
ABSTRACT
Background Cutaneous drug eruptions are a significant source of morbidity, mortality, and cost to the healthcare system. Identifying the culprit drug is essential; however, despite numerous methods being published, there are no consensus guidelines.
Objectives Conduct a scoping review to identify all published methods of culprit drug identification for cutaneous drug eruptions, compare the methods, and generate hypotheses for future causality assessment studies.
Eligibility criteria Peer-reviewed publications involving culprit drug identification methods.
Sources of evidence Medline, Embase, and Cochrane Central Register of Controlled Trials.
Charting methods Registered PRISMA-ScR format protocol on Open Science Forum.
Results In total, 135 publications were included comprising 656,635 adverse drug events, most of which were cutaneous. There were 54 methods of culprit drug identification published, categorized as algorithms, probabilistic approaches, and expert judgment.
Algorithms had higher sensitivity and positive predictive value, but lower specificity and negative predictive value. Probabilistic approaches had lower sensitivity and positive predictive value, but higher specificity and negative predictive value. Expert judgment was subjective, less reproducible, but the most frequently used to validate other methods. Studies suggest that greater accuracy may be achieved by specifically assessing cutaneous drug eruptions and using combinations of causality assessment categories.
Conclusions Culprit drug identification for adverse drug reactions remains a challenge. Many methods have been published, but there are no consensus guidelines. Using causality assessment methods specifically for cutaneous drug eruptions and combining aspects of the different causality assessment categories may improve efficacy. Further studies are needed to validate this hypothesis.
INTRODUCTION
Rationale
Skin reactions are the most common manifestation of adverse drug events (ADEs). Cutaneous drug eruptions (CDEs) are a common and a significant source of morbidity and mortality. (1) The mainstay of management is identifying and stopping the culprit drug. (2) Many methods have been proposed for culprit drug identification (CDI), but presently there are no consensus guidelines. (2–4) There are few causality assessment methods (CAMs) that are specific to CDEs, but most methods are applied to all types of ADEs.
There are 3 main categories of causality assessment: operational algorithms, probabilistic approaches, and expert judgment. Each of the published methods of culprit drug identification usually fit into one of these categories. (4,5) Operational algorithms involve specific criteria related to drug exposure and the resulting adverse event. They are relatively simple to use and are reproducible, but can be restrictive because specific information is often required. (6) Probability assessment methods use likelihood ratios relating to the case. For example, different types of CDEs often have specific latencies between drug exposure and rash onset, which narrows the time-frame when the drug exposure likely occurred. Amongst other criteria, the frequency with which the drug has been reported to cause the adverse event is expressed as an overall probability score, implicating the drug with the highest score as the culprit drug. (7,8) Unfortunately, such methods often rely on previously reported adverse events. Probabilistic methods can be complex, time consuming, do not account for unreported drugs, and are not always practical in real-world settings. (6,9) Expert judgment approaches are based on the clinical opinion of an expert physician, the physician treating the patient, or sometimes a clinical pharmacist. All available data in a case is considered, and how much weight each piece of data holds is determined by the expert and a decision regarding causality is made based on this judgment. Although this is one of the simplest methods, it is often subjective and biased, with poor inter-rater agreement and reproducibility. (6,10)
ADEs are heterogeneous, and often affect more than one organ system. Clinical signs of drug eruptions have been extensively studied and categorized. Cutaneous manifestations often happen early and may allow for a more accurate timeline compared to internal involvement which can often be sub-clinical. Developing CAMs using ADE databases may not always be accurate because of the heterogeneity between drug exposures, cutaneous and systemic manifestations. A scoping review was employed to identify all published methods of CDI for CDEs, compare the methods to uncover strengths and limitations, and generate hypotheses for future causality assessment studies.
METHODS
Protocol and Registration
The protocol was drafted using the Preferred Reporting Items for Systematic Reviews and Meta-analysis Protocols extension for scoping reviews (PRISMA-ScR) (11), and was registered with Open Science Forum (OSF). (Bose R, Boshra M, Ogbalidet S, Finstad A, Fahim S. A scoping review of cutaneous drug eruptions and methods for identifying culprit drugs. 2020. osf.io/r7k3z.)
Eligibility criteria
Inclusion Criteria: Peer-reviewed publications were included if they were written in English, published in 1993 or later, and involved a method of CDI. A cut-off of 1993 was selected because notable CDE reclassifications had taken place prior to this time, specifically the classification of Stevens Johnson syndrome as a separate entity from erythema multiforme. Relevant review articles were analyzed separately from articles containing primary patient data.
Exclusion Criteria: Publications were excluded if there was no mention of a method for identifying culprit drugs, if all participants were ≤18 years old, or if the publication was of low-level evidence (i.e. case reports, case series involving <10 cases, commentaries, editorials, conference posters/abstracts or opinion pieces).
Information sources
Medline (Ovid), Embase, and Cochrane Central Register of Controlled Trials (CENTRAL) databases were used. The most recent search was executed: February 5th, 2020. Studies were imported into Covidence, a systematic review software.
Search strategy
Developed and conducted with the assistance of our institutional research library services. See Table 1 for details.
The following electronic search strategy, developed with assistance of a research librarian, was conducted with Medline (Ovid), Embase, and Cochrane Central Register of Controlled Trials (CENTRAL) databases.
Selection of sources of evidence
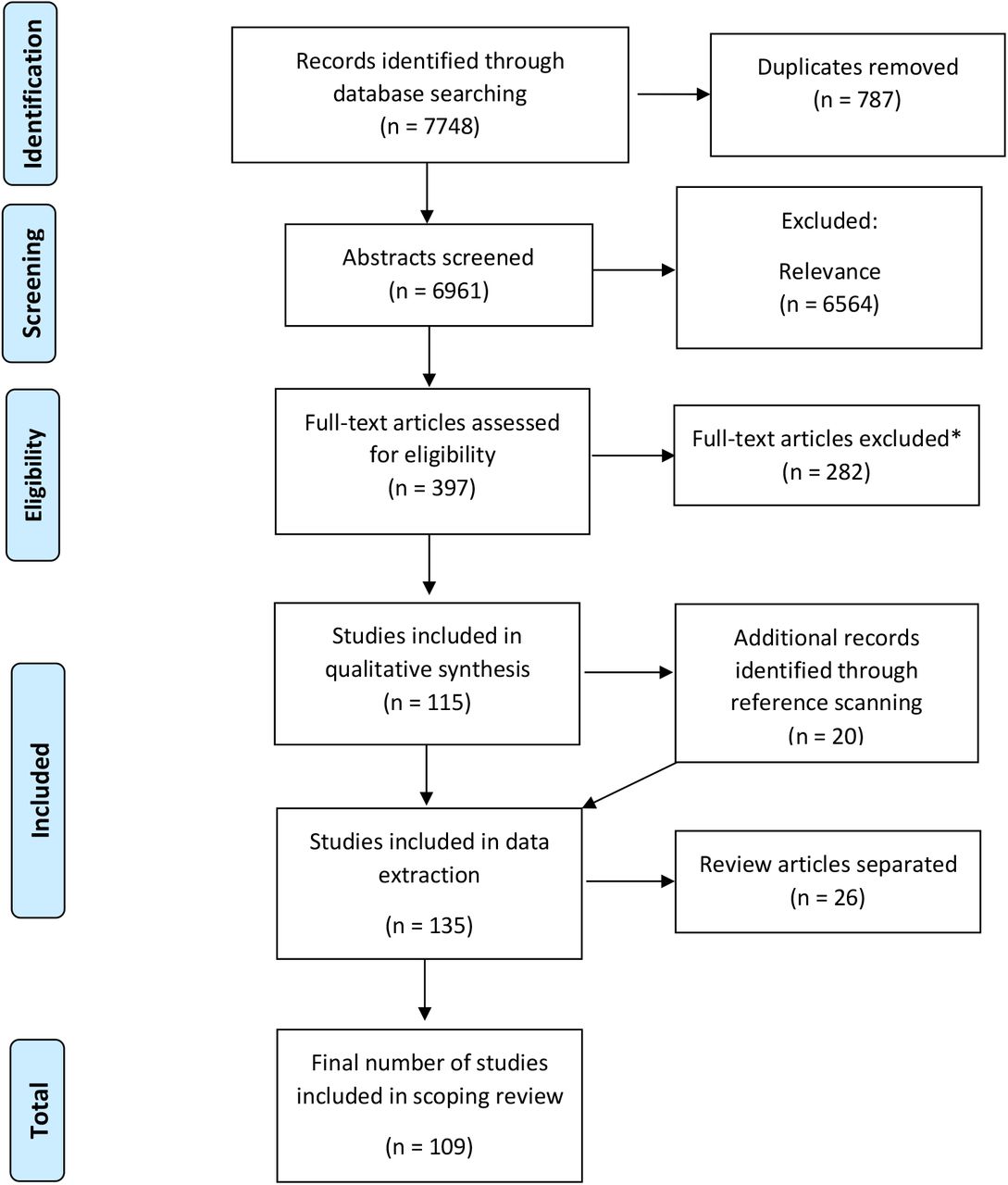
A list of publications was generated with the search strategy, and duplicates were removed. Two groups of reviewers independently screened all abstracts followed by full texts. Disagreements were settled by consensus vote. Reference lists of included publications were screened for relevant studies not captured by the initial search. Publications involving patients were separated from review articles (See Figure 1).
{kind=link}
PRISMA-ScR flow diagram mapping the process used to include and exclude publications. *Excluded studies (n=282): Wrong study design (n=106), wrong outcomes (n=89), abstract only (n=28), reviews with causality testing not included (n=16), wrong patient population (n=12), wrong setting (n=9), pediatric only (n=7), posters (n=6), duplicates (n=5), unavailable (n=2) and not available in English (n=2).
Data charting process
A priori data categories were used to organize extracted data. Review articles were analyzed separately to determine if additional data categories should be extracted from the primary studies containing patient data. Quality assurance assessment for accuracy of entered data was conducted by the primary author.
Data items extracted
The list of data extraction items can be found in Table 2. The data from included publications were organized into tabular format using Microsoft Excel.
A priori data extraction items for included publications in the scoping review.
Synthesis of results
The extracted data from each publication was entered into a database for easier synthesis and comparison of data (Supplemental Table 4). Some CAMs used different syntax to assign a likelihood rating for suspected culprit drugs. Analogous terms were grouped together to compare the different CAMs (Table 5). Most studies used a Likert-style scale to assign different levels of causality for suspected culprit drugs being investigated. For example, for 5-term scales, causality assessment Method A may report the likelihood of a culprit drug as: very likely, likely, possible, unlikely, or very unlikely. Method B may report likelihood as: certain, probable, possible, doubtful, or exclude. In this case the analogous categories were grouped: ‘Certain/very likely’, ‘probable/likely’, ‘possible’, ‘doubtful/unlikely’, and ‘exclude/very unlikely’. Some methods used a 3 term rating scale such as ‘positive’, ‘neutral’, and ‘negative’. To report this 3-term scale with the 5-term scales the ‘positive’ rating would be grouped with ‘very likely/certain’, the ‘neutral’ rating would be grouped with ‘possible’ and the ‘negative’ rating would be grouped with ‘exclude/very unlikely’.
Characteristics of included papers (N=135; 109 studies, 26 reviews). ADE: adverse drug events, SJS/TEN: Stevens Johnson syndrome/toxic epidermal necrolysis, MDE: morbilliform drug eruption, FDE: fixed drug eruption, Drug rash eosinophilia and systemic symptoms.
Table 4. Raw extracted data form. Supplemental. Excluded from pre-print.
Analysis and comparison of criteria/components of published methods of culprit drug identification. Green = criteria/component present, White = criteria/component not present in method. L: latency; S: prior sensitization; A: alternate diagnosis; DL: drug level/dose change; C: challenge, DC: de-challenge, RC: re-challenge; ET: eruption type; CT: confirmatory testing; O : other drug suspect; DCt: Drug chart; ASPS: Spanish pharmacovigilance algorithm system C/D/P/C/V: certain, definite, positive, causative, very likely; P/L: probable/likely; Po: possible; R/U/D/C/Du: remote/unlikely/doubtful/coincidental/dubious; N/U/E/Co: negative, unrelated, exclude, contradictory; Ua/Uc/C: unaccessable/unclassifiable/conditional.
For the studies reporting quantitative results such as sensitivity and specificity (See table 6), the data analyzed for this study was reported in a descriptive manner in line with accepted reporting guidelines for scoping reviews.(11)
Published causality assessment methods that have been quantitatively studied. SN: sensitivity, PPV: positive predictive value, SP: specificity, NPV: negative predictive value, SPVA: Spanish pharmacovigilance algorithm, BARDI: Bayesian adverse reaction diagnostic instrument. Cornelli, Emanueli, Hsu Stoll, Jones, Kramer and Naranjo algorithms assumed all the identified adverse events were ADRs therefore presenting 0% specificity and 0% NPV. Given (wider 95% CIs) as a result of the small number of algorithm’s high sensitivity, even for serious or uncases considered non-drug related by the GI.
Review articles were analyzed to ensure all necessary data items were used to extract data from primary studies and to compare the findings and associations uncovered in this review.
RESULTS
Selection of sources of evidence
Sources of evidence were gathered using the search strategy, registered on OSF (Table 1). The screening process, and application of inclusion and exclusion criteria was conducted as per the PRISMA-ScR extension protocol and reasons for exclusion of sources of evidence were recorded (Figure 1).
Characteristics of sources of evidence
The characteristics of included sources of evidence were recorded using the items outlined in Table 2 and shown in Table 3. Studies were primarily retrospective cohort, case-control, and prospective cohort or observational.
Results of individual sources of evidence
For the complete list of publications and extracted data included in the scoping review (Table 4, supplemental).
Synthesis of results
A total of 109 peer-reviewed articles with patient data involving at least one CDI method, were analyzed (raw data, Table 4, study characteristics Table 3). There were 26 review articles that were analyzed to compare parameters and determine the relevance in the present review (Table 7). Overall, data from 656,635 case events were represented. A total of 29 papers (26.6%) compared 2 or more CAMs, and 19 (17.4%) statistically analysed the methods. There were 54 different CAMs published and operational algorithms were the most studied (71 publications, 65.1%). From these 71 publications, 34 CAMs were identified as operational algorithms. There were 58 publications (53.2%) that studied probabilistic approaches in which 18 CAMs were identified. Finally, 48 publications (44.0%) involved the use of expert judgment and 2 different methods were identified. Many studies used more than one CAM.
Analysis of review article publications included in study. CDE: cutaneous drug eruptions; CDI: culprit drug identification; CAM: causality assessment methods; EEM: erythema exsudativum multiforme majus.
The benchmark, or standard, is a method assumed to be correct and can be used to assess or validate another CAM. Expert judgment was the most common standard used to validate other CAMs. Tissue biopsy was a component of the work-up in 27 studies (24.8%), and provocation/confirmatory testing (i.e. patch testing, prick testing, intradermal testing, challenge, re-challenge) was performed in 21 studies (19.3%). To statistically compare agreement between the benchmark method and the method(s) being studied, kappa values of agreement were sometimes included in studies.
Eleven publications (10.1%) studied lab-based methods for CDI either in the acute setting during a drug rash, or as confirmatory testing after an eruption had resolved. They can be divided into cytokine/cytotoxic-based testing and cell-based testing.
Review article analysis
There were 26 review articles included. Each review article dealt with the management of ADEs (Table 7). A minority were explicitly skin focused and reviewed CAMs with one type of drug eruption or delineated methods used to assess, diagnose, and categorize CDEs. There were 14 reviews that studied lab-based methods and provocation testing. The latest review of CDI methods was in 2016 and discussed a select number of methods, their strengths, and weaknesses. In-depth comparisons between methods were not conducted. (8) Only 3 reviews quantitatively assessed CAMs by calculating sensitivity (SN), specificity (SP), positive predictive value (PPV) and negative predictive value (NPV).(6,12,13) The studies were heterogeneous and often did not assess CDEs separately from other types of ADEs. If a study utilized different scoring categories (e.g. 5 factor vs. 3 factor Likert scale) then they were often excluded from the review; therefore, not all published CAMs were actually studied.
Diagnosing the type of drug eruption
Thirty-three types of CDEs were identified and the clinical and histologic characteristics, scoring systems, and commonly implicated drugs were investigated. SCARs have a significant morbidity and mortality risk. Clinical signs suggestive of SCARs include fever, prodromal malaise and fatigue, rapidly progressing rash, bullae/desquamation, Nikolsky sign, mucosal involvement, and systemic findings (liver, kidney, thyroid, GI, cardiac abnormalities). Risk factors have been identified that are associated with increased frequency and severity of drug hypersensitivity reactions. Specific risk factors are discussed in a subsequent section.
Latency between drug exposure and onset of rash
The latencies between drug exposure and rash onset are known to vary depending on drug rash type. Over 75% of published CAMs utilized time from drug exposure to rash onset as a criterion. It was also observed that there were drug class specific latencies, suggesting that drug rash type is not the only factor affecting latency. For example, a relatively shorter exposure to rash latency was seen with radio contrast dye (<6h) as well as antibiotics and acetaminophen/NSAIDs (<15 days). Drugs found to have longer latencies include anticonvulsants (>15 days) and xanthine oxidase inhibitors (21-90 days). (14,15)
These trends were noted when controlling for drug rash type in some publications, but more robust, larger studies are needed to confirm these associations. (16–18) Anticonvulsant hypersensitivity had a mean latency of 28 days when causing DRESS, an eruption known to have a longer latency. When DRESS was caused by an antibiotic, a drug class shown to have a shorter latency, the average delay was much shorter (∼18 days). (19) Another factor affecting latency occurs with re-exposure to the causative drug. It is well established that re-exposure (re-challenge) to a culprit drug shortens the latency independent of rash type or medication class. (20) While absolute latency ranges were very broad, most cases of a certain eruption type had either long or shot latencies on average. For example, eruptions with longer latencies include DRESS (∼14-42 days) and SJS/TEN (∼7-21 days), and eruptions with shorter latencies include urticaria (<24h), morbilliform drug eruption (∼4-14 days), AGEP (<4 days), and fixed drug eruption (∼7-14 days). (1,17,21)
If latencies differ by drug rash type, or drug class, it is possible that erroneously narrowing the latency range may result in a false negative causality assessment, missing the culprit drug and stopping the wrong medication.
Risk factors and associated conditions
Risk factors for severity and frequency of CDEs have been identified including: Polypharmacy, old age, female sex, re-exposure, liver and kidney disease, diabetes, HIV, malignancy, and certain HLA subtypes (14,19,22,23). Many of these risk factors are integrated into select diagnostic and prognostication tools (e.g DRESS RegiSCAR criteria, SCORTEN for SJS/TEN, RegiSCAR AGEP score). (14,19,22,23) Co-morbidities were also seen as important for ruling out non-drug related conditions (e.g. auto-immune disease, and infection). Accurate characterization of these risk factors as they relate to drug eruptions, and their prognostic significance should be considered when managing CDEs.
Causality methods comparison
This review identified 54 published CAMs. They share many similarities, differences, strengths, and limitations. CAMs were first compared based on their respective components (Table 5). Algorithmic methods tended to have more questions related to clinical changes with exposure to the suspected drug (challenge), discontinuation (de-challenge) and re-exposure (re-challenge). Probabilistic approaches tended to have more criteria related to ruling out other causes of the reaction, assessment of other potential culprit medications and determining how often the suspected drug had been reported to cause the CDE. Drug exposure to rash latency was a criterion in 66.0% of published methods. Prior sensitization was a criterion for 34.6% of methods (Algorithmic 45.5%, Probabilistic 16.7%). Considering an alternate diagnosis/cause was a criterion in 57.4% (algorithmic 67.7%, probabilistic 38.9%). An alternate drug cause or drug notoriety was a criterion in 31.5% (algorithmic 20.6%, probabilistic 44.4%). Considering dose changes and therapeutic drug levels were part of 44.2% of methods (algorithmic 60.6%, probabilistic 11.1%). Challenge, de-challenge, and rechallenge were criteria for 20.4%, 48.1, 60.4%, respectively (algorithm: 26.5%, 58.8%, 76.5%; Probabilistic: 5.6%, 22.2% and 33.3%). Causality assessment ratings were often reported on scales of varying levels such as the 5-point Likert scale (e.g. Very likely, likely, possible, unlikely, very unlikely). A 5-point scale for probability of causality was found in 25.9% of methods, of which 78.6% were algorithms, 7.1% probabilistic, and the remaining 14.3% from expert judgment CAMs. Less than a 5-point scale for probability of causality was found in 74.1% of methods, of which 57.5% were algorithms and 42.5% probabilistic approaches.
A number of studies and several review articles reported the efficacy (i.e. SN, PPV, SP, NPV) of many published methods to display how studies have attempted to validate, compare, and analyze the CAMs (See Table 6). Generally, algorithms had relatively higher SN and PPV, but lower SP and NPV. Probabilistic approaches generally had lower SN and PPV, but higher SP and NPV. Methods that combine elements of the different categories were found to be more effective in several studies. (24–26) Additional studies, such as with a systematic review, are required to determine the significance of this observation. Expert judgment was the most common CAM used as the standard when validating other methods, but was repeatedly noted to be subjective, have lower reproducibility and inter/intra-rater agreement.
There were 9 lab-based culprit drug investigations published in 11 studies and 14 reviews. They were mainly based on measurement of immune cells or inflammatory cytokine/chemokine parameters. The main tests included lymphocyte transformation test (LTT), interferon gamma release assay, CellScan technique, histamine releasing test (HRT), HLA-B allelic variation, granzyme B-ELISpot assay, granulysin expression, cytokine beads array assay, and chemi-informatics based QSAR model (quantitative structure-activity relationship).
DISCUSSION
Summary of evidence
Drug reactions pose a significant health problem, and are costly to the healthcare system. (27) ADEs are heterogeneous, and often affect more than one organ system. The most common organ for early manifestation of ADEs is the skin. Cutaneous manifestations may allow for a more accurate timeline compared to internal involvement which can often be sub-clinical. This may translate to more efficacious causality assessment. Developing CAMs using ADE databases may not always be accurate because of the heterogeneity between drug exposure, cutaneous and systemic manifestations. CAMs designed for CDE may, therefore, be higher yield, and easier to validate.
When dealing with drug eruptions, important aspects of the patient history include degree/duration of drug exposure, time of rash onset, confounding factors (e.g. comorbidities), rechallenge (re-exposure to drug), dechallenge (improvement with removal of the causative drug), and background epidemiological and clinical information. This data is also vital for accurate pharmacovigilance adverse event reporting (6)
Medication history and onset of cutaneous eruption
Accurate documentation regarding medication administration (i.e. when drug was started, last taken, and dose increases) is important in order to determine the latency between possible drug exposures and the reaction. CDE may allow for the most accurate determination of latency as cutaneous manifestations are often an early finding compared to signs of end organ damage. Studying CAMs for CDE separate from non-skin ADE could potentially ameliorate the issue of heterogenicity and problematic validation methods. (2,20,28)
Determining the type of eruption and causative drug
Different types of drug eruptions have different causative drugs and different latencies between exposure and rash onset. This review has demonstrated that in addition to drug rash type, drug classes may also play an important role in affecting this latency. If drug class specific latency ranges can be standardized in conjunction with rash type, the latency window could be narrowed, increasing accuracy and decreasing confounding by concurrent medications and conditions. As we learn more about the pathophysiology of different drug rashes, we may uncover potential diagnostic and therapeutic markers using lab-based techniques, but the importance of clinical methods must be underscored, especially with rapidly progressive and deadly SCARs. (29)
Tissue biopsy can often be helpful to determine the type of drug eruption or rule out non-drug related conditions, but often have non-specific findings and may delay appropriate management.
Causality assessment methods
A systematic review of causality assessment with adverse drug reactions in 2008, identified approximately 40 different CAMs, but did not specifically address the issue of cutaneous adverse drug events. (6) The information gathered was very heterogeneous and effect modification may have obscured certain findings because of the inherent differences between clinical behaviour and diagnostic accuracy with cutaneous versus other types of ADEs. The current review has identified 54 CAMs, not including investigative or lab-based techniques. The number of published methods continues to grow, yet the data suggests we are no closer to being able to reliably test the efficacy of any proposed methods, nor develop guidelines to guide causality assessment. The findings also show that compared to systemic/internal ADEs, cutaneous adverse reactions may be easier to diagnose early. There are also more accessible investigations available to diagnose CDEs (e.g. morphology and evolution, tissue biopsy, direct immunofluorescence, indirect immunofluorescence, in vitro blood tests, skin based confirmatory testing and HLA-typing). This may allow for more accurate ascertainment of date of onset, progression, and improvement over time, making the study of CAMS more effective and may even serve as the benchmark to appraise and develop consensus guidelines for CDI in the future.
There are three main categories of ‘causality assessment and most of the proposed methods fall into one or more of them. Algorithmic approaches (i.e. operational algorithms), were found to be the most commonly studied method, had high sensitivity and PPV, and were easiest to use. Probabilistic approaches were the second most commonly studied method and had the highest specificity and NPV, but were time consuming, complex, and not always practical. Lastly, expert judgment, which was often used as the standard when studying other methods, was subjective, and had poor intra/inter-rater reproducibility. Confounding variables, including multiple medications and co-morbidities, compromise algorithmic sensitivity and specificity. (6)
A small number of studies compared more than one CAM and when they studied a method that used aspects of more than one category (e.g. combined algorithmic and probabilistic approaches), they were found to have higher efficacy and reduced some limitations seen in the methods used separately. (3,26,30) It has been suggested that greater accuracy may be obtained by first employing the method with the highest sensitivity to capture true positive cases (e.g. algorithmic approach), followed by employing a method with greater specificity to rule out the greatest number of true negatives (e.g. probabilistic method), resulting in a higher percentage of true positives than either method alone.
Investigations: Lab-based, pharmacogenomic and confirmatory testing
Lab-based investigations are becoming more prevalent and may complement clinical CAMs. We identified 11 studies and 14 reviews that compared various types of in vitro testing: lymphocyte transformation test (LTT), interferon gamma release assay, CellScan technique, histamine releasing test (HRT), HLA-B allelic variation, granzyme B-ELISpot assay, granulysin expression, cytokine beads array assay, and chemi-informatics based QSAR model (quantitative structure-activity relationship). Limitations of lab-based studies included cost, expertise needed to conduct tests, interpretation of results, and the fact that lab-based ex vivo investigations may not be representative of in vivo conditions. As well, allergies to drug intermediates or drug-carrier protein conjugates may result in false negatives because the techniques often test the parent drug and not the intermediate or metabolite that may actually be the culprit such as with acrolein, the metabolite of cyclophosphamide, responsible for hemorrhagic cystitis, a serious ADR. (31,32) Generally, they have shown promising results, but with significant variability. If sufficiently validated, these investigations may be useful alternatives to the riskier current gold standard, which is re-exposure to the culprit drug.
Methods of confirmatory testing include re-exposure or provocation testing which can be done through oral or cutaneous modalities such as with patch, prick and intradermal testing. The efficacy of this type of testing varies on drug eruption type and causative drug. There is also a risk for severe reactions caused by re-exposure to the culprit drug, even in small quantities. Confirmatory/provocation testing usually needs to be performed 4-6 weeks after the eruption has resolved. Patch testing was reported to be most accurate for SDRIFE, AGEP, FDE, DRESS, MDE, and to a lesser degree SJS/TEN. Cross-reactivity between different antiepileptic drugs was also detectable. (33–36).
Limitations
This scoping review intended to collate all published, peer-reviewed works relating to CDI. Limitations include the possibility that our search strategy did not to capture all appropriate papers. This was mitigated by scanning the references of included papers to identify sources not captured by our search strategy. A scoping review is descriptive and meant to gather available information rather than attempt to statistically compare published methods, conduct meta-analyses, or determine superiority. Cutaneous reactions may be easier to identify by patients and physicians than systemic ADEs. Some of the included studies used national and international ADE registries that did not always specify if the ADE was cutaneous or systemic. Some of the CAMs were studied using these databases containing all types of drug reactions. This may have contributed to why some of the studied CAMs performed poorly and with low reproducibility. Standard, or benchmark, methods for validating or comparing CAMs can be problematic. The accuracy of the standard, which was most commonly expert judgment or provocation testing, may themselves be inaccurate. Additionally, many CAMs do not account for polypharmacy, especially when drugs are initiated concomitantly. Stopping multiple drugs may leave other co-morbidities untreated which may be a potential confounder when assessing ADEs severity, response to treatment and resolution after stopping the culprit drug.
CONCLUSIONS
The mainstay of managing drug eruptions is identifying and stopping the culprit drug, which can be challenging. This review has synthesized the highest quality published methods available, focusing on CDEs. While none of the 54 published methods have been shown to be the most effective, consistently accurate, or widely applicable, some have shown promise, including CAMs that combine more than one category (e.g. operational algorithms combined with probabilistic approaches), lab-based methods to test for drug specific immune cells, and HLA-based pharmacogenomic risk assessment. Confirmatory testing such as with provocation/re-challenge, patch testing, and intradermal testing are currently the gold standard for correct drug identification, but they too can have variable efficacy, risks, and are mainly applicable 4-6 weeks after the eruption has subsided. From this scoping review, more studies can be conducted that integrate the strengths of published CAMs and avoid the limitations seen in past methods.
Data Availability
Sources of evidence: Medline, Embase, and Cochrane Central Register of Controlled Trials.
FUNDING
No funding was required for this study.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to disclose.
Appendix
Footnotes
Funding statement: This article has no funding source.
Conflict of interest: The authors have no conflict of interest to declare.
IRB status: Exempt from review
ABBREVIATIONS AND ACRONYMS
- ADE
- Adverse drug event
- AGEP
- Acute generalized exanthematous pustulosis
- CAM
- Causality assessment method
- CDE
- Cutaneous drug eruption
- CDI
- Culprit drug identification
- DIHS
- Drug induced hypersensitivity syndrome
- DRESS
- Drug reaction with eosinophilia and systemic signs
- EM
- Erythema multiforme
- FDE
- Fixed drug eruption
- HHV6 & 7
- Human herpes virus 6 & 7
- HRT
- Histamine release assay
- LTT
- Lymphocyte transformation test
- NPV
- Negative predictive value
- PPV
- Positive predictive value
- SJS
- Stevens Jonson syndrome
- SN
- Sensitivity
- SP
- Specificity
- TEN
- Toxic epidermal necrolysis
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.
- 35.
- 36.↵
- 37.
- 38.
- 39.
- 40.
- 41.
- 42.
- 43.
- 44.
- 45.
- 46.
- 47.
- 48.
- 49.
- 50.
- 51.
- 52.
- 53.
- 54.
- 55.
- 56.
- 57.
- 58.
- 59.
- 60.
- 61.
- 62.
- 63.
- 64.
- 65.
- 66.
- 67.
- 68.
- 69.
- 70.
- 71.
- 72.
- 73.
- 74.
- 75.
- 76.
- 77.
- 78.
- 79.
- 80.
- 81.
- 82.
- 83.
- 84.
- 85.
- 86.
- 87.
- 88.
- 89.
- 90.
- 91.
- 92.
- 93.
- 94.
- 95.
- 96.
- 97.
- 98.
- 99.
- 100.
- 101.
- 102.
- 103.
- 104.
- 105.
- 106.
- 107.
- 108.
- 109.
- 110.
- 111.
- 112.
- 113.
- 114.
- 115.
- 116.
- 117.
- 118.
- 119.
- 120.
- 121.
- 122.
- 123.
- 124.
- 125.
- 126.
- 127.
- 128.
- 129.
- 130.
- 131.
- 132.
- 133.
- 134.
- 135.
- 136.
- 137.
- 138.
- 139.
- 140.
- 141.
- 142.
- 143.
- 144.
- 145.
- 146.
- 147.
- 148.
- 149.
- 150.



