
Abstract
Background Containment of the COVID-19 pandemic requires evidence-based strategies to reduce transmission. Because COVID-19 can spread via respired droplets, many states have mandated mask use in public settings. Randomized control trials have not clearly demonstrated mask efficacy against respiratory viruses, and observational studies conflict on whether mask use predicts lower infection rates. We hypothesized that statewide mask mandates and mask use are associated with lower COVID-19 case growth rates in the United States.
Methods We calculated total COVID-19 case growth and mask use for the continental United States with data from the Centers for Disease Control and Prevention and Institute for Health Metrics and Evaluation. We estimated post-mask mandate case growth in non-mandate states using median issuance dates of neighboring states with mandates.
Results Case growth was not significantly different between mandate and non-mandate states at low or high transmission rates, and surges were equivocal. Mask use predicted lower case growth at low, but not high transmission rates. Growth rates were comparable between states in the first and last mask use quintiles adjusted for normalized total cases early in the pandemic and unadjusted after peak Fall-Winter infections. Mask use did not predict Summer 2020 case growth for non-Northeast states or Fall-Winter 2020 growth for all continental states.
Conclusions Mask mandates and use are not associated with slower state-level COVID-19 spread during COVID-19 growth surges. Containment requires future research and implementation of existing efficacious strategies.
Introduction
Since being linked to SARS-CoV-2 in early 2020, COVID-19 has increased mortality and induced socioeconomic upheaval worldwide [1]. Typical COVID-19 symptoms mirror influenza, with loss of taste and smell being differential indicators [2]. Age, obesity, cardiovascular disease, and diabetes are associated with severe COVID-19 symptoms (e.g., pneumonia, blood clots, cytokine storm) and hence higher risks of hospitalization and death [3, 4]. Given the incidence of comorbidities, evidence-based containment strategies are warranted. Respired droplets and aerosols containing SARS-CoV-2 are intuitively likely modes of community transmission [5]. To reduce COVID-19 spread, governments have issued mandates to wear medical masks or cloth face coverings (henceforth masks) in public settings. 40 of the United States have issued mask mandates since April 2020. Mask mandates have limited precedent, making efficacy unclear. Therefore, our first objective was to evaluate the efficacy of mask mandates in attenuating COVID-19 case growth at the state level.
Prior studies have conflicted on whether masks reduce SARS-CoV-2 transmission. For USS Theodore Roosevelt crew, reported mask use was lower among COVID-19 cases (56% vs. 81%) [2]. There were no infections for 47.9% of patrons of two hair stylists with COVID-19 with universal masking [6], but PCR tests were not obtained for the other 52.1% of patrons [6], and first wave COVID-19 hospitalizations were no higher in public schools (high density with minimal masking) than elsewhere in Sweden [7]. A randomized controlled trial (RCT) of Danish volunteers found no protective benefit of medical masks against COVID-19 infection [8]. In RCTs before COVID-19, viral infections were more common for Vietnamese clinicians with cloth masks than medical or no masks (which were indistinguishable from each other) [9], and N-95 respirators (but not medical masks) protected Beijing clinicians from bacterial and viral diseases compared to no masks [10]. To be sure, mask use compliance in RCTs is not always clear [11]. Mask use was 10% and 33% for Beijing households with and without intrahousehold COVID-19 transmission, respectively [12]. This suggests greater mask use may reduce COVID-19 spread. Hence, our second objective was to assess whether COVID-19 case growth is negatively associated with mask use.
Earlier studies have not compared COVID-19 case growth rates in states with and without mandates, and effects of compliance (proportion of people masked) are not clear. We assessed if statewide mask mandates and compliance predict (and thus potentially decrease) statewide COVID-19 growth rates after 1 June 2020, when test capacity reached a threshold for minimal contact tracing [13]. We found little to no association between COVID-19 case growth and mask mandates or mask use at the state level. These findings suggest that statewide mandates and enhanced mask use did not detectably slow COVID-19 spread. We conclude by affirming the need for evidence-based strategies to minimize COVID-19 related morbidity and mortality and briefly discussing mechanisms of spread.
Materials and methods
Data Sources and Terms
We obtained total COVID-19 cases up to 6 March 2021 for the 50 United States from the Centers for Disease Control and Prevention (CDC) [14]. Total cases include confirmed and probable cases as defined by the Council of State and Territorial Epidemiologists. Briefly, confirmed cases require PCR amplification of SARS-CoV-2 RNA from a patient specimen. Probable cases require one of the following: clinical and epidemiologic evidence, clinical or epidemiologic evidence supported by COVID-19 antigen detection in respiratory specimens, or vital records listing COVID-19 as contributing to death. Statewide mask mandates were emergency executive public health orders that require nose and mouth coverings in public settings (including but not limited to retail locations) in more than 50% of counties within a state [15, 16]. Mandate issuance dates were obtained from state health departments and press releases. Early and late mandates were issued before and after 2 August 2020, respectively. Non-mandate states did not have statewide orders as of 6 March 2021.
Mask use is defined as the percentage of people who always wear masks in public settings. We assessed mask use with the University of Washington Institute for Health Metrics and Evaluation (IHME) COVID-19 model site [17], which estimates mask wearing from Premise, the Facebook Global Symptom Survey (University of Maryland), the Kaiser Family Foundation, and the YouGov Behavior Tracker Survey. To identify regional patterns of COVID-19 case growth, we grouped states into five categories: Northeast (Connecticut, Delaware, Massachusetts, Maryland, Maine, New Hampshire, New Jersey, New York, Pennsylvania, Rhode Island, and Vermont); Midwest (Illinois, Indiana, Iowa, Kentucky, Kansas, Michigan, Minnesota, Missouri, Ohio, West Virginia, Wisconsin); Mountains-Plains (Colorado, Idaho, Montana, Nebraska, New Mexico, North Dakota, Oklahoma, South Dakota, Utah, Wyoming); South (Alabama, Arkansas, Florida, Georgia, Louisiana, Mississippi, North Carolina, South Carolina, Tennessee, Texas, Virginia); and Pacific (Alaska, Arizona, California, Hawaii, Nevada, Oregon, Washington).
Parameter Derivation
We calculated COVID-19 case parameters from total cases per 100,000 state residents (normalized total cases; Worksheet A in S1 Table). As infectious diseases such as COVID-19 exhibit exponential growth, we used logarithmic transformation to quantify daily case growth as shown elsewhere [15, 18]:
 Where Cx is normalized cases on a particular day and Cx-1 is normalized cases on the prior day. To reduce effects of reporting lags, we used a 7-day simple moving mean.
Where Cx is normalized cases on a particular day and Cx-1 is normalized cases on the prior day. To reduce effects of reporting lags, we used a 7-day simple moving mean.
For each state, growth minima and maxima were the 20-day mean lowest and highest cases/day between the end of the Summer infection wave and the height of the Fall-Winter infection wave. Surge refers to the difference between maximal and minimal growth rates (the magnitude of growth rate increase) for each state. Surge rate refers to the speed at which case growth increased from minimal to maximal levels for each state (Surge/days between minima and maxima), normalized to the mean surge rate for all states.
Cases or masks at minima and maxima were the 20-day mean number of cases/100,000 state residents or mask use for each state at its growth extrema. Change in masks refers to the percent increase in mask use between extrema for each state.
To model post-mask mandate case growth in the 48 contiguous states (excluding Alaska and Hawaii), we calculated the difference of natural logarithms of normalized total cases between 6 March 2021 (C306) and the date of mandate issuance (CM) for each state with an early mandate:
 For states with late or no mandates, effective dates were modeled as medians of issuance dates among bordering states with early mandates. For example, the effective mandate issuance date of Tennessee was the median of issuance dates among the early mandate states Kentucky, Arkansas, Alabama, North Carolina, and Virginia.
For states with late or no mandates, effective dates were modeled as medians of issuance dates among bordering states with early mandates. For example, the effective mandate issuance date of Tennessee was the median of issuance dates among the early mandate states Kentucky, Arkansas, Alabama, North Carolina, and Virginia.
We reported mask use for Summer (1 June-1 Oct 2020) and Fall-Winter (1 Oct 2020-1 Mar 2021) as mean mask use during these periods for each state. Cases on 1 June or 1 Oct were the 20-day mean number of cases/100,000 on these two dates. Summer and Fall-Winter case growth were defined as differences of natural logarithms of normalized total cases at the beginning and end of each period:

Statistics
We used Prism 9.1 (GraphPad; San Diego, CA) to construct figures and perform null hypothesis significance tests (Worksheet D in S1 Table). The significance threshold for all tests was p < α=0.05. All datapoints are state-level values, and we performed D’Agostino-Pearson tests to assess normality of residuals.
To evaluate mask mandate efficacy, we performed two-tailed, two-sample t-tests (early vs. no mandates) or ordinary one-way ANOVA with Holm-Šídák posttests (early vs. late vs. no mandates) and used Welch’s correction for heteroscedastic data. For non-normal data, we performed Mann-Whitney U tests (early vs. no mandates) or Kruskal-Wallis with Dunn posttests (early vs. late vs. no mandates). This decision tree conforms with recommended practices for datasets with N > 5 [19]. Hawaii was excluded because its dates of extrema deviated from those of continental US states. Alaska and Hawaii were excluded from post-mandate case growth assessment because they lack contiguous US border states. To determine top and bottom mask use quintiles, we ranked mean mask use among states (excluding Hawaii) from 1 June 2020 to 1 March 2021. For t tests comparing top and bottom quintiles, we assessed days between the indicated normalized case totals and mean mask use over this interval for each state. To evaluate mask use efficacy at and between extrema, we performed simple linear regressions with null hypotheses of zero slope. We similarly evaluated mask use efficacy during the Summer and Fall-Winter infection waves. For the Summer wave, Northeast states were excluded because they deviated from other states with respect to covariation between normalized cases and growth. For the Fall-Winter wave, Hawaii was excluded because it deviated from other states with respect to covariation between normalized cases and growth. Infectious disease research commonly uses OLS [20, 21], with simple linear and simple ln-linear models reported in recent COVID-19 studies [22, 23]. We used ordinary least squares (OLS) for homoscedastic data and weighted least squares (WLS) for heteroscedastic data, as determined by the GraphPad Prism Test for Homoscedasticity. Regardless of statistical significance, R2 values denote coefficients of determination for lines of best fit with unconstrained slopes.
Results
COVID-19 growth rates vary with time
Normalized COVID-19 cases increased more than 1500-fold from March 2020 to March 2021 in the United States [14]. To identify patterns of COVID-19 spread, we quantified case growth for each of the 50 US States (Worksheet B in S1 Table). Natural log (Ln)-linear plots revealed six phases of COVID-19 growth up to 6 March 2021: first wave (before May 2020), first minimum (May-June 2020), Summer wave maximum (June-August 2020), second minimum (August-October 2020), Fall-Winter wave maximum (October-January 2020), and third minimum (March 2021) (S1-3 Figs).
Mandates are not associated with state COVID-19 case growth
We next assessed associations between mask mandates and case growth. 33 US states issued statewide mask mandates on or before 2 August 2020 (early), when case growth was low, while 7 other states issued mandates after this date (late). We observed a six-phase pattern in states with early (S1 Fig), late (S2 Fig), and no mask mandates (S3 Fig). This suggests qualitatively comparable courses of viral spread among states regardless of mask mandates.
A recent study reported negative association between statewide mask mandates and subsequent COVID-19 log growth rates [15]. We hypothesized that case growth would be lower in states with mandates. 64% of early state mandates were issued during the Summer wave, which precluded determination of whether mandates were associated with lower Summer wave case growth. We therefore examined case growth after mandate issuance during the second minimum and the Fall-Winter wave maximum (henceforth minimum and maximum) (Fig 1A). Hawaii was excluded because its minimum and maximum did not chronologically align with continental states. Average Fall-Winter mask use was ∼10% higher in early mandate states than in late and no mandate states (Holm-Šídák p≤0.001; Fig 1B), confirming that mandates promote greater mask use. Contrary to our hypothesis, early mandates were not associated with lower minimum case growth (Mann-Whitney p=0.087; Fig 1C). Maximum case growth was the same among states with early, late, and no mandates (ANOVA p=0.29; Fig 1D). This indicates that mask mandates were not predictive of slower COVID-19 spread when community transmission rates were low or high. We wondered if mask mandates were associated with smaller or slower surges in case growth. Differences between minimum and maximum case growth were similar among early, late, and no mandate states (ANOVA p=0.12; Fig 1E), and surges from minimum to maximum growth occurred at similar rates (ANOVA p=0.16; Fig 1F). These findings suggest that mask mandates are not predictive of smaller or slower shifts from low to high case growth.
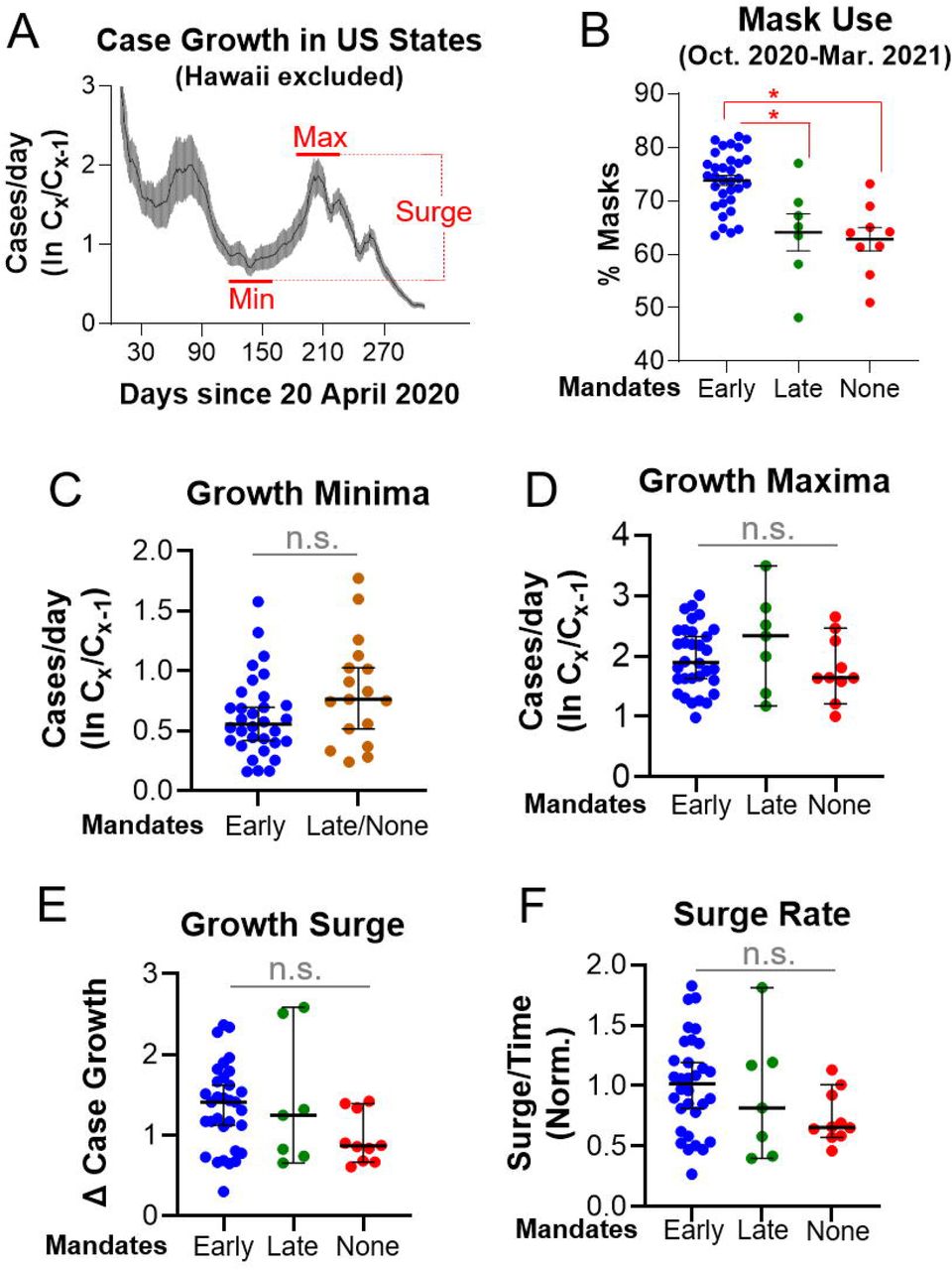
A. Daily COVID-19 case growth rate for continental US states from 20 April 2020 to 6 March 2021. Red horizontal lines denote growth rate minima (Min) and maxima (Max) after the Summer wave. Surge: difference in case growth between min. and max. Thin black line and wide gray bars denote mean and 95% confidence intervals, respectively. B. Early mandate states (blue) exhibited greater mask use than late (green) and no (red) mandate states during the Fall-Winter wave. C. Minimum growth rates were indistinguishable between early (blue) and combined late and no mandate (orange) states. D. Maximum growth rates were indistinguishable among early, late, and no mandate states. E-F. Surge sizes (E) and surge rates (F) were indistinguishable among early, late, and no mandate states. *: p<0.05 by Šídák post-test after one-way ANOVA. n.s.: not significant by Mann-Whitney U test (C) or one-way ANOVA (D-F). Error bars: 95% confidence intervals.
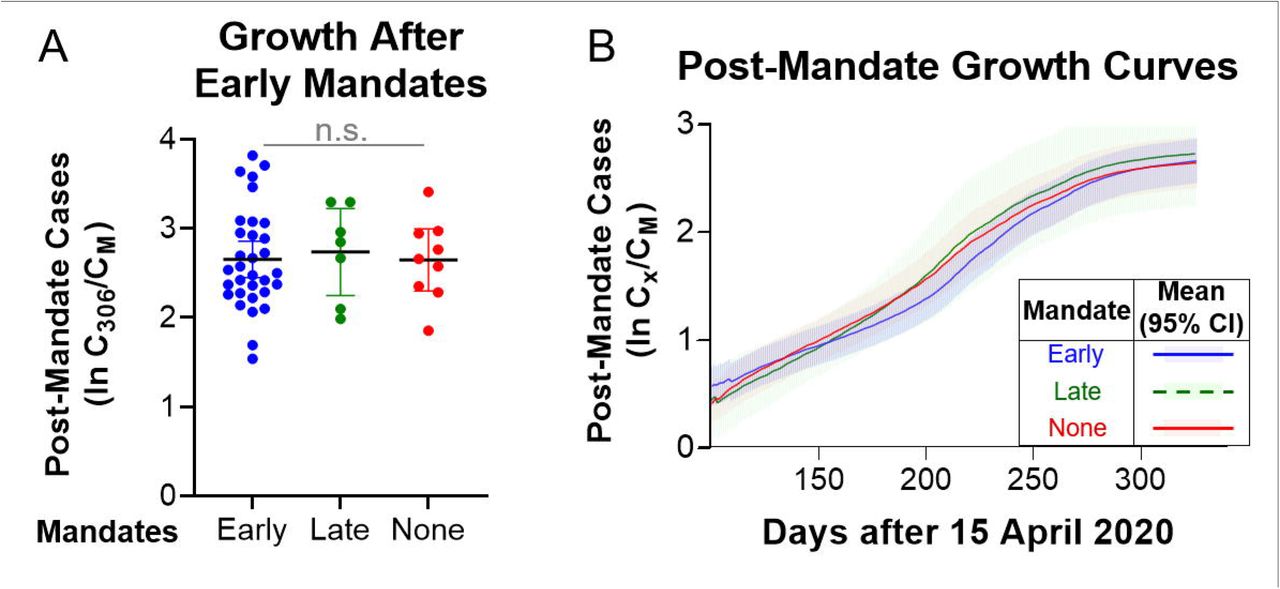
Normalized COVID-19 cases as of 6 March 2021 were 18.6% lower in states with early mandates than states without mandates (Holm-Šídák p=0.036), but early mandates were issued over a range of dates (15 April to 2 August 2020). To assess how early mandates relate to cumulative cases, we calculated normalized case growth for contiguous states between early mandate issuance and 6 March 2021. For states with late and no mandates, we expressed effective dates (when states could have reasonably issued mandates) as median dates of neighboring early mandate states. We expected to find lower case growth among early mandate states. Surprisingly, normalized case growth after mandates (actual and effective) were indistinguishable among state groups (ANOVA p=0.93; Fig 2A). Moreover, growth curves after actual and effective mandates were not distinguishable among state groups at any date between mandate issuance and 6 March 2021 (Fig 2B). Together, these data do not support an association between statewide mandates and COVID-19 spread.

A. Case growth was indistinguishable among states with early (blue), late (green), and no (red) mandates. n.s.: not significant by one-way ANOVA. Error bars: 95% confidence intervals. B. Growth curves were indistinguishable for states with early (blue), late (green), and no (red) mandates. Heavy lines and shaded regions denote means and 95% confidence intervals, respectively. Post-mandate case growth refers to cumulative cases between mandate issuance date and 6 March 2021 (A) or growth curves after mandate issuance up to 6 March 2021 (B). For states with late and no mandates, effective dates are medians of issuance dates among bordering states with early mandates.
Mask use is not associated with most state COVID-19 case growth
We speculated that statewide mask use, rather than mask mandates per se, may predict COVID-19 case growth. The University of Washington IHME provides robust estimates for mask use (defined as the percentage of people who always wear masks in public settings) [17]. Mask use was associated with lower minimum case growth (WLS p<0.0001; Fig 3A), but not normalized total cases at minima (OLS p=0.54; S4 Fig). States with the highest first wave normalized cases and July 2020 seroprevalence were primarily in the Northeast [14, 24], which could explain the lack of Summer growth in these states. Excluding Northeast states, normalized cases predicted lower minimum case growth (WLS p=0.001; S4 Fig). Eight Northeast states were among the 10 states with highest mean mask use [17]. Intriguingly, normalized cases grew from 400 to 1350 per 100,000 at similar rates between the first and last 10 states for mask use (unpaired t test p=0.49), albeit ∼50 days later for the last 10 states (Fig 3B). These findings suggest the link between masks and minimum growth may be an artifact of the tendency for faster case growth to occur at lower case prevalence. In support of this, we found no association between mask use and case growth at maxima (OLS p=0.11; Fig 3C), when case prevalence differences were smaller among states. There was also no association between mask use and normalized cases at maxima (OLS p=0.073; S5 Fig), although residuals were slightly non-normal. The 10 states with highest and lowest mask use exhibited indistinguishable growth rates from 0 to 80 days after maxima (Mann-Whitney p=0.85; Fig 3D), and higher normalized cases predicted lower maximum growth rates among continental states (OLS p<0.0001; S5 Fig). While there was unexpected weak association between mask use and surge size (OLS p=0.03; Fig 3E), mask use at minima did not predict surge rate (OLS p=0.69; Fig 3F). Together, these data suggest that mask use is a poor predicter of COVID-19 growth at the state level.

A. Mask use was associated with lower minimum growth rates. B. First and last mask use quintiles grew from 400 to 1350 cases per 100,000 at indistinguishable rates before minima. C. Mask use was not associated with maximum growth rates. D. Growth rates and normalized cases were indistinguishable after maxima between first and last mask use quintiles. E. Mask use was associated with larger surge sizes. F. Mask use was not associated with surge rates. A, C, E, F: Each SLR includes both Northeast (solid light blue; ●) and non-Northeast (black; ●) state data. Equations are given when p<0.05 for the null hypothesis of zero slope. R2 values refer to unconstrained lines of best fit.
Mask use does not predict Summer and Fall-Winter statewide COVID-19 case totals
Greater statewide mask use could predict fewer cumulative cases during a growth wave. We tested this by calculating COVID-19 case growth during Summer and Fall-Winter waves (Fig 4A-B). Summer wave growth differed notably between Northeast and all other states; excluding the Northeast, greater normalized cases on 1 Jun 2020 predicted lower Summer growth (OLS p<0.0001; Fig 4C). By contrast, normalized cases on 1 October 2020 predicted Fall-Winter growth for Northeast and all other states (WLS p<0.0001; Fig 4D). Excluding Northeast states, masks were not associated with lower Summer growth between 1 June and 1 October 2020 (OLS p=0.27; Fig 4E). We likewise found no association between mask use and Fall-Winter growth between 1 October 2020 and 1 March 2021 (OLS p=0.93; Fig 4F). These data indicate that mask use does not predict Summer wave or Fall-Winter wave growth at the state level and that low Summer growth in Northeast states did not predict low Fall-Winter growth. We conclude that statewide SARS-CoV-2 transmission waves are independent of reported mask use [17].
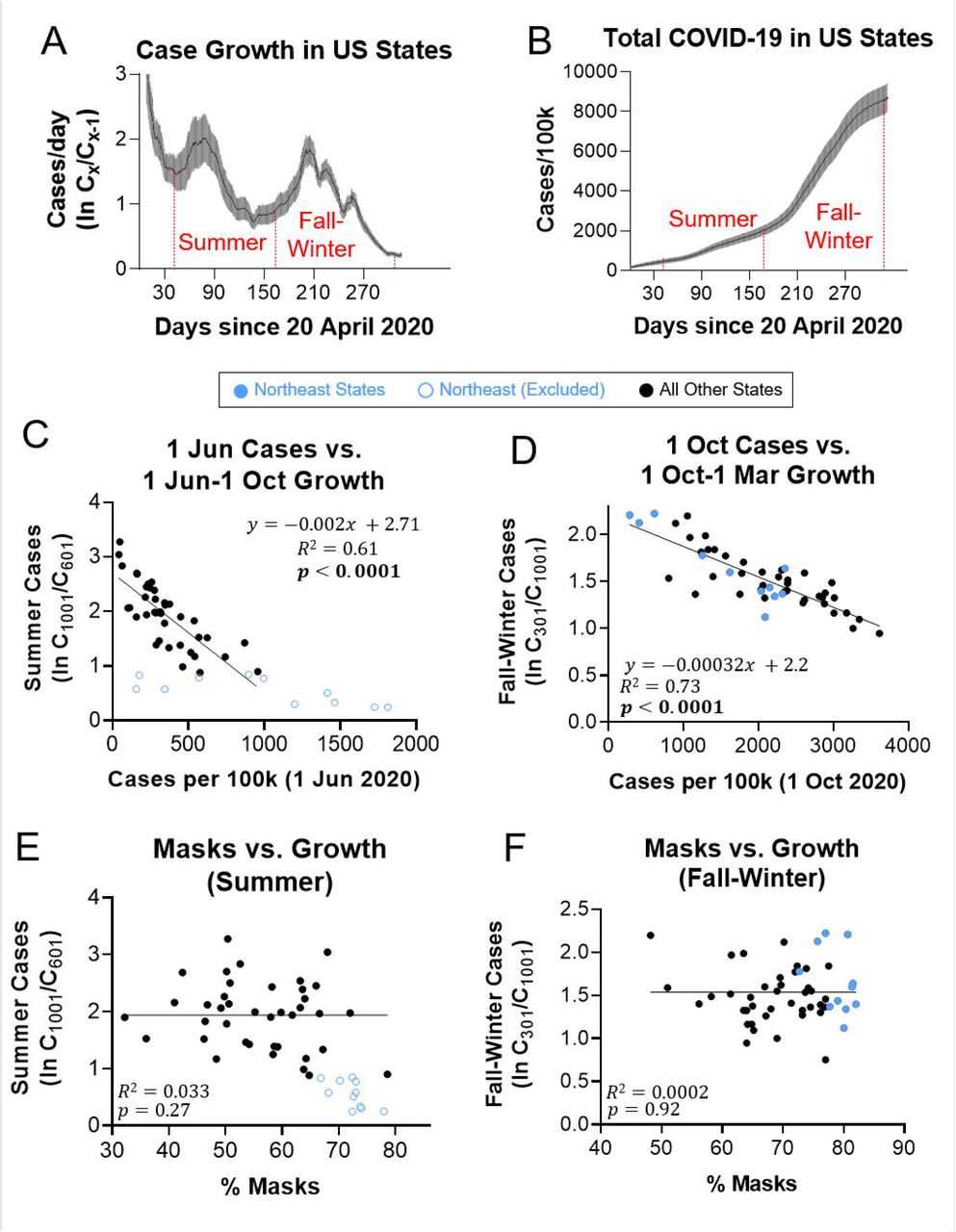
A-B. Daily COVID-19 case growth rate (A) and total COVID-19 cases (B) for US states from 20 April 2020 to 6 March 2021. Red vertical lines denote Summer (Jun-Oct 2020) and Fall-Winter (Oct 2020-Mar 2021) waves. Thin black line and wide gray bars denote mean and 95% confidence intervals, respectively. C. Higher normalized cases predicted lower Summer case growth in non-Northeast states (black; ●). D. Higher normalized cases predicted lower Fall-Winter case growth in Northeast (solid light blue; ●) and non-Northeast (●) continental states. E. Summer case growth was independent of mask use in non-Northeast states (●). F. Fall-Winter case growth was independent of mask use in Northeast (●) and non-Northeast (●) continental states. C, E: SLR models exclude Northeast states (○). D, F: SLR models include both Northeast and non-Northeast continental states. Equations are given when p<0.05 for the null hypothesis of zero slope. R2 values refer to unconstrained lines of best fit.
Discussion
Our main finding is that mask mandates and use are not associated with lower SARS-CoV-2 spread among US states. 80% of US states mandated masks during the COVID-19 pandemic. Mandates induced greater mask compliance but did not predict lower growth rates when community spread was low (minima) or high (maxima). We infer that mandates likely did not affect COVID-19 case growth [15], as growth rates were similar on all days between actual or modeled issuance dates and 6 March 2021. Higher mask use (rather than mandates per se) has been argued to decrease COVID-19 growth rates [11]. While compliance varies by location and time, IHME estimates are robust (derived from multiple sources [17]) and densely sampled (day-level precision). Higher mask use did not predict lower maximum growth rates, smaller surges, or less Fall-Winter growth among continental states. Mask-growth rate correlation was only evident at minima. This may be an artifact of faster growth at fewer normalized cases, as well as regional differences in case prevalence early in the pandemic. States in the high mask quintile grew at similar rates as states in the low mask quintile after maxima (when interstate total case differences were smaller than before minima). In addition, mask use did not predict normalized cases at minima, and low mask growth curves trailed those of high mask (particularly Northeast) states before minima. Growth maxima and Fall-Winter surges did not differ between Northeast and other states. Northeast states exhibited the highest seroprevalence up to at least July 2020 [24] and constituted 80% of the top quintile of mask use, which may explain their comparatively lower Summer growth. Overall, mask use appears to be an intra-state lagging indicator of case growth.
There is inferential but not demonstrable evidence that masks reduce SARS-CoV-2 transmission. Animal models [25], small case studies [6], and growth curves for mandate-only states [16] suggest that mask efficacy increases with mask use [11]. However, we did not observe lower growth rates over a range of compliance at maximum Fall-Winter growth (45-83% between South Dakota and Massachusetts during maxima) [17] when growth rates were high. This complements a Danish RCT from 3 April to 2 June 2020, when growth rates were low, which found no association between mask use and lower COVID-19 rates either for all participants in the masked arm (47% strong compliance) or for strongly compliant participants only [8]. Masks have generally not protected against other respiratory viruses. Higher self-reported mask use protected against SARS-CoV-1 in Beijing residents [26], but RCTs found no differences in PCR confirmed influenza among Hong Kong households assigned to hand hygiene with or without masks (mask use 31% and 49%, respectively) [27]. Medical and cloth masks did not reduce viral respiratory infections among clinicians in Vietnam [9] or China [10], and rhinovirus transmission increased among universally masked Hong Kong students and teachers in 2020 compared with prior years [28]. These findings are consistent with a 2020 CDC meta-analysis [29] and a 2020 Cochrane review update [30].
Our study has implications for respiratory virus mitigation. Public health measures should ethically promote behaviors that prevent communicable diseases. The sudden onset of COVID-19 compelled adoption of mask mandates before efficacy could be evaluated. Our findings do not support the hypothesis that SARS-CoV-2 transmission rates decrease with greater public mask use. As masks are required in public in many US states, it is prudent to weigh potential benefits with harms. Masks may promote social cohesion as rallying symbols during a pandemic [31], but risk compensation can also occur [32]. Prolonged mask use (>4 hours per day) promotes facial alkalinization and inadvertently encourages dehydration, which in turn can enhance barrier breakdown and bacterial infection risk [33]. British clinicians have reported masks to increase headaches and sweating and decrease cognitive precision [34]. Survey bias notwithstanding, these sequelae are associated with medical errors [35]. By obscuring nonverbal communication, masks interfere with social learning in children [36]. Likewise, masks can distort verbal speech and remove visual cues to the detriment of individuals with hearing loss; clear face-shields improve visual integration, but there is a corresponding loss of sound quality [37, 38]. Future research is necessary to better understand the risks of long-term daily mask use [30]. Conversely, it is appropriate to emphasize interventions with demonstrated or probable efficacy against COVID-19 such as vaccination [39] and Vitamin D repletion [40].
In summary, mask mandates and use were poor predictors of COVID-19 spread in US states. Case growth was independent of mandates at low and high rates of community spread, and mask use did not predict case growth during the Summer or Fall-Winter waves. Strengths of our study include using two mask metrics to evaluate association with COVID-19 growth rates; measuring normalized case growth in mandate and non-mandate states at comparable times to quantify the likely effect of mandates; and deconvolving the effect of mask use by examining case growth in states with variable mask use. Our study also has key limitations. We did not assess counties or localities, which may trend independently of state averages. While dense sampling promotes convergence, IHME masking estimates are subject to survey bias. We only assessed one biological quantity (confirmed and probable COVID-19 infections), but the ongoing pandemic warrants assessment of other factors such as hospitalizations and mortality. Future work is necessary to elucidate better predictors of COVID-19 spread. A recent study found that at typical respiratory fluence rates, medical masks decrease airway deposition of 10-20µm SARS-CoV-2 particles but not 1-5µm SARS-CoV-2 aerosols [41]. Aerosol expulsion increases with COVID-19 disease severity in non-human primates, as well as with age and BMI in humans without COVID-19 [42]. Aerosol treatment by enhanced ventilation and air purification could help reduce the size of COVID-19 outbreaks.
Supporting Information Legends
S1 Fig. COVID-19 case growth rates in US states with statewide mask mandates issued on or before August 2nd 2020. Top. COVID-19 growth phases. Y-axis values are differences between the natural logarithm of total cases on a day and the natural logarithm of total cases on the prior day. Thin black and wide gray denote mean and 95% confidence intervals, respectively. Bottom. Individual states. Red vertical lines denote dates of mask mandate issuance. Red horizontal lines indicate growth rate minima (phase 4) and maxima (phase 5) after Summer waves.
S2 Fig. COVID-19 case growth rates in US states with statewide mask mandates issued after August 2nd 2020. Top. COVID-19 growth phases. Y-axis values are differences between the natural logarithm of total cases on a day and the natural logarithm of total cases on the prior day. Thin black and wide gray denote mean and 95% confidence intervals, respectively. Bottom. Individual states. Red vertical lines denote dates of mask mandate issuance. Red horizontal lines indicate growth rate minima (phase 4) and maxima (phase 5) after Summer waves.
S3 Fig. COVID-19 case growth rates in US states without statewide mask mandates. Top. COVID-19 growth phases. Y-axis values are differences between the natural logarithm of total cases on a day and the natural logarithm of total cases on the prior day. Thin black and wide gray denote mean and 95% confidence intervals, respectively. Bottom. Individual states. Red horizontal lines indicate growth rate minima (phase 4) and maxima (phase 5) after Summer waves.
S4 Fig. Total cases, growth rates, and mask use at minima in continental US states. Left. Normalized cases do not predict mask use at minima. Right. More normalized cases predict lower growth rates in non-Northeast states at minima. Black circles (●): all states except Hawaii. Blue hollow circles (○): Excluded Northeast states. Red squares (■): Midwest states. Green triangles (▲): Mountain-Plains States. Grey triangles (▼): South states. Gold diamonds (♦): Pacific states except Hawaii. SLR models include all states except Hawaii (left) or all states except Hawaii and Northeast states (right). R2 values refer to unconstrained lines of best fit.
S5 Fig. Total cases, growth rates, and mask use at minima in continental US states. Left. Normalized cases do not predict mask use at maxima. Right. More normalized cases predict lower growth rates in all continental states at maxima. Black circles (●): all states but Hawaii. Light blue circles (●): Northeast states. Red squares (■): Midwest states. Green triangles (▲): Mountain-Plains States. Grey triangles (▼): South states. Gold diamonds (♦): Pacific states but Hawaii. SLR models include all states but Hawaii. R2 values refer to unconstrained lines of best fit. ε: Non-normal residuals (D’Agostino-Pearson p=0.008).
S1 Table. Total normalized cases, daily case growth, mask use, and statistical tests. Worksheet A. Total normalized cases (cases per 100,000 residents of each US state) from 6 March 2020 to 6 March 2021. Total cases obtained from the CDC were divided by 2019 projected state populations and multiplied by 100,000. Worksheet B. Daily case growth for each US state from 2 April 2020 to 1 March 2021. 7-day rolling averages are given. Red and gold text denote minima and maxima, respectively. Bold, highlighted text indicate actual mandate issuance dates for early and late mandate states (yellow highlight, bold red) and effective mandate issuance dates for late and no mandate states (blue highlight, bold orange). Worksheet C. Mask use for each US state on specified dates or ranges of dates. Date range mask use values are simple arithmetic means of daily mask use over the specified date range. Blue and red text indicate states in the first and last mask use quintile, respectively (i.e., states with highest and lowest mean mask use between 1 June 2020 and 1 March 2021). Mask use data are estimates provided by the University of Washington Institute for Health Metrics and Evaluation. Worksheet D. Statistical test summaries. Tests are reported in the order they appear in the Results. Red text specifies model assumption violations, followed by alternative tests that fulfill assumptions. All reported statistics and parameters were calculated with GraphPad Prism 9.1 (Prism files available upon request).
Acknowledgments
The authors thank Brandy Jesernik, Jay Bhattacharya, Scott Atlas, and Erik Fostvedt for manuscript input.
References




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Subject Area
Reviews and Context
185
Comment
0
TRIP Peer Reviews
0
Community Reviews
0
Automated Services
26
Blogs/Media
Author Videos