
Abstract
Background Evidence to date indicates that mortality of acute coronavirus disease (COVID-19) is higher in men than in women. Conversely, women seem more likely to suffer from long-term consequences of the disease and pronounced negative social and economic impacts. Sex- and gender specific risk factors of COVID-19-related long-term effects are unknown.
Methods We conducted a multicentre prospective observational cohort study of 5838 (44.6% women) individuals in Switzerland who were tested positive for SARS-CoV-2 RNA between February and December 2020. Of all surviving individuals who met the inclusion criteria, 2799 (1285 [45.9%] women) completed a follow-up questionnaire.
Findings After a mean follow-up time of 197±77 days, women more often reported at least one persistent symptom (43.0% vs 31.5%, p<0.001) with reduced exercise tolerance and reduced resilience being the most frequently reported symptom in both sexes. Critical illness (intermediate or intensive care unit admission) during acute SARS-CoV-2 infection (odds ratio[95%CI]: 4.00[2.66-6.02], p<0.0001 was a risk factor of post-COVID syndrome in both women and men. Women with pre-existing mental illness (1.81[1.00-3.26], p=0.049), cardiovascular risk factors (1.39[1.03-1.89], p=0.033), higher self-reported domestic stress levels (1.15[1.08-1.22], p<0.0001), and feminine gender identity (1.12[1.02-1.24], p=0.02) increased the odds of experiencing post-COVID syndrome. Conversely, obesity (1.44[1.03-2.02], p=0.034) increased the odds of post-COVID syndrome in men, but not in women. Being responsible for household work (men, OR 0.82[0.69-0.97], p=0.021), taking care of children/relatives (women, 0.90[0.84-0.96], p=0.002) or being pregnant at the time of acute COVID-19 illness (OR 0.48[0.23-1.01], p=0.054) was associated with lower odds of post-COVID syndrome.
Interpretation Predictors of post-COVID syndrome differ between men and women. Our data reinforce the importance to include sex and gender to identify patients at risk for post-COVID syndrome so that access to care and early intervention can be tailored to their different needs.
Evidence before this study We performed a PubMed search for studies investigating short- and long-term health sequelae in COVID-19 survivors. We included all studies published prior to May 30th, 2021. The search comprised the following terms: (COVID-19 OR SARS-CoV-2 OR Coronavirus disease 2019 OR 2019-nCoV) AND (post COVID OR long COVID OR survivor OR recover OR persistent OR follow up OR discharge OR long-term OR sequelae). Previous studies have reported a variety of symptoms in COVID-19 survivors from different countries such as China (Wuhan), the UK, and the U.S. Overall, these studies showed that a substantial burden of health issues spanning multiple organ systems is experienced by patients who survive after the acute phase of COVID-19. The most frequent symptoms reported after acute infection were fatigue, muscle weakness, sleep disturbances, headache, dyspnoea, anxiety, depression, and anosmia. Two studies indicate that women are overrepresented amongst post-COVID-19 syndrome patients suffering from fatigue, headache, dyspnoea, or anosmia. However, the representativeness of the studies and the explicitness of provided information were insufficient due to lacking variables and/or small numbers of cases and the short duration of follow-up. Sex-and gender-specific predictors of post-COVID-19 syndrome are currently unknown.
Added value of this study In a large cohort study (n=2799) with long follow-up (mean follow-up 197±77 days), we investigated sex- and gender-specific predictors of post-COVID-19 health sequalae. Our data allow for identification of sex- and gender-specific predictors of post-COVID-19 syndrome. In a multivariable association model, post-COVID-19 syndrome was associated with severity of illness and number of symptoms during acute SARS-CoV-2 infection in both sexes, while pre-existing mental illness and cardiovascular risk factors were significant predictors only in women. Conversely, obesity was independently associated with post-COVID-19 syndrome in men, but not in women. Gender-related risk factors of post-COVID syndrome were feminine traits and higher amount of domestic stress, both increasing the odds of post-COVID-19 syndrome in women, while pregnancy during acute COVID-19 illness and responsibility for childcare protected women, and responsibility for household work protected men from experiencing post-COVID-19 syndrome.
Implications of all the available evidence Evidence indicates that mortality from COVID-19 infection is higher in men than women. We provide evidence that female sex and gender is associated with long-term sequalae of COVID-19. Our data reinforce the importance of including gender to identify patients at risk for post-COVID-19 syndrome so that the functional return of both male and female COVID-19 survivors can be maximized.
Introduction
The coronavirus disease (COVID)-19 pandemic has become one of the greatest public health challenges in modern times. As the COVID-19 pandemic continues to evolve across the globe, male sex, cardiovascular and metabolic diseases, and advanced age have been identified as predominant risk factors for a more severe disease course of COVID-19 and poor prognosis.1 Accordingly, male patients with COVID-19 are reported to die at twice the rate of females when they contract the virus.2 Biological (sex) differences in immune responses and expression levels of receptors responsible for viral entry and priming have been suggested to account for the higher COVID-19-related mortality rates seen in men.3,4 Furthermore, male specific comorbidities such as cardiometabolic diseases may explain the greater susceptibility for COVID-19-related complications. However, despite the emerging understanding of sex differences in COVID-19, many questions including the impact of social and behavioural (gender) factors on COVID-19 remain.
Increasing evidence suggests that Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2) can cause a prolonged disease course beyond acute illness.5,6 Only few studies to date have examined the clinical presentation of post-COVID-19 syndrome and report fluctuating and unpredictable symptoms which affect pulmonary and extrapulmonary organs thereby posing a rising burden on healthcare systems. Two large cohort studies suggest that women are overrepresented amongst patients suffering from neurological and psychological long-term consequences of COVID-19.7,8 However, sex- and gender-specific risk factors of post-COVID-19 syndrome are unknown.
Despite growing recognition of the relevance of sex and gender in the COVID-19 pandemic,9 the effect of gender, which comprises roles, norms, and behaviours that may vary by sex, has been inadequately examined and reported in current COVID-19 literature. The latter, however, is crucial to improve the effectiveness of health interventions, and to achieve gender and health equity goals. We therefore sought to investigate the factors associated with post-COVID-19 syndrome in women and men by reporting gender roles and behaviours in addition to sex-disaggregated data in a large multi-centre cohort in Switzerland.
Methods
Study design and study population
This study is based on data from participants of the Swiss COGEN Cohort study, a prospective, observational cohort of polymerase chain reaction (PCR)-confirmed SARS-CoV-2 infected individuals diagnosed between February and December 2020 at one of four Swiss study sites: the University Hospital Basel, the University Hospital Zurich, the University Hospital Bern, and the Cantonal Hospital Baden. Eligible patients were adults aged ≥18 years who survived acute COVID-19 infection and fluent in German, English, French, or Italian and able to provide informed consent. The study protocol was approved by the responsible ethics committee of the Canton of Basel (EKNZ, ethics approval #2020-01311). Informed consent was obtained from all participants or their legal representative, as appropriate. More details on study design and population are provided in Supplementary Methods.
Procedures and data sources
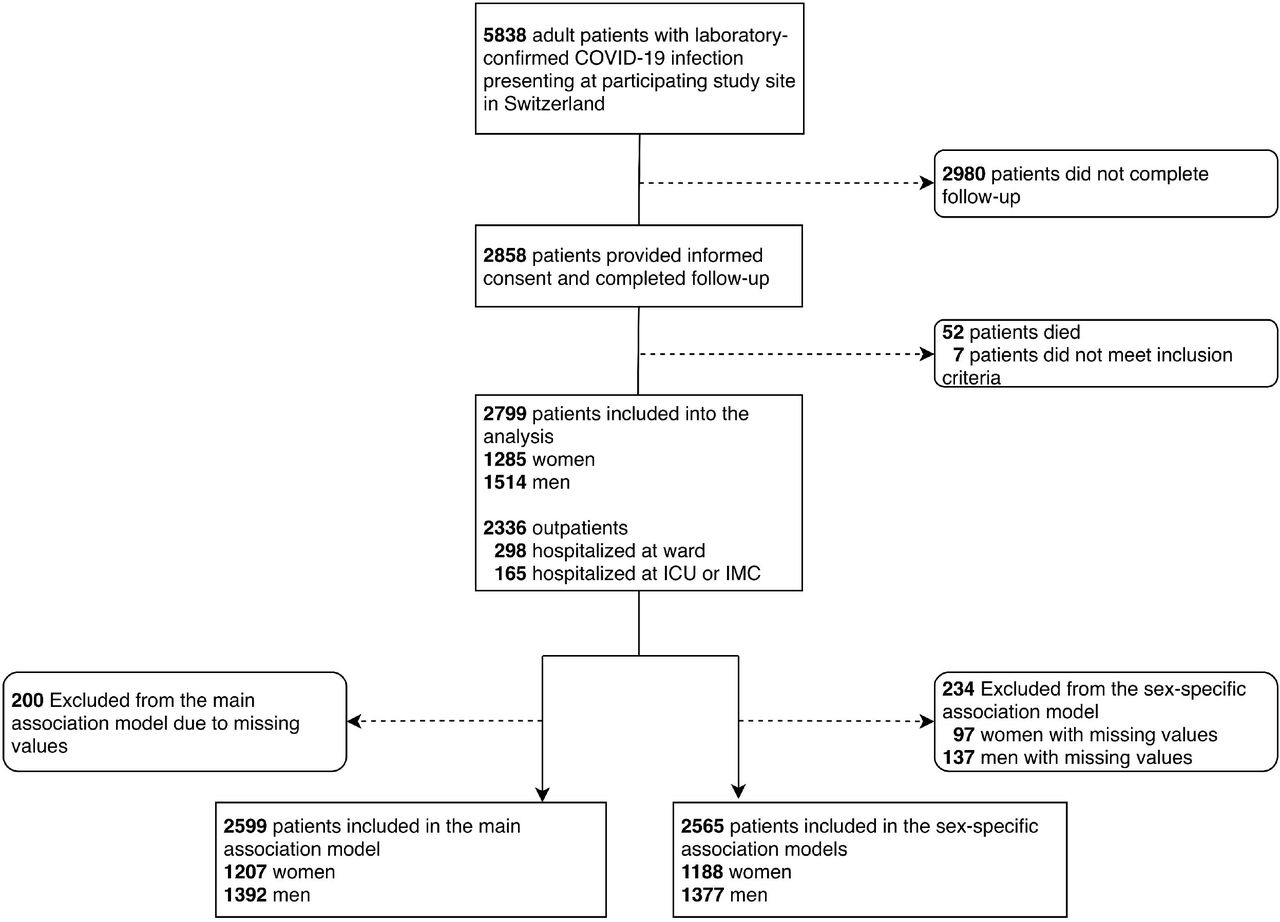
After a minimum follow-up time of 60 days (mean follow-up time 197±77 days), each participant was contacted by telephone and was asked to complete a questionnaire either by phone, email or written form. Details regarding the questionnaire are provided in Supplementary Methods. Out of 5838 patients, 2858 patients or their legal representatives completed the questionnaire after giving informed consent. Out of 2858 patients, 52 patients (8 women and 44 men) died during or after treatment for COVID-19, 7 did not meet inclusion criteria. A flowchart depicting patient recruitment is provided in Figure 1 and more details on procedures and data sources are given in Supplementary Methods.
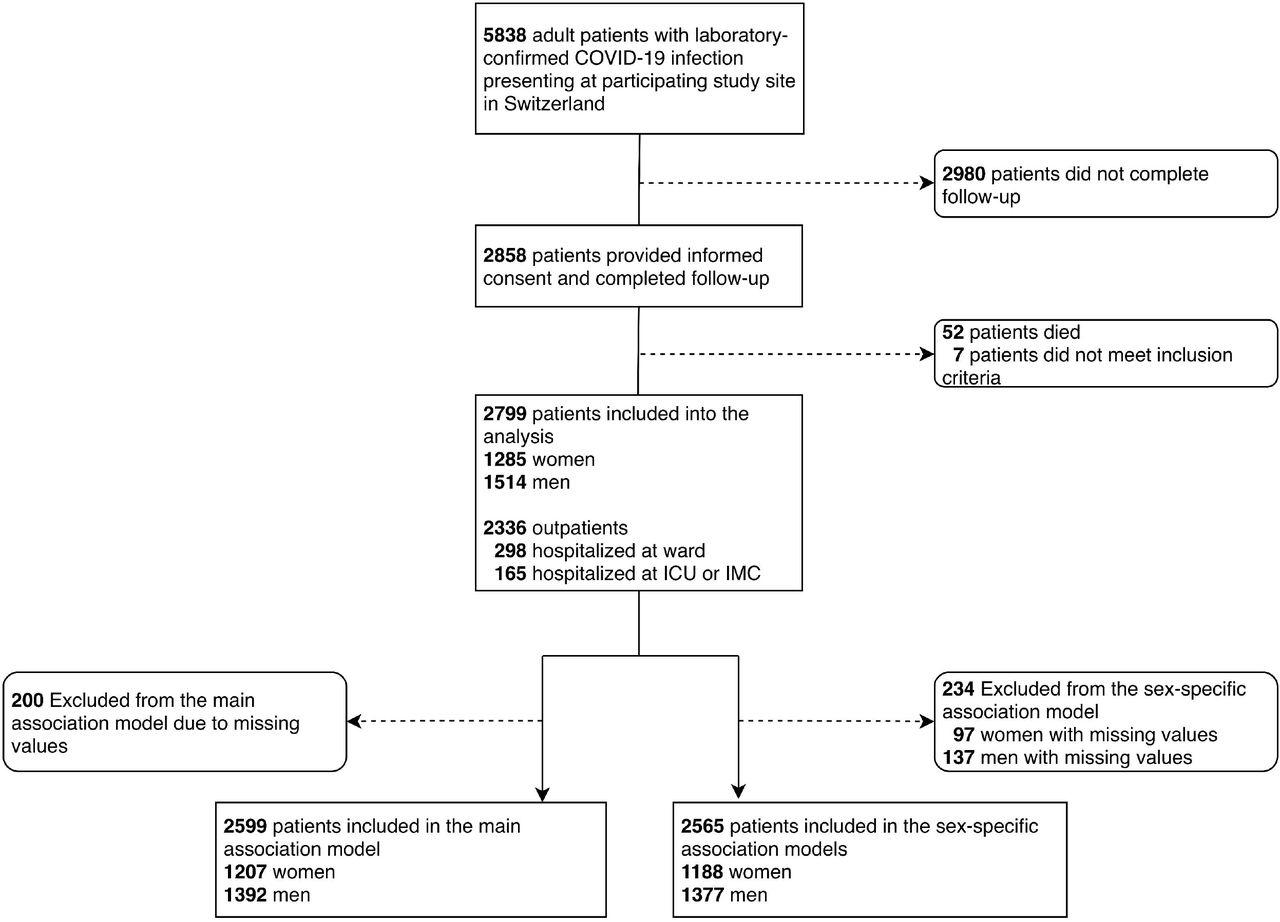
Flowchart depicting patient selection. IMC, intermediate care unit; ICU, intensive care unit.
Outcome measures
The primary outcome measure of our analysis was defined as the persistence of at least one COVID-19 related symptom for more than 60 days. Secondary outcome measures included the description of current quality of life as compared to before the COVID-19 disease (much better, slightly better, about the same, slightly worse or much worse compared to before COVID-19), hospital readmission (yes or no), and the nature (shortness of breath, reduced exercise capacity/physical weakness, chest pain, joint pain, skin changes, loss or change of smell, loss of sense or taste, visual disorders, excess salivation, concentration problems, loss of memory or forgetfulness, balance problems, depression, anxiety, persistent pain, sensory disturbances, palsy, trembling, headache and/or other symptoms) of persistent symptoms. Additionally, patients were asked in the questionnaire to elaborate on their experience in free text.
Statistical analyses
A detailed description of the statistical method is provided in Supplementary Methods. Briefly, descriptive statistics for baseline characteristics included means and standard deviations or counts and percentages of total for categorical variables. Participants were stratified by sex (binary). For group comparisons, exploratory p-values from t-tests for continuous variables, χ2 test, or Fisher’s exact tests for categorical variables were applied, as appropriate. The primary outcome of persistent symptoms at a minimum of 60 days following acute SARS-CoV-2 infection, was addressed with multiple logistic regression models (Supplementary Methods). The statistical analysis was performed through a fully scripted data management system to combine decrypted data from different sources, data pre-processing, and analysis pathway, using the statistical programming environment R for computations and visualization.10 Models were fitted to complete case (CC) populations first, in which all patients with missing data were excluded row-wise, and subsequently a sensitivity analysis with 100-fold multiply imputed (MI) data sets was performed.11
Results
Patient baseline characteristics
The final study cohort comprised 2799 individuals of whom 1285 (45.9%) were women and 1514 (54.1%) were men (Figure 1). The mean age (±SD) of the study population was 44±17 years. The most common risk condition in the overall cohort was hypertension (431 patients, 15.4%), followed by obesity (402 patients, 14.4%). Cardiovascular disease including valvular heart disease, cardiomyopathies, or coronary artery disease, was present in 304 patients (10.9%). On average, men were older than women (45±17 years vs 42±16 years, p<0.001), had a higher BMI (26.2±4.4 kg/m2 vs 24.5±5.2 kg/m2, p<0.001), were more often smokers (29.6% vs 25.4%, p=0.014), more often had dyslipidaemia (9.1% vs 4.8%, p<0.001), diabetes mellitus (7.7% vs 2.9%, p<0.001), hypertension (19.0% vs 11.2%, p<0.001), and pre-existing cardiovascular disease (13.0% vs 8.3%, p<0.001), while women more often had a positive family history of coronary artery disease (15.6% vs 12.5%, p=0.022) and more often suffered from pre-existing autoimmune disorders (9.7% vs 5.3%, p<0.001). Baseline characteristics of the study population are summarized in Table 1. All sex- and gender-related baseline characteristics are provided in Table 2 and described in Supplementary Results.
Baseline characteristics of the total study population stratified by sex. BMI, body mass index; CRP, C-reactive protein; QoL, quality of life. * hospitalized patients only, p-values are reported for comparison between women and men.
Socioeconomic and sex-specific characteristics of men and women. p-values are reported for comparison between women and men.
Acute COVID-19 illness
Out of 2799 individuals who were tested positive for SARS-CoV-2 and survived acute SARS-CoV-2 infection, 2336 (83.5%, 1131 [88.0%] women and 1205 [79.6%] men) remained outpatients, 463 (16.5%) were inpatients. 298 patients (10.6%, 106 women [8.2%] and 192 men [12.7%]) were admitted to a normal ward, and 165 (5.9%, 48 women [3.7%] and 117 men [7.7%]) were admitted to an intermediate or intensive care unit (p<0.001 for men vs women, Table 1). Amongst hospitalized patients, there was strong evidence for sex differences in routine laboratory markers of inflammation with the maximum C-reactive protein level being significantly higher in men (142.3±110.64 µg/dL in men vs 103.98±114.3 µg/dL in women, p=0.001, Table 1). There was no evidence for sex differences in maximal white blood cell counts (11.8±15.1 G/L in women and 10.8±6.5 G/L in men, p=0.296), and weak evidence for lower minimal lymphocyte count in men, with minimal lymphocyte counts in men fulfilling the criteria for lymphopenia (0.9±1.4 G/L in men vs 1.5±4.7 G/L in women, p=0.056, Table 1). The average number of reported symptoms during acute COVID-19 was higher in women as compared to men (5.2±2.4 in women vs 4.4±2.3 in men, p<0.001). Accordingly, more women than men reported to have suffered from more than five symptoms during acute COVID-19 (44.7% in women vs 29.9% in men, p<0.001, Table 1).
Post-COVID-19 sequelae
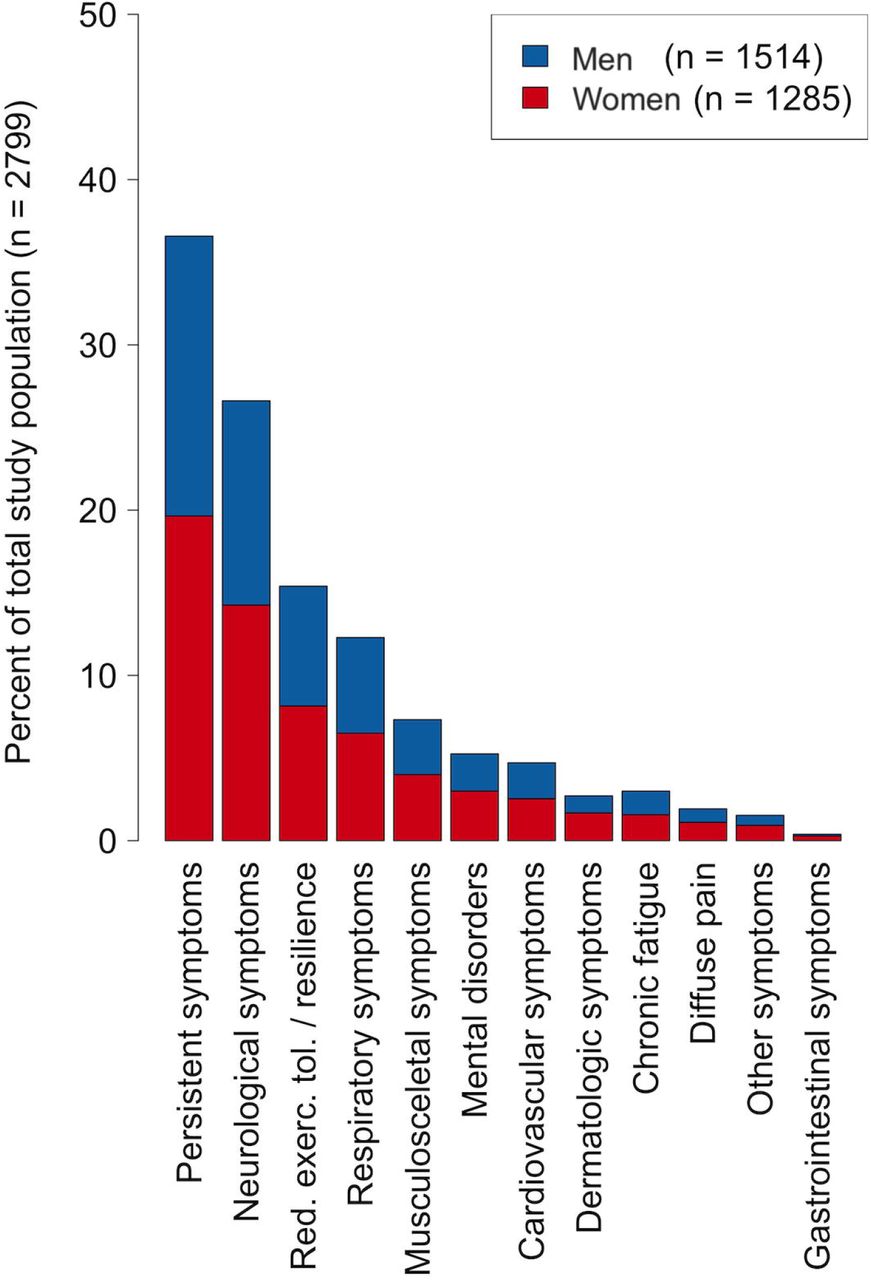
During a mean follow-up time of 197 days 1024 (36.8%) individuals reported at least one persistent symptom (primary outcome measure). 152 (5.5%) individuals (66 [5.2%] women and 86 [5.7%] men, p=0.573 for women vs men, Table 1) were re-hospitalized at least once for persistent symptoms or complications of COVID-19. 807 patients (28.8%) reported a worse quality of life as compared to their pre-illness situation (p=0.139 for women vs men, Table 1). Women more often reported at least one persistent symptom as compared to men (43.0% vs 31.5%, p<0.001, Table 1, Figure 2) and the average number of reported symptoms at follow-up was significantly higher in women as compared to men (1.31±2.2 vs 0.92±1.8, p<0.001, Table 1). Across all organ-systems, except for cardiovascular and gastrointestinal symptoms, women more often reported persistent symptoms as compared to men (Figure 2). Amongst individuals with persistent symptoms, the most frequent symptom reported at follow-up was reduced exercise tolerance and reduced resilience, which was reported by 43% of men and 41% of women with persistent symptoms (Figure 3). More details on specific post-COVID-19 symptoms and subgroup analyses are provided in Supplementary Results.

Persistent symptoms reported at follow-up stratified by sex. Symptoms are clustered in organ-systems and shown as percentage of total study population (n=2799). Red. exerc. tol, reduced exercise tolerance.

Persistent symptoms reported at follow-up stratified by sex and symptom. Data are presented as percentage of patients reporting persistent symptoms (n=1024).
Sex- and gender-specific determinants of post-COVID-19 syndrome
Individuals who reported at least one persistent symptom at follow-up were more likely to be female (odds ratio [OR] and 95% confidence interval [CI] 1.65[1.26-2.17], p=0.0003) or obese (1.40[1.08-1.81], p=0.01), suffered more often from >5 symptoms during acute COVID-19 illness (2.69[2.25-3.21], p<0.001), were more often hospitalized on the normal ward (1.65[1.21-2.25], p=0.002) or ICU (4.00[2.66-6.02], p<0.0001), had more often pre-existing mental illness (1.63[1.08-2.48], p=0.021), and reported more often an increased domestic stress-level (1.10[1.05-1.14], p<0.0001, Table 3). Being the main person responsible for childcare/care of family members was associated with a reduced risk of experiencing post-COVID-19 syndrome (0.95[0.91-0.99], p=0.014, Table 3).
General model for the association between demographic characteristics, acute COVID-19 illness, preexisting disease, sex- and gender-specific variables and the occurrence of post-COVID syndrome in the overall study population. BMI: Body mass index; CVRFs, cardiovascular risk factors.
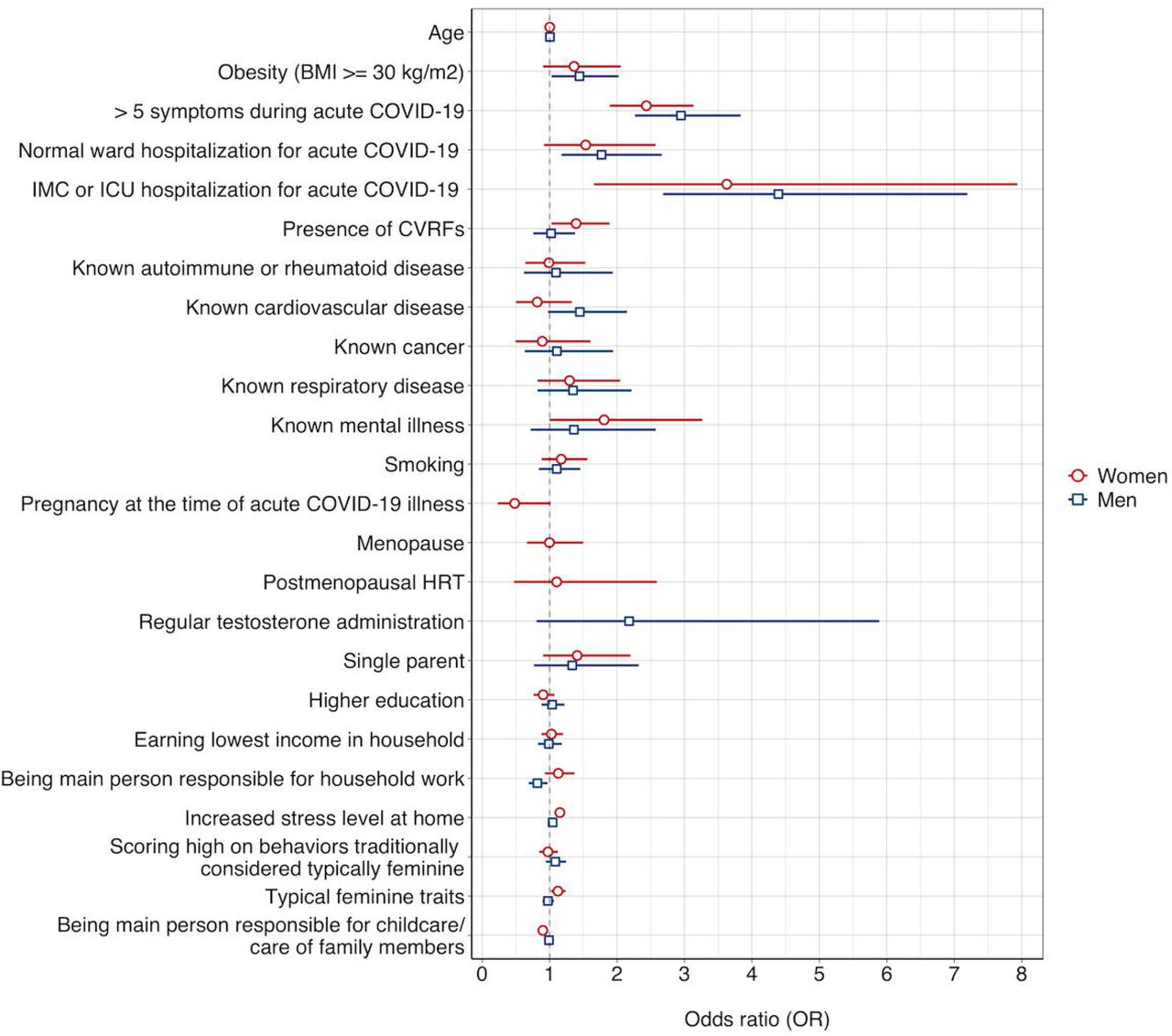
In women, having experienced more than 5 symptoms (2.43[1.89-3.13], p<0.0001) or being hospitalized at the ICU during acute COVID-19 illness (3.63[1.66-7.93], p=0.001) as well as the presence of cardiovascular risk factors (1.39[1.03-1.89], p=0.033), pre-existing mental illness (1.81[1.00-3.26], p=0.049), an increased domestic stress level (1.15[1.08-1.22], p<0.0001), self-assessment of gender identity according to BEM score (1.12[1.02-1.24], p=0.02) were all associated with an increased risk of experiencing post-COVID-19 syndrome (Table 4, Figure 4). Conversely, being the main person responsible for childcare/care of family members was associated with lower odds of post-COVID-19 syndrome (0.90[0.84-0.96], p=0.002, Table 4, Figure 4). Similarly, there was a trend towards an inverse relationship between being pregnant at the time of acute COVID-19 illness and the occurrence of post-COVID-19 syndrome (0.48[0.23-1.01], p=0.054, Table 4, Figure 4).
General model for the association between demographic characteristics, acute COVID-19 illness, preexisting disease, sex-and gender-specific variables and the occurrence of post-COVID syndrome in women. BMI: Body mass index; CVRFs, cardiovascular risk factors; HRT, hormone replacement therapy.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest Plot depicting odds ratios and 95% confidence intervals of risk/protective factors associated with post-COVID-19 syndrome in women and men. ICU, intensive care unit; IMC, intermediate care unit; CVRF, cardiovascular risk factor.
In men, obesity (1.44[1.03-2.02], p=0.034), having experienced more than 5 symptoms during acute COVID-19 illness (2.95[2.25-3.83], p<0.0001), being hospitalized at normal ward (1.77[1.18-2.66], p=0.006) or ICU (4.39[2.68-7.19], p<0.0001) during acute COVID-19 illness were all associated with an increased risk of post-COVID-19 syndrome (Table 5, Figure 4). The presence of pre-existing cardiovascular disease was only weakly associated with increased odds of post-COVID-19 syndrome (1.45[0.98-2.15], p=0.066, Table 5, Figure 4). Conversely, being the main person responsible for household work was associated with a reduced risk of experiencing post-COVID-19 syndrome in men (0.82[0.69-0.97], p=0.021, Table 5, Figure 4).
General models for the association between demographic characteristics, acute COVID-19 illness, preexisting disase, sex- and gender-specific variables and the occurrence of post-COVID syndrome in men. BMI: Body mass index; CVRFs, cardiovascular risk factors.
Discussion
Although growing attention is paid to the relevance of sex and gender in the COVID-19 pandemic, the influence of both variables on the occurrence of post-COVID-19 symptoms is currently unknown. Our study is the first to examine the combined effect of clinical biological variables and variables that refer to the sociocultural dimension gender on COVID-19 health consequences. While our study confirms previous data pointing to a higher prevalence of post-COVID-19 syndrome in women, to our knowledge, we are the first to identify sex-and gender-specific risk factors for post-COVID-19 multiorgan dysfunction. In our cohort of individuals with proven SARS-CoV-2 infection who were on average followed up for as long as 6.5 months after acute illness, 43% of women and 32% of men reported at least one persistent symptom months after acute illness with the number of symptoms per individual being also significantly higher in women. Pre-existing mental illness and cardiovascular risk factors increased the odds of post-COVID-19 syndrome in women, but not in men. Conversely, obesity was an independent predictor of post-COVID-19 syndrome in men, but not in women. Gender-related variables were independently associated with post-COVID-19 syndrome with self-assessed gender identity and a higher domestic stress level both increasing the odds of post-COVID-19 syndrome in women. In contrast, pregnancy during acute COVID-19 illness and responsibility for childcare seemed to protect women from experiencing post-COVID-19 syndrome. Our data indicate that post-COVID-19 sequalae and their predictors differ between men and women suggesting that a tailored and sex- and gender-sensitive approach of healthcare services may be required to support their needs.
Consistent with our observation, previous studies report that one to two thirds of patients did not return to baseline health within six months following acute SARS-CoV-2 infection.12,13 Not surprisingly, persistent symptoms were associated with worsened quality of life which has previously been reported to occur in one third of cases of mild COVID-19 cases and is consistent with our data.12 Of note, however, the incidence rates of post-COVID-19 syndrome vary widely in previous studies ranging from 10% to 96% of patients reporting persistent symptoms following acute illness.14-16 Differences in study populations, follow-up periods, and sample sizes likely affect the comparison of results across studies. Also, many previous reports have several limitations, including lack of an agreed-upon case definition and potential bias, as most reports excluded either outpatients or hospitalized patients. Re-hospitalisation due to persistent symptoms or complication of COVID-19 has been reported to occur in 9% to 20% of patients.17,18 The observed readmission rate of 5.5% in our study is lower than these estimates. Although we did not analyse the most common reasons for readmission, the lower re-hospitalization rate in our study likely reflects the lower acuity of illness in our cohort relating to differences in age and disease severity between study populations. Further research is needed to assess the extent to which improvements in the management of post-COVID-19 syndrome might reduce readmission rates.
In our study, reduced exercise tolerance and/or resilience was the most commonly reported symptom occurring in 41% of women and 43% of men with post-COVID-19 syndrome. While differences in study populations and outcome measurement are likely to affect the comparability of studies on post-COVID-19 syndrome, a relatively high prevalence of chronic fatigue, dyspnoea or exercise intolerance, and psychological symptoms have consistently been noted across studies.19,20 In particular, neuropsychiatric symptoms including depression and anxiety, cognitive impairment, headache or olfactory dysfunction seem to persist in a substantial number of patients (32% of individuals in our study) which is in accordance with previous studies.15,16 The incidence of persistent neuropsychiatric symptoms was significantly higher in women as compared to men in our study indicating that women exhibit a higher vulnerability to encountering long-term neurological and mental health consequences of COVID-19. The latter is supported by the fact that women reported a higher post-COVID-19 stress level as compared to men which is consistent with data from the SARS epidemic in 2003 demonstrating that female SARS survivors encountered higher stress levels and higher levels of depression and anxiety.21 As an involvement of angiotensin-converting enzyme (ACE) receptors has been suggested to be a gateway for this neurotropism,22 the known sex-specific expression levels of these receptors4 might be a potential mechanism driving the observed gender dysbalance in long-term neuropsychiatric consequences of SARS-CoV-2. Finally, intracerebral microembolisation has recently been described in patients with a severe disease course of COVID-19 and might play a role in neuropsychiatric long-term effects of the disease.23 The fact that men in our study were more often on antithrombotic or anticoagulant treatment as compared to women could have exerted a protective effect on the endothelium of brain capillaries and might have prevented long-term sequelae. Independent of the underlying mechanism, the high incidence of persistent neuropsychiatric symptoms in women calls for implementation of targeted treatments for individuals affected by post-COVID-19 syndrome.
In our statistical model, we noted an association between pre-existing diagnosis of mental illness and the incidence of post-COVID-19 syndrome in women, but not in men. While an association between known depression and chronic postviral fatigue has previously been described,24 our study is the first to observe that pre-existing mental disorders increases the risk of post-COVID-19 syndrome in women, but not in men. This sex-specific association might be due to the higher prevalence of mental illness in the female population which is also seen in our cohort. Also, a specific immune signature has previously been suggested to account for the persistence of fatigue following acute illness,25 and preliminary data indicate that dysfunctional immune cells with an autoimmune phenotype are present in patients with post-COVID-19 syndrome, particularly in those with persistent neurological symptoms.26 Thus, the higher prevalence of autoimmune disorders in our female study population as well as known sex-differences in immune responses to SARS-CoV-23 including a more robust T-cell response and a potential long-term hyperinflammatory state in women following SARS-CoV-2 infection27 might drive sex differences in the prevalence of post-COVID-19 syndrome. Also, the presence of lymphopenia in men being hospitalized for acute COVID-19 in our study supports this assumption as the latter might be associated with a lower number of autoreactive B- and T-cell lymphocytes. Accordingly, a recent study comparing 50 individuals suffering from post-COVID-19 syndrome to 50 SARS-CoV-2 negative controls found a higher prevalence of autoimmune disorders and elevated ANA titers in the post-COVID-19 cohort.19 Therefore, we propose to study this interaction in prospective well-powered studies, even though no consistent association between a persistent (auto)immune response to the virus and post-COVID-19 syndrome has been reported across multiple smaller studies.25 Furthermore, as a multifactorial aetiology of post-COVID-19 syndrome seems likely, our study emphasizes the importance of identifying clusters of sex-specific risk markers driving post-COVID syndrome in women and men so that multidisciplinary care can be offered to post-COVID patients.
Women in our study reported a higher domestic stress level as compared to men. Accordingly, an increased stress level at home was a significant predictor of post-COVID-19 syndrome in women, but not in men. This is consistent with recent work demonstrating an association between lacking social support, female sex and COVID-19-related posttraumatic stress disorder15 indicating that women suffer more emotional reactivity and stress response symptoms. Although no data exist regarding the impact of domestic emotional stress on viral disease outcomes, our data are also in line with previous cardiovascular studies demonstrating that family and marital stress is a strong and independent risk factor for the progression of atherosclerosis in women, while relative protection from the disease was obtained from partner support.28 Consequently, our study emphasizes the importance of psychosocial interventions with an emphasis on coping with family-related stress exposure in women affected by post-COVID-19 syndrome.29 The fact that household responsibility (in men), responsibility for childcare (in women), and pregnancy at the time of acute SARS-CoV-2 infection all had protective effects on post-COVID-19 syndrome may indicate that taking care of other individuals may either allow less time for self-reflection or provide a base for more positive thinking and optimistic attitude during recovery from COVID-19. These findings suggest that reduced social contact and loneliness might exacerbate symptoms of post-COVID syndrome. Finally, it is worth mentioning that being a single parent was associated with a trend towards higher odds of post-COVID-19 syndrome in the overall association model. Given that being a single parent in Switzerland usually comprises childcare responsibilities as well as full-time employment, it is conceivable that employment level and the resulting exposure to a higher level of stress also plays a role in post-COVID-19 risk prediction.
Our study has several limitations related to its cross-sectional and observational study design. First, like all observational studies, residual confounding due to unmeasured variables in our dataset is possible. However, the risk factors in our study covered many aspects of demographic characteristics, pre-existing diseases, sex-and gender-specific variables, and acute COVID-19 simultaneously. Second, increasing awareness of post-COVID-19 syndrome during the last few months may have resulted in more frequent reporting of health issues by participants over the course of the study. Third, compared to individuals not participating in our study, participants in our study were more often hospitalized during acute COVID-19, which could increase our estimate of the prevalence of post-COVID-10 syndrome. Conversely, post-COVID-19 syndrome prevalence may have been underestimated if individuals with prolonged and severe symptoms or cognitive dysfunction were more likely not to complete the questionnaire. Fourth, the effect that more men than women died during acute infection may have shifted the appearance of post-COVID-19 syndrome towards the female demographic group. However, the number of cases contributing to this phenomenon are small and likely did not cause a statistically significant effect. Finally, self-selection or other biases may have occurred if individuals who are more concerned with their health were more likely to participate.
Taken together, our multicentre study is the first to our knowledge to demonstrate that characteristics and risk factors of post-COVID-19 syndrome differ between men and women. While 37% of individuals in the current study showed symptoms consistent with post-COVID-19 syndrome after a mean follow-up time of 197 days, our results demonstrate that women in our cohort were at particular high risk of developing post-COVID-19 syndrome. Our data indicate that both biological variables as well as gender identity and social roles were independent predictors of post-COVID-19 syndrome. We emphasize that multidisciplinary and sex- and gender-tailored therapeutic strategies are of particular importance in post-COVID-19 syndrome given that women receive less often intensive diagnostic and treatment interventions as compared to men.30 Sex- and gender-specific research on the underlying pathophysiology of post-COVID-19 syndrome is now urgent to better understand symptom development and identify targets for intervention.
Data Availability
Based on the Business Administration System for Ethics Committees (BASEC) ethics approval, the non-anonymized raw data cannot be shared publicly. However, anonymised data that underlie the results reported in this article will become available to interested parties for non-commercial reasons, after the publication upon reasonable requests made to the corresponding author. Data requestors will need to sign a data access agreement.
Data Availability
Data sharing
Based on the Business Administration System for Ethics Committees (BASEC) ethics approval, the non-anonymized raw data cannot be shared publicly. However, anonymised data that underlie the results reported in this article will become available to interested parties for non-commercial reasons, after the publication upon reasonable requests made to the corresponding author. Data requestors will need to sign a data access agreement.
Dissemination to participants and related patient and public communities
The size of the study population precludes direct dissemination to participants.
Declarations
Research ethics approval
The study was approved by the responsible ethics committee of the Canton of Basel, Switzerland (EKNZ; BASEC-Nr 2020-01311). Informed consent was obtained from all participants or their legal representative, as appropriate.
Competing interests
CG has received research grants from the Novartis Foundation and speaker’s fees from Sanofi Genzyme, Switzerland outside of the submitted work. The University Hospital Zurich (CG, RRB, APP, MM, PAK) holds a research contract with GE Healthcare outside of the submitted work. CG and AM have received research grants from Bayer Pharmaceuticals outside of the submitted work. JCS and TS reports (full departmental disclosure) grants from Orion Pharma, Abbott Nutrition International, B. Braun Medical AG, CSEM AG, Edwards Lifesciences Services GmbH, Kenta Biotech Ltd, Maquet Critical Care AB, Omnicare Clinical Research AG, Nestle, Pierre Fabre Pharma AG, Pfizer, Bard Medica S.A., Abbott AG, Anandic Medical Systems, Pan Gas AG Healthcare, Bracco, Hamilton Medical AG, Fresenius Kabi, Getinge Group Maquet AG, Dräger AG, Teleflex Medical GmbH, Glaxo Smith Kline, Merck Sharp and Dohme AG, Eli Lilly and Company, Baxter, Astellas, Astra Zeneca, CSL Behring, Novartis, Covidien, Nycomed, and Phagenesis, outside of the submitted work. The money went into departmental funds, no personal financial gain applies. All other authors declare: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years, no other relationships or activities that could appear to have influenced the submitted work.
Funding
This project is funded by the Swiss National Science Foundation (Project #196140, to CG, CEG, and VRZ), the LOOP Zurich (CG, VRZ, UH) and an unrestricted research grant from the intensive care unit (ICU) research foundation of the University Hospital of Basel (CEG). The funders of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report. All authors had full access to the anonymized data in the study and share final responsibility for the decision to submit for publication.
Authors’ contributions
CG, CEG, and VRZ conceptualized and designed the Swiss COGEN study. CEG, CS, SB, KPB, NH coordinated the study. CEG, PO, SB, AM, NZ prepared the study data. UH, MD, and CEG, SB, and CG have verified the underlying data, performed the statistical analysis and prepared tables and figures. CG, CEG, CS, UH, MD, and NL wrote the first manuscript draft. VRZ, VT, PAK, RRB, MM, APP, RS, AZ, JHB, AF, MS, HP, JCS, RT, GMK, JB, and STS contributed to interpretation of the results and critical revision of the manuscript. SB, KPB, CEG, CG, SDB, CA, DP, and BW implemented and coordinated the recruitment of study participants and biobank samples. TS, JCS, ADC, CH, MP, DFS, LM, MCG, ASZ, LC, DJS, AH, MG, NM, AR, FF, AT, JB, and AP contributed to the enrolment of study participants and data collection. All authors approved the final manuscript. CG is the guarantor for the study. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Acknowledgement
We would like to thank the study administration staff including Elvira Krämer, Livia Krüger, Mariano Paredes Heck, Mina Qadirie, Marie-Louise Sieber, Anna Zaiser, and Anja Zabel as well as the staff of the Department of Nuclear Medicine of the University Hospital Zurich and the Intensive Care Units of the University Hospital Basel and the University Hospital Zurich for their excellent work and dedication to this study. And last, we thank all the study participants for their valuable time and commitment to the Swiss COGEN Cohort.
References



