not avoiding versus avoiding contact with others (e.g., RR=3.96 [95%CI 3.84, 4.07] for none versus all of the time). Political affiliation of state governor was excluded from the multivariable model due to collinearity with county Trump support. Associations from the multivariable model were attenuated but in the same direction, except for April 2021 COVID-19 death rate, which was not independently related to hesitancy.
COVID-19 vaccine hesitancy by specific health conditions is provided in eTable 6. Compared to participants reporting none of the queried high-risk health conditions, hesitancy was lower among participants with each health condition category except weakened or compromised immune system (RR 1.10, [95%CI 1.02, 1.19]; aRR 1.43 [95%CI 1.33, 1.52]).
A sensitivity analysis including participants who were excluded due to selecting “prefer to self-describe” gender is provided in eTable7 and eTable 8. Overall, results were similar; however, hesitancy prevalence was higher for a few categories (e.g., age ≥75 years, Hispanic, and Doctorate) where mis-reporting was suspected.
Reasons for COVID-19 vaccine hesitancy
Reasons for hesitancy by applicable levels of intent are reported in Table 3. Concern about side effects was chosen most frequently at 49.2% (95%CI, 48.7, 49.7) among hesitant participants, and was similarly common across intent levels. In contrast, among adults who would “definitely not” choose to be vaccinated, not trusting the COVID-19 vaccine and not trusting the government were reported most frequently (59.2% [95%CI, 58.6, 59.8] and 51.2% [95%CI, 50.6, 51.7], respectively), double the prevalence seen among those who would “probably not” get vaccinated and almost quadruple that of adults who “yes, probably” would. Conversely, 52.3% (95%CI, 51.5, 53.1) of the “probably not” group said they would wait to see if it was safe, versus only 24.3% (95%CI, 23.8, 24.8) of the “definitely not” group. Compared to most reasons for vaccine hesitancy, not liking vaccines in general was chosen less frequently across all intent levels (7.6% in “probably yes” to 17.6% in “definitely not”).
Reasons for not getting the COVID-19 vaccine in May, 2021, by vaccine intent level among US adults (N=87,984)a
Reasons for COVID-19 vaccine hesitancy among hesitant US adults by race/ethnicity are provided in eTable9. Concern about side effects, followed by not trusting the COVID-19 vaccine, were the most common concerns in all race/ethnicity groups, with the ranking reversed among Native Americans and Pacific Islanders. Both were chosen by more than 40% of each group except Asians (38.4% [95%CI, 31.5, 45.4] lacked trust in COVID-19 vaccines). There was more racial variability in not trusting the government (range: 26.2-50.0%; >40% among multi-racial, White, and Native American); in waiting to see if safe (range: 27.0-42.5%; >40% among Asian, Hispanic, and Black), and in do not need (range: 22.3-47.0%; >40% among multi-racial and White). Other reasons were chosen by <40% of hesitant adults in each race/ethnicity group.
Discussion
In this massive national survey of US adults, COVID-19 vaccine hesitancy decreased by one-third between January and May, 2021. However, there was minimal change in the prevalence of the most hesitant subgroup (those responding “definitely not”). A decrease in hesitancy was observed across almost all categories evaluated, however, there was a substantial difference in the magnitude of change of education and race/ethnicity categories. The largest decreases, in general, were seen in the categories with the highest January hesitancy prevalence, such that the disparity in hesitancy by these factors decreased. Still, May 2021 data indicates that at the launch of universal vaccine eligibility, COVID-19 vaccine hesitancy varied by a wide array of demographic, geographic, political and COVID-19 environment, health, belief and behavioral factors. Additionally, important differences in reasons for COVID-19 vaccine hesitancy exist both by degree of vaccine intent and racial/ethnic groups.
Racial/ethnic disparities have been observed in all aspects of the COVID-19 pandemic26, with communities of color experiencing higher rates of SARS-CoV-2 infection (despite higher positivity rates indicative of lower access to testing27), as well as COVID-19-related hospitalizations and mortality27,28. Racial/ethnic disparities in COVID-19 vaccine acceptance at the start of the vaccine rollout threatened to continue this trend29, spurring groups from at-risk communities to initiate targeted outreach campaigns30. The large decreases in COVID-19 vaccine hesitancy we measured among Blacks and Pacific Islanders, suggest that the messaging and outreach campaigns combined with the opportunity to observe the initial months of the vaccine rollout, had positive effects; by May 2021, Blacks and Pacific Islanders joined Asian and Hispanics in having a lower prevalence of hesitancy than Whites.
Most previous studies of COVID-19 vaccine hesitancy grouped Asians with American Indian/Alaska Native, Native Hawaiian or other Pacific Islanders.12,31–33 However, our study, which included 11,962 Asian participants in the May sample, identified a remarkably lower prevalence of hesitancy among Asians versus all others. This study also identified an interaction between race/ethnicity and age (e.g., Blacks had relatively high hesitancy among adults under 35 years while Whites had relatively high hesitancy among adults 45 and older), which have previously been reported as independent predictors of vaccine hesitancy without investigation an interaction12,34. Thus, our study provides better data better to inform race/ethnicity and age orientated COVID-19 vaccination uptake efforts.
January through May, there was a dose-response relationship between relative degree of local Trump support in the 2020 presidential election and COVID-19 vaccine hesitancy that grew over time; by May, even after controlling for potential confounders, those living in a county in the top quartile were 44% more at risk of being hesitant, highlighting the politicization of public health recommendations.
Those who were not intentionally avoiding contact with others had much higher likelihood of COVID-19 vaccine hesitancy, as did those working outside the home, indicating non-vaccinated individuals may be the most likely to engage in activities with transmission risk, and thus, are worthy of further study and focused vaccination uptake efforts.
In May 2021, only 14.7% of COVID-19 vaccine hesitant respondents chose not liking vaccines as a reason, indicating that COVID-19 vaccine hesitancy may be a distinct phenomenon from general vaccine hesitancy. However, we also found that those who had not received a flu vaccine were 211% more likely to be COVID-19 vaccine hesitant, even after controlling for a wide array of covariates, which indicates that efforts to increase flu vaccination uptake should address reasons of COVID-19 vaccine hesitancy and vice versa.
Concern about side effects of COVID-19 vaccines was common across levels of vaccine intent and among all racial groups. However, several reasons for COVID-19 vaccine hesitancy varied substantially by subgroups. Among less hesitant (probably not) participants, waiting to see if the vaccine is safe was a common response, suggesting messaging about safety and policy interventions to address downstream impacts of vaccine side effects, such as potential lost work, could be impactful. Conversely, the most hesitant (definitely not) participants commonly reported they don’t trust the COVID-19 vaccine, don’t trust the government, and/or don’t need the vaccine, suggesting the existence of a subgroup with entrenched hesitancy and high distrust that may only respond to vaccine mandates.
Limitations and Strengths
The study employs a novel sampling method with a soft ask and low response rate, the effect of which has not yet been fully studied. Survey weights adjust for non-response and coverage bias (i.e., matching the sample to gender, age, and geographic profile of the US). However, Facebook users may differ from non-users, and our sample is more educated35 and has higher vaccine uptake8 than the general population, indicating that we underestimated vaccine hesitancy compared to the US general US population. Importantly, these sample characteristics have been consistent over time, CTIS results follow similar patterns observed by others,12 and have been used to track trends and inform policies36,37. Demographic questions were asked at the end of the survey and had high unit non-response (e.g., 12% for age). To maximize the analysis sample and control for bias, “missing” was included as a variable category; however, interpretation of estimates for this category is difficult. Additionally, we assume the survey was completed in good faith. However, as noted above, a small percentage of participants selected “prefer to self-describe” gender to make political/discriminatory statements and the frequency of other characteristics in this group was suspect. Thus, they were excluded from the primary analysis sample, but included in a sensitivity analysis that yielded largely similar results. It is possible that additional respondents completed the survey in bad faith but did not self-describe their gender.
A strength of our novel sampling method is that it generated a large sample with diverse characteristics enabling detailed subgroup analyses that identified new findings (e.g., an age-race interaction). Additionally, while a previous study evaluated changes in hesitancy by age, sex, education, or income level, October 2020 through March 202112, estimated change by these categories had large overlapping 95% CI, and the racial and education categories collapsed groups in which we have identified meaningful differences.
Conclusion
As the US enters another wave of COVID-19 infections24, a better understanding of factors related to and reasons for vaccine hesitancy is essential for policy makers working to increase vaccination uptake. This study identified several subgroups of US adults with relatively high COVID-19 vaccine hesitancy (Native American and multi-racial adults, White and Blacks adults <35 years, adults with ≤high school education or some college, those living in rural areas and counties with high Trump support, and those not worried about serious illness from COVID-19, working outside the home, never intentionally avoiding contact with others) and top reasons for hesitancy (concerns about side effects, lack of trust, lack of belief in need). To achieve the level of vaccination required to blunt the impact of highly infectious variants, a range of messaging and policy options to target high-hesitancy groups is urgently needed.
Data Availability
Survey microdata is available to researchers under a nondisclosure agreement protecting the confidentiality of responses. Access can be requested at https://cmu-delphi.github.io/delphi-epidata/symptom-survey/.
https://cmu-delphi.github.io/delphi-epidata/symptom-survey/coding.html
Authors Contributions
Dr. Reinhart and Mr. Rubinstein had full access to all of the data and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Obtained funding, supervised study and acquired data: AR
Developed study concept and design: WK, RM, AR
Performed statistical analysis: MR
Drafting of the manuscript: WK, RM
Interpreted data: WK, RM, AR, MR
Critically revised manuscript for important intellectual content: WK, RM, AR, MR
Other Acknowledgements
We would like to thank the Delphi Group at Carnegie Mellon University for input and support on the survey instrument. Wichada La Motte-Kerr, MPH, of Delphi contributed to the development and deployment of the survey and received compensation for her contributions to the study. We thank Sarah LaRocca, PhD and Katherine Morris, PhD of Facebook for contributions to the survey instrument design.
Conflict of Interest Disclosures
Drs. King, Mejia and Mr. Rubenstein have no conflict of interest to report. Dr. Reinhart received salary support from an unrestricted gift from Facebook described in the funding section of the paper.
Funding/Support
This material is based upon work supported by Facebook (unrestricted gift) and a cooperative agreement from the Centers for Disease Control and Prevention (U01IP001121). Any opinions, findings and conclusions or recommendations expressed in this material are those of the authors and do not necessarily reflect the views of Facebook or the Centers for Disease Control and Prevention.
Role of the Funder
Facebook was involved in the design and conduct of the study. The CDC provided funding only. Neither Facebook nor the Centers for Disease Control and Prevention had a role in the collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; or decision to submit the manuscript for publication.
Data
Survey microdata is available to researchers under a nondisclosure agreement protecting the confidentiality of responses. Access can be requested at https://cmu-delphi.github.io/delphi-epidata/symptom-survey/.
Acknowledgements
Footnotes
kingw{at}edc.pitt.edu
mrubinst{at}andrew.cmu.edu
areinhar{at}stat.cmu.edu
A new exclusion criteria, applicable to <1% of survey responses, was applied to the analysis sample. Specifically, participants who selected "prefer to self-describe" for gender were excluded because the majority of fill-in responses for self-described gender were political/discriminatory statements or otherwise questionable answers (e.g. Apache Helicopter or Unicorn), and that as a group, those who selected self-described gender had a high frequency of uncommon responses (e.g., Hispanic ethnicity [41.4%], the oldest age group [23.2% ≥75 years] and highest education level [28.1% Doctorate]), suggesting the survey was not completed in good faith. A sensitivity analysis including these participants is provided in supplemental material.
References



