
Abstract
Background Covid-19 has caused significant global mortality. Multiple vaccines have demonstrated efficacy in clinical trials though real-world effectiveness of vaccines against Covid-19 mortality in clinically and demographically diverse populations has not yet been reported.
Methods We used a retrospective cohort assembled from a cross-institution comprehensive data repository. Established patients of the health care system were categorized as not immunized, partially immunized, or fully immunized against SARS-CoV-2 with an mRNA vaccine through April 4, 2021. Outcomes were Covid-19 related hospitalization and death.
Results Of the 91,134 established patients, 70.2% were not immunized, 4.5% were partially immunized and 25.4% were fully immunized. Among the fully immunized 0.7% had a Covid-19 hospitalization, whereas 3.4% among the partially immunized and 2.7% non-immunized individuals were hospitalized with Covid-19. Of the 225 deaths among Covid-19 hospitalizations, 219 (97.3%) were in the not immunized, 5 (2.2%) in the partially immunized, and 1 (0.0041%) in the fully immunized group. mRNA vaccines were 96% (95%CI: 95 — 99) effective at preventing Covid-19 related hospitalization and 98.7% (95%CI: 91.0 — 99.8) effective at preventing Covid-19 related death when participants were fully vaccinated. Partial vaccination was 77% (95%CI: 71 — 82) effective at preventing hospitalization and 64.2% (95%CI: 13.0 — 85.2) effective at preventing death. Vaccine effectiveness at preventing hospitalization was conserved across subgroups of age, race, ethnicity, Area Deprivation Index, and Charlson Comorbidity Index.
Conclusions In a large, diverse cohort in the United States, full immunization with mRNA vaccines was highly effective in the real-world scenario at preventing Covid-19 related hospitalization and death.
Introduction
The Covid-19 pandemic has caused great suffering and mortality across the globe since the pathogen Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) emerged late in 2019. The United States (US) has been disproportionately affected by SARS-CoV-2 in terms of mortality and according to preliminary mortality data, Covid-19 was the third leading cause of death in the US in 2020 with 91.5 deaths per 100,000 of the population or 11.3% of all deaths.1 Due to the Covid-19 pandemic, life expectancy in the US dropped by one full year in 2020 comparing to 2019.2 Vaccines against SARS-CoV-2 remain the most effective means to stymie the morbidity and mortality attributable to this virus and curb its global spread. Three vaccines currently have currently received emergency use authorization in the US—all with high vaccine efficacy in clinical trials.3-5
The real-world effectiveness of Covid-19 outside of clinical trials is needed to inform clinical and policy decisions. The reporting of real-world effectiveness, particularly against severe forms of Covid-19 requiring hospitalization or leading to mortality, may also help alleviate some hesitancy around vaccination. The United States’ experience with Covid-19 vaccines represents an important opportunity for the study of vaccine effectiveness due to the high burden of Covid-19, the high prevalence of underlying comorbidities, and the diverse population. The US, compared to many other countries, has administered earlier mass Covid-19 vaccination programs which allows for longer follow-up time. Prior real-world cohort studies have not addressed the impact of Covid-19 vaccination on mortality after full vaccination. Estimating the vaccines’ effectiveness at reducing Covid-19 mortality remains an important question as the clinical trials that allowed for their approval did not have large enough sample sizes to precisely estimate mortality benefit from vaccination. To address this question, we assembled a large diverse retrospective cohort from a single health care system in the US.
Methods
Study Setting and Population
Houston Methodist (HM) is an expansive healthcare system serving a socio-economically diverse population across the 9-county greater Houston metropolitan area. The system comprises eight tertiary care hospitals and a large primary care network that has regionally been on the forefront across various phases of the Covid-19 pandemic. We established an Electronic Health Record (EHR) driven, cross-institutional comprehensive data repository (COVID-19 Surveillance and Outcomes Registry or CURATOR) early in the pandemic to support Covid-19 related outcomes research across several clinical domains. The CURATOR is approved by HM institutional review board (PRO 00025445:1, dated: April 13, 2020). Details of CURATOR design, data collection, validation, and informatics infrastructure have been published.6 Briefly, CURATOR comprises a testing and a vaccination cohort. Individuals of all ages, sexes, races and ethnicities who were tested (molecular, antigen or serological tests regardless of test results) across the HM system are included in the testing cohort. The vaccination cohort includes data on all individuals who have been administered either one of the three US Food and Drug Administration (FDA) approved Covid-19 vaccines under emergency use authorization (EUA). CURATOR captures detailed sociodemographic, comorbidity, hospitalization treatment, complications, clinical course, and outcomes variables. Furthermore, CURATOR houses longitudinal data on all prior and subsequent hospital and outpatient encounters for the included testing and vaccination cohorts. In this cohort, we identified established HM patients (described subsequently) for whom comprehensive follow-up data were available.
Study Design
Houston Methodist rolled out Covid-19 vaccination across all of its hospitals simultaneously starting December 15, 2020. We identified individuals in CURATOR who had at least one hospitalization and one outpatient or emergency department encounter before December 15, 2020 and categorized them as established HM patients. We evaluated this cohort of established HM patients for vaccination status with either one of the two mRNA Covid-19 vaccines from December 15, 2020 to April 4, 2021. Type of vaccine, vaccination status (either single or both doses), and dates of vaccine administration were included.
We categorized individuals as fully immunized if they had received two doses of an mRNA vaccine and 7 days had passed after the receipt of the second dose. Individuals were considered partially immunized if they had received one dose of the vaccine and 14 days had passed. The partially immunized group also included individuals who did not receive the second dose by the end of the study period. We intentionally characterized the exposure variable as full, partial, and no immunization as opposed to the number of doses because the expected effectiveness of vaccines does not only depend on the number of doses but also the amount of time elapsed since receiving each of these doses.
Our primary outcomes of interest were Covid-19 associated hospitalizations and in-hospital deaths. Covid-19 associated hospitalizations were defined on the basis of final primary discharge diagnosis International Classification of Disease, Tenth Version (ICD-10) code for Covid-19 (U07.1). All deaths among these hospitalizations were counted as Covid-19 associated deaths. Among those admitted after a single dose, if hospitalization occurred > 14 days post-vaccination and during this admission the patient died, the death was counted towards partial immunization; if hospitalization occurred ≤14 days post-immunization it was counted with not-immunized. Similarly, among those admitted after the second dose, if hospitalization occurred > 7 days post-vaccination and during this hospitalization the patient died, the death was counted towards full immunization, if hospitalization occurred ≤ 7 days it was counted with partial immunization.
Persons were excluded if they received vaccine other than the two primary mRNA Covid-19 vaccines being used by the health system: 25,828 BNT162b2 or mRNA-1273. Demographics (age, sex, race, ethnicity, area deprivation index [ADI], zip code-based income), risk factors (tobacco/alcohol use and obesity) and comorbidities included in the Charlson comorbidity index (CCI) were obtained from CURATOR for the included study participants. No study participants had missing data on vaccination and outcomes. Missing data for covariates are reported and complete case analyses were utilized for adjusted estimates.
Statistical Analysis
Descriptive summary statistics are provided as frequencies, proportions with 95% confidence intervals (CI), means (standard deviations [SD]) or medians with interquartile range (IQR). We fit multivariable cox-proportional hazard models adjusted for age, sex, race, ethnicity, ADI and CCI and report hazard ratios (HR) with 95% CI for hospitalization risk associated with various immunization states. Vaccine effectiveness (VE) was calculated as 1 – HR. VE across various age, race, ethnicity, ADI and CCI sub-groups was also evaluated. Evolution of odds ratios (OR) over time was determined to estimate the risk of hospitalization associated with cohort transition across states of partial and full immunization during the study period. Owing to the small number of Covid-19 mortality events, OR and VE (1 – OR) were reported among the fully and partially immunized cohorts (compared to unimmunized) without any adjusted analyses. All analyses were performed in a statistical computing environment supported by R (version 3.6.1) and Python. Python packages lifeline version 0.25.10 were used for time-to-event analyses.
Results
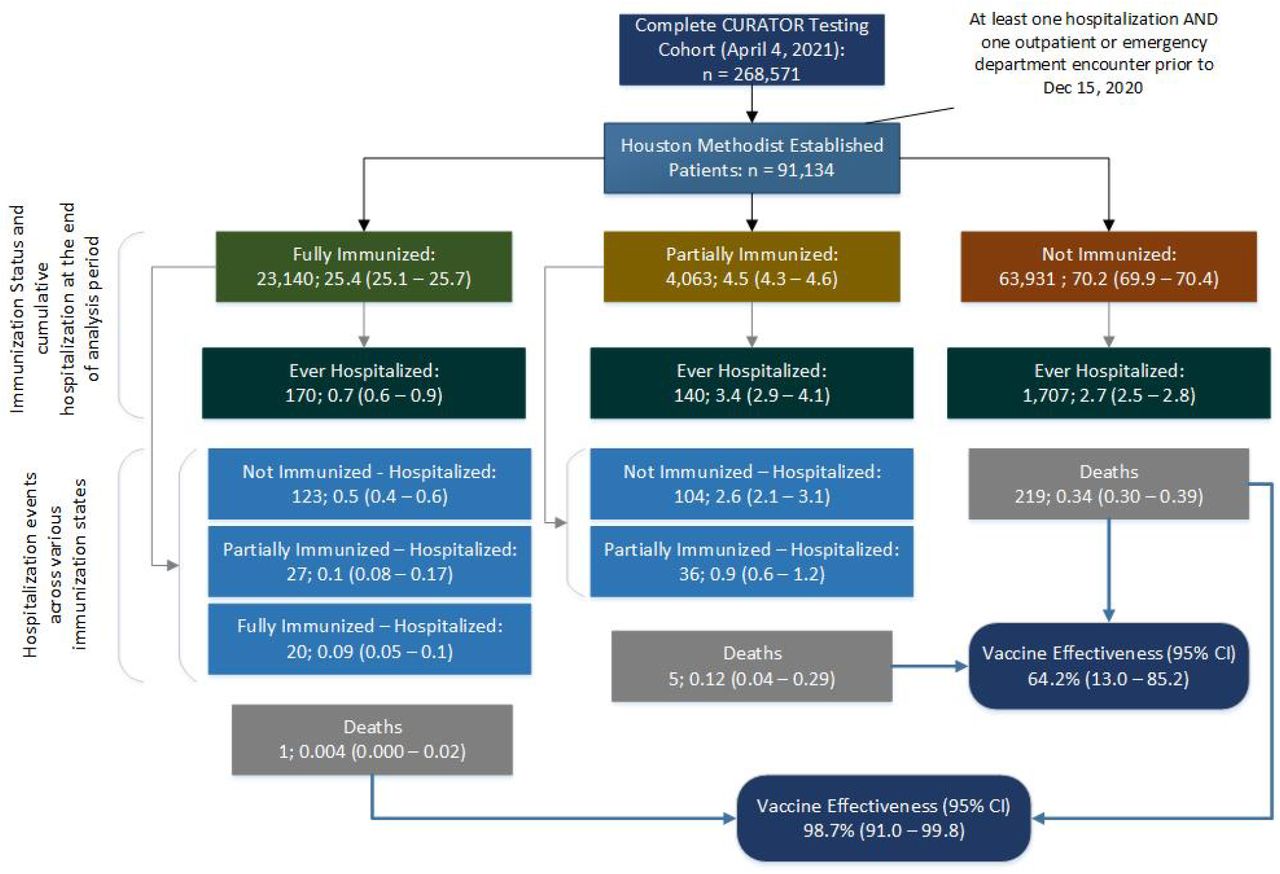
Of the 268,571 people in the testing cohort, 91,134 were identified as established patients of the health system. Twenty-five individuals were excluded who had received the JNJ-78436735 viral vector vaccine manufactured by Johnson & Johnson. By the end of the study period, 23,140 (25.4%) people were fully immunized, 4,063 (4.5%) were partially immunized and 63,931 (70.2%) were not immunized. Figure 1 provides a schematic representation of included individuals, their final immunization status, and frequencies along with proportion and 95% CI of hospitalization and death events broken down by concurrent immunization status.

Cohort members are described by their immunization status and hospitalization at the end of the study period ending March 26, 2021. Percentages compare this population to the total established patients. Each group is then divided into when hospitalized events occurred across immunization status. These percentages compare the number of events to the population in the immunization status at the end of the analysis period.
Baseline socio-demographic characteristics and comorbidity profile of fully immunized, partially immunized, and unimmunized, participants are reported in Table 1. Fully immunized individuals were older, (mean [SD] age 66.0 [15.1] years) compared to the partially immunized (60.7 [13.3] years) and not immunized (54.7 [20.1] years). Also, fully immunized individuals had higher levels of cardiovascular, cerebrovascular, metabolic, and renal comorbidity burden as demonstrated by an overall higher CCI median (IQR); 6 (3 – 9) among the fully immunized compared to 4 (2 – 8) among partially immunized and 3 (1 – 7) among the unimmunized.
Socio-demographic, Risk Factors, Comorbidities and Outcomes Among Fully, Partially and Not Immunized Groups
Overall, 28,988 first doses of the two mRNA vaccines were administered in the included cohort, some of which were counted in the unimmunized group, as the 14-day partial immunization threshold had not been achieved. Of these, 26,312 (90.8%) were for the BNT162b2 vaccine whereas 2,676 (9.2%) represent the mRNA-1273.351 vaccine.
Vaccine effectiveness for Covid-19 Hospitalizations
During the study period, a total of 2,017 (2.2%) patients were hospitalized for Covid-19. Among the fully immunized 0.7% (95% CI: 0.6 – 0.9) had a Covid-19 hospitalization; whereas 3.4%(95% CI: 2.9– 4.1%) among the partially immunized and 2.7% (95% CI: 2.5 – 2.8) non-immunized individuals were hospitalized with Covid-19 (Figure 1).
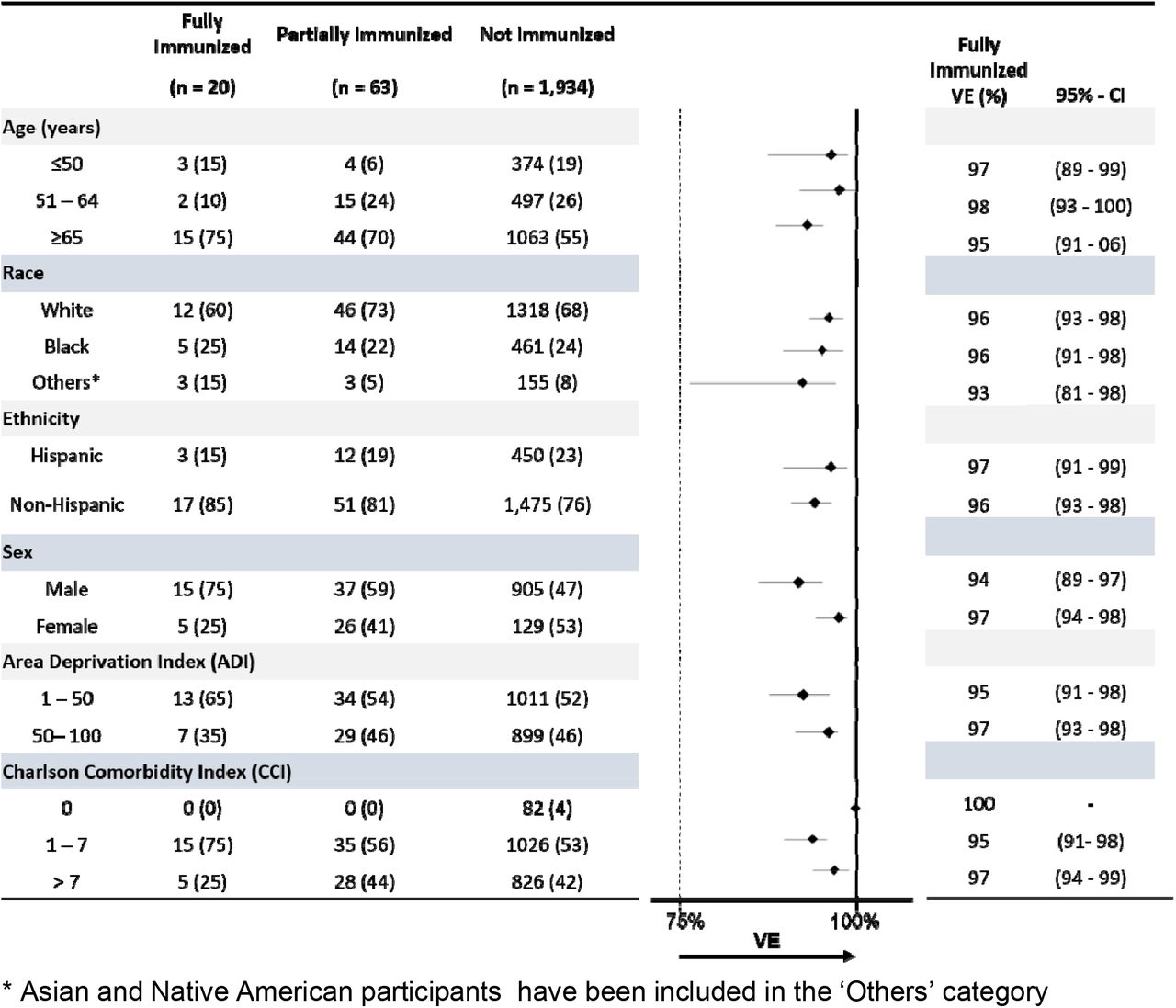
Figure 2 presents the cumulative incidence (1 - Kaplan-Meier risk) curves (95% CI) across the full, partial and unimmunized states and the number at risk and cumulative hospitalizations per week. In the proportional hazards model adjusted HR (95% CI) for Covid-19 hospitalization among the fully immunized (vs. unimmunized) was 0.04 (0.01 – 0.05) and the partially immunized (vs. unimmunized) was 0.23 (0.18 – 0.29) (Table 2). This translated into 96% (95% CI: 95 –99) VE against Covid-19 hospitalization among the fully immunized group and 77% (95% CI: 71–82) VE against Covid-19 hospitalization among the partially immunized group. The rolling time-dependent, cumulative vaccine effectiveness (VE: 1 - OR) and 95% CI for the partially and fully immunized groups vs. the not immunized demonstrates consistent vaccine effectiveness over time (Supplemental Figure 1). In the sub-group analysis for the fully immunized cohort, VE against Coivd-19 hospitalization was ≥ 93% for all subgroups and was conserved across age, race, ethnicity, ADI, and CCI subgroups. (Figure 3).

The number of patients at risk per week and the cumulative number of hospitalizations are also shown.
{kind=link}
{kind=link}
{kind=link}
Disaggregation of hospitalization cases for the fully, partial, and unimmunized cohorts is presented in the left part of the figure and VE (95% CI) for the fully immunized cohort in the right one.
Vaccine Effectiveness for Covid-19 deaths
Overall, 225 deaths among Covid-19 hospitalizations were observed in the cohort, 219 (97.3%) in the unimmunized, 5 (0.12%) in the partially immunized, and 1 (0.004%) in the fully immunized group. The VE to prevent death for full immunization (vs. unimmunized) was 98.7% (95%CI: 91.0–99.8). For the partially immunized compared to the not immunized, the VE was 64.2% (95%CI: 13.0–85.2). Comparing full or partial immunization to not immunized, the VE was 93.6% (95%CI: 85.6–97.1) against Covid-19 mortality among the partially or fully immunized (Table 2).
Discussion
This is the first large study to examine the real-world effectiveness of Covid-19 vaccinations at preventing hospitalizations and death in the US. Moreover, this is the first study anywhere to evaluate the impact of full immunization on Covid-19 mortality. The two mRNA Covid-19 vaccines were highly protective against hospitalization and death especially in those who were fully immunized.
In our analyses, mRNA vaccines were 96% (95%CI: 95 –99) effective at preventing Covid-19 related hospitalization and 98.7% (95%CI: 91.0–99.8) effective at preventing Covid-19 related death when participants were fully immunized. Partial immunization, defined as hospitalization more than 14 days after dose 1 of an mRNA vaccine through 7 days after dose 2, was found to be 77% (95%CI: 71-82) effective at preventing hospitalization and 64.2% (95%CI: 13.0-85.2) effective at preventing death.
Compared with other studies published previously on Covid-19 VE, ours has several advantages and fills several gaps in the current understanding of Covid-19 vaccination. While prior studies in the US have looked at partial vaccination7 or specific subgroups of the population such as healthcare workers8 or skilled nursing facility residents7, our study had a broad and diverse population base that is more representative of the population at large. The study by Hyams et al. examined vaccines administered in the United Kingdom, including the BNT162b2 vaccine, reported VE after one dose of the vaccine not after the complete vaccine series9. This study specifically looked at preventing hospitalization specifically in patients over 80 years of age, as opposed to the population at large or the VE at reducing mortality. Separately in Israel, Dagan and colleagues reported a 74% effectiveness at preventing hospitalization and a 72% effectiveness at preventing death with partial vaccination.10 Full vaccination was 87% effective at preventing hospitalization and 92% effective at preventing severe disease. Our study adds value by evaluating VE for preventing death for both partial and full vaccination.
There has been considerable public discussion of increasing vaccine access by administering a single dose of a two-dose vaccine or at least delaying the second dose. Prior studies of VE in the US looked at the impact of partial immunization and full immunization on Covid-19 in certain special populations. Our findings suggest that partial immunization (i.e., receipt of one dose of an mRNA vaccine) is associated with reduced protection against severe disease leading to hospitalization and poor outcomes such as in-hospital mortality. While we document lower effectiveness against mortality, the estimates are imprecise due to the small number of outcome events. However, the point estimate of effectiveness against mortality as well as VE against hospitalization suggest that policy-makers should account for the lower level of protection against severe outcomes vs. the ability to cover a higher number of individuals while recommending a single-dose strategy for two-dose vaccines.
Vaccine equity remains a vital component of Covid-19 vaccine research, distribution, and administration. Black and Hispanic communities have been disproportionately affected by Covid-19 with higher rates of cases, hospitalizations and mortality.11 Our data provide reassuring evidence of VE achieved with full immunization against Covid-19 hospitalizations across various age, race, ethnicity, Area Deprivation Index and Charlson Comorbidity Index subgroups.
The arrival of widespread vaccination in the United States occurred in parallel with the arrival of new variants of SARS-CoV-2, notably B.1.1.7. During this study period, the most common lineages were B.1, B.1.2, and B.1.596 in the United States, although the B.1.1.7 variant has been increasing steadily since mid-February.12 In Texas, variant B.1.1.7 was 7.1% of variants and B.1.427/B.1.429 was 7.3% of variants in the four week period before February 27, 2021.12 Though the mRNA vaccines appear to make neutralizing antibodies to the mutated spike protein of B.1.1.713, the effectiveness of these vaccines remains to be demonstrated for this and the other emerging variants.
Limitations of this study include its observational design, as there may have been some differences in testing behavior between those who were unvaccinated, partially vaccinated and fully vaccinated that are unaccounted for in this analysis. For example, there may have been differences in health-seeking behavior between these groups or different thresholds to test for SARS-CoV-2 amongst clinicians. However, it is unlikely there were large differences in hospitalization rates based on behavior alone. Across the pandemic timeline, the criteria for hospitalization have been consistently based on risk stratification by evaluation of the severity of symptoms, comorbidities, diagnostic findings and pulse oximetry. Second, as this is an observational study, there may be some residual unmeasured confounding, however, this is unlikely to alter the overall interpretation. It is also possible that certain individuals in the established cohort may have been tested and/or hospitalized elsewhere in the region. However, our healthcare system has a relatively high rate of patient retention. For example, in the overall tested cohort in CURATOR, > 95% have had at least one prior healthcare system encounter. Overall the vaccine effectiveness seen in this study was similar to the vaccine efficacy of clinical trials, which is reassuring. Finally, this study only examined two of the three vaccines currently approved for use in the US due to the timing of the study. It will be important going forward to study the real-world effectiveness of the different Covid-19 vaccines approved in the US and across the globe.
Conclusion
To date, this is the largest Covid-19 VE cohort study in the US. In this diverse and well-characterized cohort, we show Covid-19 vaccines have a large impact in reducing Covid-19 hospitalization and mortality. Vaccines remain the central tool for disease control strategies and so ensuring broad and equitable access to vaccines remains imperative for pandemic control moving forward.
Acknowledgments
The authors would like to acknowledge infrastructural, material and financial support provided by Houston Methodist and the Houston Methodist Academic Institute for the COVID-19 Surveillance and Outcomes Registry (CURATOR). This study was partially funded by the Yale Institute for Global Health.
Footnotes
COI: The authors do not report any conflicts of interest,



