
Abstract
The rapid spread of SARS-CoV-2 globally continues to impact humanity on a global scale with rising morbidity and mortality. Despite the development of multiple effective vaccines, new vaccines continue to be required to supply ongoing demand. We report Day 42 interim safety and immunogenicity data from a Phase 2, randomized, placebo-controlled trial in Adults aged 18+ immunized with a virus-like particle vaccine candidate produced in plants displaying SARS-CoV-2 spike glycoprotein (CoVLP) adjuvanted with AS03 (NCT04636697). This report focuses on presenting safety, tolerability and immunogenicity, as measured by neutralizing antibody (NAb) and cell mediated immunity (IFN-γ and IL-4 ELISpot) responses, in Adults aged 18-64 (Adults) and Older Adults aged 65+ (Older Adults). CoVLP adjuvanted with AS03 was well-tolerated and adverse events (AE) were primarily mild or moderate and of transient duration. AEs in Older Adults were more limited than those observed in the Adult population. CoVLP with AS03 induced a significant humoral immune response in both age cohorts. CoVLP with AS03 induced a greater humoral response in Adults than Older Adults after a single dose but this effect was overcome with a second dose when both age cohorts responded with NAb titers that were ∼10-fold higher than those in a panel of sera from patients recovering from COVID-19. A single dose of CoVLP with AS03 induced a significant IFN-γ response in both age cohorts; a second dose significantly boosted IFN-γ and IL-4 responses in both age cohorts. Adults generated a stronger IFN-γ and IL-4 cellular response than did Older Adults after one or two doses of AS03-adjuvanted CoVLP. Safety and immunogenicity from Adults with comorbidities as well as final safety and immunogenicity responses after 12 months will be reported upon availability.
Introduction
Following a cluster of pneumonia cases in the city of Wuhan in Hubei province of China in December 2019 1, a novel coronavirus (Severe Acute Respiratory Syndrome Coronavirus 2 [SARSCoV-2]) was identified as the causative agent. The disease was subsequently named ‘coronavirus disease 2019’, or COVID-19 1,2. The rapid international spread of COVID-19 prompted the World Health Organization (WHO) to declare a pandemic in March 2020 3. As of May 6th, there has been more than 150 million cases of COVID-19 and >3.2 million deaths 4. This public health emergency sparked a remarkable global effort to develop vaccines using a wide range of traditional and novel platforms including messenger ribonucleic acid (mRNA), deoxyribonucleic acid (DNA), inactivated virus, live viral vectors, recombinant proteins, peptides, or virus-like particles (VLPs) 5,6. At the time of writing, >60 of these vaccines have entered clinical testing and at least 14 of them have been authorized for use in at least one country. Despite these successes, there remains an urgent global need to approve and distribute further safe and effective vaccines 7.
While it is now clear that humoral immunity is highly correlated with protection 8, both innate 9-12 and cellular immunity make significant contributions to lasting protection against SARS-CoV-2 infection. Passive antibody transfer has proven protective in both non-human primate animal models and in the therapeutic treatment of patients 13-15. Correlates of protection have recently been proposed for both binding and neutralizing antibody titers 8,16. Similarly, a clear role for cell-mediated immunity has been suggested for viral clearance and prevention of serious disease, as well as for long-term immunity 14,17-19. Optimally, SARS-CoV-2 specific vaccines should provide a well-coordinated response involving multiple elements of the immune system.
The vaccine candidate developed by Medicago, a Coronavirus-like particle (CoVLP), is a self-assembling VLP that displays trimers of recombinant S protein of SARSCoV2 embedded into the lipid bilayer of the nanoparticles. These VLPs are produced in a plant (Nicotiana benthamiana) and closely resemble the native structure of SARS-CoV-2 viruses 20,21. These plant-produced VLPs lack viral genetic material and can be stored at 2 – 8 °C. Medicago’s vaccine is administered with the oil-in-water Adjuvant System 03 (AS03) 22. The AS03 initiates a transient innate immune response at the injection site and draining lymph node in animal models 23,24 and in human peripheral blood 10,25,26. That innate immune response potentiates and shapes the adaptive immune response to the vaccine antigen including both antibody and T-cell responses, resulting in increased response magnitude, breadth, durability, and antibody avidity27-29. AS03 has been used in the licensed pandemic A/H1N1pdm09 influenza vaccines Arepanrix H1N1 (in Canada) and Pandemrix (in Europe), of which 90 million doses have been administered worldwide, as well as in other licensed (Q Pan H5N1 in the USA) or vaccine candidates 30. In Medicago’s Phase 1 study, AS03 significantly enhanced both cellular and humoral responses to CoVLPs and the vaccine had an acceptable safety profile 21.
Herein we report interim results of the Phase 2 portion of an on-going Phase 2/3 randomized, placebo-controlled study conducted at multiple sites in Canada and the USA. The Phase 2 portion of this study was designed to confirm the chosen formulation and dosing regimen (2 doses of 3.75 µg CoVLP adjuvanted with AS03 given 21 days apart: hereafter CoVLP+AS03) in adults ≥18 years of age. This report includes responses in healthy adults aged 18-64 (Population #1: “Adults”) and in older adults aged 65 years and older (Population #2: “Older Adults”). Analysis of the Phase 2 data for Population #3 (“Adults with Comorbidities”) is underway and will be released once available. Assessment of the efficacy of CoVLP+AS03 in all three adult Populations is currently on-going in the global, Phase 3 portion of the study.
Results
Demographic and baseline clinical characteristics
Subjects were screened for SARS-CoV-2 antibodies using a commercial ELISA that targets the nucleocapsid protein (although both seronegative and seropositive subjects were enrolled) and randomized 5:1 to receive CoVLP+AS03 or placebo (saline).
Participant demographics are presented in Table 1 and subject disposition is presented in Figure 1. The mean ages in Population 1(Adults), were 43.7 years and 42.4 years in vaccinated and placebo groups, respectively. The mean ages in Population 2 (Older Adults), were 71.1 years and 71.7 years in vaccinated and placebo groups, respectively. In all groups, subjects were mostly White or Caucasian (96.7% in Adults, 98.6% in Older Adults). Subject in the Adult and Older Adult populations self-identified as Hispanic or Latino (2.9% and 1.8%), Asian (2.0% and 1.1%) or Black or African American (1.0% or 0%) respectively. Eleven countries are planned for the Phase 3 portion of the Phase 2/3 study to include a more diverse population than that recruited in Phase 2.

Enrollment and follow-up of study participants vaccinated with CoVLP with AS03 or placebo after the first and second dose administration. For both Adults and Older Adults one subject was misdosed for the second dose administration and received a placebo in error. For more details of subject disposition, see Table 1.
306 Adults and 282 Older Adults were enrolled in the study. Of the 588 subjects who received a first dose of vaccine, 573 (97.4%) also received their second dose.
Safety
Safety and tolerability data after the first and second doses (as of April 2, 2021) are provided for 306 and 301 subjects in the Adult and for 282 and 272 in the Older Adult groups respectively. Overall, the vaccine was well-tolerated in both populations, with a slightly milder reactogenicity profile in the Older Adults.
Reactogenicity is illustrated in Figure 2 for solicited A) local and B) systemic AE. Frequency of solicited AE increased after the second dose relative to the first dose in both age cohorts although Older Adults generally had more muted responses than Adults: 94.5% and 88.4% of Adults reported at least one local AE after the first and second doses respectively compared to 61.7% and 54.2% of the Older Adults. In both study populations after the second dose, pain at the injection site was the most frequently reported local AE (89.3% of Adults and 72.8% of Older Adults) while fatigue (67.6% of Adults and 46.1% of Older Adults) and muscle aches (66.0% of Adults and 43.0% of Older Adults) were the most frequently reported systemic AEs.


Subjects were monitored for solicited local (panel A) and systemic (panel B) AEs from the time of vaccination through 7 days after administration of each dose. No Grade 4 (potentially life-threatening) events were reported. Participants who reported no adverse events (AEs) make up the remainder of the 100% calculation (not shown). If any of the solicited AEs persisted beyond Day 7 after each vaccination (when applicable), it was recorded as an unsolicited AE. Fever was defined as oral temperature ≥38.0°C.
In both populations, the majority of AEs were mild (Grade 1) or moderate (Grade 2) in severity (2.1% and 6.3% of Adults experienced grade 3 AEs after the first and second doses respectively while in Older Adults 0% and 8.7% of participants experienced grade 3 AEs after the first and second doses) and transient, typically resolving within 24 hours to 3 days. No Grade 4 AEs were reported in either study population. No clinically significant laboratory abnormalities, related serious AEs, or cases of Vaccine-Associated Enhanced Disease (VAED), anaphylaxis, or potential immune-mediated disorders monitored as Adverse Events of Special Interest (AESI) have been reported. No pregnancies have been reported to date.
Immunogenicity: Antibody Response
Pseudovirion neutralizing antibody (NAb) responses (based on a data cut-off of April 9th, 2021) are illustrated in Figure 3. Relative to both pre-vaccine sera (Baseline) and placebo controls, significant increases were observed in GMTs in both age cohorts at 21 days (D21) after the first dose with further significant increases 21 days after the second dose (D42).
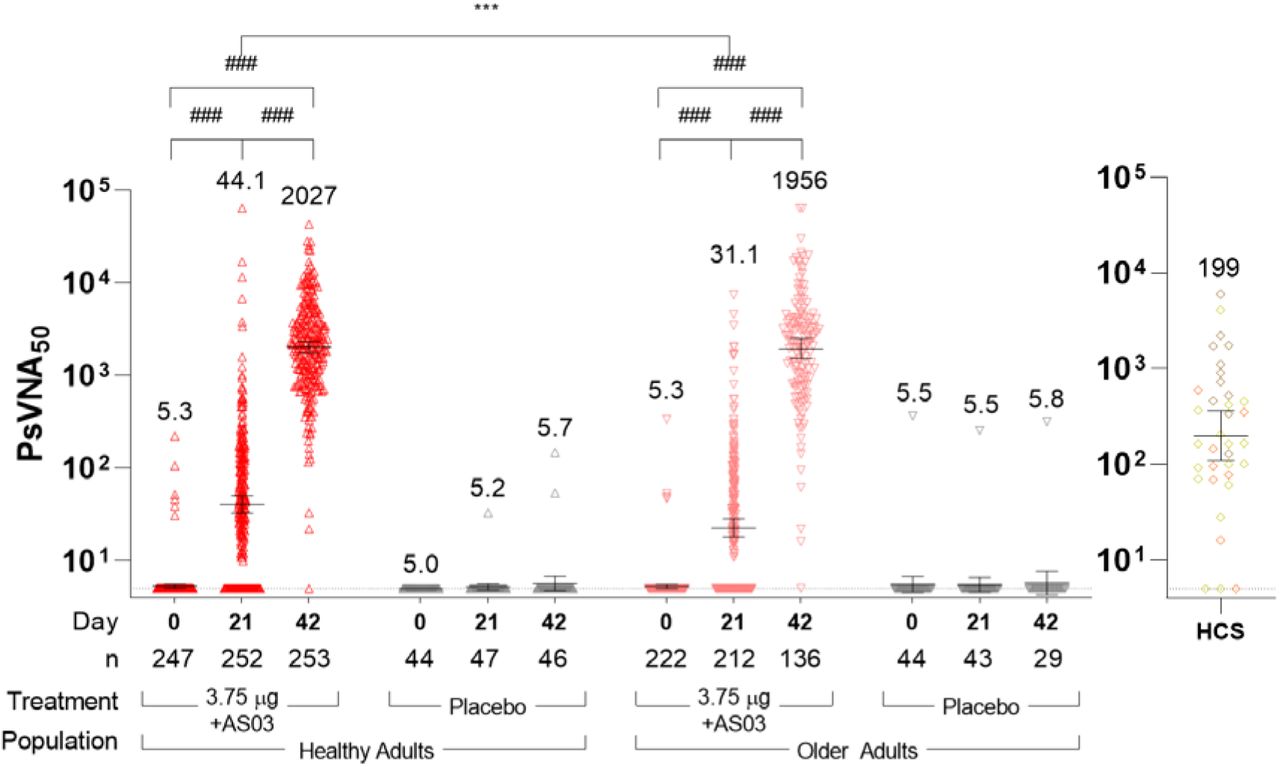
Virus neutralization titers at baseline (Day 0) and 21 days after the first (Day 21) or the second dose (Day 42) of CoVLP +AS03 or placebo. Bars and numerical values indicate geometric means and error bars indicate 95% CI. Significant differences between Days 0, 21 and 42 are indicated by # (###p<0.001; paired T-test of log-transformed values, GraphPad Prism, v9.0). Significant differences across study populations are indicated by *(*p<0.05; Adults vs Older Adults, one-way ANOVA on log-transformed data for GMT). The figure is based on a data cut-off of April 9th.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
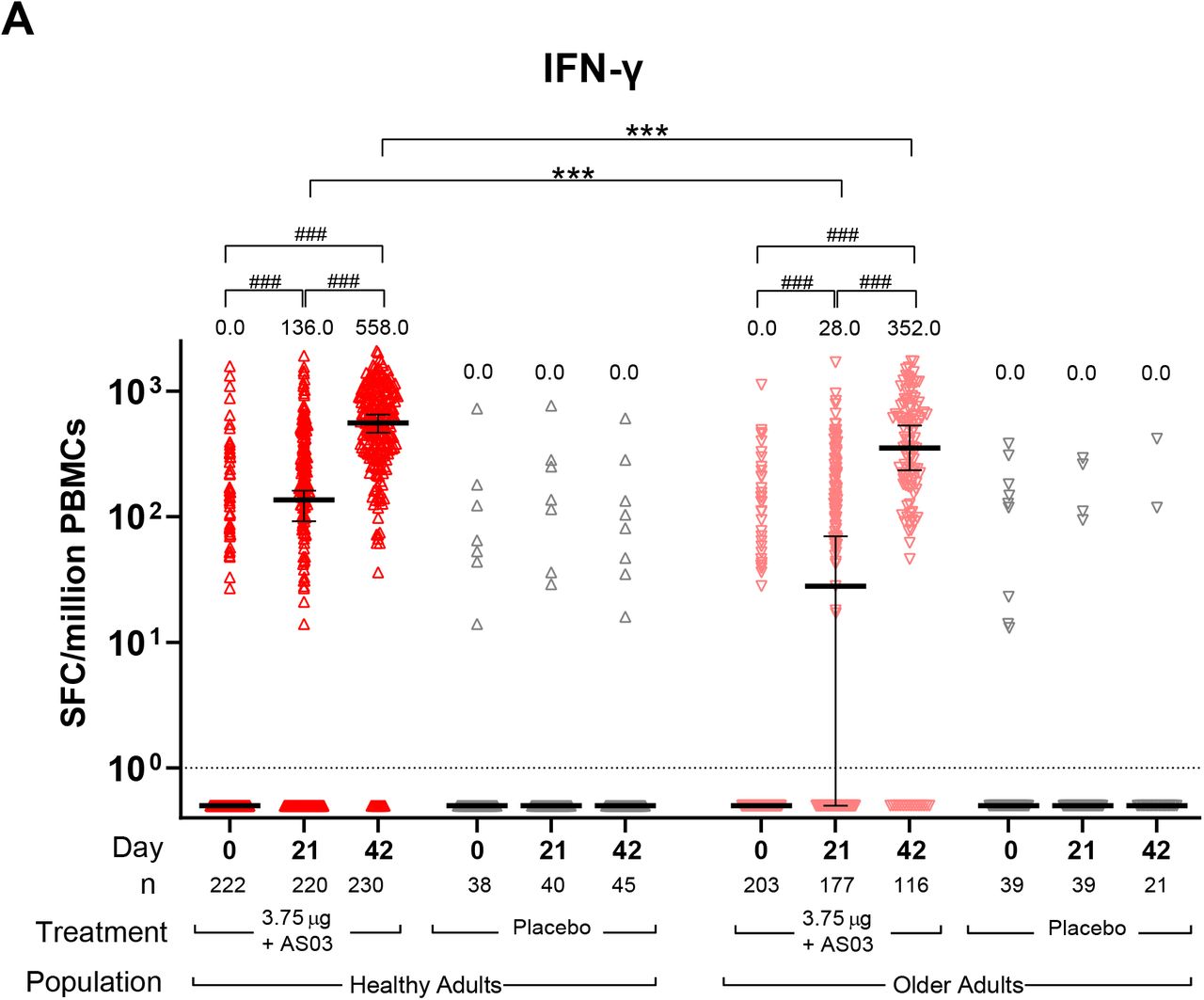
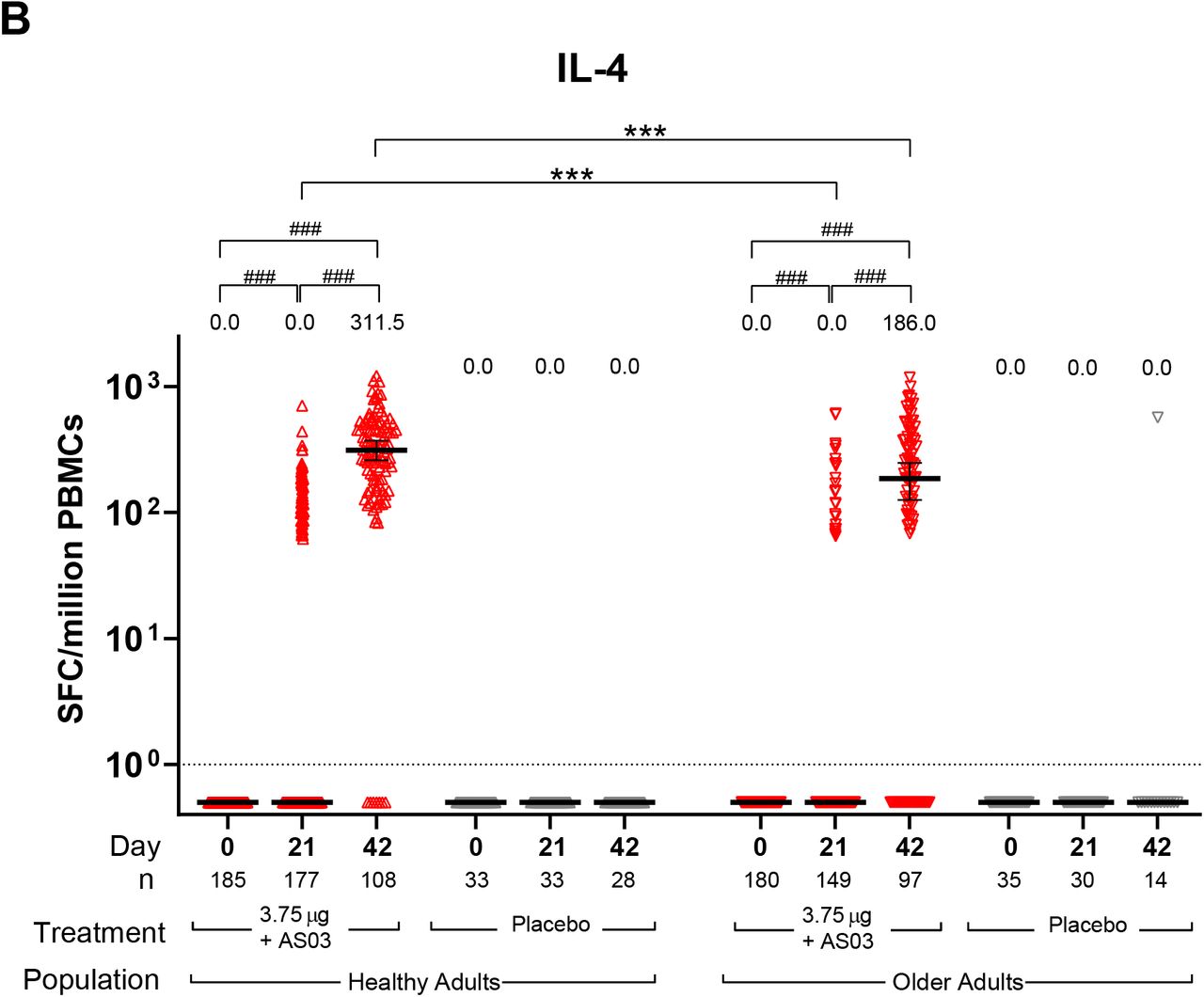
IFN-γ and IL-4 ELISpot Responses. IFN-γ (A) and IL-4 (B) spot forming cell (SFC) counts at baseline (Day 0), 21 days after the first immunization (Day 21) and 21 days after the second immunization (Day 42) with CoVLP (3.75 µg) adjuvanted with AS03 or placebo are represented. Bars indicate median (± 95% CI). Results of statistical analysis are represented for relevant comparisons. Significant differences between time-points for each vaccine regimen are indicated by # (###p<0.001; Wilcoxon signed rank test, SAS). Significant differences between study populations at each time-point are indicated by * (***p<0.001; Mann Whitney test, GraphPad Prism v9.0.1). Both IFN-γ and IL-4 responses in subjects injected with placebo were significantly lower (not represented, Wilcoxon rank sum test, SAS) than subjects who received the adjuvanted CoVLP at both Day 21 and Day 42 regardless of the population cohort. An arbitrary value of 0.5 SPC was assigned to samples with undetectable values to allow for representation on a logarithmic scale.
A single dose of CoVLP+AS03 induced a four-fold rise in NAb in a larger proportion of the Adults (51.3%, 95CI: 44.7-57.7) relative to Older Adults (39.6%, 95CI: 32.8-46.7, p=0.017), an effect also reflected in the D21 GMTs (44.1%, 95CI: 35.7-54.6 in Adults and 31.1%, 95CI: 24.7-39.1 in Older Adults, p<0.001). This difference between the two age cohorts disappeared with the second dose of CoVLP+AS03 and GMTs were not significantly different at D42 (2027, 95CI: 1749-2350 for Adults and 1956, 95CI: 1526-2509 in Older Adults, p=0.797). The seroconversion rates were also comparable between the two age cohorts at D42 (99.2%, 95CI: 97.0-99.9 in Adults and 97.7%, 95CI: 93.4-99.5 in Older Adults, p=0.348).
Consistent with observations from the Phase 1 study, the NAb titers elicited by CoVLP+AS03 at D42 were approximately 10-fold higher than those observed in a panel of convalescent sera (10.2x in Adults and 9.8x in Older Adults).
To assist in standardizing the NAb results, the WHO pooled plasma reference standard 20/136, was included in the pseudovirion NAb assay yielding a reference GMT value of 1872.
Expressing the GMT results in International Units (IU/mL), the Adults in our Phase 2 study had NAb values of 23.6 and 1083 IU/mL and the Older Adults had values of 16.6 and 1045 IU/mL after the 1st and 2nd doses respectively.
Prior to vaccination, 9 (1.5%) of the subjects the Phase 2 portion of the study were seropositive at Baseline (6 Adult and 3 Older Adults); all received CoVLP+AS03. At D21, their NAb GMTs were significantly increased in all groups (5756 at D21 relative to 63.9 at D0 in Adults and 4909 at D21 relative to 49.6 at D0 in Older Adults). A second dose was only moderately effective in further increasing NAb titers in Older Adults (5786 at D42 in Adults and 10400 at D42 in Older Adults). These data illustrate the potential for CoVLP+AS03 to boost the NAb response even in those presumed to have had prior infection.
Overall, CoVLP + AS03 induced comparable NAb responses in both age cohorts. Although small differences between the groups were observed at D21 after the first dose, these differences were overcome by the second dose.
Immunogenicity: Cell Mediated Response
Th1- and Th2–type cellular responses were assessed by IFN-γ and IL-4 ELISpots in peripheral blood mononuclear cells (PBMC) restimulated with a spike protein peptide pool (Figure 3). These interim data reflect a data cut-off of April 16th, 2021.
As observed in the Phase 1 study of CoVLP+AS03 21 and previously reported in several studies31,32, a significant minority (∼20%) of individuals were observed to have pre-existing (D0) IFN-responses to the spike protein. There was no relationship between NAb seropositivity and IFN-responses at baseline. In both age cohorts, vaccination with CoVLP+AS03 induced a significant increase in IFN-response at D21 which was further significantly increased after a second dose at D42 (Figure 3A). Adults had a significantly greater IFN-γ response relative to Older Adults at both D21 (p <0.0001) and D42 (p <0.0001). Sixty-nine percent of the Adults and 51% of Older Adults displayed a detectable IFN-γ response after one dose (D21). The frequencies of responders eliciting a detectable response increased to 96% and 86% after the second dose in Adults and Older Adults respectively.
Also consistent with the results from the Phase 1 study, no subject in either group had a measurable IL-4 response pre-vaccination (D0). While a limited portion of subjects responded to CoVLP+AS03 with a detectable IL-4 response after one dose (35% in Adults and 17% in Older Adults), the proportion of ‘responders’ increased to 94% and 75% after the second dose of CoVLP+AS03 in Adults and Older Adults respectively. Although the second dose of CoVLP+AS03 significantly increased the response in both populations, the Adults had median counts significantly higher than Older Adults (p=0.0002).
Discussion
The Phase 2 portion of the ongoing Phase 2/3 study of CoVLP+AS03 was designed to confirm the selection of CoVLP dose and adjuvant identified in the Phase 1 trial and to assess the performance of the chosen formulation in both adults aged 65 or less in good health, adults 65 years and more, and adults with comorbid conditions that put them at increased risk from COVID-19. This interim report focuses on healthy individuals ≥18 years of age. The data for individuals with comorbidities are being compiled and will be released in a separate manuscript. The primary outcomes for the Phase 2 portion of this study focused on short-term (up to D42) safety and tolerability of CoVLP+AS03 and the ability of this novel candidate to induce both NAb and cellular responses to SARS-COV-2 spike protein.
Reactogenicity in Adults in the Phase 2 study confirmed the profile observed in the much smaller Phase 1 study in 18–55-year-old adults that received CoVLP(3.75μg) with AS03 (n=20). Local reactogenicity was characterized by injection site pain in most subjects while systemically, reactogenicity was characterized by muscle aches, fatigue, and/or headache in approximately 60% of the study participants. There was a trend towards increased local and systemic reactogenicity after the second dose, although almost all reported AEs were mild-to-moderate and transient in nature. Although only the 3.75 µg dose level of CoVLP was used in the Phase 2 study, data from the Phase 1 trial that included groups given unadjuvanted CoVLP at three dose levels (3.75, 7.5 and 15μg/dose) showed that local and systemic reactogenicity was higher in adjuvanted groups as compared to non-adjuvanted groups, as would be expected from its use with other antigens 25,33,34. As expected 26 and has been observed for mRNA, adenovirus vector, inactivated virus, and recombinant protein-based COVID-19 vaccines 35-42 reduced reactogenicity was observed in the older adults. The safety profile in the Older Adults was consistent with the safety profile in the Adult population no new safety concerns were reported relative to our phase 1 study, suggesting that CoVLP+AS03 is well-tolerated in healthy individuals 18 years of age and older.
Both the humoral and cellular immune responses seen in the Phase 2 study confirmed the robust immunogenicity results documented in the 18-55 year old healthy adults during the Phase 1 study 21 as well as extending these observations to older adults. After two doses of CoVLP+AS03, seroconversion occurred in >99% of the subjects and NAb titers were ∼10x higher than those observed in convalescent sera. Although the NAb response after the first dose of CoVLP+AS03 was slightly weaker in the Older Adult population than in the Adults, the differences in seroconversion rate and GMTs between the two age cohorts disappeared after the second dose. This observation is consistent with the generally reduced capacity of older individuals to respond to vaccination and with findings for other SARS-CoV-2 vaccines 42-44. The decreased ability of even healthy older individuals to mount strong immune responses after vaccination is likely multi-factorial including a general decline in immune function (ie: immunosenescence) and chronic low-level inflammation (so-called ‘inflammaging) 45. Consistent with the observations that adjuvants can enhance vaccine-induced responses in older individuals 46, these results suggest that two-doses of CoVLP+AS03 can overcome these age-associated limitations for NAb production at least.
The number of Adult or Older Adult subjects in the current study with pre-existing NAb titers to SARS-CoV-2 was very low (n=9, 1.5%) but vaccination with CoVLP+AS03 nonetheless appeared to induce a substantial increase in NAb titers, suggesting that this vaccine candidate can significantly boost a pre-existing memory response 47,48. This is consistent with observations made by Goel et al.49 following mRNA vaccination. The increase in NAb titers was greater after the first dose of CoVLP+AS03 (GMT 58.7 → 5458) than the second dose (GMT of 5458 → 7035) suggesting there may be limited additional benefit in providing a second dose to such individuals. These observations provide strong support for vaccinating both infection naïve and previously infected individuals with CoVLP+AS03.
Overall, the NAb titers induced by CoVLP+AS03 in both the Adult and Older Adult populations compared well to a panel of convalescent serum/plasma. While this method can be used to draw broad comparisons between studies 8,16, there is a growing consensus that this approach has serious limitations for comparing responses between groups and between trials with different vaccines. For this reason, we included the WHO reference standard 20/136, pooled antibodies from recovered COVID-19 patients with very high NAb response in multiple laboratory studies 50 in our serological analysis so that the performance of CoVLP+AS03 can be assessed relative to other vaccines.
Although attention on vaccine-induced immune responses for SARS-COV-2 has focused primarily on antibody production, there is compelling evidence that cellular responses contribute to both recovery from infection and long-term immunity 14,32. Despite this growing consensus, what constitutes a ‘good’ or ‘desirable’ response is not yet fully understood 51. In the current study, the mixed Th1 (IFN-γ) and Th2 (IL-4) cellular response to CoVLP+AS03 was, like the NAb response, entirely consistent with the Phase 1 results. In both age cohorts, an IFN-γ dominated response was observed after the first dose that shifted to include a substantial IL-4 response after the second dose. Even though the IL-4 response increased significantly after the second dose, SFU counts for IFN-γ remained approximately 2-fold higher than those for IL-4. Of course, the limited nature of using only these two ELISpots to assess the pattern of cellular immunity generated by CoVLP+AS03 should be acknowledged.
While Th2–type responses and possible VAED were initially a point of concern in COVID-19 vaccine development 52,53, there has since been no evidence of disease enhancement in either animal models or across all of the human trials reported to date, nor any evidence that Th2 responses are associated with VAED 51. Indeed, it even possible that the Th2-response induced by CoVLP+AS03 as characterized by IL-4 production, may contribute significantly to the high titers of neutralizing antibody observed in vaccinated subjects through its role in T helper follicular cell involvement, optimal germinal center formation, and B-cell maturation 18,54,55. Such Th2-driven effects may also contribute to longevity of SARS-CoV-2 specific memory B-cell responses and longer-term immune response 56.
Unlike the NAb response, both IFN-γ and IL-4 responses in the Older Adults were significantly weaker than those observed in the Adult population even after the second dose suggesting that at least some aspects of the aged immune system cannot be overcome with multiple doses of an AS03-adjuvanted vaccine. Given the clear age-related differences in both the clinical manifestations of COVID-19 and the immune response generated by SARS-COV-2 infection 57, it is not surprising that vaccine-induced responses might also differ between younger and older individuals 58. Indeed, similar age-related differences in immune responses have been reported for several of the SARS-COV-2 vaccines in development or in use 38,59 and age-related differences in vaccine efficacy with some of the deployed vaccines are emerging 60-62. Given the very high NAb titers induced by CoVLP+AS03 across all ages, it is unclear whether or not the in vitro differences in cellular responses between younger and older adults will result in clinically relevant differences in protection. Any such differences might only become apparent as the Phase 3 portion of the study progresses and/or with greater time should CoVLP+AS03 be licensed.
This study as presented has several obvious limitations. First, the cut-off for data in this interim report was D42 so longer-term safety and immunogenicity results are not yet available. Also, the report does not include Adults with Comorbidities from the Phase 2 study as these data are still being analyzed. Some immunogenicity data, particular for D42 cell-mediated immune responses, have not yet been fully analyzed. Whether or not the NAb induced by CoVLP+AS03 have activity against variants of concern is of obvious interest and these studies are underway. Finally, the limited demographic diversity of the Phase 2 study participants is acknowledged and is primarily a reflection of the demographics of the study sites where the majority of these participants were recruited. The ongoing global Phase 3 efficacy portion of the trial is being conducted on three continents and is expected to provide efficacy results in a highly diverse population.
In conclusion, this interim report of our on-going Phase 2/3 study of CoVLP+AS03 confirms that this formulation is well-tolerated and highly immunogenic in healthy adults ≥ 18 years of age. Compared to either a panel of convalescent serum/plasma or the WHO standard serum reagent (20/136), the NAb response induced by CoVLP+AS03 was among the highest reported for any SARS-COV-2 vaccine. Across the broad age range of study participants (18 – 88 years of age), >99% mounted either a strong NAb response, a balanced Th1/Th2-pattern cellular response, or both following two doses of CoVLP+AS03.
Data Availability
Medicago Inc. is committed to providing access to anonymized data collected during the trial that underlie the results reported in this article, at the end of the clinical trial, which is currently scheduled to be 1 year after the last participant is enrolled, unless granted an extension. Medicago Inc. will collaborate with its partners (GlaxoSmithKline, Rixensart, Belgium) on such requests before disclosure. Proposals should be directed to wardb{at}medicago.com or landryn{at}medicago.com. To gain access, data requestors will need to sign a data access agreement and access will be granted for non-commercial research purposes only.
Author Contributions
All authors contributed significantly to the submitted work. BJ Ward, N Landry, A Seguin contributed to all aspects of the clinical study from conception to completion. P Gobeil, A. Mahmood, S Pillet, I Boulay, N Charland contributed to design and execution of the study as well as analysis and presentation of the data. F. Roman, R. Van Der Most, M de los Angeles Ceregido Perez contributed to analysis and presentation of data. MP Cheng provided access to critical reagents and consulted on study design and execution. All authors contributed to critical review of the data and the writing of the manuscript. All Medicago authors had full access to the data. BJW and NL made the final decision to submit the manuscript.
Funding Statement
The study was sponsored by Medicago Inc.
Data Availability
Medicago Inc. is committed to providing access to anonymized data collected during the trial that underlie the results reported in this article, at the end of the clinical trial, which is currently scheduled to be 1 year after the last participant is enrolled, unless granted an extension. Medicago Inc. will collaborate with its partners (GlaxoSmithKline, Rixensart, Belgium) on such requests before disclosure. Proposals should be directed to wardb{at}medicago.com or landryn{at}medicago.com. To gain access, data requestors will need to sign a data access agreement and access will be granted for non-commercial research purposes only. The following publicly-available databases were accessed to complete this work: GISAID database (https://www.gisaid.org/) and Genbank (https://www.ncbi.nlm.nih.gov/genbank/).
Conflict of Interest
P. Gobeil, S. Pillet, A. Séguin, I. Boulay, A. Mahmood, N. Charland, B. Ward, and N. Landry are either employees of Medicago Inc or receive salary support from Medicago Inc. P. Boutet, F. Roman, R. Van Der Most, and M. de los Angeles Ceregido Perez are employees of GlaxoSmithKline.
Methods
CoVLP Vaccine Candidate and Adjuvant
The CoVLP vaccine candidate has previously been described in detail 21. Briefly, full-length spike protein from SARS-CoV-2 (strain hCoV-19/USA/CA2/2020) incorporating the modifications R667G, R668S, R670S, K971P, and V972P is expressed in Nicotiana benthamiana by transient transfection, resulting in spontaneous trimer formation and VLP assembly and budding. The VLPs are purified and shipped to the vaccination site where it is mixed with AS03 adjuvant prior to injection.
AS03 adjuvant, an oil-in-water emulsion containing DL-α-tocopherol (11.69 mg/dose) and squalene (10.86 mg/dose), was supplied by GlaxoSmithKline.
Vaccine Preparation and Injection
CoVLP was available in single-dose vials (0.30 mL) at 15 µg/ml and stored at 2-8°C until shortly before use. The AS03 adjuvant was supplied in multi-dose vials (10 doses/vial) containing DL-α-tocopherol (53.76 mg/mL) and squalene (43.44 mg/mL). Immediately prior to use 0.3 mL of CoVLP and 0.3 mL of AS03 were mixed gently 1:1 volume: volume in the CoVLP vial and a 0.5 mL withdrawn for injection. All injections were administered intramuscularly using a 23g needle in the deltoid. The first and second doses were administered contralaterally when possible.
Study Design
The phase 2 portion of the study is a randomized, observer-blinded, placebo-controlled study with male and female subjects. The study was approved by a central Research Ethics Review Board (Advarra 372 Hollandview Trail, Suite 300, Aurora, ON L4G 0A5 Canada) as well as the Health Products and Food Branch of Health Canada and was carried out in accordance with the Declaration of Helsinki and the principles of Good Clinical Practices. Written informed consent was obtained from all study participants prior to any study procedure. Subjects were offered modest compensation for their participation in this study (ie: time off work, displacement costs).
Subjects were screened up to 14 days in advance of the first vaccine administration and must have demonstrated a satisfactory baseline medical assessment by history, general physical examination, hematologic, biochemic, and serologic analysis. Although a test for SARS-CoV-2 antibodies was performed at screening using a commercial ELISA that targets the nucleocapsid (N) protein (ElecSys: Roche Diagnostics), both seronegative and seropositive subjects were enrolled.
For Population 1 (Adults), subjects had to be 18-64 years of age. For Population 2 (Older Adults), subjects had to be 65 years of age or older and to be non-institutionalized (eg, not living in rehabilitation centers or old-age homes; living in an elderly community was acceptable).
For both study population presented, subjects must have had a body mass index less than 30 kg/m2 and be in good general health with no clinically relevant abnormalities that could jeopardize subject safety or interfere with study assessments, as determined by medical history, physical examination, and vital signs. Investigator discretion was permitted with this inclusion criterion. Female subjects of childbearing potential had to have a negative serum pregnancy test result at screening and/or a negative urine pregnancy test result at vaccination. Additional exclusion criteria included i) any significant acute or chronic, uncontrolled medical or neuropsychiatric illness, ii) any chronic medical condition associated with elevated risk of severe outcome of COVID-19 including obesity, diabetes (type 1 or type 2), significant cardiovascular or respiratory diseases including asthma, chronic renal failure, disorders of bleeding/coagulation, chronic inflammatory or autoimmune conditions, immunosuppressive conditions (including HIV), and hypertension, iii) any confirmed or suspected current immunosuppressive condition or immunodeficiency, including cancer, HIV, hepatitis B or C infection, iv) current autoimmune disease, v) administration of any medication or treatment that could alter the vaccine immune response, vi) administration of any vaccine within 14 days prior to vaccination or planned administration of any vaccine up to Day 28 of the study, vii) administration of any other SARS-CoV-2 / COVID-19, or other experimental coronavirus vaccine at any time prior to or during the study, viii) history of virologically-confirmed COVID-19, ix) a rash, dermatological condition, tattoos, muscle mass, or any other abnormalities at injection site that could interfere with injection site reaction rating, x) use of prophylactic medications (eg, antihistamines [H1 receptor antagonists], nonsteroidal anti-inflammatory drugs [NSAIDs], systemic and topical glucocorticoids, non-opioid and opioid analgesics) within 24 hours prior to the Vaccination, xi) history of a serious allergic response to any of the constituents of CoVLP including AS03, xii) history of documented anaphylactic reaction to plants or plant components (including tobacco, fruits and nuts), xiii) personal or family (first-degree relatives) history of narcolepsy, xiv) a history of Guillain-Barré Syndrome. Enrollment into the Phase 2 portion of the study was closed on 25 March 2021.
The participants and the personnel collecting the safety information and working in testing laboratories remained blinded to treatment allocation. On Day 0, D21 and D42, serum and peripheral blood mononuclear cells (PBMC) were processed for immune outcomes. All safety information was collected, and all laboratory procedures were carried out by study staff blinded to treatment allocation. There were no major Protocol changes during the conduct of this study prior to the preparation of the current manuscript.
Primary and Secondary Objectives
The primary objectives of the Phase 2 portion of the study were to assess safety and tolerability and immunogenicity to CoVLP and AS03 at day 0, 21, and 42 post vaccination compared to placebo in Adults and Older Adults.
Primary safety outcomes were the occurrence(s) of i) immediate AEs within 30 minutes after each vaccination; ii) solicited local and systemic AEs up to 7 days after each vaccination; iii) unsolicited AEs, serious AEs (SAEs), AEs leading to withdrawal, AEs of special interest (AESIs), and deaths up to 21 days after each vaccination; iv) normal and abnormal urine, haematological, and biochemical values.
Primary immunogenicity outcomes were i) neutralizing antibody (NAb) titers measured using a pseudovirion neutralization assays and ii) interferon (IFN)-γ and IL-4 ELISpot responses at 21 days after each dose of vaccine.
Secondary objectives were to assess the immunogenicity in study populations at days 128, 201 and 386 post-vaccination.
A secondary safety outcome was the occurrence(s) of SAEs, AEs leading to withdrawal, AESIs, and deaths from 22 days after the last vaccination up to the end of the study that is still on-going. Secondary immunogenicity outcomes were immune responses measured at days 128, 201 and 386 post-vaccination.
The safety and immunogenicity data collected at later timepoints in this on-going study will be released once study follow-up has been completed.
Safety Assessments
Both passive (diary) and active monitoring of safety signals were performed for the first 42 days of the study and will be continued throughout the study. Active monitoring included telephone contacts with subjects one and eight days (D1, D8) after each vaccination as well as a site visit on D3 after vaccination. Solicited AEs were assessed by the subjects as Grade 1 to 4 (mild, moderate, severe, or potentially life-threatening) according to the criteria previously described 21. Unsolicited AEs, and AEs leading to subject withdrawal were collected up to D21 after each vaccination. The following event(s) would pause or halt the study for further review and assessment of the event(s) by the IDMC: i) Any death, ii) Any vaccine-related SAE; iii) Any life-threatening (Grade 4) vaccine-related AE; iv) If 10 % or more of subjects in a single treatment group, experienced the same or similar listed event(s) that could not be clearly attributed to another cause: v) A severe (Grade 3 or higher) vaccine-related AE; vi) A severe (Grade 3 or higher) vaccine-related vital sign(s) abnormality; vii) A severe (Grade 3 or higher) vaccine-related clinical laboratory abnormality.
In the event that a pre-defined safety signal was met in any treatment group, at least a transient halt to the study was planned to permit complete evaluation of the reported event(s) and to consult with the IDMC.
Subjects will return to the Investigator site on Days 128, 201, and 386 for safety follow-ups and immunogenicity assessments.
Safety signals for VAED, hypersensitivity reactions, and potential immune-mediated diseases were monitored as previously described 21.
SARS-CoV-2 Pseudovirus Immunogenicity- Neutralisation Assay
Full details of the pseudovirus neutralization assay (Nexelis, Quebec, Canada) have previously been described 21. Briefly, the assay is based on a genetically modified Vesicular Stomatitis Virus (VSV) from which the glycoprotein G was removed, and a luciferase reporter introduced. The modified VSV vector expresses full length SARS-CoV-2 S glycoprotein (NXL137-1 in POG2 containing 2019-nCOV Wuhan-Hu-1; Genebank: MN908947) from which the last nineteen amino acids of the cytoplasmic tail were removed (rVSVΔG-Luc-Spike ΔCT). Pseudovirions are mixed with vaccinee sera and the degree of neutralization quantified using human ACE-2 expressing VERO cells and reduction in luciferase-based luminescence. For each sample, the neutralizing titer was defined as the reciprocal dilution corresponding to the 50% neutralization (NT50), when compared to the pseudoparticle control. Samples below cut-off were attributed a value of 5 (half the minimum required dilution).
To facilitate the comparability of results across different trials, the WHO International Standard for anti-SARS-CoV-2 immunoglobulin (human; NIBSC code: 20/136) was established to allow conversion of neutralization assay titers into international units (IU/mL). This standard consists of pooled plasma obtained from eleven individuals recovered from SARS-CoV-2 infection. Upon multiple assessments using this validated PNA assay, a conversion factor of 1.872 was established. Hence, the antibody titers presented throughout this manuscript can be expressed as IU/mL by dividing the NT50 by this factor.
Immunogenicity- Interferon-γ and Interleukin-4 ELISpot
PBMC samples from study subjects were analyzed by IFN-γ or IL-4 ELISpot (Caprion, Quebec, Canada) using a pool of 15-mer peptides with 11aa overlaps from SARS-CoV-2 S protein (USA-CA2/2020, Genbank: MN994468.1, Genscript, purity >90%). Full details of the methodology are detailed elsewhere 21.
Convalescent serum and plasma samples
Sera/plasma from COVID-19 convalescent patients were collected from a total of 35 individuals with confirmed disease diagnosis. Time between the onset of the symptoms and sample collection varied between 27 and 105 days. Four sera samples were collected by Solomon Park (Burien, WA, USA) and 20 sera samples by Sanguine BioSciences (Sherman Oaks, CA, USA); all were from non-hospitalized individuals. Eleven plasma samples were collected from previously hospitalized patients at McGill University Health Centre. Disease severity were ranked as mild (COVID-19 symptoms without shortness of breath), moderate (shortness of breath reported), and severe (hospitalized). These samples were analysed in parallel of clinical study samples, using the assays described above. Demographic characteristics were previously described in Ward et al. 21.
Analysis Populations and Statistical Analysis Plan
Randomization was managed by Syneos Health with Medicago oversight using Medidata Rave RTSM interactive randomization tool (2021.2.0, Medidata, USA). The sample size of 306 vaccinated Adults and 282 Older Adults made it possible to perform the initial evaluation of the vaccine immunogenicity and detect major differences in rates of AEs between groups. The sample size was not large enough to detect all types of, including less frequent or rare, AEs. With 494 subjects receiving the CoVLP formulation, there was at least 95% probability of observing an AE that occurs as frequently as 1 in 165 vaccinees. The analyses of all immunogenicity endpoints were performed using the Intent-to-Treat population set (ITT). The ITT consists of all randomized subjects who received the CoVLP and AS03 or placebo and analyzed prior to the data cut (Adults: Day 21 n=299; Day 42 n=299; Older Adults Day 21 n=255; Day 42 n=165). Immunogenicity was evaluated by humoral immune response (NtAb assays) and cell-mediated immune (CMI) response (ELISpot) induced in subjects on D0, 21 and 42. To assess the humoral immune response, the GMT was calculated and compared between CoVLP and AS03 and placebo using an ANOVA on the log-transformed titers. The log transformation was used to meet the normal assumption for the ANOVA. At each timepoint, the GMT and corresponding 95% CI of each treatment were obtained by exponential back-transformation of the least square mean. GMT were compared between Adults and Older Adults at Day 21 and Day 42 using an ANOVA. Fisher’s exact test was used to compare seroconversion rate between the treatment groups. The 95% CI for seroconversion was calculated using the exact Clopper-Pearson method. The specific T helper type 1 (Th1) and Th2 CMI responses along with the corresponding 95% CI for the median induced on D0, D21 and D42 were measured by the number of T cells expressing IFN-γ and IL-4 respectively, using ELISpot. The difference in IFN-γ and IL-4 response between treatment group at each timepoint was compared using a non-parametric Wilcoxon Rank Sum Test. Since the response between timepoints are paired data, the Wilcoxon Signed Rank Test was used to estimate the difference in response between timepoints, along with the corresponding 95% CI for the median separately for each treatment group. The difference in IFN-γ and IL-4 were also compared between Adults and Older Adults at Day 21 and Day 42 using a Wilcoxon Rank Sum Test. Safety assessment are based on the Safety Analysis Set, i.e. all subjects who received either the CoVLP candidate vaccine with or without an adjuvant. Occurrence and incidence of safety events were reported for each treatment groups. No formal hypothesis-testing analysis of AE incidence rates was performed, and results were not corrected for multiple comparisons.
Acknowledgements
The authors would like to acknowledge Karyne Framand with support identifying appropriate references. The authors acknowledge Dr Matthew P Cheng (Research institute of the McGill University Health Centre) for supplying convalescent plasma samples from hospitalized Covid patients. The authors also wish to acknowledge all the Medicago employees, their contractors and all the volunteers who participated in the study as well as the site investigators and their staff who conducted the studies with a high degree of professionalism.
References



