
ABSTRACT
Background Women and gender-diverse individuals face disproportionate socioeconomic burden during COVID-19. We compared mental health symptom changes since pre-COVID-19 by sex or gender.
Methods We searched MEDLINE, PsycINFO, CINAHL, EMBASE, Web of Science, China National Knowledge Infrastructure, Wanfang, medRxiv, and Open Science Framework December 31, 2019 to March 22, 2021 for studies that reported mental health outcomes prior to and during COVID-19 by sex or gender. We conducted restricted maximum-likelihood random-effects meta-analyses.
Results All 11 included studies (9 unique cohorts) compared females or women to males or men; none included gender-diverse individuals. Continuous symptom change differences were not statistically significant for depression (standardized mean difference [SMD]= 0.15, 95% CI - 0.09 to 0.39; 3 studies, 4,159 participants; I2=77%) and stress (SMD= -0.09, 95% CI -0.21 to 0.02; 3 studies, 1,217 participants; I2=0%), but anxiety (SMD= 0.14, 95% CI 0.01 to 0.26; 3 studies, 4,028 participants; I2=34%) and general mental health (SMD= 0.15, 95% CI 0.12 to 0.18; 2 studies, 15,590 participants; I2=0%) worsened more among females or women than males or men. There were no significant differences in changes in proportion above a cut-off: anxiety (difference= 0.00, 95% CI -0.01 to 0.02; 2 studies, 6,684 participants; I2=0%), depression (difference= 0.12, 95% CI -0.04 to 0.28; 1 study, 217 participants), general mental health (difference= -0.03, 95% CI -0.09 to 0.04; 3 studies, 18,985 participants; I2=94%), stress (difference= 0.04, 95% CI -0.11 to 0.18; 1 study, 217 participants).
Interpretation Mental health outcomes did not differ or were somewhat worse among women than men.
The COVID-19 pandemic has caused over 3.8 million deaths and disrupted social and economic activities across the globe.1,2 Men infected with COVID-19 are at greater risk of intensive care admission and death than women,3,4 but socioeconomic burden has disproportionately impacted women.5-12 Economically, most single parents are women, and women earn less, are more likely to live in poverty, and hold less secure jobs than men, which heightens vulnerability during COVID-19.5,8-11 Women are overrepresented in health care, which involves infection risk.5-10 They provide most childcare and family elder care.5,8-10 Intimate partner violence has increased with the majority directed towards women.5,7-10,12 Sex and gender minority individuals may also face additional socioeconomic challenges during COVID-19.13,14 Some studies have reported that COVID-19 mental health effects have been greater for women than men.5,15-18 These, however, have been cross-sectional studies that evaluated proportions of participants above cut-offs on self-report measures without consideration of pre-COVID-19 differences, even though mental health disorders and symptoms are more common among women.19-23
Evidence from longitudinal cohorts that compare mental health symptoms pre-COVID-19 to during COVID-19 is needed. We are conducting a series of living systematic reviews on COVID-19 mental health,24-26 including mental health changes.26 The objective of this study was to compare mental health changes by sex or gender.
METHODS
Our series of living systematic review was registered in PROSPERO (CRD42020179703), and a protocol was posted pre-initiation (https://osf.io/96csg/). The present study is a sub-study of our main mental health changes review.26 Results are reported per the PRISMA statement.27
Study Eligibility
For our main symptom changes review, studies on any population were included if they compared mental health outcomes assessed between January 1, 2018 and December 31, 2019, when China first reported COVID-19 to the World Health Organization,28 to outcomes collected January 1, 2020 or later. Compared samples had to include at least 90% of the same participants pre-COVID-19 and during COVID-19 or use statistical methods to account for missing data. Studies with < 100 participants were excluded for feasibility and due to their limited relative value. For the present analysis, studies had to report mental health outcomes separately by sex (assignment based on external genitalia, usually at birth; e.g., female, male, intersex) or gender (socially constructed characteristics of roles and behaviours; e.g., woman, man, trans woman, trans man, non-binary).29
Search Strategy
MEDLINE (Ovid), PsycINFO (Ovid), CINAHL (EBSCO), EMBASE (Ovid), Web of Science Core Collection: Citation Indexes, China National Knowledge Infrastructure, Wanfang, medRxiv (preprints), and Open Science Framework Preprints (preprint server aggregator) were searched using a strategy designed by an experienced health science librarian. The China National Knowledge Infrastructure and Wanfang databases were searched using Chinese terms based on our English-language strategy. The rapid project launch did not allow for formal peer review, but COVID-19 terms were developed in collaboration with other librarians working on the topic. See Appendix 1 for search strategies. The initial search was conducted from December 31, 2019 to April 13, 2020 with automated daily updates. We converted to weekly updates on December 28, 2020 to increase processing efficiency.
Selection of Eligible Studies
Search results were uploaded into DistillerSR (Evidence Partners, Ottawa, Canada). Duplicate references were removed. Then two reviewers independently evaluated titles and abstracts in random order; if either reviewer believed a study was potentially eligible, it underwent full-text review by two independent reviewers. Discrepancies at the full-text level were resolved by consensus, with a third reviewer consulted if necessary. An inclusion and exclusion coding guide was developed, and team members were trained over several sessions. See Appendix 2.
Data Extraction
For each eligible study, data were extracted by a single reviewer using a pre-specified form with validation by a second reviewer. Reviewers extracted (1) publication characteristics (e.g., first author, year, journal); (2) population characteristics and demographics, including eligibility criteria, recruitment method, number of participants, assessment timing, age; (3) mental health outcomes, which were defined broadly and could have included, for example, symptoms of anxiety, depression, stress, loneliness, anger, grief, or other emotional disturbance; (4) if studies reported outcomes by sex or gender or used these terms inconsistently (e.g., described using gender but reported results for females and males, which are sex terms); and (5) if sex or gender were treated as binary or categorical.
Adequacy of study methods and reporting was assessed using an adapted version of the Joanna Briggs Institute Checklist for Prevalence Studies, which assesses appropriateness of the sampling frame for the target population, appropriateness of recruiting methods, sample size, description of setting and participants, participation or response rate, outcome assessment methods, standardization of assessments across participants, appropriateness of statistical analyses, and follow-up.30 See Appendix 3. Discrepancies were resolved between reviewers with a third reviewer consulted if necessary.
Statistical Analyses
For changes from pre-COVID-19 to COVID-19, in continuous and dichotomous outcomes, within sex or gender groups, we presented results as positive when mental health worsened pre-COVID-19 to COVID-19 and negative when it improved. For continuous outcomes, separately for each sex or gender group, we extracted a standardized mean difference (SMD) effect size with 95% confidence intervals (CIs) for change from pre-COVID-19 to COVID-19. If not provided, we calculated it using Hedges’ g,31 as described by Borenstein et al.32 For each study, we then calculated a Hedges’ g difference in change between sex or gender groups with 95% CI.
For studies that reported proportions of participants above a scale cut-off, for pre-COVID-19 and COVID-19 proportions, if not provided, we calculated a 95% CI using Agresti and Coull’s approximate method for binomial proportions.33 We then extracted or calculated the proportion change in participants above the cut-off, along with 95% CI, for each sex or gender group. If 95% CIs were not reported, we generated them using Newton’s method for differences between binomial proportions based on paired data.34 To do this, which requires the number of cases at both assessments, which is not typically available, we assumed that 50% of pre-COVID-19 cases continued to be cases during COVID-19 and confirmed that results did not differ substantively if we used values from 30% to 70% (all 95% CI end points within 0.02; see Appendix 4). Finally, we calculated a difference of the proportion change between sex or gender groups with 95% CI.35
Meta-analyses were done to synthesize differences between sex or gender groups in SMD change for continuous outcomes and in proportion change for dichotomous outcomes via restricted maximum-likelihood random-effects meta-analysis. Heterogeneity was assessed with the I2 statistic. Meta-analysis was performed in R (R version 3.6.3, RStudio Version 1.2.5042), using the metacont and metagen functions in the meta package.36 Forest plots were generated using the forest function in meta. Positive values indicated more relatively worse changes in mental health for females or women compared to males or men.
RESULTS
Search Results and Selection of Eligible Studies
As of March 22, 2021, there were 45,777 unique references identified and screened for potential eligibility, of which 45,251 were excluded after title and abstract review and 394 after full-text review. Of 132 remaining articles, 121 were excluded because they compared symptoms at different points during the pandemic but not to pre-COVID-19 data or because they did not compare results by sex or gender, leaving 11 included studies that reported data from 9 cohorts (Figure 1).

PRISMA flow diagram.
Characteristics of Included Studies
Four publications37-40 reported on two large, national, probability-based samples from the United Kingdom (N = 10,918 to 15,376)37,38 and the Netherlands (N = 3,983 to 4,064).39,40 One study41 reported on adults from a national sample from China (N = 6,467). Two studies42,43 assessed young adults; one reported on a sample of twins from the United Kingdom (N = 3,563)42 and another on a sample from Switzerland (N = 786).43 One study assessed adolescents from Australia (N = 248),44 and three studies45-47 assessed undergraduate students from China (N = 4,085),45 India (N = 217),46 and the United Kingdom (N = 214).47 Four studies assessed anxiety symptoms,41,42,44,46 3 depression symptoms,42,44,46 4 (2 cohorts) general mental health,37-40 and 3 stress.43,46,47 Table 1 shows study characteristics. All studies compared women and men or females and males; none included other sex or gender groups. Results during COVID-19 were assessed between March and June 2020 for all studies. Two cohorts also reported results from September 202038 and November to December 2020.40
Characteristics of included studies (N=11)
Adequacy of Study Methods and Reporting
Four studies (2 cohorts)37-40 were rated as “yes” for adequacy for all items39,40 or “yes” on all items except one, which was rated “unclear”.37,38 Other studies were rated “no” for 1-3 items (plus 0-2 unclear ratings)41,43-47 or “no” on none but unclear on 3 items.42 There were 5 studies43- 47 rated “no” for appropriate sampling frame (45%), 7 “no” or “unclear” for adequate response rate and coverage (64%),37,38,41-44,47 and 4 “no” or “unclear” for follow-up response rate and management (36%).41,42,44,47 See Table 2.
Adequacy of methods and reporting of included studies (N=11)
Mental Health Symptom Changes
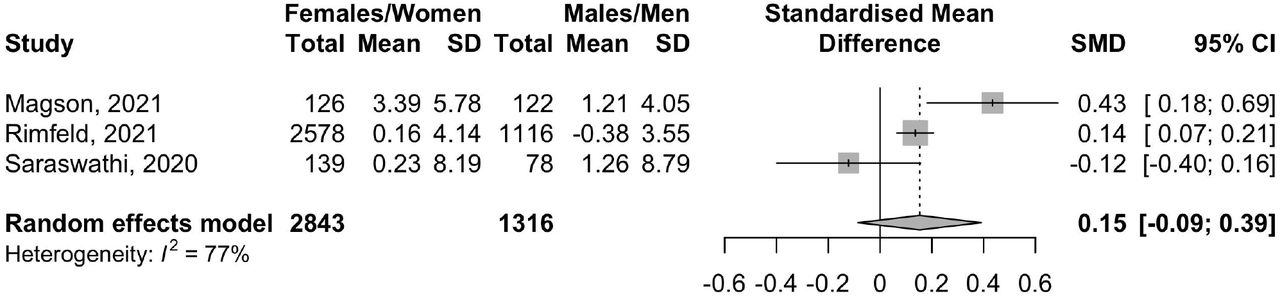
There was a total of 11 comparisons of continuous score changes and 9 of proportion changes; in all but one, females or women had higher scores or proportions above a cut-off pre-COVID-19. Mental health scores and symptom changes for all outcome domains are reported separately by sex or gender groups in Table 3. Differences in continuous and dichotomous changes by sex or gender are shown in Figures 2 to 5. Estimates of difference in change by sex or gender were close to zero and not statistically significant for anxiety symptoms with dichotomous outcomes (Figure 2b; proportion change difference = 0.00, 95% CI -0.01 to 0.02; N = 2 studies,41,46 6,684 participants; I2 = 0%), depression symptoms with continuous (Figure 3a; SMD change difference = 0.15, 95% CI -0.09 to 0.39; N = 3 studies,42,44,46 4,159 participants; I2 = 77%) and dichotomous outcomes (Figure 3b; proportion change difference = 0.12, 95% CI - 0.04 to 0.28; N = 1 study,46 217 participants), general mental health dichotomous outcomes (Figure 4b [all results from early 2020]; proportion change difference = -0.03, 95% CI -0.09 to 0.04; N = 3 studies,38,39,45 18,985 participants; I2 = 94%), and stress with continuous (Figure 5a; SMD change difference = -0.09, 95% CI -0.21 to 0.02; N = 3 studies,43,46,47 1,217 participants; I2 = 0%) and dichotomous outcomes (Figure 5b; proportion change difference = 0.04, 95% CI - 0.11 to 0.18; N = 1 study,46 217 participants). Of the 3 studies that reported dichotomous general mental health, 2 also reported outcomes from late 2020; when those results were used, the null finding did not change (Figure 4c; proportion change difference = 0.00, 95% CI -0.02 to 0.03; N = 3 studies,38,40,45 19,067 participants; I2 = 67%).
Outcomes from Included Studies by Sex or Gendera


Forest plots of standardized mean difference of the difference in change in continuous anxiety symptom scores (2a) and the difference in change in proportion above a cut-off (2b) between females or women and males or men. Positive numbers indicate more negative change in anxiety symptoms in females or women compared to males or men.


Forest plots of standardized mean difference of the difference in change in continuous depression symptom scores (3a) and the difference in change in proportion above a cut-off (3b) between females or women and males or men. Positive numbers indicate more negative change in depression symptoms in females or women compared to males or men.



Forest plots of standardized mean difference of the difference in change in continuous general mental health scores (4a) and the difference in change in proportion above a cut-off (4b) between females or women and males or men. Positive numbers indicate more negative change in general mental health in females or women compared to males or men. Figures 4a and 4b reflect COVID-19 mental health measured in early 2020, whereas 4c reflects measurements from late 2020 for Daly38 and van der Velden.39


Forest plots of standardized mean difference of the difference in change in continuous stress scores (5a) and the difference in change in proportion above a cut-off (5b) between females or women and males or men. Positive numbers indicate more negative change in stress in females or women compared to males or men.
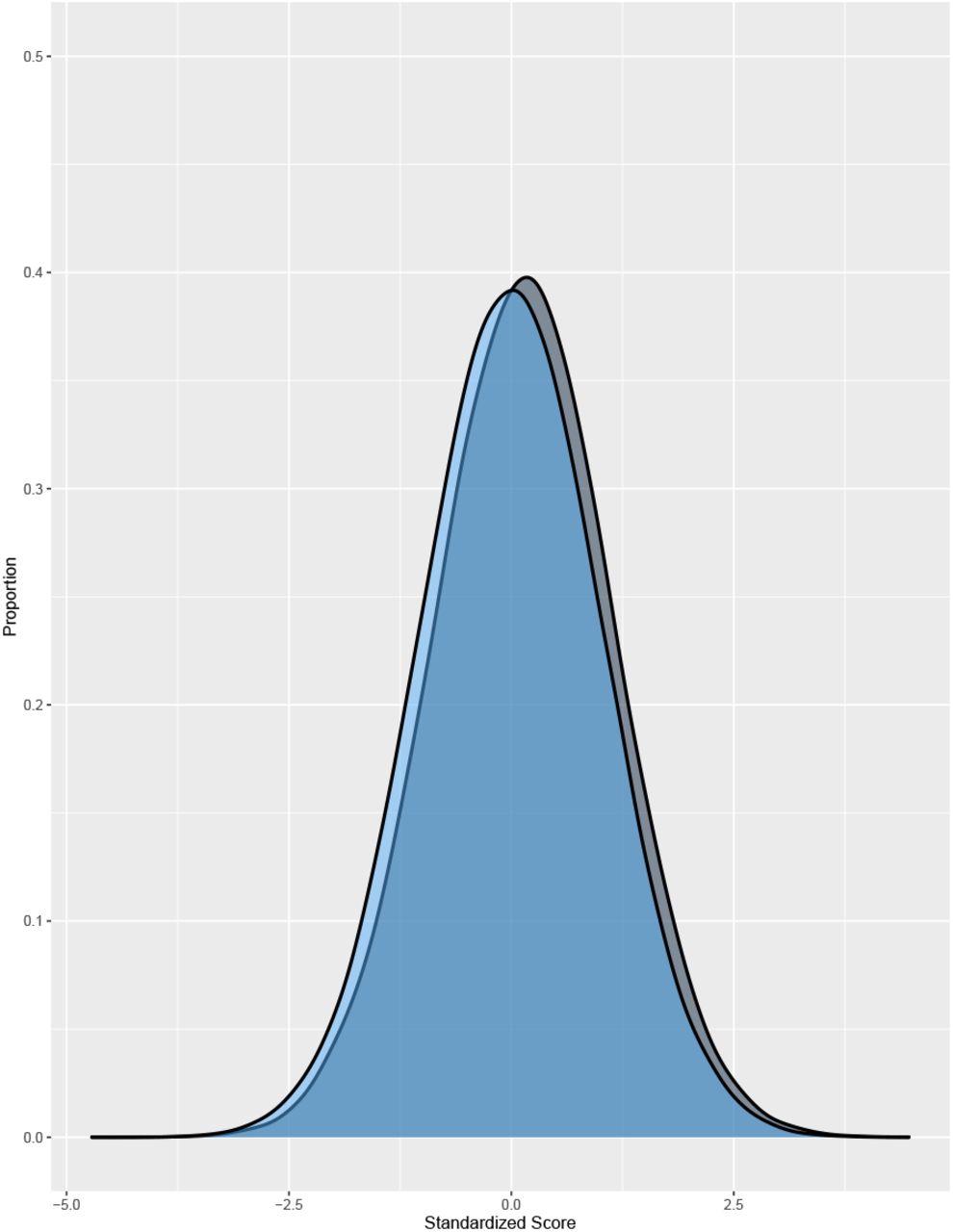
Anxiety, measured continuously, worsened significantly more for females or women than for males or men (Figure 2a; SMD change difference = 0.14, 95% CI 0.01 to 0.26; N = 3 studies,42,44,46 4,028 participants; I2 = 34%). General mental health, measured continuously, also worsened more for females or women than for males or men in early COVID-19 (Figure 4a; SMD difference in change = 0.15, 95% CI 0.12 to 0.18; N = 2 studies,37,47 15,590 participants; I2 = 0%). This was predominantly based on a large population-based study from the United Kingdom.37 That study did not report results from fall 2020 for continuous outcomes, but as shown in Table 3 and Figures 4b and 4c, the difference in change between females or women and males or men decreased between early and late 2020 for dichotomous outcomes in the same cohort.38 The magnitude of both statistically significant differences was small (see Figure 6).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Illustration of the magnitude of change for SMD = 0.15 assuming a normal distribution. The hypothetical blue distribution represents pre-COVID-19 scores, and the grey distribution represents post-COVID-19 scores with a mean symptom increase of SMD = 0.15.
DISCUSSION
The COVID-19 pandemic has affected women and gender minorities disproportionately.5-14 We reviewed evidence from studies that reported mental health changes from pre-COVID-19 to COVID-19 by sex or gender. We examined 11 studies (9 cohorts) that reported on anxiety symptoms, depression symptoms, general mental health, and stress. We compared females or women with males or men; no studies compared gender minorities with any other group. Syntheses of continuously measured anxiety symptoms (SMD = 0.14, 95% CI 0.01 to 0.26) and general mental health (SMD = 0.15, 95% CI 0.12 to 0.18) found that mental health worsened more for females or women than males or men, but the magnitude was small and not typically considered clinically important.48 No other mental health outcomes changed more for females or women than males or men.
Sex and gender differences in mental health disorder prevalence, symptoms, and risk factors are well-established.49-52 Likely risk factors include gender inequities and discrimination, higher rates of interpersonal stressors, and violence,53,54 and many of these risk factors have been exacerbated for women during COVID-19.5-12 Overall mental health does not appear to have changed substantively for the general population based on our main systematic review,26 but there is concern that there could, nonetheless, be important sex- or gender-based differences. We found small symptom change differences that reflect relative worsening for women for 2 of 8 outcomes assessed, but no differences appeared to be clinically meaningful.
Based on our findings, it is possible that despite the challenges women have faced, most have been resilient and that the mental health disaster that has been predicted by many has not occurred.55 This finding departs from what has been reported in some research and by the media. Three factors may feed this discrepancy. One is the publication of many cross-sectional studies that report proportions above cut-offs on self-report measures, which are not designed for that purpose, and assume that high numbers must not have been present pre-COVID-19.26 A second is the use of surveys that ask questions about well-being with COVID-19 explicitly assigned as a cause; illustrating the pitfalls of this, a study of over 2,000 young Swiss adult men found significant angst when questions were asked in this way, but no changes in validated measures of depression symptoms and stress from pre-COVID.56 A third reason relates to news media reports that emphasize dramatic events and anecdotes without evidence that demonstrates changes.55
Strengths of our study include the use of rigorous systematic review methods; searching 9 databases, including Chinese-language databases, without language restrictions; and including studies that enabled the direct comparison of mental health changes by sex or gender. There are limitations to consider. First, this review only included 11 studies from 9 cohorts, and many had limitations related to study sampling frames and recruitment methods, follow-up rates, and management of missing data. Second, heterogeneity was high for some meta-analyses. Third, there were not enough studies to attempt sub-group analyses by additional sociodemographic or other factors. Fourth, we did not identify any studies that compared results from gender-diverse individuals to other gender groups.
In sum, we identified small sex- or gender-based differences for anxiety symptoms and general mental health, continuously measured, but other outcomes (continuous depression symptoms and stress; dichotomous anxiety symptoms, depression symptoms, general mental health, stress) were not different by sex or gender. These are aggregate results, though, and many individuals have certainly experienced negative mental health changes related to increased socioeconomic burden. Mental health changes should continue to be monitored in COVID-19, taking into consideration sex and gender, and studies should examine reasons for what appears to be resilience among many women despite facing disproportionate hardships in the pandemic.
Data Availability
All data used in the study are available in the manuscript and its tables or online at https://www.depressd.ca/covid-19-mental-health.
Appendix 1.
Search Strategies
Search strategies can be found in the project folder on the Open Science Framework: https://osf.io/2zh9n/
Appendix 2.
Title and Abstract and Full-Text Review Inclusion and Exclusion Criteria Coding Guides
Title and Abstract Coding Criteria
MENTAL HEALTH SYMPTOM CHANGES CODING CRITERIA:
No: not original human data or a case study or case series.
If it is clear from the title and abstract that the article is not an original report of primary data, but, for example, a letter, editorial, systematic review or meta-analysis, or it is a single case study or case series, then it is excluded. Studies reporting only on animal, cellular, or genetic data are also excluded. Conference abstracts are included.
No: not a study of any population affected by the COVID-19 outbreak.
If it is clear from the title or abstract that the study is not about any population affected by the COVID-19 outbreak, it is excluded. Studies that include fewer than 100 subjects, are excluded.
No: not a study which reports mental health symptom changes over a demarcated period.
If it is clear from the title or abstract that the study does not report proportions of participants meeting diagnostic criteria using a validated diagnostic interview or validated mental health scale, or proportions of symptoms (based on a threshold or measured continuously) prior to and after a delineated event related to COVID-19,then it will be excluded. Delineated events for pre-post comparisons may include pandemic announcements, social isolation regulations, etc. Pre- and post-samples must include the same cohort, not representative samples. Pre- and post-samples should have less than 10% missing data, or should statistically account for missing data if N between samples varies by more than 10%.
Yes: study eligible for inclusion in full-text review.
Full Text Coding Criteria
MENTAL HEALTH SYMPTOM CHANGES CODING CRITERIA:
No: not original human data or a case study or case series.
If the article is not an original report of primary data, but, for example, a letter, editorial, systematic review or meta-analysis, or it is a single case study or case series, then it is excluded. Studies reporting only on animal, cellular, or genetic data are also excluded. Conference abstracts are included.
No: not a study of any population affected by the COVID-19 outbreak.
If the study is not about any population affected by the COVID-19 outbreak, it is excluded. Studies that include fewer than 100 subjects, are excluded.
No: not a study which reports mental health symptom changes over a demarcated period.
If it the study does not report proportions of participants meeting diagnostic criteria using a validated diagnostic interview or validated mental health scale, or proportions of symptoms (based on a threshold or measured continuously) prior to and after a delineated event related to COVID-19,then it will be excluded. Delineated events for pre-post comparisons may include pandemic announcements, social isolation regulations, etc. Delineated events for pre-post comparisons may include pandemic announcements, social isolation regulations, etc. Pre- and post-samples must include the same cohort, not representative samples. Pre- and post-samples should have less than 10% missing data, or should statistically account for missing data if N between samples varies by more than 10%.
Yes: study eligible for inclusion in systematic review.
Appendix 3: Adequacy of Study Methods and Reporting
Q1. Was the sample frame appropriate to address the target population?
Yes: The sampling frame was a true or close representation of the target population.
No: The sampling frame was NOT a true or close representation of the target population. Unclear: Not enough information provided to determine.
Q2. Were study participants recruited in an appropriate way?
Yes: A census was undertaken, OR, some form of random selection was used to select the sample (e.g. simple random sampling, stratified random sampling, cluster sampling, systematic sampling).
No: A census was NOT undertaken, AND some form of random selection was NOT used to select the sample.
Unclear: Not enough information provided to determine.
Q3. Was the sample size adequate?
Yes: There is evidence that the authors conducted a sample size calculation to determine an adequate sample size OR the study was large enough (e.g., a large national survey) whereby a sample size calculation is not required. In these cases, sample size can be considered adequate. If at least 200 participants are included for continuous outcomes and 250 for proportions, this is considered low risk.
No: The authors did not reach their intended sample size, or no sample size calculation is provided and there are < 100 participants for continuous outcomes, or < 125 for proportions.
Unclear: No sample size calculation is provided, and between 100-199 participants are included for continuous outcomes or between 125-249 for proportions.
Q4. Were the study participants and setting described in detail?
Yes: Data included age, sex, and at least 1 socioeconomic indicator (e.g., income, education, work status).
No: The minimum sociodemographic variables have not been reported.
Unclear: Not stated
Q5. Was the response rate adequate and was the data analysis conducted with sufficient coverage?
Yes: The overall response rate or response rate for intended subgroups was >/=75%, OR, an analysis was performed that established that there was not a substantive difference in relevant demographic characteristics between responders and non-responders within a subgroup (if non-response too high (e.g., > 50%), code “No”)
No: The overall response rate or response rate for subgroups was <75%, and if any analysis comparing responders and non-responders was done, it showed a meaningful difference in relevant demographic characteristics between responders and non-responders.
Unclear: Not enough information provided to determine.
Q6. Were valid methods used for the identification of the outcome variable?
Yes: The study instrument had been shown to have reliability and validity, e.g., test-retest, piloting, validation in a previous study, etc.
No: The study instrument had NOT been shown to have reliability or validity.
Unclear: Not stated.
Q7. Was the mental health outcome measured in a standard, reliable way for all participants?
Yes: All self-report data were collected directly from the participants. Any clinical interview data includes at least information about the interviewers’ level of education or training received. The same mode of data collection was used for all participants. All aspects of this question must be present (where relevant).
No: In some instances, data were collected from a proxy (e.g., a spouse). The qualifications of clinical interviewers are not reported or not appropriate. The same mode of data collection was NOT used for all participants. If any aspects of this item are absent, it is high risk.
Unclear: Not stated.
Q8. Was there appropriate statistical analysis?
Yes: Continuous variables report (1) mean (SD) of change or (2) pre mean (SD) and post mean (SD) with/out correlation between pre and post scores. For dichotomous variables, numerator, denominator, and percentages are clearly reported. Continuous variables are not artificially dichotomized. The statistical analyses section is detailed enough for readers to understand change scores (see STROBE reporting guidelines, if necessary).
No: Continuous variables do not include a report of the (1) mean (SD) of change or (2) pre mean (SD) and post mean (SD) with/out correlation between pre and post scores. For dichotomous variables, the numerator, denominator, or percentages are not clearly reported. The statistical analyses section does not clearly describe the methods used to assess change scores.
Q9. Was the follow-up rate adequate, and if not, was the low follow-up rate managed appropriately?
Yes: At least 75% of those who participated in the pre-COVID-19 assessment(s) provided follow-up responses and had their responses included in the follow-up, OR, an analysis was performed that showed no substantive difference in relevant demographic characteristics between participants who stayed in the study and drop-outs (if dropout too high (e.g. > 50%), code “No”).
No: Less than 75% of those participated in the pre-COVID-19 assessment(s) provided responses and had their responses included in the follow-up, and if any analysis comparing participants who stayed in the study and drop-outs was done, it showed a substantive difference in relevant demographic characteristics between the two groups.
Unclear: Not stated.
Appendix 4. Confidence Intervals for Proportion Change When Using 30% and 70% of pre-COVID-19 Cases were Cases during COVID-19: Calculated for Studies that Did Not Provide 95% Confidence Intervals for Change
Footnotes
Funding: The study was funded by the Canadian Institutes of Health Research (CMS-171703; MS1-173070) and McGill Interdisciplinary Initiative in Infection and Immunity Emergency COVID-19 Research Fund (R2-42). YWu and BL were supported by Fonds de recherche du Québec – Santé (FRQS) Postdoctoral Training Fellowships. DBR was supported by a Vanier Canada Graduate Scholarship. AB was supported by a FRQS senior researcher salary award. BDT was supported by a Tier 1 Canada Research Chair.
Declaration of Competing Interests: All authors have completed the ICJME uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years. All authors declare no relationships or activities that could appear to have influenced the submitted work. No funder had any role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Data Sharing: All data used in the study are available in the manuscript and its tables or online at https://www.depressd.ca/covid-19-mental-health.
REFERENCES



