
ABSTRACT
Objectives remdesivir is currently approved for the treatment of COVID-19. The recommendation for using remdesivir in COVID-19 was based on the in vitro and in vivo activity of this drug against SARS-CoV-2.
Methods this was a prospective, observational study conducted on a large population of patients hospitalized for COVID-19. The primary endpoint of the study was to evaluate the impact of remdesivir-containing therapy on 30-day mortality; secondary endpoint was the impact of remdesivir-containing therapy on the need of high flow oxygen therapy (HFNC) or non-invasive ventilation (NIV) or mechanical ventilation. Data were analyzed after propensity score matching.
Results 407 patients with SARS-CoV-2 pneumonia were consecutively enrolled. Out of these, 294 (72.2%) and 113 (27.8%) were respectively treated or not with remdesivir. Overall, 61 (14.9%) patients were treated during hospitalization with non-invasive or mechanical ventilation, while a 30-day mortality was observed in 21 (5.2%) patients with a global in-hospital mortality of 11%. Cox regression analysis, after propensity score matching, showed that therapies, including remdesivir-containing therapy, were not statistically associated with 30-day survival or mortality, while need of HFNC/NIV (HR 17.921, CI95% 0.954-336.73, p=0.044) and mechanical ventilation (HR 3.9, CI95% 5.36-16.2, p=0.003) resulted independently associated with 30-day mortality. Finally, therapies including or not remdesivir were not independently associated with a lower or higher risk of HFNC/NIV or mechanical ventilation.
Conclusions this real-life experience about the remdesivir use in hospitalized patients with COVID-19 was not associated with significant increase in rates of survival or reduced use of HFNC/NIV or mechanical ventilation, compared to patients treated with other therapies not including remdesivir.
INTRODUCTION
Severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) is identified as the cause of an outbreak of respiratory illness, evolving in a pandemic. The virus causes respiratory illness and can rapidly spread from person to person; then, in a large number of patients this virus causes coronavirus diseases (COVID-19) characterized by pneumonia, severe acute respiratory syndrome, kidney failure, and a significant rate of mortality [1-2-3].
To date, treatment of critically ill infected patients is primarily supportive with a robust evidence reported in literature about the use of steroids, especially dexamethasone, in lowering mortality especially in critically ill patients [4]; some important evidence suggests also the role of low-molecular-weight heparin (LMWH) to reduce in-hospital mortality [5].
As a matter of fact, only remdesivir was currently approved for the treatment of COVID-19. The recommendation for using remdesivir as treatment of COVID-19 is based on the in vitro and in vivo activity of remdesivir against SARS-CoV-2 [6]. Moreover, remdesivir showed an acceptable safety profile and exhibits in vivo prophylactic and therapeutic efficacy against SARS-CoV-2 infection [7].
According to randomized clinical trials, its administration might shorten the time to recovery and reduce severity of infection in adults hospitalized with COVID-19 [8]. However, there are still many ongoing clinical trials and more evidence is needed to confirm the efficacy of remdesivir in treating patients with COVID-19 at different stages of severity.
Aim of our study was to evaluate in a real-life, prospective, experience the impact of remdesivir on 30-day mortality and the need of non-invasive or invasive ventilation in hospitalized patients with SARS-CoV-2 pneumonia.
RESULTS
During the study period 407 patients with SARS-CoV-2 pneumonia were consecutively enrolled. Out of these, 294 (72.2%) and 113 (27.8%) were respectively treated or not with remdesivir. Overall, 61 (14.9%) patients were treated during hospitalization with non-invasive or mechanical ventilation, while a 30-day mortality was observed in 21 (5.2%) patients, with a global in-hospital mortality of 11%.
In Table 1 is reported univariate analysis about demographics and clinical characteristics of COVID-19 patients treated or not with remdesivir. Statistically significant differences were observed in remdesivir group about male sex (80% Vs 62%, p<0.001), fever (79% Vs 50%, p<0.001), cough (50% Vs 29%, p<0.001), dyspnea (57% Vs 37%, p<0.001), compared to patients not treated with remdesivir. No statistically significant differences were observed in the remdesivir group about age (63.2 Vs 62.5 years, p=0.717), length of hospital stay (15.02 Vs 16.06 days, p=0.487), and days to nasopharyngeal swab negativization (22.07 vs 24.77 days, p=0.378). Finally, no differences were observed about bacterial co-infection (20% Vs 21%, p=0.928) and 30-day mortality (4% Vs 6%, p=0.411).
Univariate analysis about demographics and clinical characteristics of COVID-19 patients treated or not with remdesivir
Other treatments used in COVID-19 patients were reported in Table 2. Comparison between patients treated or not with remdesivir showed that steroids (93% Vs 81%, p<0.001), LMWH (93% Vs 52%, p<0.001) were more frequently prescribed in remdesivir group. Antibiotic therapy (58% Vs 27%, p<0.001) was more frequently prescribed for patients not treated with remdesivir, while no differences were reported about the use of HFNC/NIV or mechanical ventilation in the 2 study groups.
Other treatments in COVID-19 patients treated or not with remdesivir
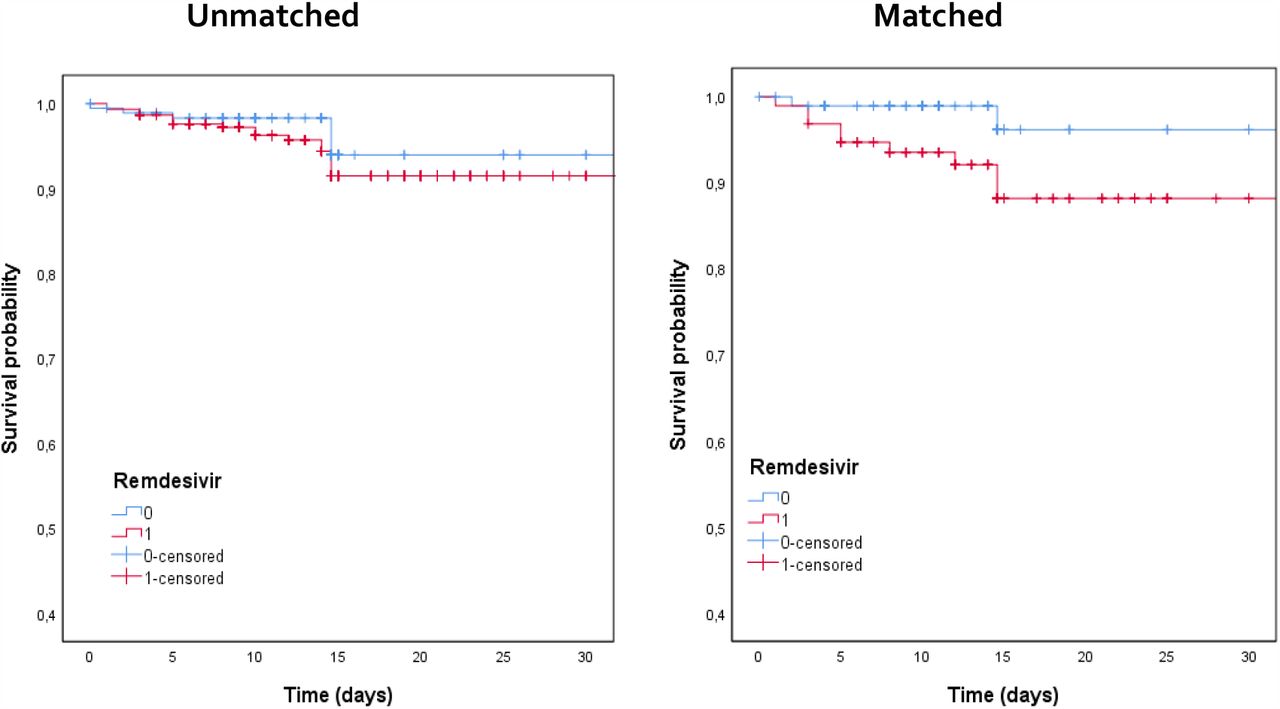
In supplementary Table 1 is reported univariate analysis after propensity score matching to evaluate the impact of remdesivir-containing regimen on study population (for reviewers’ information only). Figure 1 showed Kaplan Meier curves about 30-day survival in patients treated or not with remdesivir before (p=0.24) and after (p=0.07) propensity score matching, reporting no differences between the 2 study groups. Standardized differences before and after propensity score matching were reported in supplementary Figure 1 (for reviewers’ information only).
{kind=link}
Kaplan Meier curves about 30-day survival in patients treated or not with remdesivir before (p=0.24) and after (p=0.07) propensity score matching
Multivariate Cox regression analysis about 30-day mortality after propensity score matching was reported in Table 3. Comorbidities and therapies, including remdesivir-containing therapy, were not statistically associated with 30-day survival or mortality. Instead, HFNC/NIV (HR 17.921, CI95% 0.954-336.73, p=0.044) and mechanical ventilation (HR 3.9, CI95% 5.36-16.2, p=0.003) resulted independently associated with 30-day mortality
Multivariate Cox regression analysis about 30-day mortality after propensity score matching
Finally, multivariate Cox regression analysis about need of non-invasive or invasive ventilation was analyzed after propensity score matching (see Table 4). Data showed that comorbidities and therapies, including remdesivir-containing regimen, were not independently associated with a lower or higher risk of HFNC/NIV or mechanical ventilation.
Multivariate Cox regression analysis about need of non-invasive or invasive ventilation after propensity score matching
DISCUSSION
This prospective clinical study reported a real-life experience about the use of remdesivir in a large population of consecutively hospitalized patients with COVID-19. Our data, also after propensity score matching, showed that remdesivir-containing regimen was not associated with 30-day survival compared to patients treated with other therapies not including remdesivir. Moreover, remdesivir-containing regimen was not independently related to progression or not to HFNC/NIV or mechanical ventilation.
In Italy, remdesivir was specifically licensed for the treatment of COVID-19 in hospitalized patients with pneumonia, requiring oxygen therapy but not treated with HFNC/NIV or mechanical ventilation at time of remdesivir prescription [9].
Different data were worldwide reported about the efficacy of remdesivir, taking in account different outcomes. Remdesivir treatment was associated with significantly higher recovery rates and lower mortality, compared to standard-of-care treatment without remdesivir in patients with severe COVID-19 [10]. In this study, significantly lower mortality was observed in those treated with remdesivir (7.6%) compared with the non-remdesivir-cohort patients (12.5%). Conversely, data from Solidarity trial, conducted in 30 countries [11], showed no decrease of in-hospital mortality in patients treated with remdesivir, with the important limitation that other outcomes, clinical improvement and adverse events, were non carefully evaluated.
Some important meta-analysis showed that COVID-19 patients receiving remdesivir had significantly higher rates of recovery and hospital discharge with lower rates of developing serious adverse events compared to patients receiving standard of care/placebo [12-13]. However, these analyses confirmed that no significant differences were observed about clinical improvement and rate of mortality during hospitalization. Specifically, mortality was the main outcome reported in all included studies, and none of the studies showed significant decrease of mortality also if they were not adequately powered for mortality outcome [12].
Wang et al. [14] reported the first double blinded, randomized, clinical trial in which were evaluated patients with an interval from symptoms onset to enrollment of 12 days or less. No differences in mortality were recorded in the 2 arms, also if authors highlighted a possible trend towards clinical benefit in remdesivir group. Of importance, a large number of patients in this study were treated also with steroids (65% of patients who received remdesivir and 68% of patients in placebo arm) which may have confounded the results and the conclusions. A strength of our study, with the limit of the non-randomized cohort, was to weight all the possible therapeutic confounders, comprising the use of steroids and LMWH.
Beigel et al. [8] randomized 1062 patients, hospitalized with COVID-19 and evidence of pneumonia, to remdesivir or placebo. The study demonstrated that remdesivir was superior to placebo in shortening the time to recovery in hospitalized COVID-19 patients with a trend towards survival benefit at day 29 without statistically significant differences. Of interest, authors reported a beneficial effect of remdesivir in severe COVID-19 patients but not requiring mechanical ventilation at enrollment; they suggested to start remdesivir early in the disease course.
Finally, in another randomized, clinical trial [15] in patients with moderate COVID-19 (no oxygen requirements, also if about 15% of patients required oxygen at time of enrollment) authors randomized 596 patients in 1:1:1 ratio to receive a 5-day course of remdesivir, a 10-day course of remdesivir, or standard of care therapy. In this study patients randomized to 5-day, but not 10-day treatment duration, showed a statistically significant difference in clinical status. A subgroup analysis excluding patients who required oxygen at baseline showed a significant difference favouring remdesivir over standard care.
Our study has some limitations. First, considering the monocentric design these results might be affected by local practice in the management of COVID-19; second, although criteria for HFNC/NIV or mechanical ventilation were based on the degree of respiratory impairment, elderly critically ill patients with ultimately fatal diseases were probably excluded from non-invasive/invasive ventilation, modifying the interpretation of some interventions. Second, in this analysis were evaluated all consecutively, hospitalized patients independently from COVID-19 severity, as demonstrated also by the low mortality (6% of remdesivir group Vs 4% of patients not treated with remdesivir). Finally, the analysis on the beneficial effects of treatments should be interpreted cautiously, because it was not conducted on randomized groups and might therefore be affected by several measured and unmeasured confounding factors. However, the comparison of remdesivir-treated patients with non-remdesivir-treated patients was based on a robust statistical methodology, appropriate for non-randomized cohort studies about therapy.
In conclusion, in our real-life experience about the remdesivir use in hospitalized patients with COVID-19 was not associated with significant increase in rates of survival or reduced use of HFNC/NIV or mechanical ventilation, compared to patients treated with other therapies not including remdesivir. These results suggest the need of more RCTs to evaluate the role of remdesivir in COVID-19 patients at different stages of disease or in combination with other drugs [16]. However, considering its safety profile and the lack of alternative drugs, remdesivir should be continued to be administered for patients with COVID-19.
METHODS
Study Design and Data Collection
This prospective, observational study included, from October 2020 to February 2021, patients admitted to University Hospital of Rome ‘‘Policlinico Umberto I‘’, in Italy. Inclusion criteria were: 1) positive SARS-CoV-2 real-time polymerase chain reaction test or an antigenic test on a nasopharyngeal swab; 2) pneumonia diagnosed either by CT thorax or chest x-ray; 3) need of hospitalization. Patients who required high flow oxygen therapy (HFNC) or non-invasive ventilation (NIV) or mechanical ventilation at time of hospitalization were excluded from this analysis.
All patients were evaluated in a dedicated Emergency Department by a dedicated staff of infectious diseases specialists that identified patients with SARS-CoV-2 pneumonia as soon as they arrived at the hospital, followed the patients during the hospital stay, and collected all data prospectively without interfering with the therapeutic decisions. This observational study was conducted according to the principles stated in the Declaration of Helsinki, and it conforms to standards currently applied in our country. The study was approved by the local EC. The patient’s informed consent was obtained.
Data were extracted from the medical records of patients and from hospital computerized databases. The following data were collected: demographics, clinical and laboratory findings, comorbidities, Charlson comorbidity index, microbiologic data, date of COVID-19 diagnosis, radiological characteristics of the pneumonia, therapies, concomitant infections, duration of mechanical ventilation, time of nasopharyngeal swab negativity, need of oxygen or ventilation support during the hospital stay, length of ICU stay, length of hospital stay. Development of moderate to severe ARDS was defined as the acute onset of hypoxemia, manifestations of pneumonia on chest computed tomography imaging of a noncardiac origin, and a PaO2/FiO2 ratio of less than 200 mmHg according to the Berlin Definition [17].
Remdesivir was administrated, after written informed consent, to patients with the following characteristics: pneumonia, less than 10 days from the onset of symptoms, no need for HFNC or NIV or mechanical ventilation, alanine aminotransferase no more than 5 times the upper limit of the reference range, estimated glomerular filtration rate (eGFR) greater than 30 mL/minute. A 5-day regimen was prescribed in all cases. Patients without these criteria were not eligible for remdesivir treatment.
All patients were followed-up until discharge or death.
Endpoints and Statistical analysis
The primary endpoint of the study was to evaluate the impact of remdesivir-containing therapy on 30-day mortality in hospitalized patients with SARS-CoV2 pneumonia. Secondary endpoint was the impact of remdesivir-containing therapy on the need of NIV or mechanical ventilation.
To reduce the impact of treatment-selection bias in the estimation of treatment effects, propensity score matching was conducted. Variables were selected for inclusion in the propensity score based on potential impact on receipt of remdesivir and association with mortality [18]. The variables included were steroids, antibiotics (excluding macrolides), age, gender, and the use of LMWH during hospital admission. A propensity score density plot and Love plot were generated to examine the balance of propensity score and covariate distribution between the two groups (see supplementary Figure 1).
To evaluate demographic factors, Welch’s t tests assuming unequal variances were used for continuous independent variables, while Pearson Chi-square or Fisher’s Exact Test when appropriate were used for categorical variables. Welch’s analysis of variance (ANOVA) was used to assess group differences for continuous outcome. Welch’s t-tests assuming unequal variances were used for post-hoc comparisons.
All tests will be two-tailed, and a p-value of <0.05 were considered statistically significant. Results were expressed as the mean with standard deviation (±SD) for continuous normally distributed variables and as a count (n) and percentage (%) for categorical variables. Multivariate analysis was used to identify independent predictors of 30-day mortality and need of NIV or mechanical ventilation. Matched bivariate analyses were conducted using a conditional logistic regression model, incorporating all variables found to be significant in the Univariate analysis (p < 0.05) with a stepwise method. Matched multivariate models was constructed using Cox proportional hazards (HRs) regression if appropriate, accounting for clustering on matched pairs. The final selected model was tested for confounding. In addition, 95% confidence intervals were calculated for HR. Survival was analyzed by Kaplan-Meier curves. All data were analyzed using a commercially available statistical software package (SPSS Statistics for Mac, 22.0; IBM Corp., Armonk, NY).
Data Availability
Data are available on request to Prof. Alessandro Russo.
Conflict of interest
none to declare.
Funding
none.
Transparency declarations
none to declare.
ACKNOWLEDGEMENT



