
Abstract
Background Currently, only dexamethasone, tocilizumab and sarilumab have conclusively been shown to reduce mortality of COVID-19. No drug for prevention or treatment in earlier stages of COVID-19 are yet found; although several new candidates including ivermectin, dutasteride, baricitinib, budesonide and colchicine are being studied with some early promising results. Safe and effective treatments will need to be both affordable and widely available globally.
Objectives This analysis will estimate and compare potential generic production costs of a selection of COVID-19 drug candidates with international list prices.
Methods Costs of production for new and potential COVID-19 drugs (dexamethasone, ivermectin, dutasteride, budesonide, baricitinib, tocilizumab, sarilumab and colchicine) were estimated using active pharmaceutical ingredients (API) data extracted from global shipping records. This was compared with national pricing data from low, medium, and high-income countries. Annual API export volumes from India were used to estimate the current availability of each drug.
Results Repurposed therapies can be generically manufactured at very low per-course costs: ranging from $2.58 for IV dexamethasone (or $0.19 orally) to $0.12 for ivermectin. No export price data was available for baricitinib, tocilizumab or sarilumab. When compared against international list prices, we found wide variations between countries. Drug API availability was generally good, with colchicine being the most available with sufficient annual API exported for 59.8 million treatment courses.
Conclusions Successful management of COVID-19 will require equitable access to treatment for all populations, not just those able to pay high prices. Analysed drugs are widely available and affordable, whilst IV treatment courses are more expensive.
Introduction
One year on from the global COVID-19 pandemic outbreak, drug repurposing remains an important focus. Given the high daily global incidence, and the emergence of new variants of concern, a strategy overly dependent on vaccines may not be fully effective.
Despite regulatory approvals, vaccine hesitancy, production bottlenecks, and “vaccine nationalism” [1] are causing deployment difficulties. As of February 2021, over 130 countries had still not administered a single vaccine [2]. By March 2021, 86% of vaccine doses were secured by high-and upper-middle income countries, with only 0.1% of vaccines heading to low-income countries [3]. For many global south countries, mass vaccination required to suppress transmission and achieve herd immunity may remain unattainable for several years. Even in countries with strong vaccination programs, many COVID-19 patients will require treatment.
In our 2020 analysis of potential costs of generic production for numerous drug candidates then under active clinical investigation [4], we proposed four key tests:
Efficacy – drugs should demonstrate therapeutic clinical efficacy and/or prophylactic properties.
Safety – drugs should be safe and well tolerated in all populations with minimal side effects or drug interactions.
Affordability – drugs should be widely accessible as low-cost generics so that all populations can equitably afford the cost of treatment.
Availability – drugs must be readily available or have the potential for rapid up-scaled production to meet global demand.
Many previously analysed and once promising drugs are now proven ineffective, or even harmful. Hydroxychloroquine [5] is one such high-profile example; and despite FDA approval, remdesivir demonstrated no clinical benefit except for shorter duration of hospitalisation [6]. Furthermore, large-scale studies such as SOLIDARITY and RECOVERY have found other previously leading candidates such as lopinavir/ritonavir [6,7], interferon beta-1a [6] and azithromycin [8] to have no clinical benefit.
Other repurposed drugs have emerged successfully from the clinical trials pipeline. Dexamethasone was first found to increase survival in severe COVID-19 patients requiring oxygen therapy, with further benefit for those in critical care [9]. This was supplemented by data showing tocilizumab and sarilumab - monoclonal antibody interleukin-6 (IL-6) receptor inhibitors, also producing improved outcomes in critical care patients [10]. However, an effective anti-viral agent for asymptomatic, mild, or moderate patients that limits progression and treats COVID-19 is still absent. No drug is currently approved for pre- or post-exposure prophylaxis, as well as no approved therapies to reduce viral load or time to viral clearance.
Currently, there is considerable interest in ivermectin, an anti-parasitic and anti-inflammatory [11-14], and colchicine, used to treat gout [15,16]. Both are being investigated in numerous clinical trials – as of February 2021, 79 ivermectin studies and 30 trials involving colchicine were listed on the WHO International Clinical Trials Registry [17]. Furthermore, recent randomised controlled trial (RCT) data from small studies have been promising for inhaled budesonide [18,19], baricitinib, a janus kinase (JAK) inhibitor given together with remdesivir [20] and the anti-androgen therapies dutasteride [21] and proxalutamide [22,23].
We therefore updated our original analysis to reflect these recent developments, based on the cost of active pharmaceutical ingredients (API). In this update we aimed to analyse the cost of production, current list prices in a range of countries, and API availability for oral and IV dexamethasone, ivermectin, colchicine, dutasteride, budesonide, baricitinib and the monoclonal antibodies tocilizumab and sarilumab.
Methods
Oral medications
Methodologies for estimating minimum costs of oral medication production were previously published [4]. Costs of Indian API exports were analysed (JW) and then reviewed by a second researcher (LE) using the online tracking database Panjiva [24], which showed API shipment details including quantities and costs per kilogram. All available data for each drug API found on Panjiva from 2016 were included. Shipments less than 1kg in volume, and the 15% highest and lowest priced shipments were removed to exclude outliers. A 5% API loss during tableting process, and a conversion cost of $0.01 per tablet was factored into our calculations, alongside a multiplier based on API mass to account for the expense of excipients (additional substances needed to convert API into the finished pharmaceutical product).
A profit margin of 10% and Indian taxation of 27% on profit was added. We assumed production in India given its leading role in global generic medicine manufacturing [25].
IV dexamethasone
For IV injectables, an adjusted and published methodology for injectable drugs was followed to account for the cost of ampules, additional transport costs, and a projected 20% API loss during formulation and filling [4,26].
Inhaled budesonide
Cost per kilogram of budesonide dry powder API was estimated using the same methodology above, before accounting for the cost of inhaler devices ($3), additional transport costs, and a projected 20% API loss during formulation and filling.
Tocilizumab, sarilumab, baricitinib
No data for the cost or volume of monoclonal antibodies production were available as this depend heavily on the efficiency and size of bioreactors used [27]. Also, no API data was available for baricitinib. Therefore, list prices in a range of countries, in particular developing economies, were tracked as a proxy.
International list price comparison
Estimated minimum costs of production were compared with published list prices for each drug in a range of countries across the economic development spectrum to give a representative sample of prices in countries with different levels of economic development.
Data sources by country are detailed in Appendix 1. Data was collected and checked by two independent researchers (JL and LE).
For consistency, a single data source per country was used for all searches of drug prices, based on the organisation of data and perceived reliability. Not all drugs analysed were available in every country, and in some countries without official databases, online pharmacy sites were used instead. Where several prices were available in the same database, the lowest price was selected.
API availability
Panjiva data was used to analyse API export volumes per drug from India and estimate the maximum number of treatment courses potentially producible over a 12-month period.
Key assumptions
Some drugs, such as dexamethasone and tocilizumab, which are dosed on a per kilogram basis we used an average adult body mass of 70kg.
The costs of regulatory filings and approvals are often significant add-ons to the initial use of drugs in any specific country. All drugs analysed in this study have been approved for treatment for some indications already. We have not included the cost or timing associated with regulatory approvals for the use of these drugs. We are assuming in our analysis that the WHO and other influential regulatory agencies will cooperate to define a pathway for use of these drugs which does not include additional financial outlays or filing for marketing approvals.
Results
The results are summarised in Table 1.
Summary of list prices, estimated production costs, and current availability of potential COVID-19 drugs selected for analysis. OD = Once daily, BD = twice per day, EUA = Emergency Use Authorisation (only to be given with remdesivir)
Dexamethasone
A widely used corticosteroid, dexamethasone has an economy of scale which supports low-cost production. Current national guidelines for dexamethasone treatment in COVID-18 most commonly recommend a 7-10-day courses of 6mg oral or IV [28,29]. Shorter courses are used if patients improve or are discharged early, and sometimes longer courses and higher doses are used in patients with fibrosis and hyper-inflammation confirmed by high-resolution CT in critical care.
This analysis used a 10-day, 6mg/day course. The weighted mean API cost between 2016-2020 was estimated to be $1116/kg; after factoring in the costs of excipients, formulation, tax, and profit, a 10-day course could be reasonably producible for around $2.58 IV and around $0.19 as oral tablets (Figs 1a, 1b). The higher cost of injectables reflect the potential for greater loss during production, cost of vials and increased cost of transport. Furthermore, significant non-drug costs associated with IV administration, including staff time, expendables required such as sterile water/syringes for reconstitution, and saline/IV lines for infusion were not included.


Comparatively, current list prices for oral dexamethasone were found to range from around $30.79 and $20.69 per course in UK and Israel respectively, to only $0.26 and $0.22 in China and Peru. For IV dexamethasone, cost per course ranged between $26.47 (UK) and $0.98 (Vietnam). (Figs 2a, 2b)









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Sufficient API export shipments were identified between March 2019 - March 2020 to form 7.4 million 10-day treatment courses. However, this could be a conservative estimate as a large volume of data points were excluded due to uncertainty as to whether they contained finished pharmaceutical products. This is a substantial decrease on the four-year average between 2016-2019 at a theoretical 34.5 million 10-day courses per annum.
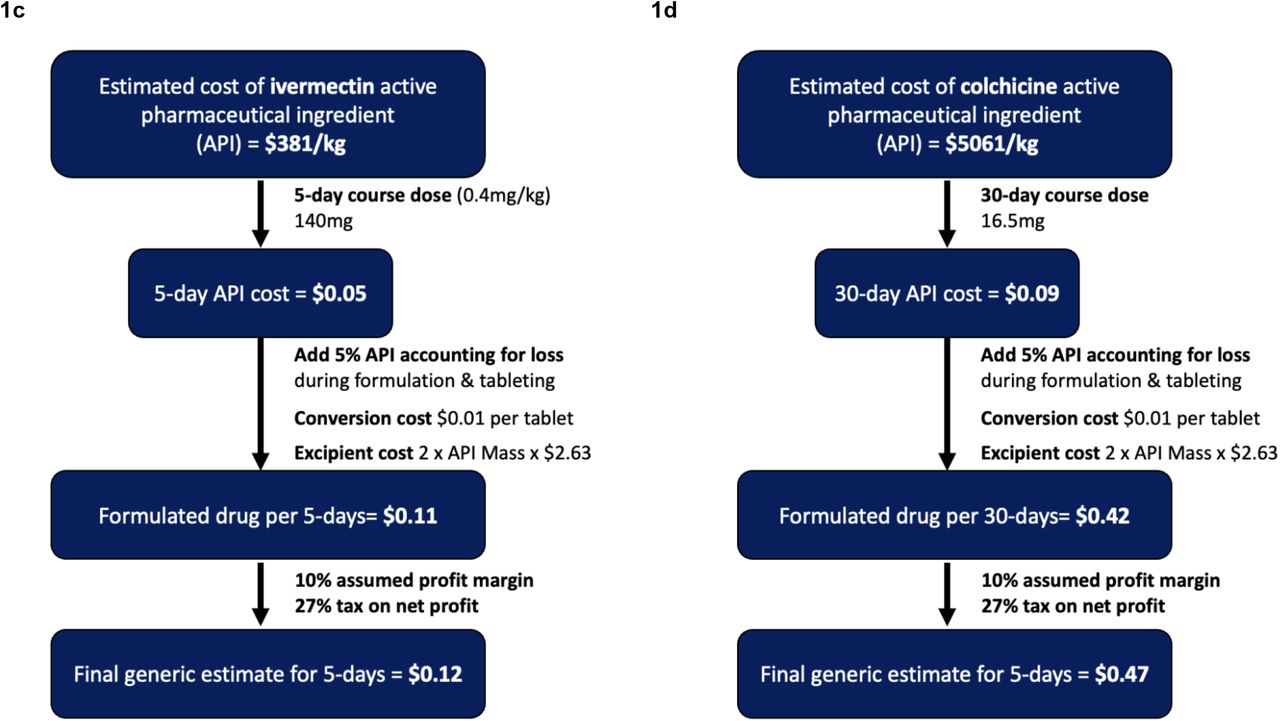
Ivermectin
Across clinical trials against COVID-19 a variety of doses and durations were used in protocols [11]. In this analysis, we assumed a 5-day course of 0.4mg/kg/day oral treatment in a 70kg adult, equivalent to a total API dose of 140mg at a weighted mean API cost of $381/kg. Therefore, it is estimated that a treatment course can be reasonably produced for $0.12 after accounting for costs of excipients, formulation, tax, and profit (Fig 1c). List prices per course of ivermectin treatment was found to range between $840.14 (Germany) and $519.61 (Norway) to only $3.47 (Bangladesh) and $1.66 in Bangladesh (India) (Fig 2c).
Indian ivermectin API shipments identified between 2017-2020 showed an increasing trend annually. API exported in 2020 was equivalent to 3.9 million courses, compared to approximated 1.2 million courses in 2019. Overall, volume remains low, reflecting how ivermectin is mainly used in regions with endemic parasite infections.
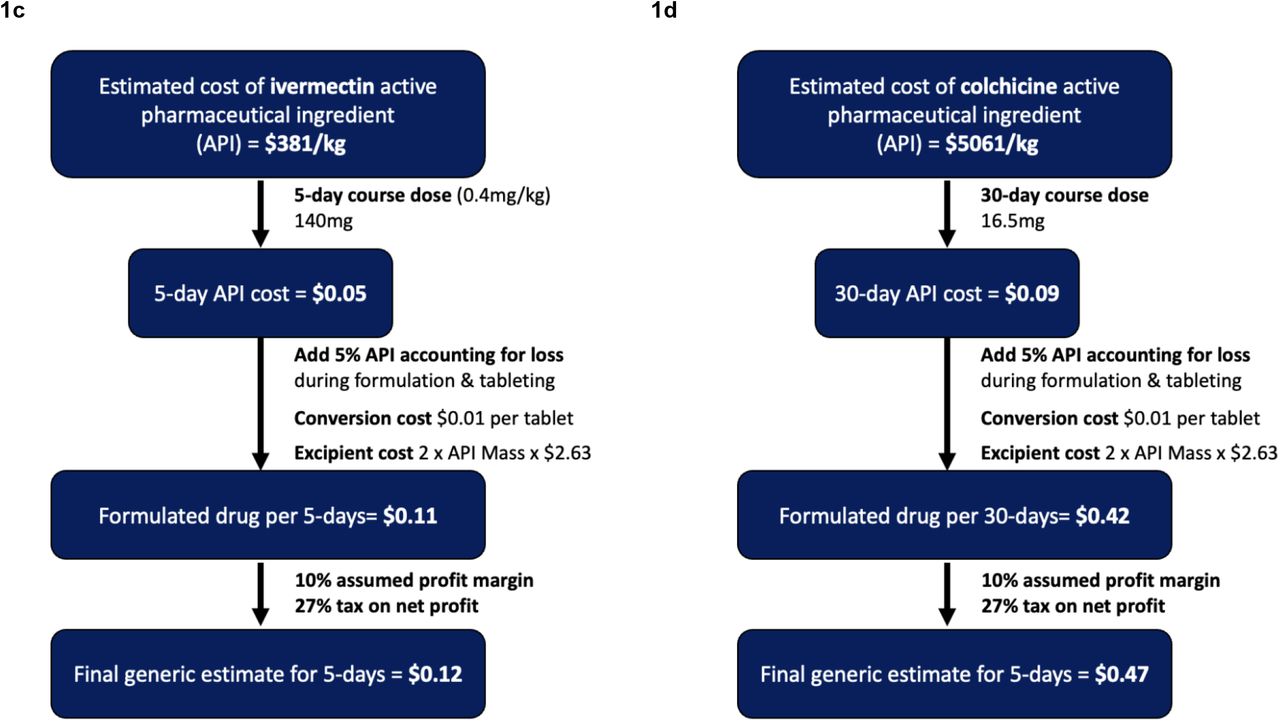
Colchicine
Again, various dosing regimens are being tested in clinical trials, including a loading dose of 0.5mg BD for three days followed by 0.5mg OD for 27-days [30], or just 0.6 mg BD or 1mg OD for 30 days [31]. Cumulative doses in a “treatment course” ranged from 16.5mg to 30mg (over 30 days), or 18.6mg over 14 days or more. For this analysis, a 30-day treatment course requiring a total API volume of 16.5mg was assumed.
The weighted mean API cost was estimated as $5061/kg. After factoring in costs of excipients, formulation, tax and profit, a treatment course could be potentially manufactured for $0.47 (Fig 1d). Comparatively, list prices ranged from $61.73 (USA) to 34.61 (Germany) per course, and $0.70 (Morocco) or $0.36 (Vietnam) (Fig 2d).
Indian 12-month API export between May 2019 - May 2020 was equivalent to a theoretical 60million 30-day courses, comparable to the four-year average between 2016-2019 which was equivalent to around 55.2 million courses per annum.
Tocilizumab and sarilumab
Dosages for both monoclonal antibodies are based on UK guidelines at time of writing [32]. Both are given as single dose IV infusions: sarilumab at 400mg, and tocilizumab at 8mg/kg (800mg maximum). In rare circumstances, a second tocilizumab dose can be given 12-24 hours later as a case-by-case basis, depending on response to first dose. This analysis is based a single infusion of sarilumab 400mg, and tocilizumab 600mg which are guideline dose-banding suggestions for bodyweights 66kg-80kg inclusive [32].
International list prices per single dose of sarilumab ranged between $4850.90 (USA) to $877.07 (Israel); whilst for tocilizumab, single dose costs ranged between $3,625.05 (Morocco) to $358.59 (Vietnam) (Figs 2e, 2f)
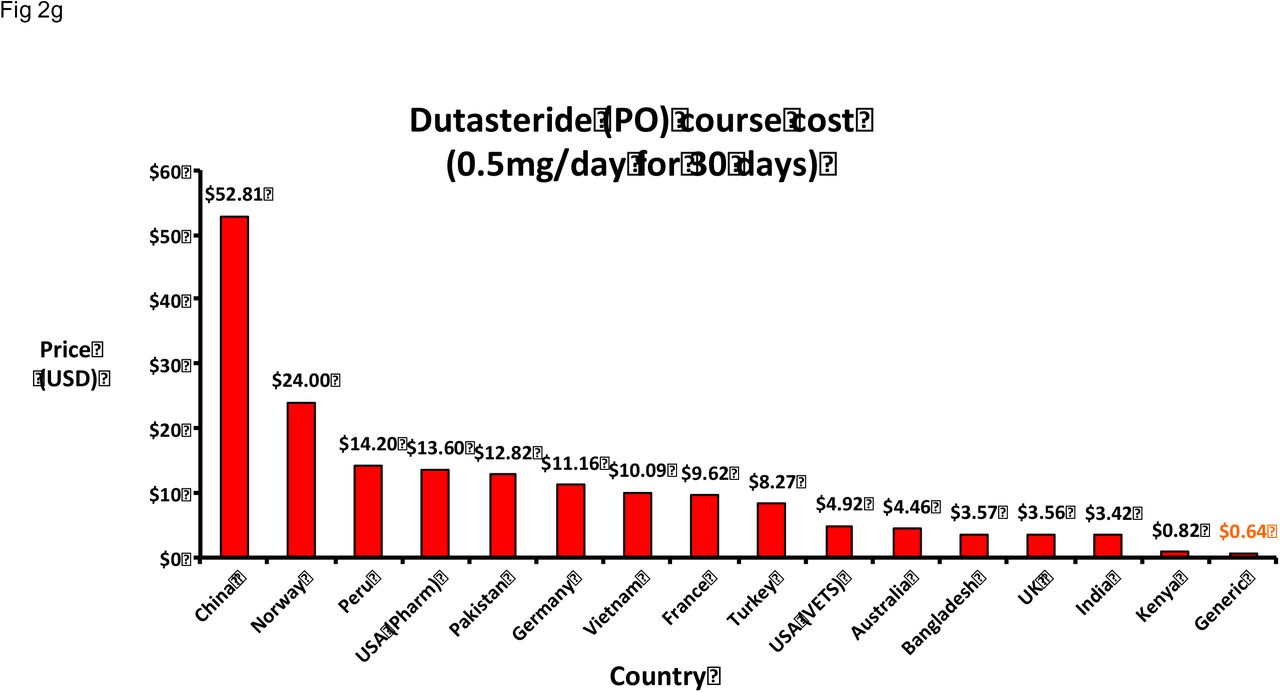
Dutasteride
A 30-day treatment course requiring a total API volume of 15mg was assumed for analysis, based on 0.5mg OD [21]. Weighted mean cost of dutasteride API was estimated to be $16,966. After factoring in the costs of excipients, formulation, tax and profit, a treatment course could be potentially manufactured for $0.64 (Fig 1d). In comparison, list prices per course was found to range from $52.81 (China) to $0.82 (Kenya) (Fig 2g).
India API exported between October 2019 - October 2020 was equivalent to a theorical 45.3 million 30-day courses. In comparison, the four-year average between 2016-2019 was much greater at approximately 119 million courses per annum.
Baricitinib
Baricitinib is an anti-rheumatic drug which in clinical trials for COVID-19 treatment [20] is dosed at 4mg/day for 14 days orally. No API data is currently available via Panjiva for a projected cost of production. International list prices for a 14-day treatment course were found to range between $2,326 (USA) to $6.67 (Bangladesh) (Fig 2h).
Budesonide
In the STOIC study, a protocol of 800mcg BD was used for up to 28 days, with the median duration being seven days [19]. In clinical practice, patients generally receive individual inhaler devices containing 60 to 200 doses of 400mcg/dose, 200mcg/dose, or 100mcg/dose, which is more than sufficient for the proposed treatment. Therefore, the production cost of one dry power budesonide inhaler containing 0.02g of API was estimated, based on a weighted-mean API cost of $4168/kg. After accounting for the cost of the inhaler device of about $3, potential API loss during production, transport costs, profit, and tax, we estimate the production cost to be $3.84 per 200mcg/dose inhaler and $4.68 per 400mcg/dose inhaler.
Discussion
Repurposed drugs with available API data could all be produced generically at very low cost, potentially for less than $0.10/patient, per day in oral formulations. Indeed, list prices found in developing economies such as India are already approaching our estimated costs. API costs were previously found to be a key determinant of generic medicine prices - in a 2015 study of sofosbuvir/daclatasvir, an antiviral combination for hepatitis-C, API costs accounted for 65-95% of final drug prices in competitive markets [33].
The analysis of list prices showed large variations between countries, especially for monoclonal antibodies. This highlights again the importance of international global health coordination to ensure accessibility instead of nationalistic stockpiling as observed with vaccines. Public-private partnerships such as the Global Fund demonstrate that it is possible to marshal resources and offer drug access at near cost-price through voluntary mechanisms. Strategies such as pooled procurement, differential pricing and voluntary licenses should be applied more widely as over time these have become more exclusionary and available only to a shrinking list of LMICs. Studies of differential or tiered pricing have shown that they can result in higher prices for MICs due to arbitrary market segmentation [34].
Other tools pertinent to expanding access to medicines in the current pandemic includes the use of the TRIPS flexibilities by national governments and civil society, in particular of compulsory licensing and patent oppositions. On multiple occasions this has proven to be effective in addressing high prices on medicines protected by intellectual property (IP) monopolies and triggering radical price reductions [35]. Also, given the pandemic situation, the so-called TRIPS waiver proposal at the WTO would be a crucial initiative for removing IP barriers to access generic and/or biosimilar medicines priced based on cost of manufacturing [36].
In terms of availability, dexamethasone, ivermectin and colchicine are already available as generic medicines with a large volume of API being produced already, although ivermectin API volumes, at approximately 3.9 million treatment course equivalent per annum is considerably less than volumes for dexamethasone and colchicine. Data from clinical trials of ivermectin and colchicine are emerging, and if these are promising results, they may become options earlier on in the disease process and production must be rapidly upscaled to meet demand. Regulators and decision makers should plan for this possibility and achieve accelerated deployment especially given that the safety profiles of these drugs are already established. An important aspect will be to protect supplies for existing patients treated for indicated conditions, for example parasitic infections and gout.
Limitations
This study presumed Indian generic production [25] with lower associated costs and no capital investment in new, dedicated facilities; however, following supply chain disruptions as seen earlier on in the pandemic, and currently with vaccines, countries may accept additional upfront costs and overheads for greater supply security in establishing domestic production. Fluctuating exchange rates and confidential in-country negotiated discounts for public healthcare providers means the prices we report are subject to change and are a snapshot of publicly available information at the time of writing [37].
Further, API production costs are subject to changes in supply and demand and optimisation of manufacturing processes. This study only examined data from Panjiva which relies on Indian custom records; production data in other countries were unavailable and thus the real volume of global API production may be higher. Conversely, API could also be used in other formulations, for example veterinary or topical use. Therefore, actual volumes of API available for oral or injectable formulations may be less than estimated. Finally, regulatory approval costs were not considered, assuming that regulatory agencies such as WHO and FDA would coordinate rapid, emergency deployment of drugs without significant burden [38-40].
Our estimates do not include research and development (R&D) costs. However, most of the R&D investment for drug repurposing in COVID-19 has originated from public sources, with significant amounts of research paid for directly by governments, universities, and public institutions such as the NIH, Gates Foundation and the WHO. It was recently estimated that governments have spent almost $100 billion in the last year solely on vaccine research for COVID-19 [41].
Neither steroids, nor IL-6 receptor antagonists are the silver bullet we desperately need against COVID-19 with mortality reductions of perhaps 11.1-29.2% [9] and 21.8-37.9% [10] respectively compared to control. Whilst conclusive efficacy of ivermectin and colchicine is yet to be confirmed, preliminary reports suggest further potential mortality reductions of up to 44% [16] for colchicine, and 75% for ivermectin [11]. Improvements in viral clearance rates, as reported with dutasteride, proxalutamide, ivermectin and molnupiravir could also help reduce the pandemic’s spread. [11,21,23,42].
Funders and regulators should take a greater co-productive role with researchers to ensure clinical trials are well designed and adequately powered. Outcomes and adverse event reporting should be standardised where possible so that results can be pooled more easily. A key barrier to regulatory approval has been evidence quality concerns – as shown by the latest WHO guidelines on ivermectin [14], despite the large volume of studies and participants. Ultimately, whether reduced mortality or faster rates of viral clearance, benefits seen in clinical studies will not be realised in the real world without guaranteed access for all people that need them, as “treatments don’t work if we can’t afford them” [43].
Overpriced treatments may harm already stretched and overwhelmed healthcare systems. The price of 5-day remdesivir treatment in the USA is approximately $2,335.50 despite offering no mortality reduction. Gilead’s patent monopoly on remdesivir enabled high prices based on the slight reduction in hospitalisation time, not related to its cost of production (<$9/course) nor quality adjusted life years – as it provides none. Additionally, Gilead has already earned over $50 billion in profit from its direct-acting-antiviral R&D program – from which remdesivir was developed [38]. This high price inflicted a large blow on many healthcare systems around the world desperate to secure treatment for patients, as Gilead largely negotiated prices for remdesivir before the clinical trial results were published.
Aspects for further research
There has been some recent promising data from small clinical trials for proxalutamide treatment in men with COVID-19, another anti-androgen [22,23], and for molnupiravir, a repurposed anti-viral therapy (EIDD-2801) originally tested against influenza. Molnupiravir appears effective in-vitro and in-vivo models against COVID-19 [44], and preliminary data from small clinical trials showed improved rates of viral clearance in humans [42]. No export and drug price data for both molnupiravir and proxalutamide were found. If either of these treatments are found to be successful in larger studies, it is imperative that the global health community does all it can to push for fair prices and equitable access. Molnupiravir is a small molecule direct-acting antiviral and synthesis is straightforward so we estimate that as an oral formulation, production costs would be less than remdesivir [45,46]. Proxalutamide is also a small molecule drug (non-steroidal androgen receptor antagonist) and is unlikely to be complex or expensive to manufacture.
Historically, dual, triple or quadruple combinations proved most effective against HIV/AIDS, hepatitis-C and TB - a similar approach might be needed for COVID-19 [47]. Combination such as antivirals given concurrently with immunomodulatory and anti-inflammatory drugs or at different disease stages may prove more effective than monotherapy and warrants further investigation.
This study demonstrates that cost-of-treatment should remain low for combination therapy. There is good accessibility and availability globally for steroids, ivermectin and colchicine. We were unable to calculate minimum cost of production of generic baricitinib, tocilizumab or sarilumab. The high prices of JAK inhibitors and monoclonal antibodies exposed from the national drug price databases are key barriers for many LMIC patients and for patients in healthcare systems requiring out-of-pocket co-payments. We note that entry of biosimilars can lead to significant price reductions even if not on the scale of chemical medications [48,49], and a reason for high biosimilar costs is the regulatory pathway that many critiqued as being overly cumbersome and should be overhauled [50]. If greater emphasis is placed on encouraging biosimilar entry, prices for tocilizumab and sarilumab could be much lower and allow for greater availability.
Conclusion
In conclusion, repurposed drugs for COVID-19 can be manufactured at very low costs should they be shown to be clinically effective. In the short term until vaccination access is more widely available, the repurposed drugs offer an affordable and widely available repurposed treatments for COVID-19 patients at all stages of the disease from pre-exposure prophylaxis to asymptotic and mild infections, through to critical care will still be urgently required.
Data Availability
Data used for this study is available upon request to the authors.
Funding
This work was supported by the International Treatment Preparedness Coalition, Make Medicines Affordable Campaign.
Conflicts of interest
None to declare.
Acknowledgements
The authors would like to thank members of the International COVID-19 Research Group, Kajal Bhardwaj and Sergey Kondratyuk for their support of this study and their contributions towards the development of this manuscript including insights, feedback, and proof-reading.
Appendix
Drug price sources
References



