
Abstract
Introduction COVID-19 vaccine hesitancy increased among US adults April-December, 2020, and threatens efforts to end the pandemic. Among US adults 18-64 years, we report prevalence of and reasons for vaccine hesitancy, overall and by employment and occupation, during the COVID-19 vaccine rollout.
Methods The Delphi Group at Carnegie Mellon University conducted a COVID-19 survey administered by Facebook. In January, February and March, 2021, 791,716, 710,529, and 732,308 Facebook users, respectively, reported age 18-64 years and answered a vaccine acceptance question. Weights matched the sample to the age, gender, and state profile of the US population. Percentages and risk ratios (RR) for vaccine hesitancy were estimated using a weighted Poisson regression; 95% confidence intervals (CI) were calculated using robust standard errors.
Results Vaccine hesitancy decreased among adults 18-64 years from January (27.5% [95%CI, 27.3-27.6]) to March (22.1% [95%CI, 21.9-22.2]). Vaccine hesitancy varied widely by occupational category: 9.6%, (95%CI, 8.5-10.7) in life/physical/social sciences to 46.4% (95%CI, 45.1-47.7) in construction/extraction. Almost half (47.9%, 95%, 47.6-48.3) of hesitant participants indicated concern about side effects, and over a third didn’t believe they needed the vaccine, didn’t trust the government, were waiting to see if it was safe, and didn’t trust COVID-19 vaccines (versus 14.5% [95%CI, 14.3-14.8] who didn’t like vaccines in general).
Conclusions In this nationally representative survey of adults 18-64 years, vaccine hesitancy decreased to 22.1% by March, 2021. Still, hesitancy, which varies widely by occupation, remains a barrier to pandemic control. Reasons for hesitancy indicate messaging about safety and addressing trust are paramount.
Introduction
Vaccine hesitancy is a barrier to ending the COVID-19 pandemic.1 Despite the increasing COVID-19 death toll,2 COVID-19 vaccine hesitancy increased among US adults April-December, 2020.3 In early December, only 56.2% reported they were likely to get vaccinated1. The likelihood was similar among healthcare workers (HCW) (55.3%)4, and lower among working-age adults (<65 years) versus older adults1. Workplace outbreaks, spread of infection from HCW to patients and from workers to customers are public health threats.5,6
The extent to which vaccine hesitancy changed during the first three months of the US COVID-19 vaccine rollout, and if and how current vaccine hesitancy varies by employment and occupation is unknown. Among a large representative sample of US adults 18-64 years, we report vaccine hesitancy by month, January-March, 2021, and for March, cumulative COVID-19 vaccine uptake and current prevalence of and reasons for vaccine hesitancy, overall and by employment status and occupation category.
Methods
Since April, 2020, the Delphi Group at Carnegie Mellon University (CMU) has been conducting an ongoing national COVID-19 survey in collaboration with the Facebook Data for Good group. Each month the survey is offered to a random sample, stratified by geographic region, of ≈100 million US residents from the Facebook Active User Base who use one of the supported languages (English [American and British], Spanish [Spain and Latin American], French, Brazilian Portuguese, Vietnamese, and simplified Chinese) via a link at the top of their Facebook News Feed to yield ≈1.3 million responders, which allows for evaluation of local trends. The CMU Institutional Review Board approved the survey protocol and instrument.
Study sample
Facebook users may be offered the survey from once a month to once every six months, depending on their geographic strata. To show trends over time in vaccine hesitancy, we used data from January 6 (date the vaccine acceptance question was initially asked in its current form) to March 31, 2021 aggregated by month. While is possible there are repeat respondents across months, respondents cannot be linked longitudinally, so data was treated as repeat cross-sectional surveys. Only March data was used in the primary analysis. In March, 104,768,154 Facebook users were offered the survey, of whom 1,291,957 completed at least two survey questions. Respondents were excluded if they did not report age 18-64 (n=558,972) or did not answer the vaccine acceptance question (n=677), leaving 732,308 participants. Applying the same criteria, the January and February samples had 791,716 and 710,529 participants, respectively.
Measures
The survey questions and response sets utilized in this report are provided in an appendix (supplemental material). Participants age 18-64 were categorized as vaccine hesitant if they answered that they probably or definitely would not choose to get vaccinated if offered a vaccine to prevent COVID-19 today (versus probably or definitely would choose to get vaccinated or were vaccinated). Participants were categorized by employment status in the past 4 weeks, and if employed, by occupation category and profession.
Statistical analysis
Percentage vaccine hesitant by month was calculated using Facebook-provided weights, which account for the sampling design, non-response, and differences between the demographics of survey respondents and the US adult population.7 Among the March sample, weighted percentages for worked outside the home, vaccinated, and vaccine hesitant were calculated, overall and by employment variables.
Additionally, risk ratios (RR) for vaccine hesitancy by employment status and occupation category were estimated using a weighted Poisson regression. Finally, weighted percentages for reasons for hesitancy were calculated among vaccine hesitant participants overall and among occupation categories with the highest hesitancy. For all parameters, 95% confidence intervals (CI) were calculated using robust standard errors.8 Analyses were conducted in R (Version 4.0.2, R Core Team, Vienna, Austria).
Results
March participants (N=732,308) had a median age range of 35-44 years, 45.0% were male, 51.1% female, 3.8% other/unknown gender; 18.9% were Hispanic, 63.8% non-Hispanic white, 6.8% non-Hispanic black, 3.2% non-Hispanic Asian, and 7.3% mixed/other/unknown race; 76.6% had at least some college. Two-thirds (66.4%, 95%CI, 66.3-66.5) worked for pay; half (50.8%, 95%CI, 50.6-50.9) worked outside the home. Demographics were similar in January and February (data not shown).
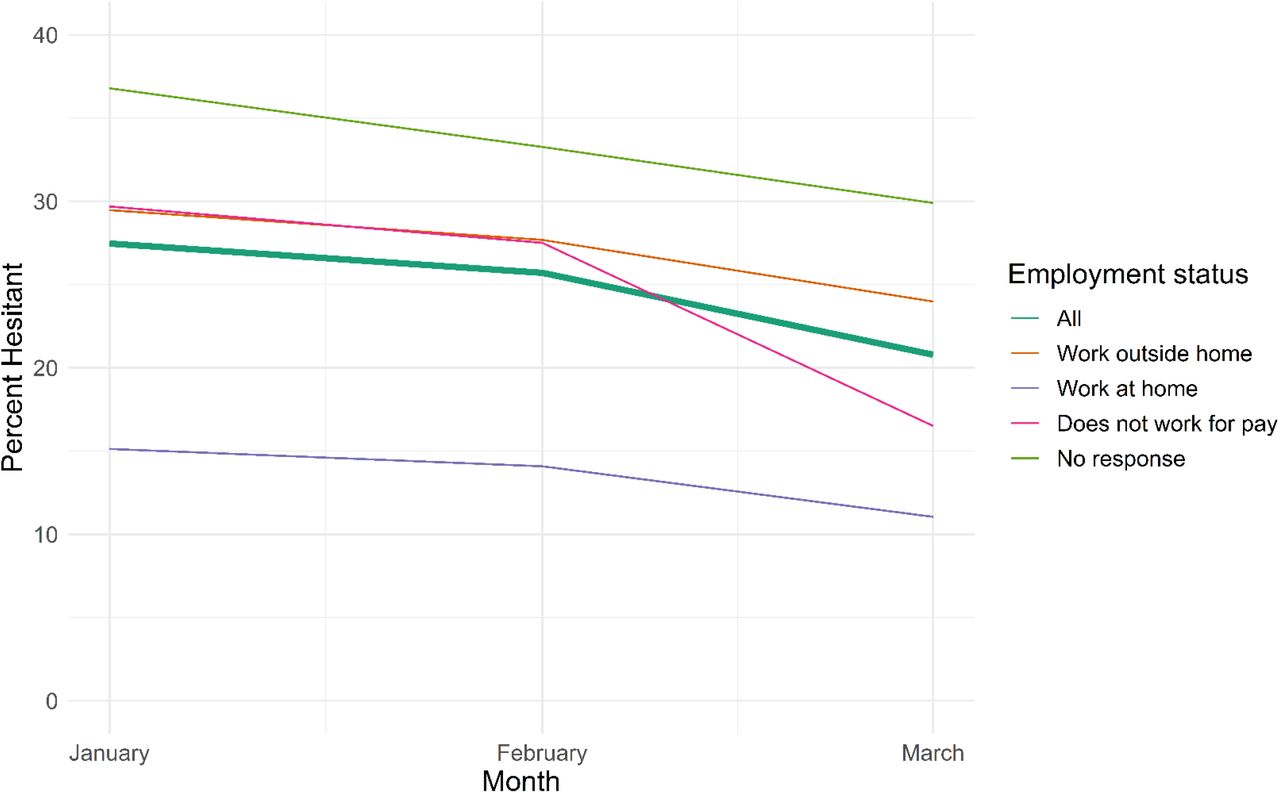
Vaccine hesitancy decreased among adults 18-64 years each month from January (27.5% [95%CI, 27.3-27.6]) to February (25.7 [95%CI, 25.6, 25.8]) to March (22.1% [95%CI, 21.9-22.2]). The time trend was similar among those who worked outside the home (January: 29.5% [95% CI, 29.3-29.7] to March: 24.8% [95%CI, 24.6-24.9]) and those who worked from home (January: 15.1% [95% CI, 14.9-15.3] to March: 11.4% [95%CI, 11.2-11.6]) (Figure 1).

{kind=link}
Vaccine hesitancy by month, 2021, overall and by employment status.
March cumulative vaccination uptake and current hesitancy by employment status and occupation category are reported in Table 1. HCW (78.3% [95%CI, 77.8-78.7] practitioners/technicians; 67.7% [95%CI, 67.0-68.3] support) and educators (68.5%, 95%CI, 68.0-69.0) led vaccine uptake, which was 38.0% (95%CI, 37.9-38.1) overall.
SARS-CoV-2 cumulative vaccination uptake and current vaccine hesitancy, overall and by employment status and category, in March, 2021, among 18-64 year old US adults.
Vaccine hesitancy varied widely by occupation category: 9.6%, (95%CI, 8.5-10.7) in life/physical/social sciences and 9.7% (95%CI,9.4-10.1) in educators to 42.6% (41.5-47.7) in installation/maintenance/repair and 46.4% (95%CI, 45.1-47.7) in construction/extraction. Several occupation categories had lower hesitancy than HCW (practitioners/technicians and support; Table 1). Among HCW, Pharmacists had the lowest hesitancy (range 8.5%, 95%CI, 6.8-10.2). Physicians (12.2% [95%CI, 11.2-12.3]) and registered nurses/nurse practitioners had relatively low hesitancy (11.7% [95%CI, 10.6-13.9]) versus licensed practical/vocational nurses (19.0% [95%CI, 17.6-20.4]). Home health/personal-care aids, medical assistants, emergency medical technicians/paramedics, and nursing assistants/psychiatric aides had the highest hesitancy (20.5% [95%CI, 19.2-21.8] to 23.1% [95%CI, 21.2-25.0]).
Reasons for vaccine hesitancy are reported in Table 2 overall and by occupation categories with at least one-third hesitant. Almost half (47.9%, 95%, 47.6-48.3) of hesitant participants indicated concern about side effects, and over a third didn’t believe they needed the vaccine, didn’t trust the government, were waiting to see if the vaccine was safe, and didn’t trust COVID-19 vaccines (versus 14.5% [95%CI, 14.3-14.8] who didn’t like vaccines in general). More than one fifth indicated allergic reaction risk, unknown efficacy and other people need more as reasons. Worry of side effects, an allergic reaction and waiting to see if safe were reported less frequently among high-hesitancy occupation categories (versus all hesitant participants), whereas lack of trust in the COVID-19 vaccine and the government, disbelief of need and dislike of vaccines were more frequent (Table 2).
Reasons 18-64 year old US adults reported vaccine hesitancy overall, and by occupational categories with the highest percentage hesitant.
Discussion
This data highlights the disparity in vaccine hesitancy by occupation. Among HCW, several professions with high patient contact (e.g., nursing assistants/psychiatric aides) reported hesitancy >20%. Occupation categories with the highest hesitancy (construction/extraction, installation/maintenance/repair, farming/fishing/forestry, transportation/material moving, and production), include some that have suffered workplace outbreaks.5 Reasons for hesitancy indicate a need for messaging about safety and addressing trust.
Limitations
Our large sample size allowed for precise vaccine hesitancy estimates by month and occupation. However, cross-sectional samples were used to evaluate time trends, and the sample representativeness may have been affected by the recruitment method and response rate, addressed with weighting.7 Compared to the [dataset] American Community Survey 2015-2019 5-year 2 Data Release9, demographics of the weighted sample are similar to the US population, but white race and higher education are slightly over-represented. Thus, overall hesitancy prevalence estimates might be underestimated.3 This should have minimal effects on time trends or comparisons between occupation categories.
Conclusion
In this nationally representative survey of adults 18-64 years, vaccine hesitancy decreased from 27.5% to 22.1% January-March, 2021. Still, hesitancy among the workforce (21.8%), which varies widely by occupation, remains a barrier to pandemic control.
Data Availability
If you are interested in using the survey data for your research, you can start the process by submitting a form requesting a data use agreement (DUA) from Facebook. The data is not available from the authors.
https://dataforgood.fb.com/docs/covid-19-symptom-survey-request-for-data-access/
Conflict of interest statement
Drs. King, Mejia and Mr. Rubenstein have no conflict of interest to report. Dr. Reinhart received salary support from an unrestricted monetary gift Facebook.
Funding/Support
This material is based upon work supported by Facebook (unrestricted gift) and a research grant from the Centers for Disease Control and Prevention (U01IP001121). Any opinions, findings and conclusions or recommendations expressed in this material are those of the authors and do not necessarily reflect the views of Facebook or the Centers for Disease Control and Prevention.
Role of the Funder
Facebook was involved in the design and conduct of the study. The CDC provided funding only. Neither Facebook nor the Centers for Disease Control and Prevention had a role in the collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; or decision to submit the manuscript for publication.
Acknowledgements
The authors would like to thank the Delphi Group at Carnegie Mellon University for input and support on the survey instrument. Wichada La Motte-Kerr, MPH, of Delphi contributed to the development and deployment of the survey and received compensation for her contributions to the study. We thank Sarah LaRocca, PhD and Katherine Morris, PhD of Facebook for contributions to the survey instrument design.
Footnotes
mrubinst{at}andrew.cmu.edu
areinhar{at}stat.cmu.edu
rmejia{at}andrew.cmu.edu



