
ABSTRACT
Background Immunization against COVID-19 in Brazil started in January 2021, with health workers and the elderly as the priority groups. We assessed whether there was an impact of immunizations on the mortality of individuals aged 80+ years.
Methods By April 22, 2021, 147,454 COVID-19 deaths had been reported to the Brazilian Mortality Information System. Denominators for mortality rates were calculated by correcting population estimates for all-cause deaths reported in 2020. Proportionate mortality at ages 80+ and 90+ years relative to deaths at all ages were calculated, and mortality rate ratios compared these two age groups with individuals aged 0-79 years. Vaccine coverage data were obtained from the Ministry of Health vaccination monitoring website. All results were tabulated by two-week periods from epidemiological weeks 1-14, 2021.
Findings As the P.1 variant spread throughout Brazil, the total number of deaths increased over time starting in epidemiological week 9 of 2021. The proportion of all deaths occurring at ages 80+ years was over 25% in weeks 1-6 and declined rapidly to 13.1% in weeks 13-14. Mortality rates were over 13 times higher in the 80+ years age group compared to that of 0-79 year olds up to week 6, and declined to 6.9 times in weeks 13-14. Coronavac accounted for 77.3% and AstraZeneca for 15.9% of all doses administered. Vaccination coverage (first dose) increased rapidly among individuals aged 80+ years, reaching 49.1% in weeks 5-6 and over 90% after week 9.
Interpretation Rapid scaling up of vaccination coverage among elderly Brazilians was associated with an important decline in relative mortality compared to younger individuals, in a setting where the P.1 variant predominates. Had mortality rates among the elderly remained proportionate to what was observed up to week 6, an estimated additional 13,824 deaths would have been expected up to week 14.
Introduction
In early 2021, Brazil became the global epicenter of the COVID-19 pandemic 1 with an average of over 2,000 daily deaths in the month of March.2 The P.1 variant, initially identified in Manaus in late 2020 3 has rapidly spread throughout the country. Although genomic analyses are infrequent, by early March the new variant accounted for over half of all cases in eight out of ten states with data on viral sequencing.4
Immunization against COVID-19 was started in late January 2021, with two types of vaccines being offered: Coronavac (Sinovac, China) and AZD1222 (Oxford-AstraZeneca, UK). Vaccination has been initially targeted at four priority groups: health workers, the elderly (starting with those aged 85 years or more, and gradually vaccinating younger age groups), indigenous populations, and institutionalized individuals. By April 22, 17.4% of the population had received the first dose, and 7.1% the second dose,5 Coronavac accounted so far for 77.3% and AstraZeneca for 15.9% of all doses delivered.6
Vaccination campaigns have been associated with reductions in hospital admissions and mortality among targeted population groups, in several of the early starting countries.7-9 Yet, there is limited evidence on the efficacy of the two vaccines being delivered in Brazil against the P.1 variant that currently accounts for the majority of cases in the country. Two observational studies among health care workers in Manaus10 and São Paulo11 suggested that the Coronavac provided partial protection against symptomatic illness in settings where P.1 accounted for 75% and 47% of all infections, respectively, at the time of the study. Yet, there is growing concern that high SARS-CoV-2 incidence rates such as those observed in Brazil in early 2021 will lead to the appearance of new variants of concern as well as increase in the risk of vaccine escape.12.
To evaluate the real-life effectiveness of the vaccination campaign in Brazil, we analyzed time trends in mortality due to COVID-19 using a database of over 370,000 registered deaths. We hypothesized that mortality would fall more rapidly among the elderly, who were the initial target group of the vaccination campaign, than among younger Brazilians.
Methods
Data on COVID-19 deaths were obtained from the Ministry of Health Mortality Information System13 including deaths reported until April 22, 2021. Coverage of the death registration system has been estimated at over 95% by 2010.14 As of 2016, the Global Burden of Disease project assigned four out of five stars for the system’s coverage and quality of cause of death ascertainment 15, and by 2019 5.6% of all deaths were coded as due to ill-defined causes (França GA, unpublished data). We analyzed deaths for which the underlying cause was coded as B34.2, which included codes U07.1 (COVID-19, virus identified) and U07.2 (COVID-19, virus not identified.16 Since early 2020, 377,124 deaths due to COVID-19 were reported in the system, of which 171,454 in 2021. For 84% of 2021 deaths, presence of the virus was confirmed in a laboratory (preliminary results based on investigation of 163,637 deaths).
Data on COVID-19 immunization coverage were obtained from a dataset made available by the Brazilian Ministry of Health.17 The data are updated daily and consist of an individual level dataset including personal information (date of birth, sex, skin color, city of residence), and information on the vaccination (local, type of facility, vaccine producer and lot number) along with whether it is the first or second dose received and the priority group for the person vaccinated. The data used here was from 19 April 2021.
Population estimates for July 1st by single age and sex were obtained from the Brazilian Institute for Geography and Statistics 18. Due to the excess mortality observed in 2020 and the higher COVID-19 mortality among the elderly 19, the population numbers from IBGE for 2020 are overestimated, particularly at older ages. Since vaccination started in Brazil in early January 2021, it is imperative to obtain an adjusted estimated population that more closely reflects the Brazilian population by the end of 2020. We considered the total deaths that were reported in 2020 (for all causes, as reported in the Mortality Information System), and the expected deaths as implied in the IBGE estimates. We excluded the additional number of deaths from the initial 2020 estimates and used that adjusted population as the denominator in our analyses. All adjustments were made by age and sex. All calculations were done in R (R core team, 2020).
Mortality results were analyzed in two ways. First, we calculated the proportionate mortality by dividing the number of COVID-19 deaths in a given age range by the number of COVID-19 deaths at all ages over two-weekly periods in 2020. We opted to use two-weeks instead of single weeks to reduce variability. Second, we calculated COVID-19 mortality rates by age (in decades) and sex using data from the Mortality Information System and the adjusted population by age group described above. Mortality rates at ages 80+ and 90+ years were then divided by rates for the age range 0-79 years, resulting in mortality rate ratios.
Formal statistical tests were not performed as all results are based on the full country population, rather than samples. Analyses were carried out using Stata version 16 (StataCorp, College Station, TX, USA). All analyses were based on publicly available, anonymized databases.
Results
From the beginning of the first epidemiological week in 2021 (January 3) to April 22, 171,517 deaths in the Mortality Information System were assigned to COVID-19. Table 1 shows the absolute number of deaths for each two-week period during 2021. There is a clear acceleration in deaths from week 9 (early March) when the P.1 variant became the dominant strain. Results for weeks 13-14 are likely affected by registration delay but remain useful for comparing proportionate mortality by age. Table 1 does not include deaths occurring after April 10 (end of epidemiological week 14), as these are affected by delay.
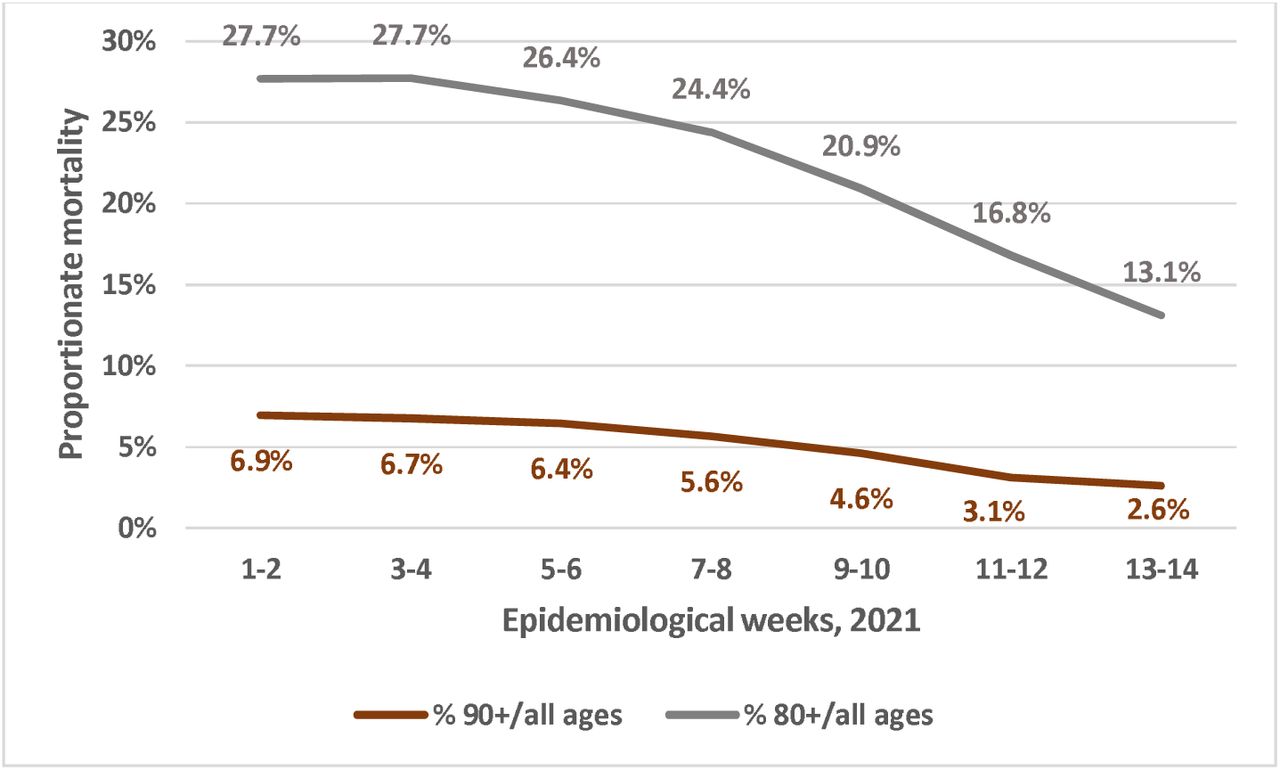
Figure 1 shows that proportionate mortality of individuals aged 90+ years fell rapidly from week 9 onwards, a trend that was also observed for subjects aged 80+ years. Up to April 22, an additional 11,195 deaths had been reported for epidemiological weeks 15 and 16, of which 11.8% were among individuals aged 80+, a finding that is consistent with a continued declining trend in proportionate mortality as shown in Figure 1.
The downturn in proportionate mortality started in weeks 7-8 of 2021. Had the number of deaths among individuals aged 80+ years continued to increase at the same rate as deaths among younger people, one would expect 47,992 such deaths during the eight-week period from mid-Feb to mid-April. Yet, 34,168 deaths were reported, or 13,824 fewer than expected under the scenario of similar trends for all age groups.
Supplementary Figure 1 shows that throughout the first year of the pandemic, proportionate mortality at ages 80+ remained between 25% and 30%, with a sharp reduction starting in mid-February 2021.

Supplementary Figure 2 shows that the decline in proportionate mortality was observed for men and women, although at every point in time proportionate mortality was higher among women, likely due to fewer deaths in mid-adulthood.

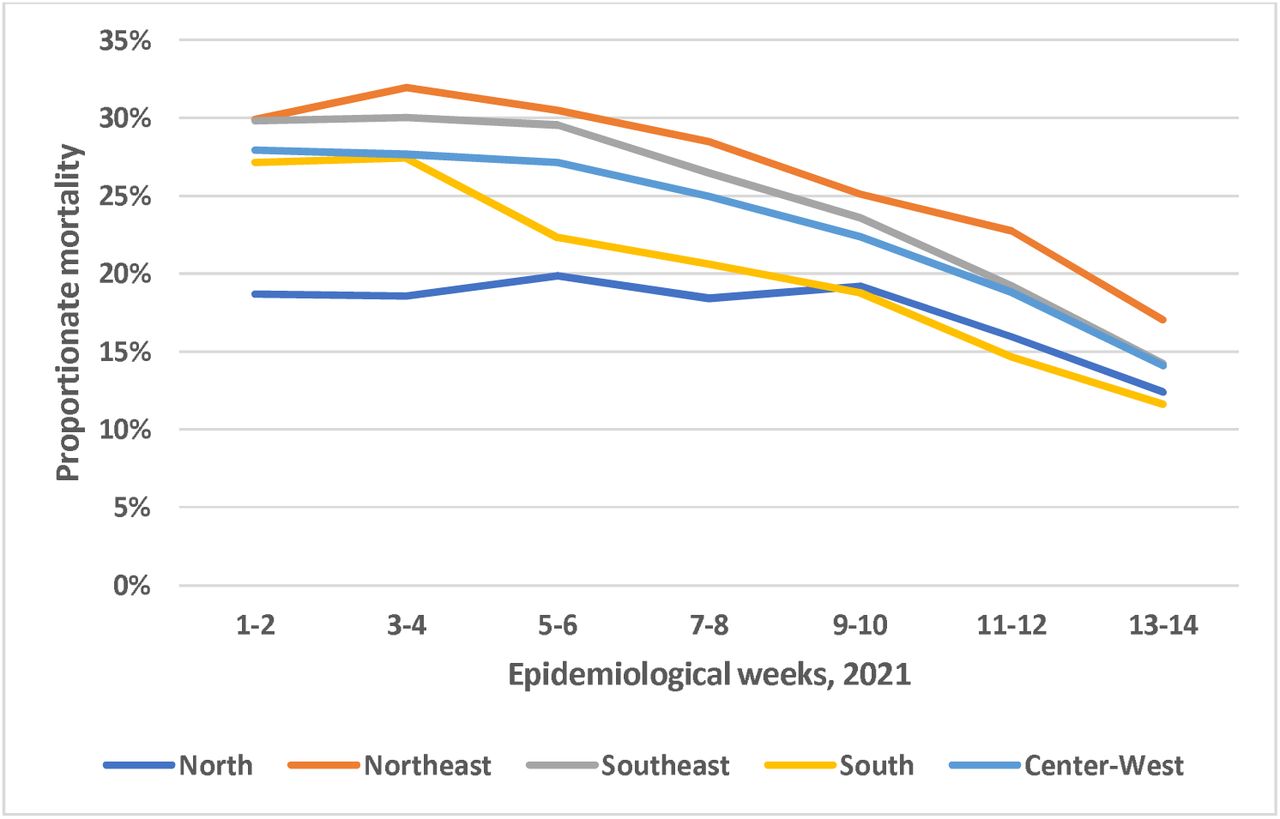
Figure 2 shows that proportionate mortality at ages 80+ years fell in all regions of the country. The trend was less marked in the North region (where the Amazon is located) than in the rest of the country.
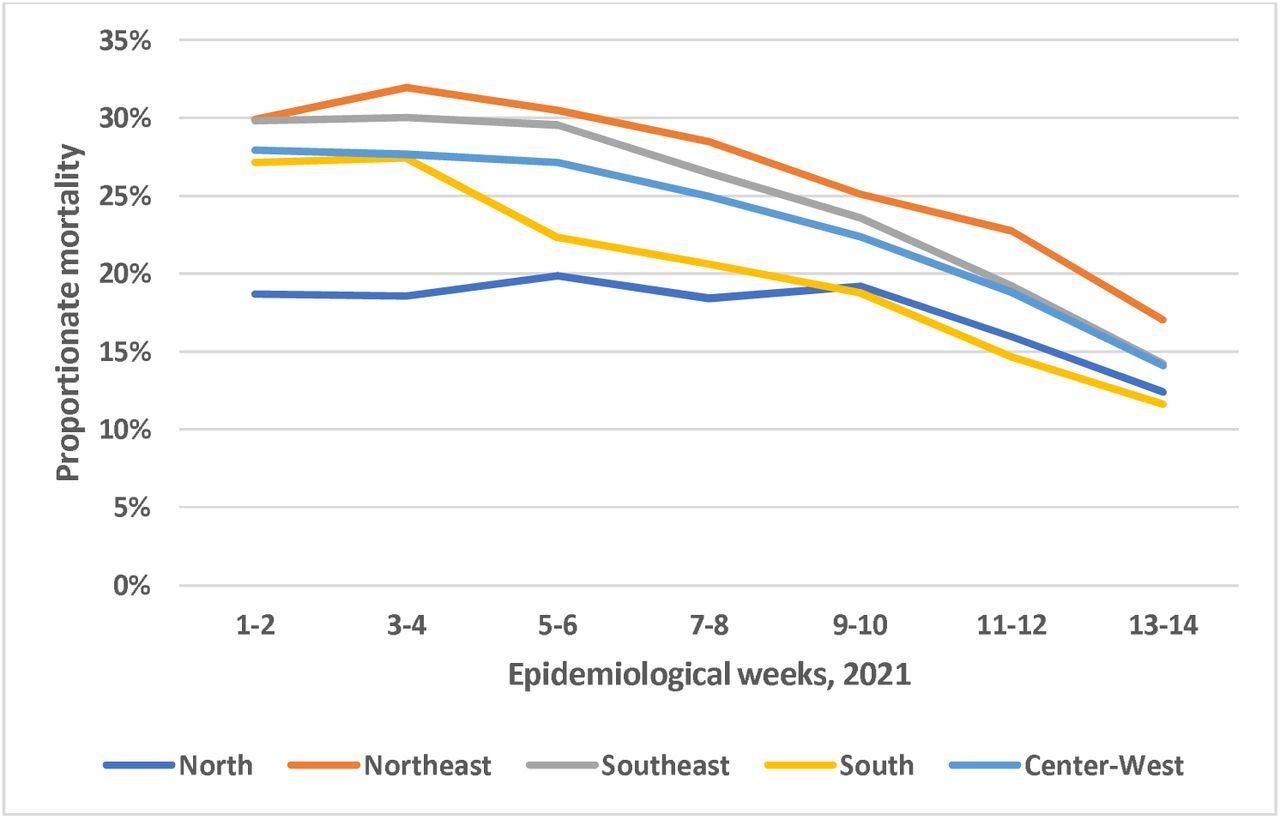
Figure 3 shows time trends in mortality rate ratios using the age group 0-79 years as the reference. During January, the mortality rate of persons aged 90+ years was 20 times higher than in the reference group, but from February onwards the ratio started declining rapidly to reach 7.7 in weeks 13-14. Partial data from weeks 15 and 16 show a ratio of 7.1, thus suggesting that the decline continues. A similar decline over time was observed for the mortality rate ratio for persons aged 80+ years, from over 13.3 in January and early February to 6.9 in weeks 13-14 and 5.8 in week 15 (partial data).

Figure 4 shows vaccine coverage by age groups over time. The increase in vaccine coverage was consistent with prioritization of older population groups, with 50% coverage reached in the first half of February and over 80% by the second half, stabilizing at around 95% in March. Coverage among younger age groups was largely restricted to health workers, indigenous peoples, and people living in institutions, who were also prioritized. Supplementary Figure 3 shows more details of how coverage increased by age group among individuals over 60 years of age. Men and women had similar coverage levels at older ages (Supplementary Figure 4), but women aged under 60 years had higher coverage than men, as they account for most health sector workers.

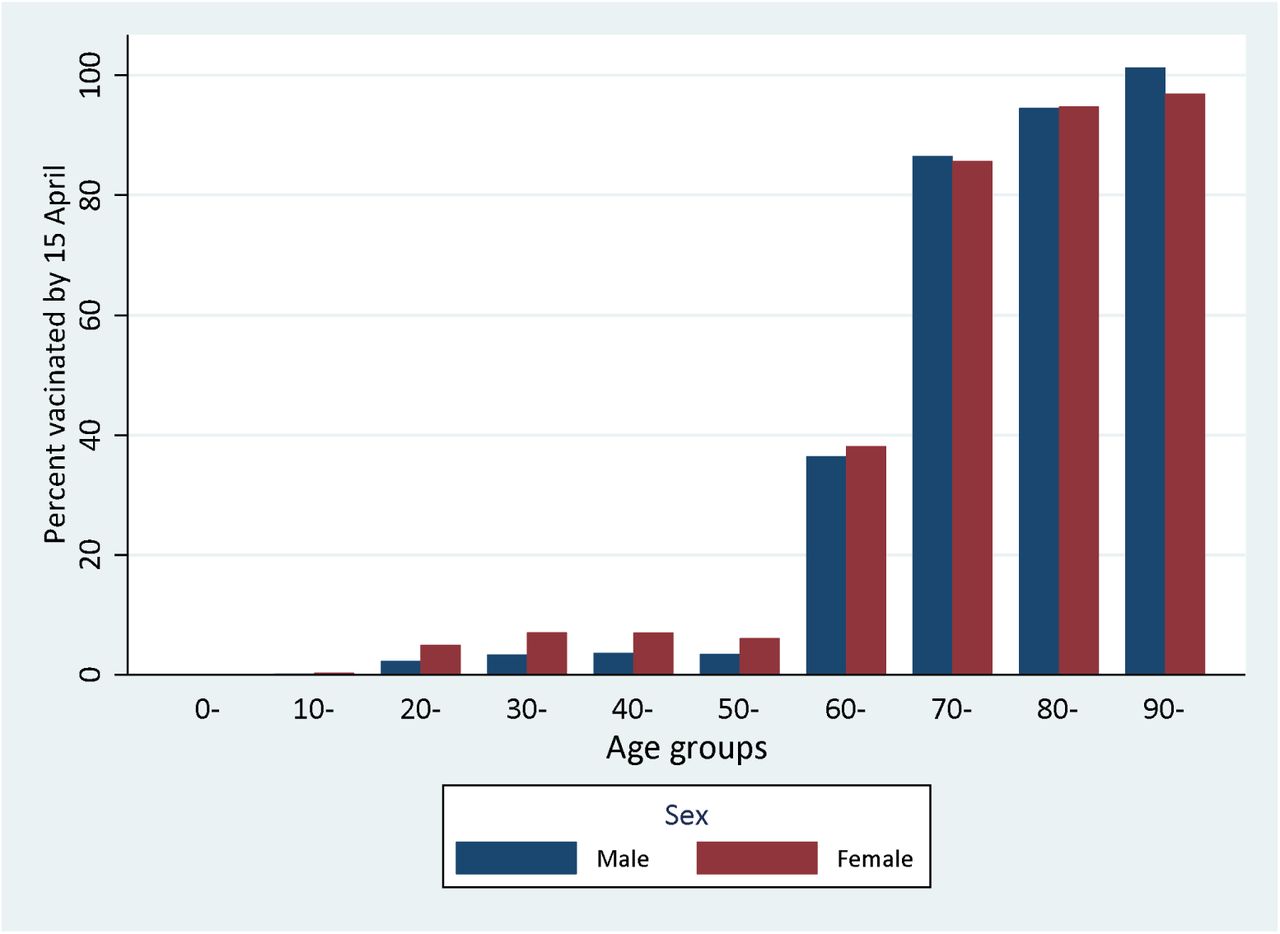
Note: vaccine coverage in males aged 90+ years apparently exceeds 100%; this is likely due to inaccuracy in the population estimate for this group

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Discussion
We found evidence that, although dissemination of the P.1 variant led to increases in reported COVID-19 death at all ages, the proportion of deaths among the elderly started to fall rapidly from the second half of February 2021. This proportion had been stable at around 25%-30% since the beginning of the epidemic in early 2020, but is now below 15% in April 2021.
Estimates of proportionate mortality must be interpreted with caution. We now describe how we handled potential caveats in these analyses.
First, the absolute number of deaths in the elderly may be reduced due to smaller number of persons at risk, resulting from high mortality in 2020 due to COVID-19 and other causes. In an estimated population of approximately 815 thousand Brazilians aged 90+ years in 2020, there were approximately 144 thousand deaths in the calendar year, of which about 10% were reported as being caused by COVID-19. To address this potential caveat, our calculations of mortality rates for 2021 were based on population estimates at the beginning of the year from which all-cause deaths had already been deducted.
Second, proportionate mortality may be spuriously reduced among the elderly if the P.1 variant of concern disproportionally affected younger individuals, either in terms of infection rates or of infection-fatality rates. The EPICOVID-19 study has been monitoring prevalence of antibodies against SARS-CoV-2 through household surveys in nine large cities in the state of Rio Grande do Sul since April 2020. In early February 2021, antibody prevalence levels were 9.6%, 11.3%, 10.0% and 8.3% for unvaccinated individuals aged 10-19, 20-39, 40-59, and 60+ years, respectively (AJD Barros, personal communication). The state has been strongly affected by the recent pandemic wave, yet there is no evidence of important age patterns in antibody prevalence.
Thirdly, our results based on ratios of mortality rates closely mirror the findings from the proportionate mortality analyses, showing that the rate ratio for individuals aged 90+ relative to those aged 0-79 years fell from 20 in January to 7.7 in April.
Another potential limitation of our analyses is the underreporting of deaths and delays in reporting. Delays are particularly relevant for estimating mortality rates for recent periods, as only deaths that reached the system by April 22 were included. However, proportionate mortality by age groups would only be affected if delays varied systematically with age, which is unlikely. As discussed in the Introduction, the overall coverage of mortality statistics has been very high in Brazil for many years, and ill-defined causes represent 5.6% of all deaths. The mortality database for the present analyses includes approximately 30% more deaths than the SIVEP-Gripe database on hospital admissions and mortality that has been employed in previous analyses of COVID-19 deaths in Brazil.19-21
However, there is evidence that the excess mortality during 2020 relative to earlier years was not fully explained by deaths due to COVID-19. It is likely that some of such deaths were reported as having been due to other causes or to ill-defined conditions, but it is also possible that increases in non-COVID-19 deaths were because health services were under stress due to the large COVID-19 case load. Unless reporting patterns varied by age or calendar time, this limitation is unlikely to affect the present results.
The decline in mortality was observed for both sexes. Proportionate mortality at older ages was higher among women than for men, which is compatible with higher case-fatality of younger male adults, possibly related to comorbidities, given that existing serological surveys do not suggest differences in infection prevalence by sex.22,23. The reductions in proportionate mortality were very similar across four of the five regions of the country. A decline was also observed in the fifth region (Northern Brazil including the Amazon), but proportionate mortality was lower at the beginning of the year than in the rest of the country, and the decline started later than in the rest of the country. The Amazon region has been badly hit by the first and second waves of the pandemic, and high prevalence, high case-fatality, and the limited availability of health services in this region24 may have led to a larger number of deaths among young adults.
The most likely explanation for the observed reductions in proportionate mortality and in rate ratios for the elderly is the rapid increase in immunization coverage in these age groups, as has been described for other parts of the world.7-9 The increase in vaccine coverage preceded the decline in mortality. Our results are original in the sense that none of existing population-based mortality studies were carried out in a setting where the P.1 variant is predominant. Recent observational studies in vaccinated health workers in Manaus and São Paulo10,11 had already suggested that Coronavac provided some degree of protection against symptomatic illness in settings where P.1 was prevalent. Coronavac represents over three of every four vaccine doses administered in Brazil, with AstraZeneca vaccine accounting for one in six doses. Individuals who received the latter are so far protected by a single dose given that the second dose is provided 12 weeks after the first, whereas the second dose of Coronavac has already been administered to about half of individuals aged 80+ years6 as doses are given four weeks apart. The health worker study in São Paulo suggested that the number of cases started to drop after the first Coronavac dose, which is compatible with our findings.11
We attempted to provide an approximate estimate of lives saved among elderly Brazilians in the eight-week period since vaccination was accelerated throughout the country. The figure of approximately 14 thousand deaths averted is likely an underestimate, because it does not take into account lives saved among other priority groups for immunization, such as health workers and indigenous populations. Also, by using the mortality in ages 0-79 years to predict expected deaths among those aged 80+ years, we are not accounting for lives saved by the vaccine among younger age groups for whom coverage also increased, albeit at a slower rate. Although it is not possible to make strong causal arguments on the basis of the data available for our analyses, our findings are consistent with the results of efficacy trials for both vaccines, and with observational studies in high-risk groups of health workers.10,11 As of late April, data on hospital admissions in several Brazilian states suggest that the second wave of the pandemic is starting to wane, although health services are still badly overstretched in many parts of the country. Because compliance with non-pharmaceutical interventions such as social distancing and mask use is limited in most of the country, rapid scaling up of vaccination remains as the most promising approach for controlling the pandemic in a country where almost 400,000 lives have already been lost to COVID-19.
Data Availability
The analyses are based on publicly available data at the www.saude.gov.br website (detailed information on the exact urls is provided in the reference list).
Funding
CGV and AJDB are funded by the Todos Pela Saúde (São Paulo, Brazil) initiative.



