
Abstract
Objective Reports of cerebral venous thrombosis (CVT) after ChAdOx1 vaccination against SARS-CoV-2 have raised safety concerns and an emerging mechanism termed vaccine induced immune thrombotic thrombocytopenia (VITT) was identified. We aimed to estimate the frequency of CVT and other cerebrovascular events after vaccination with BNT162b2, ChAdOx1, and mRNA-1273, 114 German Departments of Neurology participated in a systematic survey.
Design descriptive study.
Setting Germany.
Population Patients with reported cerebrovascular events within the first month after a COVID-19 vaccine administration.
Methods We designed web-based questionnaire, which was e-mailed to all Departments of Neurology of University and non-university hospitals in Germany on April 6, 2021. Data collection was closed at midnight on April 14, 2021. We asked to report cases of cerebral sinus-venous thrombosis, cerebral venous thrombosis, ischemic stroke and haemorrhage within one month of a COVID-19 vaccination. Incidence rates of cerebral events and CVT within one month from first vaccine shot administration was calculated by using official statistics of 9 German States.
Results A total of 62 cases were detected, of whom 45 had CVT, 9 primary ischemic stroke, 4 primary intracerebral hemorrhage (ICH), and 4 other events. Eleven patients of 60 (18.3%) had a fatal outcome. Mean age was 46.7 years (48 patients <60 years, 77.4%), 75.8% of patients were female. Fifty-three events were observed after vaccination with ChAdOx1 (85.5%), 9 after BNT162b2 (14.5%). No events were reported after mRNA-1273 vaccination. The overall incidence rate of CVT within one month from first dose administration was 6.5 (95% CI, 4.4 to 9.2) per 100,000 person-years and 8.8 (95% CI, 6.4 to 11.9) for any included cerebrovascular event. The one-month incidence rate of CVT was higher among ChAdOx1 vaccinated persons (17.9, 95% CI, 11.8 to 26.1). The incidence rate ratio was 9.68 (3.46 to 34.98) for ChAdOx1 compared to mRNA-based vaccines and 3.14 (1.22 to 10.65) for women compared to non-women after adjusting for age group. In 26/45 patients with CVT (57.8%), VITT was graded highly probable, in 19/45 patients (42.2%) the association was less likely. A high-grade probability was not confined to CVT but also occurred in 5/9 patients (55.6%) with primary ischemic stroke and 2/4 patients (50%) with ICH following vaccination.
Conclusions Given an incidence of CVT in the general population of 0.22 – 1.75 per 100,000 person-years, these findings point towards and higher risk for CVT after ChAdOx1 vaccination, especially for women.
Introduction
A major breakthrough in managing the COVID-19 pandemic was the development and administration of vaccines against SARS-CoV2, namely BNT162b2 (BioNTech/Pfizer), mRNA-1273 (Moderna), Ad26.COV2.S (Johnson & Johnson) and ChadOx1 (AstraZeneca). Typical side effects of these vaccines were reported in clinical trials with several thousands of volunteers, but without evidence of a vaccine-associated increase in thromboembolic events1–5. Until April 2021, several vaccines have been approved and administered to millions of people. In Germany, 16,428,425 persons received the first and 5,517,282 the second dose of a vaccine as of April 18th, 2021 (https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Daten/Impfquotenmonitoring.xlsx?__blob=publicationFile). This included about 16.2 million doses BNT162b2, 1.2 million doses mRNA-1273 and 4.6 million doses of inChAdOx1m.
Outside of the context of COVID-19 vaccination, cerebral venous thrombosis is a very rare disease with an incidence of about 0.22 – 1.75 per 100.00 person-years, based on data from four European countries, Australia, Iran and Hong Kong6–8. Well-known risk factors are female sex, pregnancy, infections and hypercoagulability9. Within hypercoagulability, hormone-related and genetic prothrombotic disorders are the most frequent causes10.
Until the end of March 2021, the majority of persons vaccinated with ChAdOx1 in Germany were below the age of 65 years (https://www.pei.de/DE/service/presse/aktuelles/). The vaccine was initially only recommended in Germany for persons below age 65 years due to insufficient data on efficacy and safety among the elderly. In several European countries, cases of cerebral venous thrombosis were reported in temporal context with ChAdOx1 vaccine administration. An immune-mediated mechanism termed vaccine-induced thrombocytopenic thrombosis (VITT) has been suggested to underlie these serious adverse events11–13. At the beginning of March 2021, 30 venous thrombo-embolic events were reported to EMA out of about 5 million persons who had received the ChAdOx1 vaccine at that time14. At that time, the Danish National Patient Registry did not report an increased incidence of thrombo-embolic events in the Danish population but excluded cases of sinus-venous thrombosis from their analysis because of low incidence15.
The aim of this report is to describe cases and estimate the incidence of cerebrovascular events in temporal relation to COVID-19 vaccination reported in Germany until April 15th, 2021 based on a retrospective survey.
Methods
Data collection
We designed a web-based questionnaire which was e-mailed to all Departments of Neurology of University (n=40) and non-university (n=251) hospitals in Germany on April 6th, 2021. Data collection was closed at midnight on April 14th, 2021. We asked to report cases of cerebral sinus-venous thrombosis, cerebral venous thrombosis, ischemic stroke and haemorrhage in possible temporal relationship with a COVID-19 vaccination, i.e., events that had occurred within 31 days after vaccination. We also allowed reporting of patients with other neurological diagnoses. We combined cerebral sinus-venous thrombosis and cerebral venous thrombosis without involvement of the vena cerebri magna—hereafter referred to as cerebral sinus and/or venous thrombosis (CVT). Thirty-seven (92%) neurology departments at university hospitals (tertiary centres) and 75 (30%) neurology departments of non-university hospitals responded (Figure 1). We recorded information about the type of vaccination, symptoms, coagulation parameters, clinical course and clinical outcomes. We developed a written protocol for data collection (see appendix). The protocol was approved by the Ethics Committee (Vote-No. 142/21, Ethics Committee of the Medical Faculty at RWTH University). Data protection and privacy conformity has been confirmed by the Data Protection Officer and the Information Security Officer of RWTH Aachen University Hospital. Coagulation parameters were also collected form the respective local laboratories. For a subgroup of patients, anti-Heparin/Platelet Factor 4 Antibody (PF4)/polyanion-IgG EIA and a platelet activation assay were performed in the laboratory of the Institute for Immunology and Transfusion Medicine at the University of Greifswald as described12. For the PF4 antibody results, we used information from the central laboratory in Greifswald, only if missing, we considered test results if positive from the respective local hospitals.

*VITT risk score = (a) time after vaccination equals one to 16 days, (b) thrombocytopenia (<150/nl) or relative thrombocytopenia (drop of thrombocytes of at least 50%), (c) positive enzyme-linked immunosorbent assay (ELISA) to detect platelet factor 4 (PF4)-polyanion antibodies, (d) modified (PF4-enhanced) platelet-activation assay (VITT function test)
Based on the first reported cases11,12 we prespecified a grading using the following criteria in order to classify each event according to its likelihood of being anti-SARS-CoV-2 vaccination-associated. (a) time after vaccination equals one to 16 days, (b) thrombocytopenia (<150/nL) or relative thrombocytopenia (drop of thrombocytes of at least 50%), (c) positive enzyme-linked immunosorbent assay (ELISA) to detect platelet factor 4 (PF4)-polyanion antibodies, (d) positive modified (PF4-enhanced) platelet-activation assay (VITT function test)12. Each criterium loaded the score with 1 point. All cases were evaluated in depth by four members of the Task Force. Cases that fulfilled criteria a and b but no test results were available for c and d, were rated with a score of 2+ to contrast them to those cases with negative results for c and d. A score of 2+ and higher was considered a high grade (highly probable VITT).
Statistical analysis
Characteristics of the reported cases were summarized as frequency and percentage or mean, standard deviation, median, and range for qualitative and quantitative variables respectively. Descriptive statistics were reported for the overall cases and by subgroups.
In order to compute the incidence rate of cerebral events and CVT within one month from first vaccine shot administration, we divided the number of cases occurred within 31 days from first vaccine shot administration by the overall amount of person-time spent at risk during the time window of interest.
We extracted CC-BY licenced data from the Robert Koch-Institute (RKI) about the number of vaccine shots administered by calendar week, age group, vaccine type, and state separately for only females and for everyone (numbers for non-females were obtained by difference). The number of vaccine shots administered within these subgroups was only available for nine German states and no distinction was possible between first and second doses.
Therefore, we restricted our estimation of the incidence to the area of the nine German States (Baden-Württemberg, Bremen, Hamburg, Mecklenburg-Vorpommern, Niedersachsen, Nordrhein-Westfalen, Rheinland-Pfalz, Saarland, and Schleswig-Holstein). We assumed that a case originated in this area if the hospital recording it was located in one of the nine States. We only considered cases occurred within 31 days from first vaccine shot administration. For cases occurred after the second shot, we computed the time from first dose assuming that the second dose was administered 10 weeks, 21 days, 14 days after the first for ChAdOx1, BNT162b2, and mRNA-1273 respectively.
Within every strata of state, age group (<60, 60+), sex (female, non-female) and vaccine type (ChAdOx1, BNT162b2, and mRNA-1273) we approximated the number of first and second doses administered every calendar week. We assumed individuals receiving their second dose in a given week were the same who had received their first dose a fixed amount of weeks before (10 for ChAdOx1, 3 for BNT162b2, and 2 for mRNA-1273). If the number of attributed second doses in a week was higher than the registered total number of administered doses, the remaining doses were attributed to the following week (and so on, iteratively). The number of first doses was obtained by difference between the total number of doses and the estimated number of second doses administered in the week.
The number of person-years each vaccinated individual spent at risk during the time window of interest (one month from first vaccine shot administration) was computed as the number of days between the day of the first dose administration (assumed in the middle of the week) and the 31st day after the first dose administration or the end of the study period (April 15th, 2021) whichever occurred first, divided by 365.25. We only considered the time contributed by individuals who received their first dose between December 28, 2020 and April 11, 2021.
Overall and group-specific incidence rates were expressed as number of cases per 100,000 person-years and reported along with their 95% exact Poisson confidence intervals.
Our approach relies on the assumptions that no individual moved from a state-age-sex-vaccine group to another during the 31 days following first dose administration, that no competing events occurred during this time window and that everyone received a second dose of vaccine according to the above specified schedule.
Finally, we fitted a Poisson log-linear regression model to investigate the association between age group (<60, 60+), sex (female, non-female), vaccine class (ChAdOx1, mRNA-based vaccines) and the CVT incidence rate within one month from first dose administration. P-values lower than or equal to 0.05 were considered statistically significant.
All analyses were performed using R version 4.0.3 and RStudio 1.1.456.
We formulated the following a priori research hypotheses:
Vaccine-induced CVTs are restricted to SARS-CoV2 vaccination with ChAdOx1 and do not occur after vaccination with mRNA-based vaccines.
Females, particularly below the age of 60 years, are more likely to be diagnosed with vaccine-induced CVT
Patients with vaccine-induced CVT after SARS-CoV2 vaccination have a high prevalence of antibodies against thrombocytes and/or thrombocytopenia resulting in venous thrombosis and bleedings.
VITT-mediated neurological events are not restricted to vaccine-induced CVTs but may also result in cerebrovascular arterial thrombotic events.
Patient involvement
No patients were directly involved in this study.
Results
After excluding duplicates, and cases without cerebrovascular outcomes, 62 patients with a cerebral event were reported in close temporal proximity to the vaccination against COVID-19 (Figure 1). Patients had a mean age of 46.6 and 75.8% were female (Table 1). All reported cases occurred after vaccination with ChAdOx1 and BNT162b2. No cases were reported with other vaccines. We identified 8 cases with CVT after BNT162b2, 37 after ChAdOx1, and none after mRNA-1273 vaccination. No other vaccines have been administered in Germany so far. Of the 45 patients with CVT, 35 (77.8%) were female (Table 3). Thirty-six (80.0%) were below the age of 60 years (Table 3). The initial diagnosis of CVT was confirmed by MR and MR-venography or CT and CT-venography in all cases. Primary intracerebral haemorrhages (ICH) were observed in 4 (6.4%) cases and 9 (14.3%) patients had primary cerebral ischemia (Table 1). A total of 4/62 (6.5%) patients had other diagnoses (1 transient global amnesia, 1 spinal artery ischemia, and 2 nausea, one of them with headache).
Characteristics of included cases with cerebral and central nervous system events 1 to 31 days after Covid-19 vaccination (N=62).
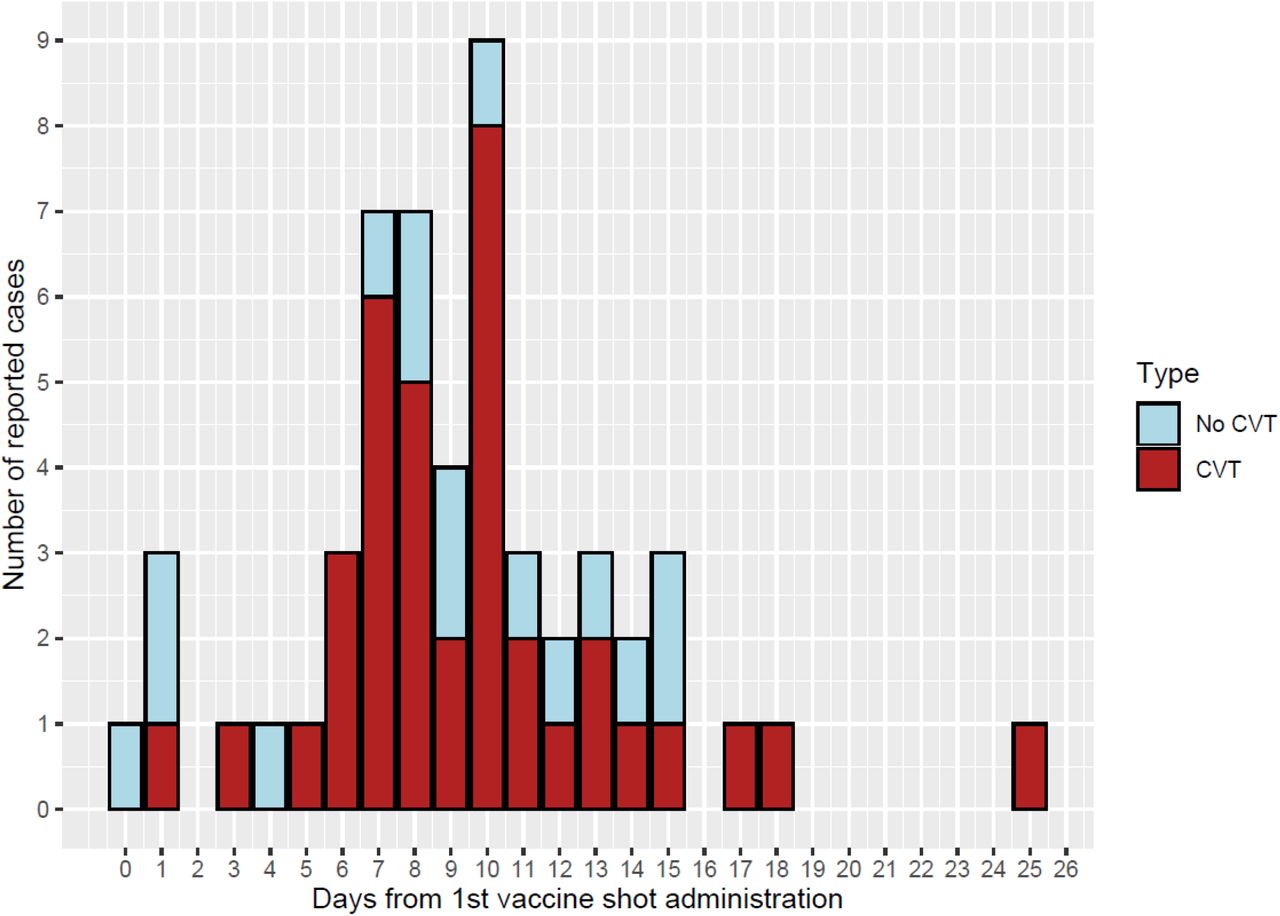
Two out of 62 patients (3.2%) presented with dermal petechia, two (3.2%) with subdermal hematoma and two (3.2%) with bleedings in other territories. A total of 59/62 (95.2%) cases occurred after the first administration of a vaccine and 3 (4.8%) after the second administration (all three BNT162b2) (Table 1). The median time interval from last administered vaccine shot to first neurological symptoms was 9 days (range 0 to 25) and for CVT events, it was 9 days (range 1 to 25 days). All cases except one experienced first neurological symptoms within 31 days (approximated value for cases occurred after BNT162b2 second shot) from the first vaccine shot administration. Days from first vaccine shot to neurological symptoms for cases occurred after ChAdOx1 are presented in Figure 2. None of the cases had a previously confirmed SARS-CoV-2-infection (Table 1). All events after ChAdOx1 occurred after the first dose, but very few people in Germany received a second dose in the study period. Three of the 9 BNT162b2 cases occurred after the second dose.

Days since first ChAdOx1 vaccination administration to symptom onset according to CVT and non-CVT events.
In total, we estimated an incidence rate within one month from first dose administration of 8.8 (95% CI, 6.4 to 11.9) cerebrovascular events per 100,000 person-years. This incidence rate was 24.6 (95% CI, 17.3 to 33.8) per 100,000 person-years for ChAdOx1, 1.6 (95% CI, 0.53 to 3.8) per 100,000 person-years for BNT162b2, and 0.00 (95% CI, 0.00 to 17.4) per 100,000 person-years for mRNA-1273. The incidence rate of cerebrovascular events within one month from first ChAdOx1 dose administration was 29.4 (95% CI, 19.8 to 42.0) per 100,000 person-years for females and 14.4 (95% CI, 5.8 to 29.6) for non-females.
In total, we estimated an incidence rate within one month from first dose administration of 6.5 (95% CI, 4.4 to 9.2) CVT per 100,000 person-years. This incidence rate was 17.9 (95% CI, 11.8 to 26.1) per 100,000 person-years for ChAdOx1, 1.3 (95% CI, 0.4 to 3.4) per 100,000 person-years for BNT162b2, and 0.0 (95% CI, 0.0 to 17.4) per 100,000 person-years for mRNA-1273. The incidence rate of CVT within one month from first ChAdOx1 dose administration was 23.5 (95% CI, 15.1 to 35.0) per 100.000 person-years for females and 6.2 (95% CI, 1.3 to 18.0) per 100,000 person-years for non-females. Incidence rates by age group, sex and vaccine are reported in Table 2 and Figure 3.
Incidence rates of CVT within one month (31 days) of first dose Covid-19 vaccine administration according to age group, sex and vaccine using data from nine States in Germany.

{kind=link}
{kind=link}
{kind=link}
Incidence (95% confidence intervals) of cerebro-vascular events (A) and CVT (B) within one month (31 days) from first dose administration of vaccine against SARS-CoV-2 by vaccine type, sex, and age group.
In the model for CVT incidence within one month from first dose administration jointly considering age group, vaccine class and sex, we estimated an adjusted incidence rate ratio of 9.68 (95% CI: 3.46 to 34.98, P <0.001) for ChAdOx1 compared to mRNA-based vaccine, 3.14 (95% CI: 1.22 to 10.65, P=0.03) for females compared to non-females, and 2.14 (95% CI: 0.83 to 6.78, P=0.15) for those aged <60 compared with those aged 60 or more.
With the pre-specified VITT risk grading we qualitatively investigated the adherence of the reported cerebrovascular events with the recently described syndrome of a vaccine-induced immunological syndrome leading to thrombocytopenia followed by thrombotic events (Table 3). Overall, 4/62 (6.5%) had a risk score of 0, 24 (38.7%) had 1, 1 (1.6%) had 2, 5 (8.1%) had 2+, 4 (6.5%) had 3, and 24 (38.7%) had a score of 4. In patients with CVT, 20/45 (44.4%) scored 4 points, fulfilling all pre-defined criteria for likelihood of vaccine association (Figure 1).
Risk grading of VITT-associated cerebrovascular events
In 3 patients PF4 antibodies were positive, but the VITT function test was negative. All 28 patients with positive PF4 antibodies had received ChAdOx1 in between 3 and 15 days before neurological symptoms. None of the CVT patients who had received BNT162b2 had positive PF4 antibodies or a positive VITT function test (but only 2 out of 8 cases had values). None had an isolated thrombocytopenia and one presented with a pre-existing pancytopenia unrelated to the vaccination.
In addition to the CVT patients, 9 cases with ischemic stroke were reported in this survey, eight of whom had received ChAdOx1 (88.9%) and one BNT162b2 (11.1%). Three of the ChAdOx1-vaccinated patients fulfilled all 4 criteria for VITT. In one patient, whose condition we also considered to be highly likely associated with the vaccination, PF4 antibodies were positive but the VITT function tests negative. Ischemic stroke was reported in an 82-year-old patient 2 days after the first BNT162b2 dose administration but without thrombocytopenia and missing results for PF4 antibodies of the VITT function test.
Four patients with a primary intracerebral bleeding without imaging signs of CVT were reported, all after ChAdOx1 vaccination. One patient fulfilled all four pre-defined criteria for a VITT-mediated event. Another case was considered highly likely because of thrombocytopenia and temporal association with the vaccination but in the absence of PF4 antibody and VITT function testing. In the remaining two patients, the clinical events were not considered to be associated with the vaccination. Table 3 summarizes the association of the risk score and the type of vaccinations.
Coagulation parameters, genetic status and antibody status of PF4 are shown in Table 4. 32/59 (54.2%) patients had thrombocytopenia below 150 /nL or a drop higher than 50% and 29/42 (69.0%) patients and elevated D-dimer levels above 500 µg/L. Eleven patients out of 60 (18.0%) died, of whom 9 had been vaccinated with ChAdOx1 and two had been vaccinated with BNT162b2. The distribution of the last available score on the modified Rankin scale (at discharge, death or last available information if still hospitalized) is presented in Table 5. Treatment was performed in 2 (3.3%) patients with plasmapheresis, 20 (32.8%) with intravenous high dose immunoglobulins and 4 (6.6%) with corticosteroids (Table 3). Anticoagulation was provided with heparin in 12 (19.7%), fraxiparin in 1 (1.6%), argatroban 18 (29.5%), vitamin-K-antagonist 6 (9.8%), and direct oral anticoagulants 9 patients (14.8%).
Laboratory values according to event and Risk grade status (N=62)
Associated factors, treatment and outcome (N=62)
Discussion
Our descriptive study from Germany identified 62 vascular cerebrovascular adverse events in close temporal relationship with a COVID-19 vaccination, of which 45 cases were CVT. Eleven patients died. We estimated an incidence rate of CVT within one month from first dose administration of 17.9 per 100,000 person-years for ChAdOx1 vaccine and 1.3 per 100,000 person-for BNT162b2. Before the COVID-19 pandemic, the incidence rate of CVT has been estimated between 0.22 – 1.75 per 100,000 person-years in four European countries, Australia, Iran and Hong Kong6–8. This corresponds to an over 10-fold higher CVT incidence rate in patients who received a first ChAdOx1 vaccine shot compared with the highest estimate of CVT incidence rate from empirical data. The incidence rate of a CVT event after first dose COVID-19 vaccination was statistically significantly increased for ChAdOx1 (9.68, 3.46 to 34.98) compared to mRNA-based vaccines and for females (3.14, 1.22 to 10.65) compared to non-females. Age group had no statistically significant association with CVT incidence after accounting for sex and vaccine class.
Comparisons with other countries and settings are challenging, as the probability of receiving a specific vaccination differs by age, sex, profession and other factors. The number of people diagnosed in the UK with cerebral venous thrombosis after receiving the Astra Zeneca COVID-19 vaccine was reported as 22 cases among 18 million people having received the vaccine (https://www.gov.uk/government/publications/). However, there are also reports from the UK of 79 cases until the end of March 2021 and in 19 patients with a fatal outcome (https://www.bbc.com/news/health-56674796).
CVT is a very rare disease and it is unlikely that the higher incidence rate among vaccinated is purely the product of chance. The identification of antibodies against thrombocytes in a high percentage of our patients in whom the test results were available is another strong argument for a causal relationship. Understandably, the recommended treatment of CVT beyond anticoagulation is the use of IVIG or plasmapheresis.
Our cases of cerebrovascular events also included 5 patients with embolic ischemic stroke and a VITT score of >2 without signs of CVT. In four of them, a thrombotic occlusion of the middle cerebral artery, the internal carotid artery and/or recurrent thrombotic material in duplex ultrasound were reported. This is similar to Heparin-induced thrombopenia, in which arterial thrombosis occurs, as well, and at a ratio of 1:4.3 compared with venous thrombosis16.
In addition, two primary intracranial haemorrhages with a VITT risk score >2 without a detectable sign of CVT were reported.
The conclusions with respect to our hypotheses are as follows:
Individuals in Germany were vaccinated with ChAdOx1, mRNA-1273 and BNT162b2. In our study, CVTs with a VITT risk score >2 only occurred after vaccination with ChAdOx1. Our results suggest that VITT-induced antibodies against PF4 do not cross-react with the spike protein of SARS-CoV-217. A recent report of an individual who developed a CVT associated with a severe thrombopenia at 14 days after immunization with Ad26.COV2.S suggests that VITT-associated thrombotic events may be associated with adenovirus vector-based vaccines directed against the SARS-CoV-2 spike protein18. Since ChAdOx1 is based on a chimpanzee and Ad26.COV2.S vaccine on a human adenovirus vector and they differ in their spike protein inserts, there was hope that a VITT is restricted to ChAdOx1.
We confirm that CVT within one month from first dose administration occur at an higher rate in females compared to non-female, accounting for age group and vaccine class. Indeed, the adjusted rate ratio is equal to 3.1 (95% CI: 1.2 – 10.6). However, the rate of CVT occurring within one month from first dose administration, once accounted for sex and vaccine class, did not significantly differ (p-value=0.15) between individuals younger than 60 years and individuals that are 60 years or older Figure 4).
We confirm that most of the patients with a CVT at one to 16 days after vaccination with ChAdOx1, who in addition have thrombocytopenia, also have VITT
VITT-mediated cerebral vascular events (VITT risk score >2) were not restricted to CVT but were also observed in cases of primary cerebral ischemia (n=5) and intracerebral hemorrhage (n=2).
Currently, several questions remain unanswered. It is unclear how many patients develop antibodies against PF4 after vaccination with ChAdOx1 (and potentially Ad26.COV2.S) without thrombotic complications. Therefore, the risk of re-exposure to the vaccine in conjunction with the second vaccination cannot be estimated.
Although the platelet activation of VITT is heparin-independent, it is unknown whether heparin therapy aggravates VITT in analogy to the clinical syndrome of autoimmune heparin-induced thrombocytopenia. Hence, non-heparin anticoagulants are recommended for the treatment of VITT-related CVT.
Although venous and less common arterial thromboses also have been reported to occur outside the central nervous system in VITT11,17, it remains open, why vessels of the central nervous system are primarily affected.
Our data cannot serve, and should not be interpreted, as a recommendation for the vaccination strategy to be implemented. While we believe this article provides crucial information to inform such decision, we only quantified the incidence of cerebrovascular events following vaccination by sex, age group and vaccine type in nine German states. The decision on which vaccination strategy is the best in a specific context is something that depends not only on the risks of the vaccination but also on its benefits, with respect to the possible alternative strategies. Specifically, it needs to be emphasized that VITT is a very rare event and that the risk-benefit ratio of a vaccination against SARS-CoV-2 needs to be taken into account. Other factors to be considered for estimating an overall risk-benefit ratio include the risk of cerebral blood clots from Covid-19 disease19,20, the existence and availability of alternative vaccines.
Strengths of our study include the standardized collection of patients’ data with cerebral outcomes within a reasonable time period after SARS-CoV-2 vaccination from almost all Departments of Neurology of German university hospitals (which represent the tertiary care hospitals in Germany). Each case was evaluated by four neurologists and one coagulation specialist who discussed all aspects of the provided clinical information. To approximate the incidences, we used official data of vaccinated people in Germany and had information on the age, sex and vaccine type distribution from 9 of the 16 States in Germany.
Limitations of our study include that we only collected information from neurological departments and patients may have been treated at other departments or died without reaching a hospital. We could not collect the brain imaging data to validate the diagnosis of CVT and other cerebral events. Due to public discussions specifically around CVT as a consequence of the ChAdOx1 vaccine, a certain overreporting is possible. We assume that neurologists in Germany would be more aware of cases with CVT after vaccination than of ischemic stroke or cerebral haemorrhage, which may result in underreporting of the latter. We did not have data on the age, sex and vaccine type distribution of vaccinated people from entire Germany but only from 9 states. In the RKI dataset, the vaccine shots administered by general practitioners are not included, probably leading to an overestimation of the true risk. Furthermore, we had to compute the overall amount of person-years spent at risk by subgroup relying on a crude approximation of the number of first doses administered. Lastly, we cannot exclude in this retrospective survey that some transferred data were misclassified or differentially missing. Two of the cases included in this report were also presented in the first description of VITT by Greinacher and colleagues12
Implications
Findings of our study imply further careful considerations in the administration of ChAdOx1 especially for women and risk-benefit considerations when considering this vector-based vaccination by age. Continued registration of all cerebrovascular events after vaccination and all rare cerebral venous thromboses in a standardized and validated manner is important in properly evaluating the risk of these events after Covid-19 vaccination.
Funding
There was no specific funding for this study.
The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Conflict of interests
All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare the following competing interests:
JBS reports (outside the present study) honoraria from advisory boards or oral presentations by Biogen, Novartis and Grifols. He receives grants from the German Research Council (DFG), the German Ministry of Education and Research (BMBF), and the European Commission.
PB serves as Editor in chief for DGNeurologie.
HCD reports outside of the present study: received honoraria for participation in clinical trials, contribution to advisory boards or oral presentations from: Abbott, BMS, Boehringer Ingelheim, Daiichi-Sankyo, Novo-Nordisk, Pfizer, Portola and WebMD
Global. Financial support for research projects was provided by Boehringer Ingelheim. HCD received research grants from the German Research Council (DFG), German Ministry of Education and Research (BMBF), European Union, NIH, Bertelsmann Foundation and Heinz-Nixdorf Foundation. HCD serves as editor of Neurologie up2date, Info Neurologie & Psychiatrie, Arzneimitteltherapie, as co-editor of Cephalalgia and on the editorial board of Lancet Neurology. HCD chairs the Treatment Guidelines Committee of the German Society of Neurology and contributed to the EHRA and ESC guidelines for the treatment of AF.
CG received (outside the submitted work) funding from German Research Council (DFG), European Union, Federal Ministery of Education and Research (BMBF), German Statutory Pension Insurance Scheme (RV Nord), National Innovation Fond, Wegener Foundation, and Schilling Foundation. CG reports (outside the submitted work) personal fees from Amgen, Boehringer Ingelheim, Daiichi Sankyo, Abbott, Prediction Biosciences, Novartis, and Bayer.
AG reports grants from Deutsche Forschungsgemeinschaft, personal fees and non-financial support from Aspen, grants from Ergomed, grants and non-financial support from Boehringer Ingelheim, personal fees from Bayer Vital, grants from Rovi, grants from Sagent, personal fees from Chromatec, personal fees and nonfinancial support from Instrumentation Laboratory, grants and personal fees from Macopharma, grants from Portola, grants from Biokit, personal fees from Sanofi-Aventis, grants from Fa. Blau Farmaceutics, grants from Prosensa/Biomarin, grants and other from DRK-BSD NSTOB, grants from DRK-BSD Baden-Wuertemberg/Hessen, personal fees and non-financial support from Roche, personal fees from GTH e.V., grants from Deutsche Forschungsgemeinschaft, outside the submitted work. In addition, AG reports having a patent, Application no. 2021032220550000DE, pending.
CK serves as a medical advisor on genetic testing reports to Centogene and on the scientific advisory board of Retromer Therapeutics.
SP received (all outside the submitted work) research grants from BMS/Pfizer, Daiichi Sankyo, European Union, German Federal Joint Committee Innovation Fund, and German Federal Ministry of Education and Research, and speakers honoraria/consulting fees from AstraZeneca, Bayer, Boehringer-Ingelheim, BMS/Pfizer, Daiichi Sankyo, Portola, and Werfen.
MP reports being partially funded by a research grant from Novartis Pharma for a self-initiated research project, unrelated to this work, on migraine remission. MP further reports being awarded a research grant from the Center for Stroke Research Berlin (private donations) for a self-initiated project, unrelated to this work, on causal diagrams.
TK reports outside of the submitted work to have received research funds from the Germain Joint Committee and the German Ministry of Health; he has received personal compensation from Eli Lilly & Company, Teva, Total S.E. and the BMJ.
RR reports outside of the submitted work to have received research funds from the German Ministry of Education and Research, German Joint Committee (GBA) and the German Ministry of Health.
HS reports outside of the submitted work to have received speaker’s honoraria from Bayer, Boehringer Ingelheim, and Teva.
TT reports grants from Deutsche Forschungsgemeinschaft, during the conduct of the study; personal fees and other from Bristol Myers Squibb, personal fees and other from Pfizer, personal fees from Bayer, personal fees and other from Chugai Pharma, other from Novo Nordisk, personal fees from Novartis, other from Daichii Sankyo, outside the submitted work.
Data sharing
Due to the votes that we received for ethics and data protection and privacy conformity for this survey, we will not be able to share data that contain information about the center, the age and the sex of the patient.
Dissemination
Upon request, the data will be available for policy makers and government bodies. The guarantor (JS) affirm that the manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as originally planned (and, if relevant, registered) have been explained.
DGN Covid-19 Vaccination Study Group
Prof. Dr. Angelika Alonso, Medizinische Fakultät Mannheim, Universität Heidelberg;
Prof. Dr. Thorsten Bartsch, Klinik für Neurologie, Universitätsklinikum Schleswig-Holstein Kiel
Dr. med. Felix Bode, Klinik für Neurologie, Uniklinik Bonn
Dr. Hakan Cangür, Neurologische Klinik, Klinikum Wolfsburg
Prof. Michael Daffertshofer, Neurologie, Klinikum Mittelbaden, Rastatt
PD Dr. med. Manuel Dafotakis, Neurologische Klinik, Uniklinik, RWTH Aachen
Prof. Dr. med. Marianne Dieterich, LMU München, Klinik für Neurologie
PD Dr. med. Ralf Dittrich Niels, Stensen Kliniken, Marienhospital Osnabrück, Klinik für Neurologie
Dr. Friederike Fabian, Neurologie, Marienhospital, Stuttgart
Dr. med. Mathias Fousse, Uniklinik des Saarlandes, Abteilung für Neurologie
Dr. Jana Godau, Klinikum Kassel, Neurologische Klinik
Prof. Dr. Martin Grond, Kreisklinikum Siegen, Klinik für Neurologie
Dr. med. Albrecht Günther, Hans-Berger-Klinik für Neurologie, Universitätsklinikum Jena, Am Klinikum 1, 07747 Jena
Prof. Dr. med. Alexander Gutschalk, Neurologische Klinik, Universitätsklinikum Heidelberg
Prof. Dr. med. Georg Hagemann, Helios Klinikum Berlin-Buch, Klinik für Neurologie; Dr. med. Corinna Hartmann, Helios Klinik Lengerich
Prof. Rüdiger Hilker-Roggendorf, Knappschaftskrankenhaus Recklinghausen, Klinik für Neurologie
Prof. Dr. med. Günter Höglinger, Klinik für Neurologie, Medizinische Hochschule Hannover
Dr. Benno Ikenberg; Neurologische Klinik, Klinikum rechts der Isar der TU München)
Dr. med. Fatme Seval Ismail, Department of Neurology, University Hospital Knappschaftskrankenhaus Bochum, Ruhr University Bochum, Germany
PD Dr. med. Sarah Jesse, Ulm University, Department of Neurology, Oberer Eselsberg 45, 89081 Ulm
PD Dr. Bernd Kallmünzer, Neurologische Universitätsklinik Erlangen.
Prof. Dr. med. Rolf Kern, Klinik für Neurologie, Klinikverbund Allgäu
Dr. med. Martin Klietz, Klinik für Neurologie, Medizinische Hochschule Hannover Dr. med. Samuel Knauß, Klinik für Neurologie, Charité, Berlin
PD Dr. med. Benjamin Knier, Neurologische Klinik, Klinikum rechts der Isar, Technische Universität München, München, Deutschland
Prof. Dr. Volker Limmroth, Neurologische Klinik, Kliniken der Stadt Köln
Dr. med. Annerose Mengel, Department of Neurology and Stroke, Universitätsklinikum Tübingen
Dr. Johannes Meyne, UKSH, Campus Kiel, Klinik für Neurologie Dr. med. Martin Morgenthaler, Westpfalz-Klinikum GmbH
Dr. med. Matthias Müller, Abteilung für Neurologie, AK Nord Heidberg
Prof. Dr. med. Simon Nagel, Neurologische Klinik, Universitätsklinikum Heidelberg
PD Dr. Oezguer A. Onur, University of Cologne, Faculty of Medicine and University Hospital Cologne, Department of Neurology, 50937 Cologne, Germany
Dr. med. Johann Pelz, Klinik und Poliklinik für Neurologie, Universitätsklinikum Leipzig, Leipzig
Dr. Johannes Plenge, USKH, Klinik für Neurologie PD Dr. Sven Poli, Universitätsklinikum Tübingen
Dr. med. Christian Roth, Neurologie, DRK-Kliniken Nordhessen, Kassel
Prof. Dr. med. Joachim Röther, Asklepios Klinik Altona
Dr. med. Christian Saß, Asklepios Klinikum Harburg, Neurologie
PD Dr. med. Silvia Schönenberger, Neurologische Klinik, Universitätsklinikum Heidelberg
Dr. med. Roger Schubert, Klinik für Neurologie, SRH-Waldklinikum Gera
Dr. med. Ole Simon, Universitätsklinikum Gießen und Marburg, Standort Marburg Ina Specht, Agaplesion Diakonieklinikum Rotenburg, Neurologische Klinik
Dr. Anne Sperfeld, Neurologische Klinik Altscherbitz, Schkeuditz PD Dr. Annette Spreer, Klinikum Braunschweig
Prof. Dr. med. Andreas Steinbrecher; Klinik für Neurologie, Helios Klinikum Erfurt Dr. med. Jochen Steiner, Universitätsklinikum Tübingen;
Dr. Henning Stetefeld, Uniklinik Köln der Universität zu Köln
Prof. Dr. George Trendelenburg, Klinikum Itzehoe & Universitätsmedizin Göttingen Dr. med. Nils Bijan Vatankhah, Diako Flensburg;
Dr. med. Christoph Michael Wahl; Neurologie, Klinikum Kempten
Dr. med. Katja Wartenberg, Klinik und Poliklinik für Neurologie, Universitätsklinikum Leipzig, Leipzig
Prof. Dr. med. Karsten Witt, Dept. of Neurology and Center of Neurosensory Sciences, University Oldenburg, Germany
PD Dr. med. Matthias Wittstock, Klinik und Poliklinik für Neurologie, Universitätsmedizin Rostock
Dr. med. Björn Wolf
PD Dr. Joachim Wolf, Diakonissenkrankenhaus Mannheim
Dr. med. Julian, Zimmermann, Uniklinik Bonn Klinik für Neurologie
Acknowledgments
We thank the Robert Koch-Institute for providing data on administered vaccine shots in Germany.
Footnotes
↵* Members of the Study Group, see appendix
References



