
Abstract
Sustained hyperglycemia in type 2 diabetes is associated with low levels of the endogenous antioxidant glutathione (GSH), which leads to oxidative stress and tissue damage. It is therefore important to investigate whether oral GSH supplementation would restore GSH levels, and also help improve redox state and glycaemia in diabetic individuals. We conducted a pragmatic clinical trial to assess effectiveness of oral GSH supplementation along with anti-diabetic treatment. 104 non-diabetic and 250 diabetic individuals were recruited. All the 250 diabetic individuals were on anti-diabetic therapy; of these 125 were given oral GSH supplementation additionally for a period of six months. Fasting and PP glucose and insulin, HbA1c, GSH and the oxidative DNA damage marker 8-OHdG were measured at the recruitment time and after three and six months of supplementation. GSH supplementation increased blood GSH and decreased 8-OHdG significantly within three months in diabetic individuals. It also reduced HbA1c within three months and stabilized it thereafter in diabetic population overall. Patients above 55 years benefited more as evidenced by a significant decrease in HbA1c and 8-OHdG and an increase in fasting insulin. Data suggest that GSH supplementation can be used as an adjunct therapy to anti-diabetic treatment to achieve better glycemic targets, especially in elderly population.
Trial registered This study has been registered with Clinical Trials Registry-India (CTRI/2018/01/011257)
Novelty bullets
Oral GSH supplementation replenishes body stores of GSH and significantly reduces oxidative DNA damage in diabetic patients over six months.
HbA1c is lowered at three months and is stabilized thereafter.
A significant decrease in HbA1c and elevated fasting insulin was observed in people older than 55 years.
Introduction
Hyperglycemia accelerates the production of reactive oxygen species (ROS) and leads to substantial oxidative stress (OS) in diabetic patients (Brownlee, 2001). Hyperglycemia-mediated ROS production leading to oxidative damage to biomolecules, is in fact, proposed to be a common unifying mechanism of diabetic complications. ROS activates four different pathways namely, advanced glycation end products (AGEs) (Shinomara et al., 1998), polyol (Lee and Chung 1998), hexosamine (Kolm-Litty et al., 1998), and protein kinase C (Derubertis and Craven, 1994), all of which are involved in the development of diabetic microvascular complications (Brownlee, 2005). Therefore, one important strategy for alleviating diabetic complications could potentially be to scavenge hyperglycemia-mediated ROS in diabetic patients. Studies in animal models of diabetes have shown that treatment with antioxidants such as, N-Acetyl-L-Cysteine (NAC) (Kaneto et al., 1999; Haber et al., 2003), lipoic acid (Moini et al., 2002), and glutathione (GSH) (Aw et al., 1991; Ueno et al., 2002) or precursors of GSH, such as glycine and cysteine (Jain et al., 2009; El-Hafidi et al., 2018), partially improves the blood glucose levels, functionality of β-cells, insulin sensitivity and reduces diabetic complications. However, human clinical trials using antioxidants in patients with cardiovascular diseases and metabolic syndrome have not been conclusive (Johansen et al., 2005).
Clinical trials of GSH supplementation as an endogenous antioxidant have recently received a great deal of attention. GSH, a water-soluble tri-peptide synthesized from glutamate, cysteine, and glycine, is an important endogenous antioxidant required for maintaining redox homeostasis of the cell. It is synthesized by glutathione synthetase and utilized by GSH peroxidase and glutaredoxin to detoxify free radicals. In the process, it is converted to its oxidized form, GSSG which is converted back to GSH by glutathione reductase (Njalson and Norgren, 2007). Low GSH levels are known to be associated with several pathological conditions, such as cancer, arthritis, cardiovascular and neurodegenerative diseases, and diabetes (Nuttall et al., 1998; Townsend et al., 2003). Several reports, including work from our lab, have confirmed that GSH levels are significantly low in diabetic patients (Martian-Gallan et al 2003; Song et al., 2007; Acharya et al., 2014; Picu et al., 2017). GSH insufficiency can be due to increased exposure to oxidants, drugs, excess nutrients or decreased rate of synthesis of GSH arising from nutritional deficiency of its precursor amino acids (De Luca et al., 2001). Genetic factors such as SNPs in the genes coding for enzymes required for GSH synthesis may also result in decreased GSH levels. It is plausible that GSH supplementation may help in arresting the development of complications in type 2 diabetes by improving the redox state and minimizing the oxidative damage to the biomolecules.
Oral administration of GSH or its precursor amino acids has been shown to enhance body stores of GSH, in plasma as well as tissues (Aw et al.,1991; Favilli et al., 1997; Kariya et al. 2007) and protected against different pathological conditions. Richie et al. (2015) demonstrated its effectiveness in restoring body stores of GSH in a dose and time dependent manner. Several different forms of GSH, such as sublingual (Schmitt et al., 2015), orobucccal (Buonocore et al., 2016; Bruggeman et al., 2019) and liposomal (Sinha et al., 2018) have recently been reported to be effective in restoring body stores of GSH. Supplementation with glycine, a precursor of GSH, has also been shown to increase the rate of GSH synthesis in elderly individuals (Sekhar et al., 2011a). However, results from human clinical trials of oral GSH supplementation have often been contrasting and debatable. Allen and Bradley, (2011) reported that oral GSH supplementation in healthy adults did not change GSH levels and other biomarkers of OS. Whereas, Richie et al., demonstrated that oral GSH supplementation leads to significant increase in body stores glutathione (Richie et al., 2015). Discrepancies in the outcomes of these studies could be attributed to differences in the dose and duration of GSH, and measurement of GSH in human plasma instead of erythrocyte fraction, where GSH is known to be turned over rapidly.
Most studies of GSH supplementation have focused on restoring body stores of GSH. However, it is likely that the relationships of GSH supplementation with pathology are complex. We have previously demonstrated that controlling hyperglycemia over a period of two months increases blood GSH levels and reduces oxidative damage significantly, regardless of the anti-diabetic treatment prescribed to them (Acharya et al., 2014). More than a dozen markers of OS were measured; of these, GSH impressively correlated with glucose recovery, that is, it responded rapidly, within 8 weeks, to changes in glycosylated haemoglobin (HbA1c) (Kulkarni et al., 2014). This suggests that altering hyperglycemia rapidly results in changes in GSH. It is equally interesting to ask whether changes in GSH feed back into glycemia? It is well understood, for instance, that β-cells are poorly protected against OS (Lenzen et al.,, 1996; Tiedge et al., 1997), hence an improvement in the redox state might, plausibly, relieve stress on β-cells, and in turn assist glycemic control. A few studies have examined the effects of GSH infusion on improving glycemic parameters in diabetic patients. Paolisso et al. (Piolisso et al., 1992a) reported increased GSH, and total body glucose disposal; further, this effect was more pronounced in elderly individuals with impaired glucose tolerance (Piolisso et al., 1992b). On the other hand, Sekhar et al. (Sekhar et al 2011b) showed that infusion with glycine, a precursor of GSH, increased the rate of GSH synthesis and reduced lipid peroxidation in diabetic individuals; however, it did not lead to changes in HbA1c.
We hypothesize that oral GSH supplementation can (i) increase body stores, (ii) improve the systemic redox state to alleviate OS and, further (iii) protect β-cells against OS (iv) improve insulin secretion, and (v) help anti-diabetic treatment in restoring normoglycemia.
Here we have conducted a pragmatic prospective clinical trial to assess whether oral GSH supplementation improves body stores of GSH in diabetic patients. We further asked if the effect of GSH supplementation in combination with anti-diabetic treatment is cumulative, that is, it has an additional benefit in improving glucose control and minimising oxidative damage in diabetic patients. We serially measured concentrations of GSH, 8-hydroxy-2-deoxy guanosine (8-OHdG), an oxidative damage marker, and glycemic parameters in diabetic patients receiving GSH supplementation in addition to anti-diabetic treatment, and compared them with serial measurements in those receiving anti-diabetic treatment alone. We find that GSH supplementation not only improved body stores of GSH, and decreased oxidative damage to DNA but also helped stabilize lowered HbA1c in diabetic patients. We noted that this effect of GSH supplementation is more pronounced in elderly diabetic patients (age more than 55 years).
Materials and methods
Study design
We conducted a pragmatic clinical trial which is designed as a case-control cohort study to assess the effect of oral GSH supplementation on blood GSH levels and glucose homeostasis in diabetic patients.
Study approval
This study was approved by the Institutional Ethical Committee of Jehangir Hospital Development Center, Pune (Dr. Ravindra Ghooi, Chairman, Ethics committee Jehangir clinical development center ECN-ECR/352/Inst/NIH/2013); Institutional Biosafety Committee of SPPU (Bot/27A/15), Pune; and Institutional Ethical Committee of IISER, Pune. Signed informed consent was obtained from all the subjects at the time of enrollment in the study after explaining the purpose and nature of the study. All participants in this study were de-identified using a numbered code. This study is registered with Clinical Trials Registry-India (CTRI/2018/01/011257).
Inclusion/Exclusion criteria for study participants
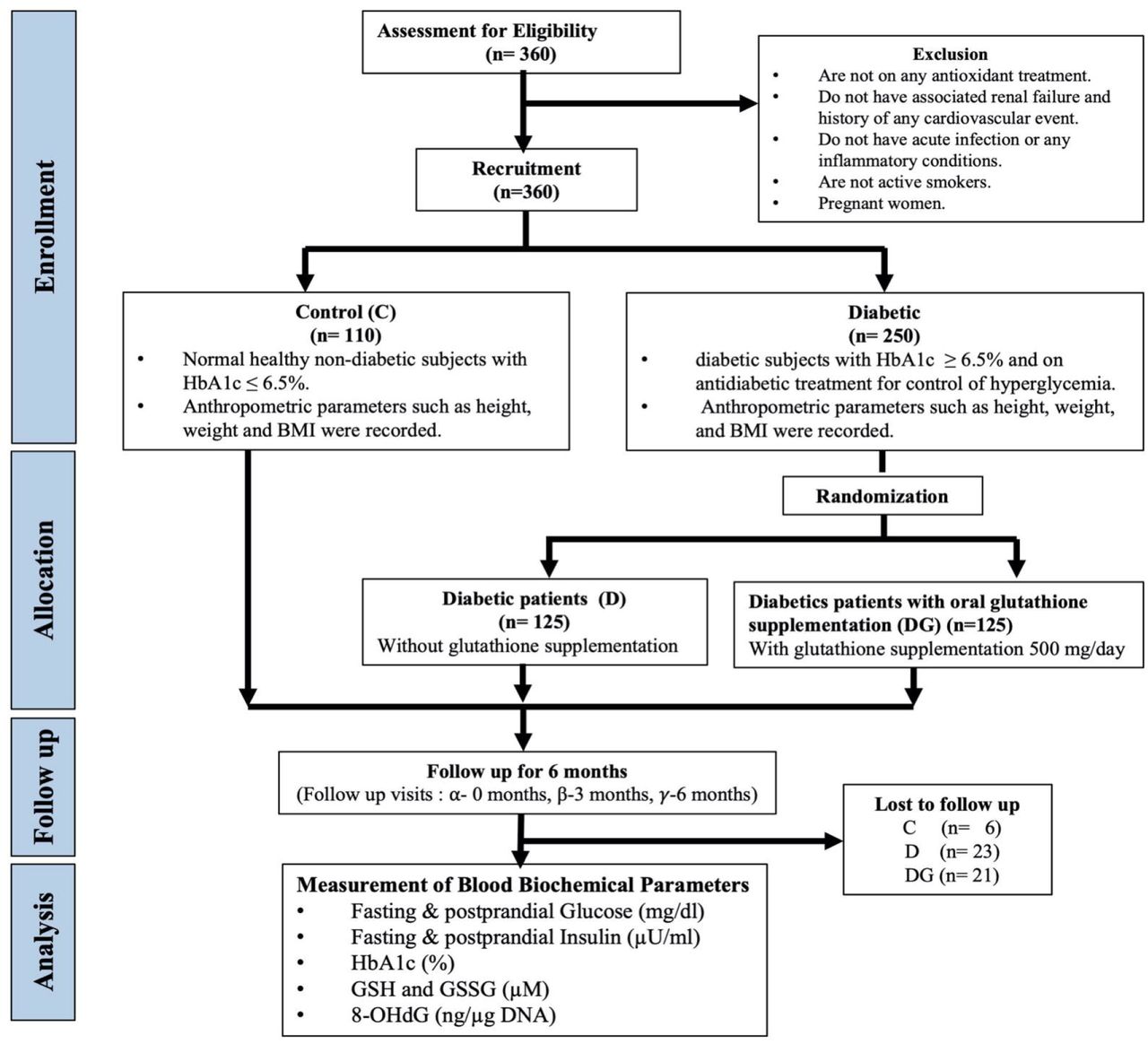
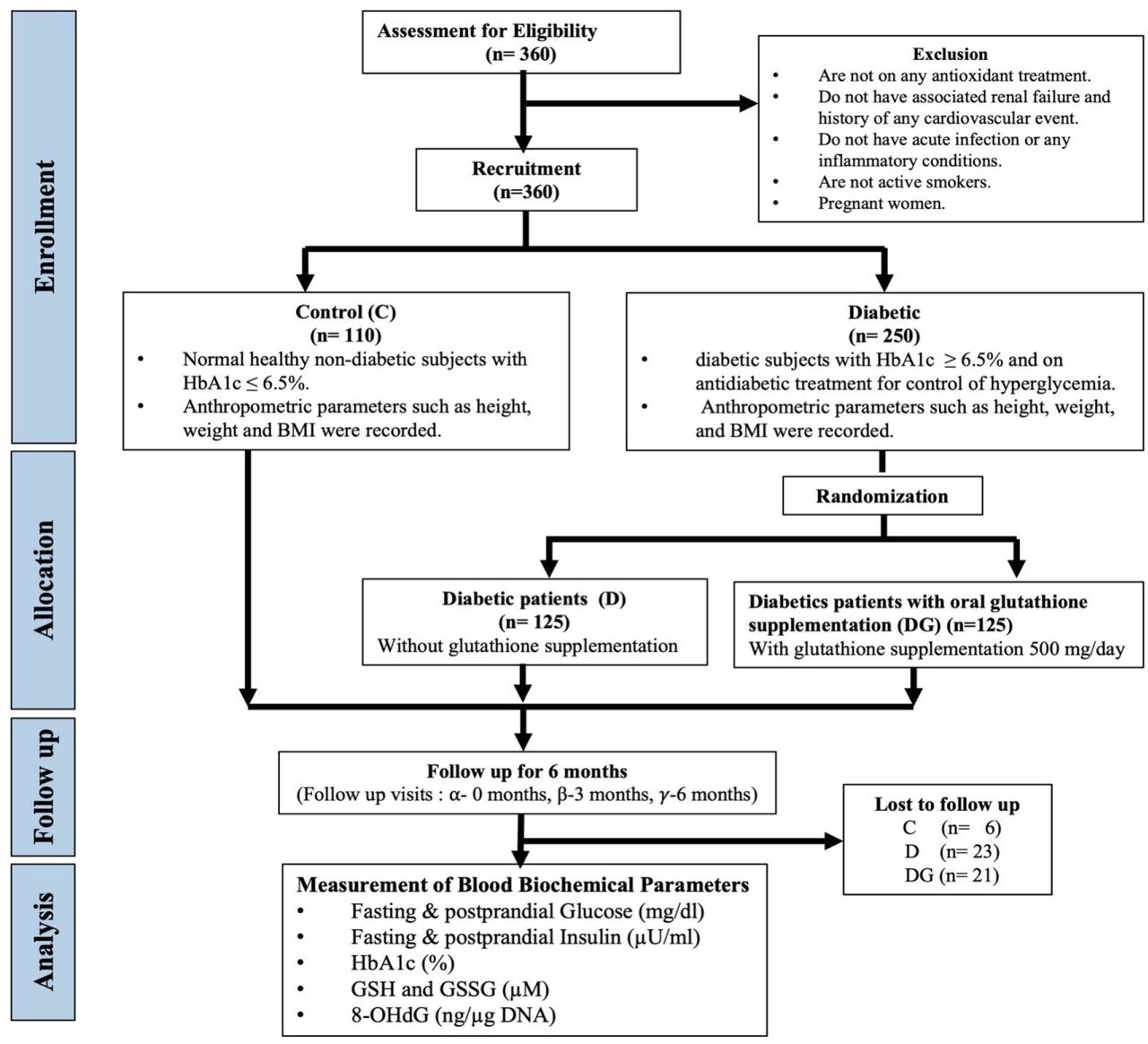
We recruited healthy non-diabetic controls (n=104) (Control group) with HbA1c < 6.5%, and known type 2 diabetic subjects (n=250) with HbA1c ≥ 6.5% (ADA, 2016) of either sex between age of 30-70 years visiting Jehangir Hospital and Iyer clinic, Pune. Pregnant women, individuals with excessive alcohol intake, heavy smokers, individuals with any clinical infection or with a history of a recent cardiovascular event, and those receiving antioxidants were excluded from the study. Body weight, height, anti-diabetic treatment and family history of diabetes were noted for each subject.
Recruitment and randomisation for GSH intervention
We recruited known diabetic subjects (n=250) who were already on anti-diabetic regimen and randomly categorized them into two groups: 125 diabetic patients who were advised to continue with their anti-diabetic regimen as prescribed by physician (Group D), and the other 125 diabetic patients who were given 500 mg glutathione (Jarrow Formulas, USA) supplementation once daily in addition to their anti-diabetic treatment (Supplemental Table S1) for a period of six months (Group DG) (Fig. 1). At the time of randomisation, concentrations of covariates fasting and PP glucose and insulin, HbA1c, GSH and oxidized glutathione (GSSG), and 8-OhdG were not available, and therefore, did not influence the assignment of diabetic patients in D or DG groups. Patients in the DG group were issued two bottles of GSH (each bottle containing 60 capsules of 500 mg each) and were called back after three months to collect an additional bottle for the remaining duration. During the tenure of the study compliance to medical treatment by patients of D and DG group and consumption of GSH by patients of the DG was emphasized by maintaining continuous communication between the physician and patients. Out of 125 diabetic patients in D and DG group, 23 were lost to follow-up in the D group and 21 in DG group for not complying with the treatment regimen. We also recruited healthy non-diabetic control subjects who were followed for six months during which they were advised to continue with their regular diet and exercise regimen. Blood samples were collected at the time of enrollment 0 (alpha (α) visit), 3 (beta (β) visit) and 6 (gamma (γ) visit) months after the date of enrollment.
Sample collection
At each visit, a total of 10 ml fasting and postprandial (PP) blood samples were collected from all the subjects by Golwilkar Metropolis, Pune-411004, in 5 and 2 ml vacutainers containing EDTA for collecting plasma and whole blood samples, and 3 ml vacutainers without EDTA for collecting serum. Whole blood samples were centrifuged at 4000 rpm for 10 mins to separate plasma and erythrocyte fraction. Plasma was separated and stored at −80°C (Thermo Fisher Scientific, USA) for further analysis.
Outcomes
Primary outcome measures include GSH and HbA1c. Secondary outcomes include GSSG, fasting glucose (FPG) and insulin (FPI), PP glucose (PPG), and insulin (PPI), and 8-OHdG.
Estimation of blood biochemical parameters
Measurement of FPG, PPG, FPI, PPI, and HbA1c was performed on an automated analyzer at Golwilkar Metropolis, Pune, by following CLSI (Clinical and Laboratory Standards Institute, USA) guidelines. Erythrocyte fraction was then used for preparation of hemolysates by washing it twice with cold saline (9.0 g/L NaCl) and hemolyzed by adding ice-cold ultrapure water (MilliQ plus reagent grade; Millipore, Bedford, MA, USA) to get 50% diluted hemolysates (Acharya et al., 2014) which were stored at −80°C for further analysis.
Estimation of GSH and GSSG
Reduced and total glutathione content in erythrocyte hemolysate was estimated using Glutathione assay kit (Cayman Chemical, USA). This kit follows DTNB (5,5’-dithio-bis-2 nitrobenzoic acid, Ellman’s reagent) method for estimation of GSH (Baker et al., 1990) where DTNB reacts with reduced GSH yielding yellow-colored 2-nitro-5-thiobenzoate, which is read at 405 nm, on ELISA reader.
Briefly, 50 µl of erythrocyte lysate was deproteinized using an equal volume of metaphosphoric acid at 4°C. After vigorous vortexing, the resulting mixture was centrifuged at 2000 g for 2 mins at 4°C. The supernatant was separated and aliquoted in two parts and used for estimation of total GSH (TGSH) and GSSG. pH of the samples was adjusted to 8 by the addition of triethanolamine (5 µl/100 µl of the sample). One of the aliquots was diluted 50 times with 1x MES buffer (0.4 M (N-morpholino) ethanesulphonic acid, 0.1 M phosphate buffer and 2 mM EDTA) and used for estimation of TGSH. In the second aliquot, 2 µl of vinyl pyridine was added and diluted 25 times with 1x MES buffer and 50 µl of this sample was used for estimation of GSSG. Both the aliquots were then incubated for 1 hour at room temperature. The reaction was started by adding 150 µl assay cocktail containing 11.25 ml MES buffer, 0.45 ml cofactor mixture containing NADP+ and glucose-6-phosphate, 2.1 ml enzyme mixture containing glutathione reductase and glucose-6-phosphate dehydrogenase, 2.3 ml water and 0.45 ml DTNB. Increase in TNB formation was determined by measuring absorbance at 405 nm at 5 min interval for 30 mins. GSSG was used as a standard for estimating the concentration of TGSH and GSSG in samples. Absorbance values of samples and standard curve (0, 0.5, 1.0, 2.0, 4.0, 8.0, 12.0, and 16.0 µM) were plotted as a function of time and slope for each sample was calculated. This was called i-slope. i slope of each concentration of standard was plotted against the concentration of GSH and the slope of this curve was called as f-slope. Values for total GSH and GSSG were calculated by using the formula given below. GSH concentration was determined by subtracting GSSG from total GSH.
Estimation of 8-OHdG
DNA was isolated from whole blood by standard phenol-chloroform-isoamyl alcohol extraction method, quantitated on nanodrop and concentration of 8-OHdG was determined by competitive enzyme-linked immunosorbent assay following the protocol of Modak et al. (2009) and expressed as nanogram 8-OHdG/µg DNA.
Statistical methods
Biochemical parameters of subjects in Control, D and DG groups at the first visit were represented using the descriptive statistics (Median, 25th percentile, 75th percentile). All intra-group and inter-group comparisons of biochemical parameters at different visits were performed using permutation tests, using the “Coin” package in R (Hothorn et a;., 2006). Statistical significance was set at p-value < 0.05. The results of permutation tests were confirmed with two-sample, two-sided t-tests, and are reported in Supplemental sections. Effect size analysis was used to quantify the difference between 6-month biochemical changes from α to γ visit in D and DG groups. Statistical analysis and effect size calculations were repeated between subgroups in D and DG consisting of elderly subjects with age more than 55 years. All effect size calculations and parametric t-tests for comparisons were carried out using Matlab version 2019.
Effect size between change in the biochemical levels of D, and DG group individuals
Biochemical measurements at α, β and γ visits of the D group subjects are represented by variables  and measurements from DG group subjects by
and measurements from DG group subjects by  , respectively. The biochemical variables, X are HbA1c, FPG, FPI, PPG, PPI, GSH, GSSG, and 8-OHdG. Changes from α to γ visit (6-months) in D were estimated by taking their paired differences as
, respectively. The biochemical variables, X are HbA1c, FPG, FPI, PPG, PPI, GSH, GSSG, and 8-OHdG. Changes from α to γ visit (6-months) in D were estimated by taking their paired differences as  , with a group-wise mean of paired difference,
, with a group-wise mean of paired difference,  . Similarly,
. Similarly,  represents the paired changes from α to γ visit (6 months) with a group-wise mean,
represents the paired changes from α to γ visit (6 months) with a group-wise mean,  in DG.
in DG.
The effect size of 6-month changes in the concentration of a particular biochemical variable, X, between D and DG groups are estimated using Cohen’s d (Cohen, 1988) as
 where pooled standard deviation of biochemical changes in D and DG, s, is given by
where pooled standard deviation of biochemical changes in D and DG, s, is given by

Here NC, ND and NDG are the number of individuals in Control, D and DG groups respectively. Cohen (1969) described an effect size of 0.2, 0.5, and 0.8 as “Small”, “Medium”, and “Large” effect respectively, and Sawilowsky (2003), classified an effect of size 1.2 as “Very large” and 2 as a “Huge” effect.
Results
Baseline characteristics of study groups
The study population included diabetic subjects with a mean age of 54 years and BMI 26.9 kg/m2 and the control group included individuals with a mean age of 41 years and BMI 26 kg/m2. D group comprised of 57 males and 45 females, DG group contained 49 males and 55 females, and the control group comprised of 62 males and 42 females. Baseline characteristics of subjects in each group are presented in Table 1.
Data from each group at the α visit are presented here as median and interquartile ranges (25th percentile-75th percentile). * indicates the significance of the comparison between baseline measurements of Control versus D or Control versus DG groups. Significance levels are *p < 0.05, **p < 0.01, ***p < 0.001. (See Table S3 for alternate comparisons using two-sample, two-sided t-tests). # indicates the significance of the comparison between D and DG using two-sample permutation tests (p <0.05).
Concentrations of FPG, PPG, FPI, HbA1c, and 8-OHdG were significantly high and that of GSH was significantly low in D and DG compared to Control (p<0.001, all parameters). Levels of PPI in D and DG were not found to be significantly different compared to the control group (Table 1).
We did not observe any significant differences in the levels of FPG, PPG, FPI, PPI, HbA1c, and GSH within D and DG groups, thus, confirming covariate balance in the two groups at baseline. The concentration of GSSG, and 8-OHdG were found to be significantly different (p<0.05) between D and DG (Table 1).
Oral GSH supplementation increases erythrocyte GSH, GSSG and decreases oxidative damage to DNA but does not alter glycemia in diabetic patients over a period of six months
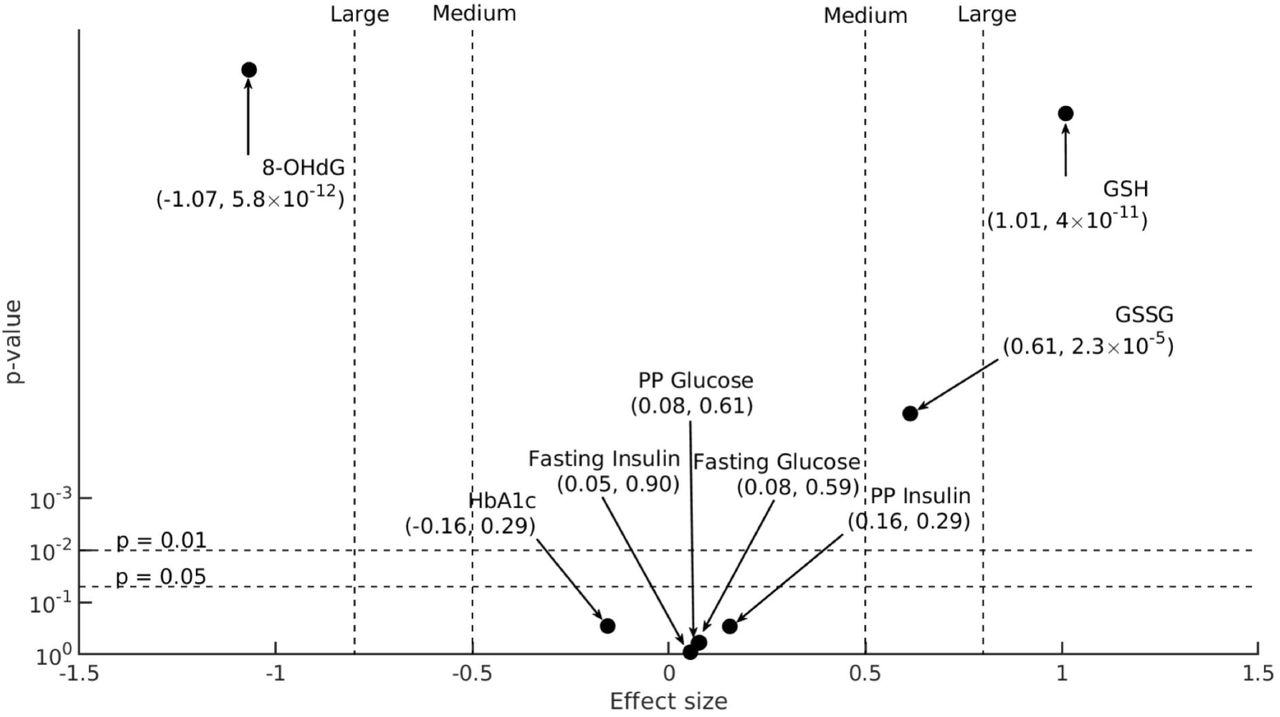
Our study estimates the effect of oral GSH supplementation on erythrocyte GSH concentrations over a period of six months in diabetic patients. GSH levels increased significantly over a period of six months, from α to γ visit in both DG (p<0.001) and D (p<0.001) groups, while they remained unchanged in the Control. We further estimated the effect size of GSH supplementation within the diabetic groups: A “Large” effect (Cohen’s d = 1.01; p<0.001) indicated that the increase in GSH is significantly high in DG compared to D (Fig. 2). GSSG was similarly increased in DG compared to D (Cohen’s d=0.61, p<0.001).
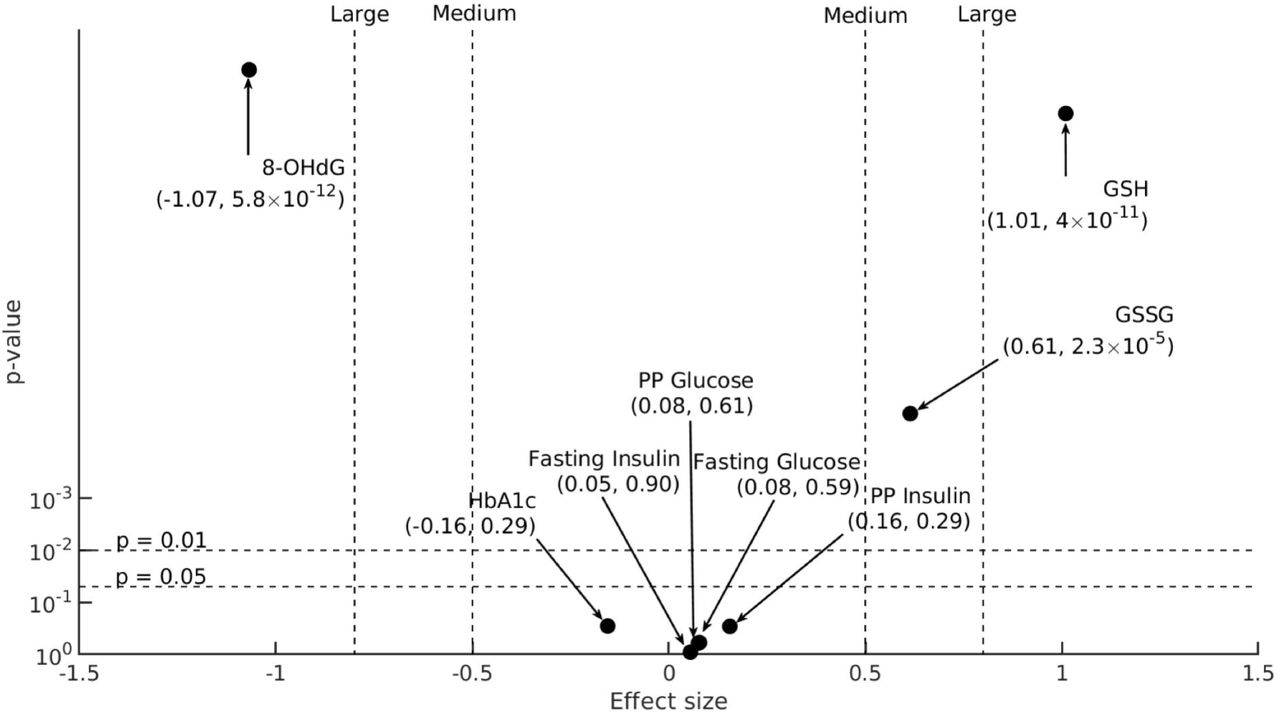
6-month changes in biochemical parameters (X= HbA1c, FPG, FPI, PPG, PPI, GSH, GSSG, and 8-OHdG) D and DG groups,  and
and  , respectively (sample sizes for HbA1c, FPG, FPI are: ND = 90, NDG = 104, for PPG and PPI:ND= 90, NDG = 102, for GSH and GSSG:ND= 89, NDG = 101, for 8-OHdG: ND = 91, NDG = 104), are compared here on a statistical significance (y-axis) versus effect size (x-axis) plot. Effect size (Cohen’s d) calculated between 6-month changes in the concentration of biochemical variables, X, in D and DG (
, respectively (sample sizes for HbA1c, FPG, FPI are: ND = 90, NDG = 104, for PPG and PPI:ND= 90, NDG = 102, for GSH and GSSG:ND= 89, NDG = 101, for 8-OHdG: ND = 91, NDG = 104), are compared here on a statistical significance (y-axis) versus effect size (x-axis) plot. Effect size (Cohen’s d) calculated between 6-month changes in the concentration of biochemical variables, X, in D and DG ( and
and  ) are denoted on the x-axis. The p-value of comparison between the group-wise means of 6-month changes in X’s concentration,
) are denoted on the x-axis. The p-value of comparison between the group-wise means of 6-month changes in X’s concentration,  and
and  (Supplemental Table S4), obtained using two-sample permutation tests are denoted on the y-axis (Supplemental Figure S1 for an alternative version of this figure using two-sample, two-sided student’s t-tests instead). Two horizontal dotted lines denote 95% and 99% significance levels. Effect size takes either a positive or negative sign based on the direction of change: a positive effect size increases towards the right and a negative effect towards the left. Vertical dotted lines represent different classifications of effect size. In particular, “Medium” effects are labeled at 0.5 and −0.5, and “Large” effects at 0.8 and −0.8.
(Supplemental Table S4), obtained using two-sample permutation tests are denoted on the y-axis (Supplemental Figure S1 for an alternative version of this figure using two-sample, two-sided student’s t-tests instead). Two horizontal dotted lines denote 95% and 99% significance levels. Effect size takes either a positive or negative sign based on the direction of change: a positive effect size increases towards the right and a negative effect towards the left. Vertical dotted lines represent different classifications of effect size. In particular, “Medium” effects are labeled at 0.5 and −0.5, and “Large” effects at 0.8 and −0.8.
We also observed a significant decrease in the concentrations of 8-OHdG from α to γ visit in DG (p<0.001) but not in D and Control groups (p>0.05). GSH supplementation resulted in a “Large” effect (Cohen’s d = −1.07; p<0.001) indicating that 8-OHdG decreased significantly in DG compared to D (Fig. 2).
We then analyzed the effect of oral GSH supplementation on glycemic parameters, namely HbA1c, FPG, PPG, FPI, and PPI in diabetic patients. We observed that HbA1c levels decreased significantly over six months in both D and DG, however, the extent to which HbA1c levels decreased in DG was comparable to D group as indicated by a small Cohen’s d = −0.16 (p>0.05) (Fig. 2). FPG, PPG, FPI, and PPI decreased over a period of six months in D and DG, however, changes in DG were comparable to those in D (p>0.05, Cohen’s d<0.2, all parameters). Mean values for biochemical variables at 0, 3 and 6 months for the study groups are detailed in Supplemental Table S2.
Overall, our results indicate that GSH supplementation leads to a significant increase in the erythrocyte GSH and GSSG and decrease in the 8-OHdG concentrations in diabetic patients. However, glycemic parameters change in D and DG to similar extents.
Next, we investigated whether the effect of oral GSH supplementation on the above mentioned biochemical parameters is accomplished rapidly, say, within the first three months of GSH supplementation, and stabilized thereafter, or whether their levels change gradually over a period of six months. We, therefore, examined changes in the concentration of FPG, PPG, FPI, PPI, HbA1c, GSH, GSSG, and 8-OHdG serially from 0 to 3 and 6 months in each of the three groups. These results are described in the following section.
Oral GSH supplementation enhances erythrocyte GSH concentration in diabetic subjects within three months
Fig. 3 a and b show serial changes in the concentrations of GSH, and GSSG, respectively, from α to β and γ visits in the three study groups. In Control, the concentrations of GSH and GSSG remained unchanged over a period of six months. GSH supplementation in DG led to a significant increase in GSH within the first three months (p<0.001) and remained stable thereafter up to six months (Fig. 3a). In the D group, on the other hand, GSH increased gradually from 0 to 3 and 6 months. In the DG group (Fig. 3b), GSSG concentration also increased significantly within the first three months (p<0.001), and did not change further. In D, on the other hand, GSSG remained unchanged during the study period (p>0.05).

Mean (black dots) and 95% confidence interval (whiskers) of (a) GSH and (b) GSSG concentrations at α visit (NC = 104, ND = 100, NDG = 101), β visit (NC = 104, ND = 100, NDG = 101), and γ visit (NC = 104, ND = 89, NDG = 101) are shown here for Control, D and DG groups. Significance levels (*) displayed above β, and γ visits denote the comparisons with α visit using permutation tests. Significance levels are *p < 0.05, **p < 0.01, ***p < 0.001 for respective comparisons. (See Supplemental Fig. S2 for alternative comparisons using paired sample t-tests instead and Supplemental Table S6 for p-values of comparisons).
Thus, oral GSH supplementation in diabetic patients increased erythrocyte GSH concentration significantly within three months and stabilized it thereafter. On the other hand, in D, anti-diabetic therapy alone led to a small increase in GSH but not in GSSG.
Oral GSH supplementation reduces 8-OHdG concentrations in diabetic subjects
Further, we evaluated the effect of GSH supplementation on serial changes in 8-OHdG in diabetic patients. In Control, its concentrations remained unchanged over a period of six months. GSH supplementation in diabetic patients led to a significant decrease in 8-OHdG within the first three months and it continued to reduce significantly thereafter (p<0.001) (Fig 4a). However, in the D group, its concentrations did not change significantly throughout the study period.

Mean (black dots) and 95% confidence interval (whiskers) of (a) 8-OHdG, (b) FPG, (c) PPG, (d) HbA1c, (e) FPI, and (f) PPI concentrations at α (sample sizes for 8-OHdG, HbA1c, FPG, FPI, PPG are: NC = 104, ND=102, NDG =104; for PPI:NC = 103, ND=102, NDG =104; and for GSH, GSSG:NC = 104, ND =100, NDG =101), β (for HbA1c, FPG and FPI:NC = 104, ND=102, NDG =103; for PPG:NC = 103, ND=102, NDG =103; for PPI:NC = 103, ND=101, NDG =102, for 8-OHdG: NC =104, ND=102, NDG = 104 and for GSH, GSSG:NC = 104, ND =100, NDG =101), and γ visit (for HbA1c, FPG, FPI:NC = 104, ND=90, NDG =104; for PPG and PPI:NC = 104, ND=90, NDG =102, for 8-OHdG: NC =104, ND=91, NDG =104 and for GSH, GSSG:NC = 104, ND =89, NDG =101 are shown here for Control, D, and DG groups. Significance levels (*) displayed above β and γ visits denote the comparisons with α visit using permutation tests. Significance levels are *p < 0.05, **p < 0.01, ***p < 0.001 for respective comparisons. (See Supplemental Fig. S3 for alternative comparisons using paired sample t-tests instead).
Serial changes in HbA1c levels are stabilized by oral GSH supplementation in diabetic patients
We examined serial changes in the levels of FPG, PPG, HbA1c, FPI, and PPI in D and DG groups in greater detail. FPG levels lowered significantly within three months in D (p<0.01) and DG (p=0.05); however, it recovered to the baseline levels by the end of six months (Fig. 4b). PPG levels, on the other hand, did not change significantly in D and DG over a period of six months (p>0.05, all) (Fig. 4c). Thus, based on these results and Fig. 2, we conclude that GSH supplementation does not have any effect on FPG, and PPG levels in diabetic patients overall.
HbA1c levels rapidly decreased from 0 to 3 months in both D (p<0.01) and DG (p<0.001) (Fig 4d). Thereafter, HbA1c levels were maintained until 6 months in DG while they appear to have returned to the baseline level in D group.
FPI levels changed significantly from 0 to 3 and 6 months in D (p<0.05), while it remained unchanged in DG (p>0.05) (Fig 4e). PPI levels remained unaltered in D and DG throughout the study period (Fig. 4f).
Thus, the glycemic parameters, namely, FPG, PPG, FPI, and PPI do not change significantly in response to GSH supplementation. Taken together, oral GSH supplementation in diabetic patients appears to have “stabilizing effect” on HbA1c i.e., it decreases rapidly within three months and continues thereafter.
Oral GSH supplementation significantly reduces HbA1c in a sub-group of diabetic patients, age>55 years
Earlier reports suggest that concentration of GSH decreases with age in healthy adults (Matsubara et al., 1991; Lang et al., 1992; Erdennal et al., 2002; Sekhar et al., 2011). Diabetes has also been reported to cause long term cardiovascular complications and congestive failure, which become marked with age. For instance, the Framingham study (Kannel, 1979) reported increased severity of chronic heart failures and related deaths in an age group above 55 years. Similarly, diabetes-related vascular complications in veterans (mean age = 60 ± 9 years) were also pointed out by Duckworth et al. (2009). Therefore, we believe it is important to assess the effect of GSH supplementation in elderly diabetic patients.
Diabetic patients in our study ranged from 31 to 78 years of age. The median age in these cohorts is about 55 years. This motivated us to use this age threshold to isolate the older sub-group. We then re-examined the effect of GSH supplementation in this sub-group diabetic population to assess whether they respond differently to oral GSH supplementation compared to the younger population.
Mean values for biochemical parameters GSH, GSSG, 8-OHdG, FPG, PPG, HbA1c, FPI, and PPI; and serial changes from 0 to 3 and 6 months in their concentrations in D (n=44) and DG (n=54) groups are shown in Supplemental Table S5 and Supplemental Fig. S5 and S6, respectively. Similar to results obtained for diabetic patients overall, the concentration of GSH and GSSG increased significantly over a period of 6 months in both D, and DG sub-groups (Supplemental Fig. S5). Changes in the mean GSH and GSSG levels over a period of 6 months in DG group (Fig. 5) was significantly higher compared to the D group (Cohen’s d = 1.14 and 0.67 for GSH and GSSG, respectively, p<0.001).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
6-month changes in biochemical parameters in D and DG sub-groups of elderly diabetic subjects (age > 55 years),  and
and  , respectively (sample sizes for HbA1c, FPG, FPI are:ND = 44, NDG = 54, and for PPG, PPI, GSH, GSSG are:ND= 44, NDG = 53, for 8-OHdG: ND= 45, NDG = 54), are compared here on a statistical significance (y-axis) versus effect size (x-axis) plot. Effect size calculated between
, respectively (sample sizes for HbA1c, FPG, FPI are:ND = 44, NDG = 54, and for PPG, PPI, GSH, GSSG are:ND= 44, NDG = 53, for 8-OHdG: ND= 45, NDG = 54), are compared here on a statistical significance (y-axis) versus effect size (x-axis) plot. Effect size calculated between  and
and  , are denoted on the x-axis. The p-values of comparison between the subgroup-wise means of 6-month changes,
, are denoted on the x-axis. The p-values of comparison between the subgroup-wise means of 6-month changes,  and
and  (Supplemental Table S8), obtained using permutation-tests are denoted on the y-axis (Supplemental Fig. S4 for alternative comparisons using two-sample, two-sided t-tests instead, and Supplemental Table S8 for p-values of comparisons).
(Supplemental Table S8), obtained using permutation-tests are denoted on the y-axis (Supplemental Fig. S4 for alternative comparisons using two-sample, two-sided t-tests instead, and Supplemental Table S8 for p-values of comparisons).
Further, we also analysed the effect size of 8-OHdG concentrations in this elderly sub-group of diabetic patients on GSH supplementation. GSH supplementation resulted in a “Very large” effect (Cohen’s d = −1.45, p<0.001) indicating that 8-OHdG decreased significantly in DG compared to the D group over the period of 6 months (Fig. 5). This suggests that oral GSH supplementation in elderly diabetic population results in a significant reduction in the accumulation of oxidative DNA damage.
Next, we examined the effect size of blood glycemic parameters in response to oral GSH supplementation in the elderly sub-group of diabetic patients (Fig. 5). In contrast to the results observed in diabetic population overall, GSH supplementation in DG sub-group led to a significant reduction in HbA1c levels over a period of 6 months compared to D (Cohen’s d = - 0.41, p<0.05).
Interestingly, FPI levels also increased significantly in DG sub-group from α to γ visit compared to D (Cohen’s d = 0.56, p<0.05). GSH supplementation had a small effect on levels of FPG, PPG, and PPI in DG sub-group (Cohen’s d <0.2, p<0.05, all parameters). Mean changes in all biochemical parameters from α to γ visit in elderly diabetic patients of D and DG sub-groups are provided in Supplemental Table S7.
Thus, GSH supplementation in DG sub-group of elderly diabetic patients over a period of 6 months led to a significant increase in the erythrocyte GSH, GSSG, and FPI concentrations and reduced HbA1c and 8-OHdG levels significantly. This suggests that the elderly diabetic population responds to GSH supplementation in conjunction with anti-diabetic therapy better in terms of a significant reduction in HbA1c levels and accumulation of oxidative DNA damage compared to the diabetic population overall.
Discussion
Sustained hyperglycemia is linked to an increase in OS which further results into risk of developing diabetic micro- and macrovascular complications (Brownlee, 2005). Interventions aiming at controlling hyperglycemia are the primary line of treatment for diabetic patients. It is interesting to ask if improving redox status by GSH supplementation can help counteract the deleterious effects of hyperglycemia-induced OS. GSH levels are known to be significantly low in diabetic patients, however, the bioavailability of oral GSH supplementation in humans is controversial (Allen and Bradley, 2011; Richie et al., 2015). Our study provides evidence that oral GSH supplementation not only improves body stores of GSH but significantly decreases accumulation of oxidative DNA damage and also helps increase the efficiency of regular anti-diabetic treatment in maintaining normoglycemia in diabetic patients.
GSH is known to be either transported in its intact form from the intestinal epithelial cells into blood lumen (Hagen et al., 1987; Hagen et al., 1990; Kovacs-Nolan et al., 2014) or broken down by gamma-glutamyltransferase (GGT) to its constituent amino acids (Hanigan, 2014). It is unclear whether GSH was either directly absorbed or was broken down into its constituent amino acids, and re-synthesized by glutathione synthetase. Additionally, we find a significant increase in the concentration of erythrocytic GSSG. This is possibly due to the conversion of erythrocytic GSH into GSSG, in line with previous reports, for instance Kovacs-Nolan et al. (2014) show that 13C-GSH administered to mice is rapidly converted to GSSG and accumulated in red blood cells and liver. Thus, oral GSH supplementation not only increases body stores of GSH but a fraction is stored as GSSG, and may be utilized for detoxification of free radicals. These results strongly suggest that GSH supplementation results in a systemic improvement of the redox state in diabetic individuals. Augmentation of antioxidant reserves, in the form of elevated GSH levels, also resulted in significant reduction in accumulation of oxidative DNA damage which is implicated in pathophysiology of diabetic complications.
HbA1c levels typically fluctuate despite regular anti-diabetic treatment in diabetic patients. We found GSH supplementation helped stabilize lowered HbA1c within three months. This effect was more pronounced in elderly patients, over 55 years of age. Other characteristics of the glycemic state, FPG, PPG, FPI, and PPI did not change in the full population of diabetic patients; however, interestingly we observed an increase in FPI levels in elderly diabetic patients. These results highlight that GSH supplementation distinguishes between the fine structure of glycemic changes, that is, while it influences long-term glycemia, as reflected in the stability of lowered HbA1c, short-term glycemic measurements, such as FPG and PPG, are unaltered. The exact mechanism by which GSH helps in maintaining normoglycemia in diabetic patients requires further investigation.
Preserving β-cell function is essential to glucose control in diabetic patients (DeFronzo and Abdul Ghani, 2011; Page and Reisman, 2013). It is crucial to maintain a healthy redox state of pancreatic β-cells as their ability to secrete insulin in response to glucose is dependent on intracellular and membrane thiols (Anjaneyulu et al., 1882). It is well established that β-cells are more vulnerable than other cells to hyperglycemia-mediated ROS due to their low antioxidant capacity and a poor ability to rectify oxidatively damaged DNA (Tiedge et al.,1997, Modak et al.,2009; Modak et al., 2014). Thus, one potential strategy towards improving glucose-stimulated insulin secretion is to provide antioxidant support to pancreatic β-cells. Enhancing extracellular GSH levels have been shown to improve β-cell response to glucose in rats (Ammon et al., 1989). These results were later confirmed by Paolisso et al.(1992a) who demonstrated that infusion with GSH enhanced β-cell response to glucose and consequently improved glucose tolerance in patients with impaired glucose tolerance. However, in routine clinical settings GSH infusion is not practical. We, therefore, sought to examine the effectiveness of oral GSH supplementation in ameliorating hyperglycemia in diabetic patients. Our results indicate that oral GSH supplementation supports anti-diabetic treatment in reducing hyperglycemia.
It is known that concentration of GSH declines with ageing (Matsubara and Machado, 1991; Sekhar et al 2011a), and this could be further aggravated in elderly diabetic patients. We indeed observed that elderly diabetic patients benefited more from GSH supplementation both in terms of reducing oxidative DNA damage and improving glycemic status.
Interestingly, we also observed a significant increase in the levels of FPI in these elderly patients. Similar observations have recently been reported by Zhang et al. (2019) in diabetic rats where ROS-induced damages to β-cell were prevented by administration of oral GSH. Islets isolated from type 2 diabetic cadaveric organ donors showed impairment in insulin secretion in response to glucose and increased level of oxidative damage markers; treating these islets with GSH led to an improvement in their functionality and also alleviated oxidative damage markers, suggesting that reducing OS in islets could be a potential target for treating type 2 diabetes (Del Guerra et al., 2005). We speculate that a systemic increase in GSH levels in diabetic patients resulted in significant reduction in oxidative DNA damage leading to an improvement in the insulin secreting ability of pancreatic β-cells and a concomitant reduction in HbA1c. However, these results need to be further validated in large clinical settings.
Conclusions
Our results strongly suggest that oral GSH supplementation replenishes the body stores of GSH and significantly reduces oxidative DNA damage in diabetic patients. It also reduces HbA1c within three months and stabilizes it thereafter in diabetic population overall. Elderly sub-group seems to benefit the most as evidenced by a significant decrease in HbA1c and increase in insulin secretion by β-cells over a period of six months. A clinical implication of our study is that oral administration of GSH can be used as an adjunct therapy to anti-diabetic treatment in achieving better glycemic targets, especially in the elderly population.
Authors statements
Conflict of interest
The authors declare that they have no conflict of interests.
Authors’ contributions
SK collected the samples and performed the biochemical assays. JA designed the biochemical assays, supervised the data collection and wrote the manuscript. VG, UD, and SK helped in the recruitment of study participants. AK and PG analyzed the data and performed the statistical analysis. SSG and PG contributed to the design and implementation of the study and editing of the manuscript.
Funding
This work was financially supported by XIIth Plan-Innovation Grant (University Grants Commission (UGC), Savitribai Phule Pune University, Pune. We also acknowledge partial financial support from UGC-Centre for Advanced Studies (CAS) and Department of Science and Technology-Promotion of University Research and Scientific Excellence (PURSE) program of the Department of Zoology, Savitribai Phule Pune University. SK is a recipient of a Junior Research fellowship from the Council of Scientific and Industrial Research (CSIR), India. AK is financially supported by DST Inspire, Government of India.
Availability of data and material
All datasets generated during and/or analyzed during the current study are not publicly available but are available from the corresponding author on reasonable request.
Acknowledgements
We thank all patients for their whole-hearted participation in the study. We thank Prof. Satyajit Rath for reading and providing critical comments on the manuscript. We acknowledge the financial help from all the funding agencies mentioned above.
Footnotes
↵† These authors share first author position.
References




Reviews and Context
0
Comment
0
TRIP Peer Reviews
0
Community Reviews
0
Automated Services
0
Blogs/Media
Author Videos