
Abstract
SARS-CoV-2 infection is generally mild or asymptomatic in children but the biological basis for this is unclear. We studied the profile of antibody and cellular immunity in children aged 3-11 years in comparison with adults. Antibody profiles in children were strong, with high titres against Spike protein and receptor binding domain (RBD). SARS-CoV-2 seroconversion in children strongly boosted antibody responses against seasonal beta-coronaviruses, partly through cross-recognition of the S2 domain, indicating a broad humoral response that was not seen in adults. T cell responses against Spike were also >2-fold higher in children compared to adults and displayed a strong Th1 cytokine profile. SARS-CoV-2 Spike-reactive cellular responses were present in more than half the seronegative children, indicating pre-existing cross-reactive responses or prior sensitization against SARS-CoV-2. Importantly, all children retained high antibody titres and cellular responses for more than 6 months after infection whilst relative antibody waning was seen in adults. Significantly Children at this timepoint also had high antibody titres to B1.1.7, B1.351 and P1 variants. Children thus distinctly generate robust, cross-reactive and sustained immune responses after SARS-CoV-2 infection, with focussed specificity against Spike protein. These observations demonstrate several novel features of SARS-CoV-2-specific immune responses in children and may provide insights into relative clinical protection in this group. Such information on the profile of natural infection will help to guide the introduction of vaccination regimens into the paediatric population.
Introduction
The SARS-CoV-2 pandemic has resulted in over 2.8 million deaths to date and the most significant determinant of outcome is age at the time of primary infection 1. In children, SARS-CoV-2 infection is generally asymptomatic or mild and contrasts with high rates of hospitalisations and deaths among older adults 2. This natural history is unusual for respiratory viruses such as influenza where children are the main drivers of infection and transmission. As such, there is interest in understanding the profile of the immune response to SARS-CoV-2 in children. Studies of SARS-CoV-2-specific immunity in children have been limited to date but initial findings have reported reduced magnitude of both antibody and cellular responses in comparison to adults, and an absence of nucleocapsid-specific antibody responses during or early post-infection 3, 4, 5. One unique feature of SARS-CoV-2 infection in children is the development of a rare complication, known as Pediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2 (PIMS-TS), also known as paediatric multisystem inflammatory syndrome (MIS-C), which shares features with Kawasaki disease and toxic shock syndrome 6, 7. MIS-C develops approximately 2-4 weeks after infection in children with a median age of 9 years 8. The immunological basis for this condition remains unclear but is characterised by diffuse endothelial involvement and broad autoantibody production 9.
One potential determinant of differential immune responses to SARS-CoV-2 across the life course may be the timing of exposure to the four additional endemic human coronaviruses (HCoV). These comprise the beta-coronaviruses OC-43 and HKU-1, which have 38% and 35% amino acid homology with SARS-CoV-2, as well as the more distantly related alpha-coronaviruses NL-63 and 229E, each with around 31% homology 10. These coronaviruses cause frequent mild childhood infections and antibody seroconversion occurs typically before the age of 5 years. Infection with one of the Alpha or Beta viruses provides short-term immunity against re-infection from coronaviruses and believed to represent transient cross-reactive immunity within the subtypes 11, 12, 13. As such, recent HCoV infection might pre-sensitize children against SARS-CoV-2 infection and may explain cross-reactive SARS-CoV-2-neutralising antibodies in some seronegative children 14. Immune responses against HCoV are retained throughout life but do not provide sterilising immunity 12. Consequently, recurrent infections are common, generating concern that a similar pattern will be observed after SARS-CoV-2 infection.
COVID-19 vaccines are now being implemented widely in adults and vaccine trials in children are currently underway, with the aim of increasing protection across the whole population. It is, therefore, imperative to understand the baseline profile of SARS-CoV-2 specific immune responses in children to inform vaccination strategy. Here we provide a comprehensive characterisation of the convalescent humoral and cellular immune response in a cohort of 91 primary school-aged children compared with 154 adults taking part in the SARS-CoV-2 Surveillance in School Kids (sKIDs) study 15. We demonstrate a markedly different profile of immune response after SARS-CoV-2 infection in children compared to adults. These findings have potential implications for understanding immune responses to infection in children and may provide insights into PIMS-TS. Furthermore, these can also be used to guide and interpret the introduction of COVID-19 vaccination for children.
Methods
Sample collection
Public Health England (PHE) initiated prospective SARS-CoV-2 surveillance in primary schools across the UK after they reopened following the easing of national lockdown in June 2020. The protocol for the COVID-19 Surveillance in School KIDs (sKIDs) is available online (https://www.gov.uk/guidance/covid-19-paediatric-surveillance) 15. Surveillance comprised two arms, one involving weekly swabbing of primary school students and staff for SARS-CoV-2 infection (from June to mid-July 2020) and the other comprising swabbing and blood sampling taken in 3 rounds: beginning (1-19 June) and end (3-23 July) of the summer half-term when primary schools were partially re-opened, and after full reopening of all schools in September 2020, at the end of the autumn term (23 November-18 December). Samples for extended humoral and cellular analysis were taken in round 3.
For each known SARS-CoV-2 seropositive individual, an age-matched (nearest age in years for students, nearest 10 years for teachers) and gender-matched participant also underwent blood sampling. In total 154 adults and 91 children had sufficient blood sample for serology and cellular responses (Table 1).
PBMC and Plasma Preparation
Blood tubes were spun at 300g for 10mins prior to removal of plasma which was then spun again at 800g 10mins and stored at -80°C. Remaining blood was diluted 1:1 with RPMI and PBMC isolated on a Sepmate (Stemcell) density centrifugation tube, washed with RPMI and rested in RPMI+10% FBS overnight at 37°C.
MSD Serology assay
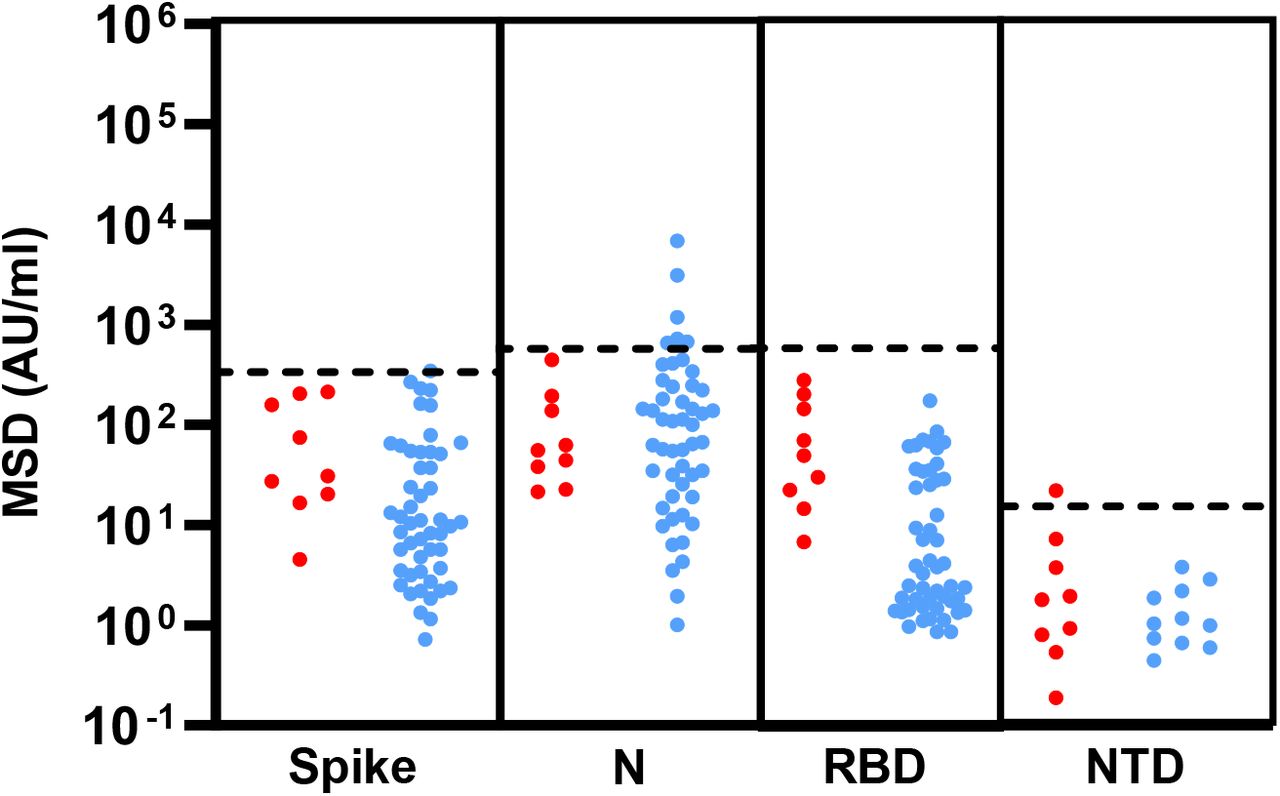
Quantitative IgG antibody titres were measured against trimeric Spike (S) protein, nucleocapsid (N) and other coronavirus using MSD V-PLEX COVID-19 Coronavirus Panel 2 (N05368-A1), Coronavirus Panel 7 (N05428A-1) responses to other respiratory viruses were measured using MSD V-PLEX COVID-19 Respiratory Panel 1 (N05358-A1). Multiplex MSD Assays were performed according to manufacturer instructions. Briefly 96-well plates were blocked. Following washing, samples diluted 1:5000 in diluent, as well as reference standard and internal controls, were added to the wells. After incubation plates were washed and detection antibody added. Plates were washed and were immediately read using a MESO TM QuickPlex SQ 120 system. Data were generated by Methodological Mind software and analysed with MSD Discovery Workbench (v4.0) software. Assay Cut-offs in respect of pre-pandemic plasma samples from healthy donors are shown in (Extended data 1). Cut-offs used are Spike; 350 AU/ml, RBD and Nucleocapsid; 600 AU/ml, NTD; 15 AU/ml.
Total IgG/A/M anti Spike SARS-CoV-2 ELISA
A total GAM anti-SARS-CoV-2 Spike ELISA kit 16 was purchased from Binding Site (Birmingham, UK). ELISA was performed following the manufacturer’s instructions. Optical density (OD) was compared to a known calibrator and expressed as a ratio to the calibrator. Samples with a ratio above 1.0 were considered sero-positive.
Cross-reactive antibody blocking
Plasma samples were pre-diluted 1:10 with PBS then pre-absorbed by adding an equal volume of either recombinant Spike S1 domain (10569-CV-100) or Spike S2 (10594-CV-100) (R&D systems) at a concentration of 500ug/ml in PBS, or PBS alone (mock). Samples were incubated at 37°C for 30min. Samples were then diluted to a final dilution of 1:5000 in MSD diluent and run on a MSD V-PLEX COVID-19 Respiratory Panel 2 plate in duplicate.
RBD-ACE-2 interaction neutralisation
The concentration of antibodies which inhibited interaction between RBD and ACE-2 was determined using a SARS-CoV-2 neutralisation assay (Biolegend), following the manufacturer’s instructions. Briefly, plasma or positive control antibody were pre-incubated with biotinylated-Fc-chimera-S1-RBD protein prior to addition of bead bound ACE-2. Binding of RBD to ACE2 was then measured by the addition of streptavidin-PE. Samples were run on a BD LSR-II flow cytometer and analysed using LEGENDplex v8.0 software (Biolegend). Results were related to a known RBD neutralising antibody standard and displayed as ng/ml.
IFNγ ELISpot
Pepmixes pool containing 15-mer peptides overlapping by 10aa from either SARS-CoV-2 Spike S1 or S2 domains and a combined pool of Nucleoprotien (N) and Membrane (M) and Envelope (E) were purchased from Alta Biosciences (University of Birmingham, UK). Overlapping pepmix from Influenza A Matrix Protein 1; California/08/2009(H1N1) ID:C3W5Z8 and Aichi/2/1968 H3N2 ID:Q67157, were purchased from JPT technologies, and combined as a relevant control.
T cell responses were determined using a IFNγ ELISpot Pro kit (Mabtech), as previously described 17. Briefly, standard fresh PBMC were rested over-night prior to assay, 0.25-0.3×106 PBMC were added in duplicate per well containing either pep-mix, anti-CD3 (positive) or DMSO (negative) control. Samples were incubated for 16-18hrs. Supernatant was harvested and stored at -80°C. Plates were developed following the manufacturer’s instructions and read using an AID plate reader (AID). Cut off values were previously determined 17.
Cytokine measurement
Supernatants from donors with a detectable response in overnight ELISpot cultures were assessed using a LEGENDplex Th profile 12-plex kit (Biolegend), following the manufactures instructions. Data was analysed using LEGENDplex v8.0 Software (Biolegend).
Intracellular Cytokine Staining
Cryopreserved PBMC were thawed and rested overnight. Cells were then stimulated with a combined Spike-S1, S2 peptide pool at a final concentration of 1μg/ml per peptide, or DMSO (Mock). After 1hr eBioscience Protein transport inhibitor cocktail (Thermofisher Scientific) was added and cells incubated for a further 5 hrs. eBioscience Cell stimulation cocktail (Thermofisher Scientific) was used as a positive control. Following stimulation cells were washed (PBS+0.1%BSA), and surface stained at 4°C, 30min. Cells were then washed and fixed in 2% paraformaldehyde. Following washing, brilliant staining buffer was added (BD Bioscience) and a final concentration of 0.4% Saponin added. Cells were stained intracellularly at room temperature for 30min. Cells were then washed and run on a BD Symphony A3 flow cytometer (BD Biosciences). Antibody details are provided in Extended Method Table 1.
Data visualisation and statistics
Statistical tests, including normality tests, were performed as indicated using Graphpad Prism v9 software. Only results found to be significant (p<0.05) are displayed.
Results
Children develop strong and broad antibody responses after SARS-CoV-2 infection
Blood samples were obtained from 91 children and 154 adults, including 35 children and 81 adults known to be seropositive in previous rounds of testing. The median age of the children was 7 years (range, 3-11) whilst that of adults was 41 years (range, 20-71). SARS-CoV-2 antibody profile was assessed using the MSD V-plex serology platform to determine serological responses against Spike, Receptor Binding Domain (RBD), N-terminal domain (NTD) and Nucleocapsid (N). In total, 47% of children and 59% of adults were found to be seropositive (Extended Data Table 1).
*Seropositive/negative defined by 1. MSD-anti-Spike titre, 2. MSD-anti-Spike or prior PHE seropositive or total IgG/A/M anti-Spike ELISA. 3. PHE sKIDS prior positive (June-July 2020). N.d. – not detected.
Seropositive children and adults demonstrated broadly similar antibody responses against the viral proteins. Geometric mean antibody titres against all four regions were, however, higher in children, most notably against the NTD and RBD domains, which showed 2.3-fold and 1.7-fold increases respectively, although these did not reach statistical significance. (Figure 1A). In contrast to previous reports 3 we observed a coordinated response against nucleoprotein, with a 1.3-fold increased antibody titre compared to adults (Figure 1 A&B).
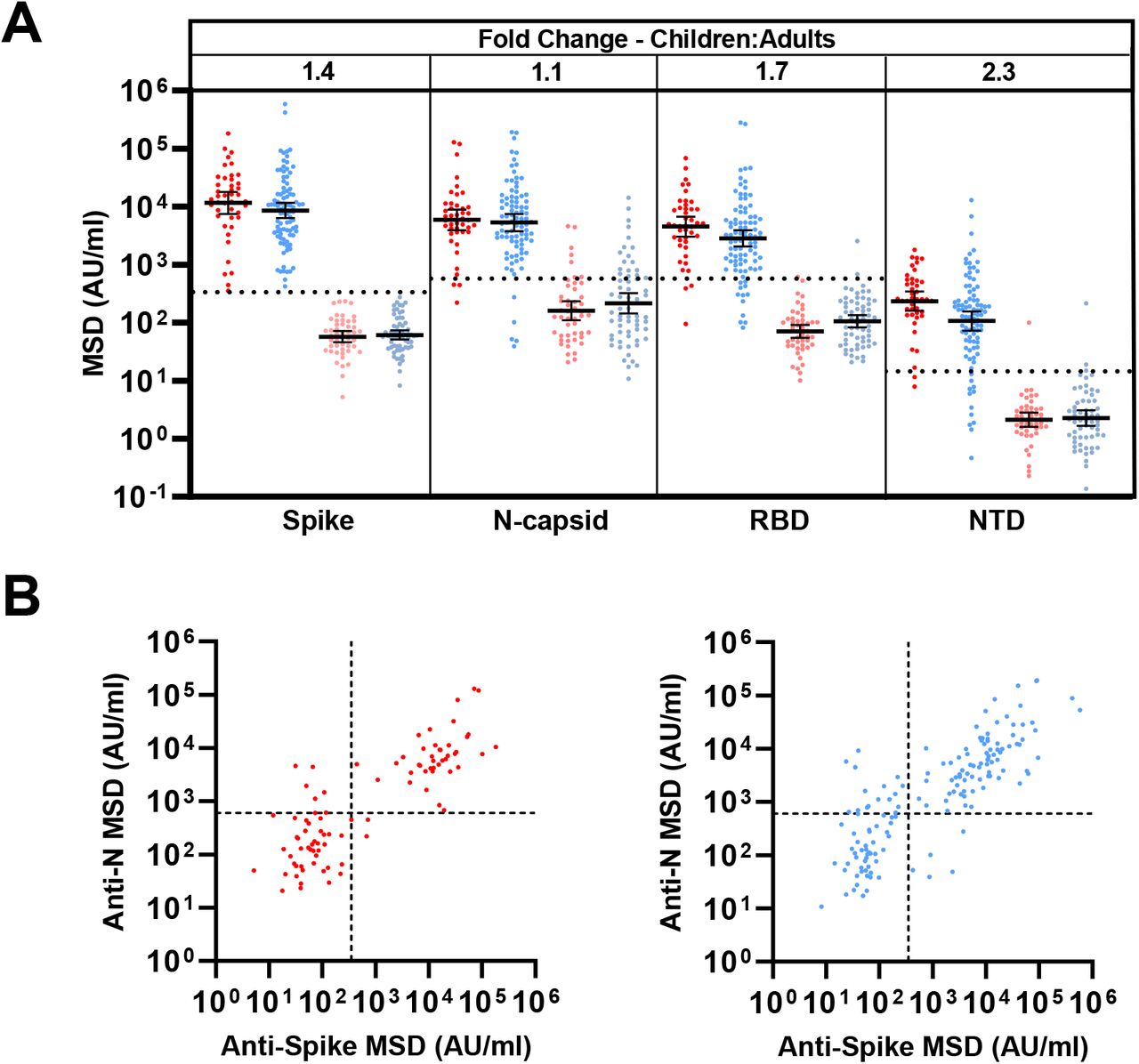
A) SARS-CoV-2 antibody levels determined by MSD assay, serostatus was determined based upon Spike serology and used to divide the cohorts into seropositive (red/blue) and seronegative (light red/blue). Dotted lines represent cut off values for serostatus. Fold change indicates the difference between the geometric mean titres in seropositive children and adults. Bars indicate geometric mean, with 95% CI.
B) The level of anti-Spike and anti-nucleocapsid were compared within the whole cohorts showing coordinated responses.
SARS-CoV-2 infection strongly boosts antibodies responses against HCoV in children
Pre-existing immune responses against seasonal coronaviruses might act to modulate clinical outcome following primary SARS-CoV-2 infection, and cross-reactive neutralising antibodies have been reported in SARS-CoV-2-seronegative children 14. Consequently, we compared antibody levels against the four HCoV in SARS-CoV-2 in seronegative and seropositive children and adults.
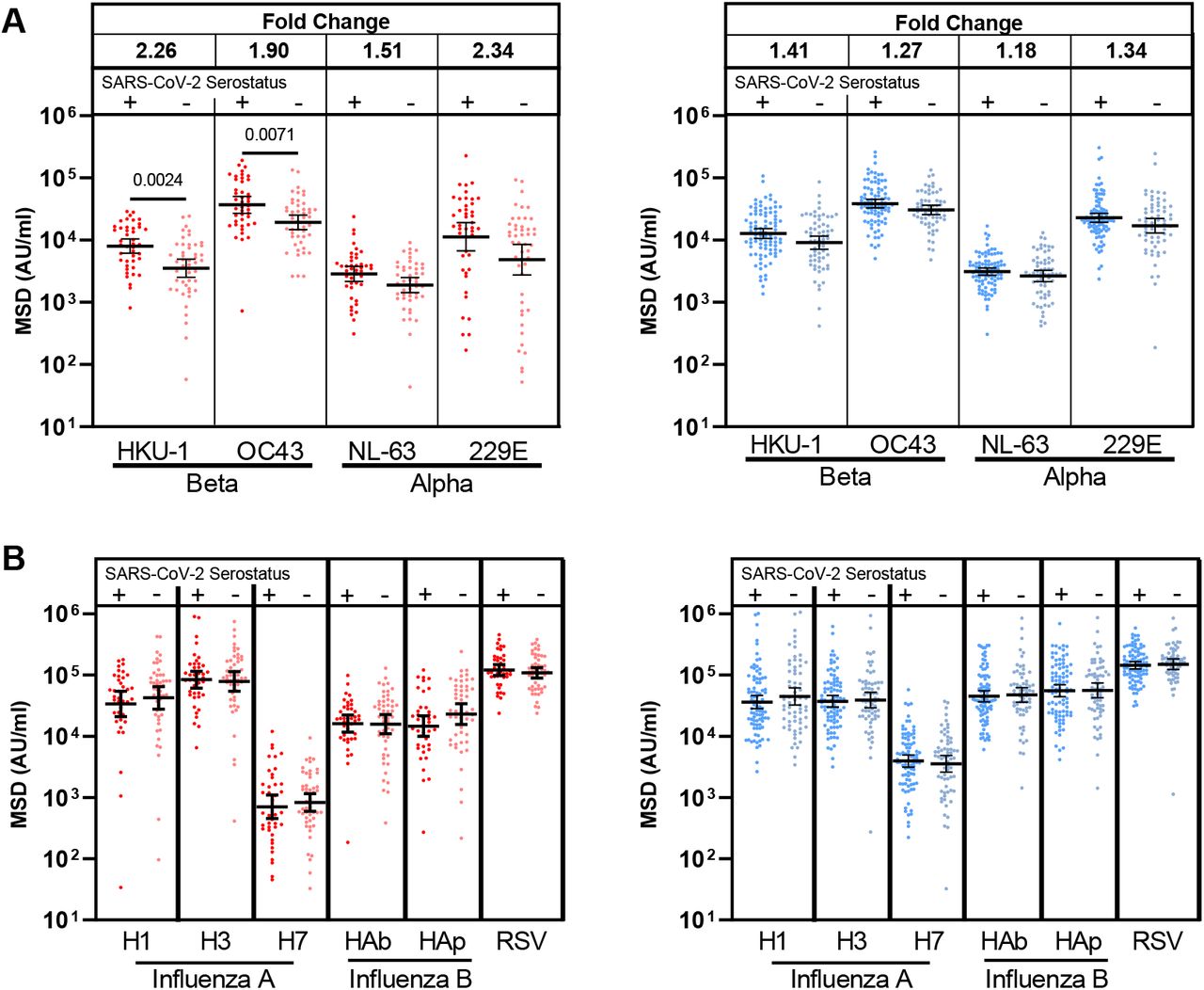
A 1.2 to 1.4-fold increase in the titre against HCoV was evident in SARS-CoV-2 seropositive adults compared to the seronegative group. In contrast, antibody levels against all four viruses were markedly higher in SARS-CoV-2 seropositive children, with 2.3, 1.9, 1.5, and 2.1 fold higher antibody levels compared to the seronegative group. These were significant for OC-43 and HKU-1 (p=0.0071, p=0.0024 Brown-Forsythe and Welch ANOVA, with Dunnett’s T3 multiple comparison test) (Figure 2A).
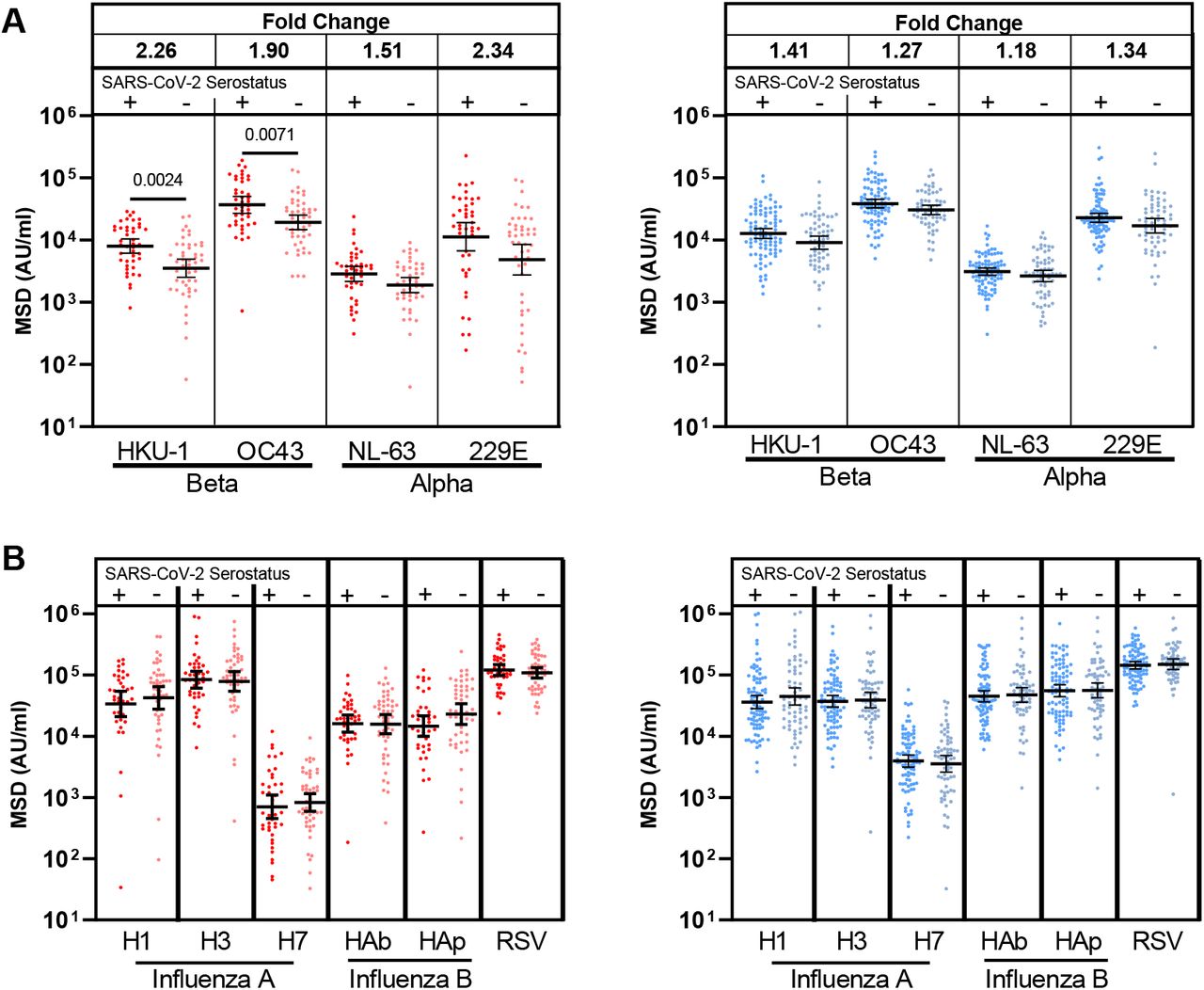
Antibody titres to the seasonal coronavirus (A)and other respiratory viruses (B) by MSD in children (red) and adults (blue) based on serostatus (dark – seropositive, light-seronegative). Fold change indicates the difference between the geometric mean titres in seropositive children and adults. Bars indicate geometric mean, with 95% CI. Only significant differences are shown. Brown-Forsythe and Welch ANOVA, with Dunnett’s T3 multiple comparison test.
In order to assess if this effect was specific to HCoV or represented a more general effect of SARS-CoV-2 infection on antibody responses against heterologous infection, we also examined antibody titres against influenza subtypes and respiratory syncytial virus (RSV) in relation to SARS-CoV-2 serostatus. No significant change in antibody titre against these viruses was seen in either children or adults (Figure 2B). These data show that SARS-CoV-2 infection in children strongly and specifically boosts humoral responses against HCoV.
SARS-CoV-2-specific antibodies in children can cross-react with the S2 domain of betacoronaviruses
Given the large increase in HCoV-specific antibody titres following SARS-CoV-2 infection in children, we were interested to assess to what extent this was cross-reactive against SARS-CoV-2 or could represent a HCoV-specific response. As such, we used recombinant S1 or S2 domains from SARS-CoV-2 to pre-absorb plasma samples prior to assessment of antibody levels to both SARS-CoV-2 and the four HCoV subtypes.
As expected, both the S1 and S2 domains significantly reduced antibody titres against total spike (p<0.0001, p0.0024 respectively, Friedman test with Dunn’s multiple comparisons test). The S1 domain but not the S2 domain, absorbed RBD and NTD-specific antibodies against SARS-CoV-2 whilst no influence was observed in relation to nucleocapsid-specific binding for either domain (Figure 3). Of note, the S1 domain did not significantly reduce antibody binding to any of the 4 HCoV subtypes indicating little evidence for cross-reactive antibodies against this domain. The S2 domain, however, selectively reduced antibody binding to the two HCoV betacoronaviruses, OC43 and HKU1 (p <0.0001 & p=0.0014, respectively by repeated measure one-way ANOVA with Holm-Sidak’s multiple comparison test). No such effect was observed in relation to binding to the alphacoronaviruses NL-63 and 229e (Figure 3).
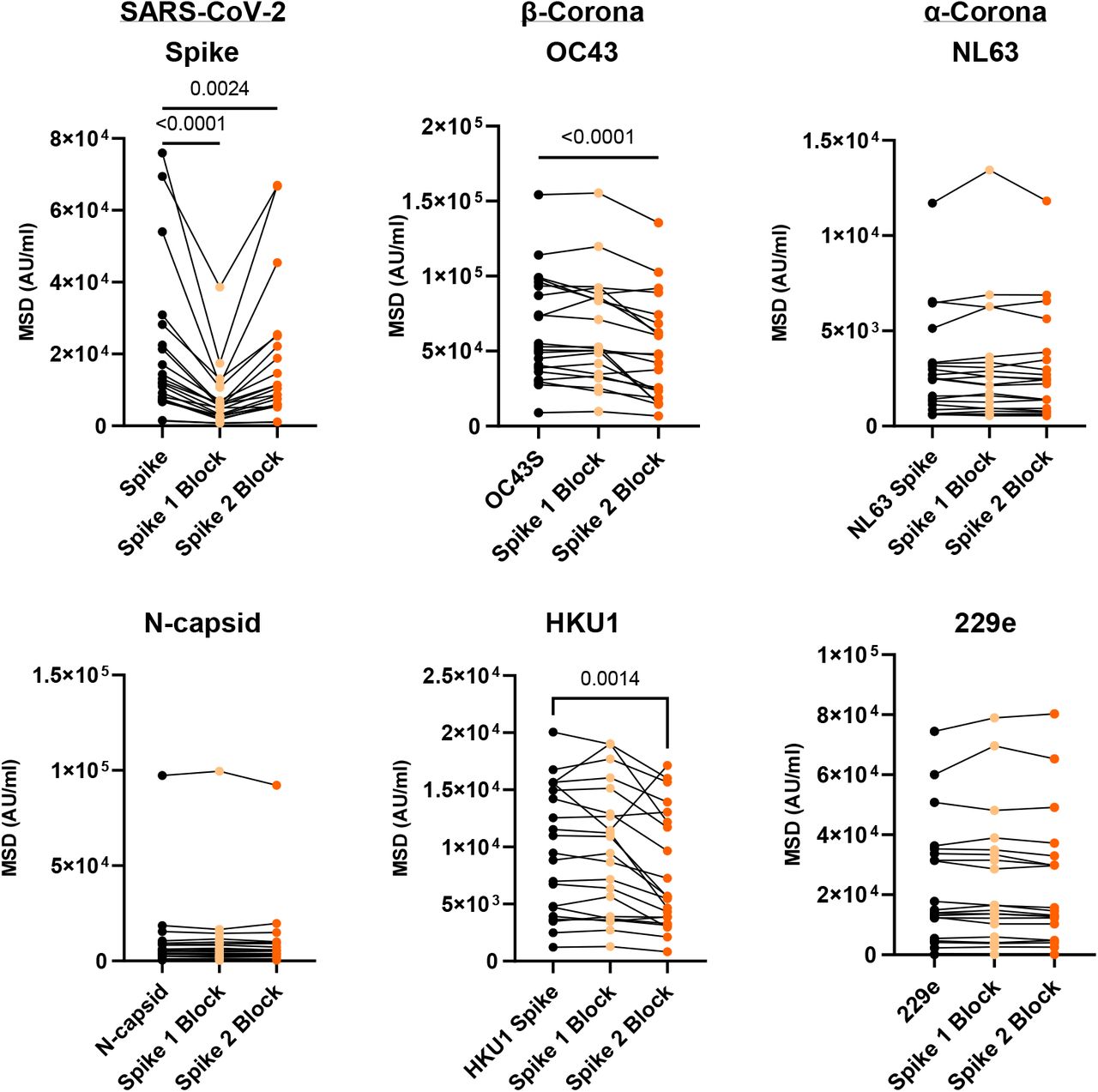
Plasma from SARS-CoV-2 seropositive children was assessed for binding to the Spike protein of the four HCoV or the Spike, or nucleocapsid regions of SARS-CoV-2. Plasma was either applied neat (control) or following pre-absorption with either recombinant S1 (Spike 1 Block) or S2 (Spike 2 Block) domain protein. S1 pre-absorption strongly reduced binding to SARS-CoV-2 Spike whilst S2 pre-absorption reduced binding to OC43 and HKU1. Repeated measure one-way ANOVA with Holm-Sidak’s multiple comparison test, or Friedman test with Dunn’s multiple comparisons test as appropriate
These data show that the enhanced antibody response to HCoV in children after SARS-CoV-2 infection is based on a combination of antibodies that are cross-reactive against SARS-CoV-2 and those that are specific for HCoV.
Children develop strong cellular immune responses against spike protein after SARS-CoV-2 infection
We next assessed the magnitude and profile of the cellular immune response against SARS-CoV-2 in children and adults. ELISpot analysis against overlapping peptide pools from spike and a combination of nucleocapsid and membrane and envelope (N/M) was performed on samples from 57 children and 93 adults, including 37 and 64 who were seropositive, respectively.
As expected, ELISpot responses were common in SARS-CoV-2 seropositive donors, with 86% (32/37) of seropositive children and 69% (45/64) of seropositive adults showing a positive ELISpot response to Spike.
The magnitude of the cellular response against spike was 2.1-fold higher in children, with median values of 533 spots/million compared to 195 in adults (p=0.0003, Brown-Forsythe and Welch Anova, with Dunnett’s T 3 multiple comparisons test) (Figure 4A). Cellular responses against the N/M pool were relatively lower in children compared to spike such that the S:N/M ratio was markedly elevated in children, at 4.7 vs 1.8 in adults (p=0.0007, Brown-Forsythe and Welch Anova, with Dunnett’s T 3 multiple comparisons test) (Figure 4B). The proportion of responders against each pool was also different, with 98% of children with a positive ELISpot responding to spike but only 45% responding to the N/M pool. In adults, the proportions were 88% and 64%, respectively (Figure 4C).
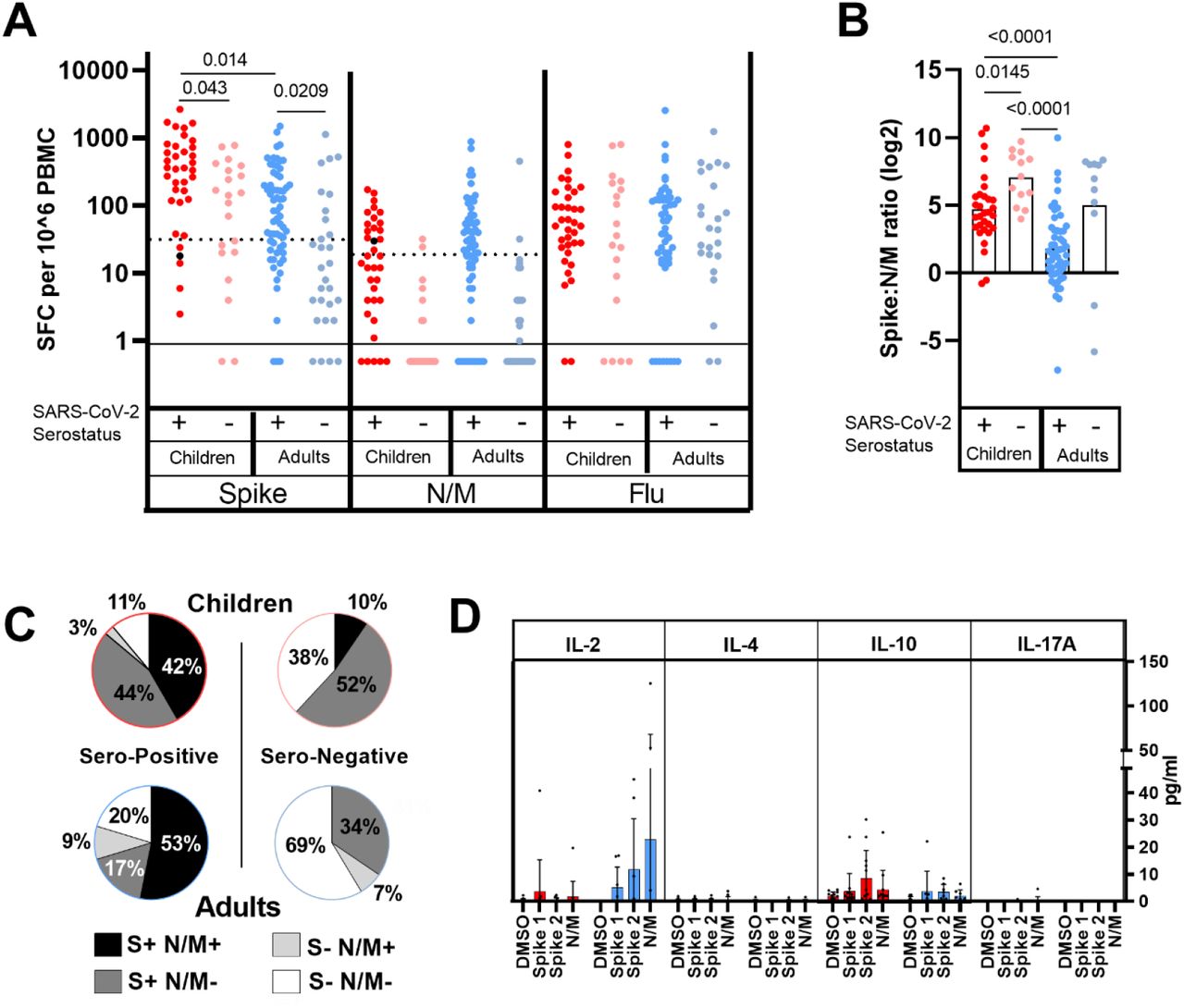
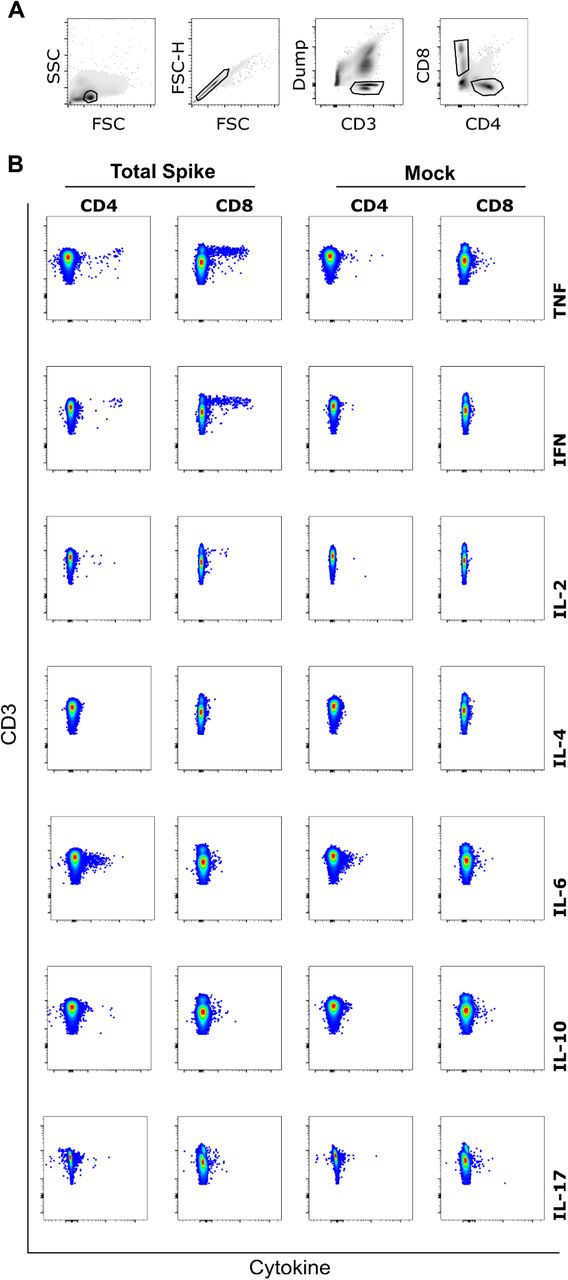
A) SARS-CoV-2 T cell response in children (red) and adults (blue) was determined by IFNγ ELISpot using pepmixes containing overlapping peptides to Spike, Nucleoprotein and viral Membrane (N/M), or Influenza, and shown in respect of Spike serostatus.
B) The level of Spike response was compared to N/M response and displayed as a ratio in seropositive and seronegative adults and children, as indicated. Bars indicate mean, Brown-Forsythe and Welch Anova, with Dunnett’s T 3 multiple comparisons test.
C) The proportions of each cohort scored as responding to SARS-CoV-2 is indicated
D) Supernatant from overnight ELISpot cultures showing responses were analyses for additional cytokines as shown (children red, adults blue). Bars indicate mean±SD.
Supernatant samples from the ELISpot were then analysed using a multi-analyte bead assay to compare the profile of cytokine production by SARS-CoV-2-specific T cells from children and adults. Samples from adult donors showed a strong IL-2 response with lower levels of IL-10 production. In contrast, IL-2 levels in samples from children were very low (Figure 4D) indicating differential functional response compared with adults. Indeed, analysis of three children by flow cytometry indicated that CD8+ IL-2-TNF+IFNγ+ T cells constituted the bulk of the spike-specific T cell response in children (Extended Data 2).
Notably, robust cellular responses were also observed in 60% (12/20) of seronegative children, all of whom were seronegative by three different serology platforms. Cellular responses of variable but lower magnitude were also present in 34% (10/29) of sero-negative adults (Figure 4 A). Two children and one adult had anti-nucleocapsid antibodies only on the MSD platform (Extended Data Table 2.), but this was considered insufficient to provide definitive sero-status. These cellular responses in seronegative donors were markedly spike-specific, with elevated S:N/M ratios of 7.1 and 5 in children and adults respectively (Figure 4B) and may indicate pre-existing cross-reactive immunity. Indeed 7/12 seronegative children and 6/10 seronegative adults with a positive ELISpot also had increased antibody levels to one or more HCoV (Extended Data Table 2), potentially indicating recent HCoV infection. Alternatively, these responses might represent cellular sensitisation to SARS-CoV-2 protein in the absence of sero-conversion.
Bold values indicate values above cut-off. Bold-italicised indicates values +50% higher than geometric mean.
Children and Adults maintain immune responses against SARS-CoV-2 for at least 6 months
We were next interested to assess the longevity of immune responses within a subgroup of 35 children and 81 adults who had seroconverted at least 6 months prior to analysis. Importantly, all children retained humoral immunity whilst 7% (6/81) of previously seropositive adults failed to show significant antibody responses. Children also maintained higher antibody titres against Spike and RBD which were 1.8-fold higher than adults (Figure 5A&B).

Antibody and T cell responses in children (red) and adults (blue) who were seropositive at first testing indicating infection greater than six months prior.
A) Antibody titres as determined by MSD assay, bars indicate geometric mean± 95%CI. Dotted lines indicate seropositive cut-offs. Fold change indicates change in geometric mean titre. Black dots indicate individuals who were seronegative for Spike but retained a nucleocapsid antibody response.
B) Proportions of individuals retaining antibody responses to antigens as indicated.
C) The level of antibodies which neutralise interaction of RBD with the ACE2 protein were determined in children (red) and adults (blue), ten pre-pandemic adult samples were included as a control (black). Dotted line indicates results below limit of detection. Bars indicate geometric mean ±95% CI.
D) IFNγ ELISPOT results in children (red) and adults (blue). Black dots indicate individuals who lacked a Spike response but retained a nucleocapsid response., Brown-Forsythe and Welch Anova, with Dunnett’s T 3 multiple comparisons test.
E) The proportions of each cohort scored as responding to SARS-CoV-2 is indicated
F) The level of Spike response was compared to N/M response and displayed as a ratio in seropositive and seronegative adults and children, as indicated. Bars indicate mean. Un-paired t-test.
The RBD region of spike is the predominant target of neutralising antibodies and as children had strong RBD-specific antibody responses, we next examined relative inhibition of virus binding in an ACE2 binding assay (n=12 children; n=15 adults). A higher, but non-significant, level of neutralising antibody was seen between adults and children (Figure 5C), indicating that both groups maintain antibodies capable of neutralisation of RBD binding to ACE2, although this may be higher in children, consistent with higher RBD antibody levels (Figure 5A).
Cellular immune responses were detectable in 84% of children and 79% of adults at least 6 months after infection. The magnitude of the spike-specific response remained higher in children than in adults (p=0.032) whereas responses to the N/M pool were seen in only 31% of children compared to 68% of adults (Figure 5D&E). As such, the ratio of the S:N/M response in children over time diverged further from adults at this later time point (p<0.0001) (Figure 5F).
Children show enhanced recognition of Variants of Concern at least 6 months after primary SARS-CoV-2 infection
SARS-CoV-2 Variants of Concern (VOC) may be able to escape immunity generated by prior infection or vaccination in adults 18, 19. The development and maintenance of cross-reactive high-level antibody responses by children suggested that children may have different responses to VOC. To examine this, we selected samples from 19 children and 18 adults at >6months after primary infection. We tested the recognition of Spike and RBD from B.1.1.7 (UK-Kent variant), B1.351 (South African variant) and P1 (Brazilian variant), compared to titres of the original Wuhan genotype, as used in previous assays. Children maintain higher levels of antibody response to the original Wuhan Spike (Figure 5A, Figure 6A). Importantly this is also reflected in the response to Spike from the three VOC with 1.74, 1.82, and 2.06-fold higher geometric mean titres against B.1.1.7, B1.351 and P1 respectively (Figure 6A).

A. Antibody titres to total Spike from Wuhan and VOC in children (red) and adults (blue), fold change shows difference in Geo mean titre between children and adults for each variant. Bars indicate Geo Mean±95%CI. Kruskal-Wallis test with Dunn’s multiple comparison test
B. Antibody titres to RBD from Wuhan and VOC in children (red) and Adults (blue), fold change shows difference in Geo mean titre between children and adults for each variant. Bars indicate Geo Mean±95%CI. Kruskal-Wallis test with Dunn’s multiple comparison test.
We then examined titres to the RBD region of the three VOC. In comparison to adults, children possessed higher titres to all the VOC, with 2.14, 1.82 and 2.92-fold higher geometric mean titres to B.1.1.7, B1.351 and P1 respectively, with significantly higher titres to B1.351 and P1 variants (p0.029 and p0.0114 respectively, Kruskal-Wallis test with Dunn’s multiple comparison test). Remarkably, using the cut-off for Wuhan-RBD, 16/19 (84%) children retained seropositive status to B1.351 and P1, compared to only 5/18 (28%) and 8/18 (44%) adults respectively (Figure 6B).
To examine if the recognition of VOC by children and adults was qualitatively different, we assessed the proportion of response to VOC normalised to the Wuhan Spike and RBD titre. In this respect, responses were similar in children and adults (Extended Data Table 3), demonstrating that children have improved recognition of VOC as a function of quantitively superior antibody responses.
*Percentage of Wuhan serotype titre †seropositivity defined based on a cut-off of 600 AU/ml.
These data show children generate durable cellular and humoral immune responses following natural SARS-CoV-2 infection within an increasing focus against the spike protein, which may provide greater immunity to variants of SARS-CoV-2.
Discussion
Age is the primary determinant of the clinical severity of SARS-CoV-2 infection and a life course assessment of virus-specific immunity is essential to understand pathogenesis and design vaccine strategies in children. Our detailed analysis of adaptive immune memory identifies a number of novel features in young children. A key finding was that the magnitude of the adaptive immune response to SARS-CoV-2 is higher in children compared to adults. This is somewhat different to previous reports which have reported lower antibody titres in children. It has also been reported that children do not mount effective antibody responses against nucleocapsid in the early post-infection period. We observed antibody responses against both spike and nucleocapsid in children, but it was also clear that immune responses were much more strongly focussed against spike. This is likely because the spike protein - and RBD in particular - is a major virulence factor for SARS-CoV-2 and antibodies against RBD correlate with neutralising activity in vitro.20 At the same time, nucleocapsid is very abundant protein within the virion and it is possible that the magnitude of the N-specific response is a reflection of peak or aggregate viral load. Levels of virus within the upper airways at the time of primary infection are equivalent in children and adults 21, but relative changes over the course of infection are not known. Enhanced innate immune responses in children may play an important role in limiting systemic replication, which may explain the higher rates of asymptomatic and transient, mild illness in children exposed to the virus compared to adults 22. One striking feature was that SARS-CoV-2 infection in children doubled the antibody titres against all four alpha and beta HCoV subtypes. This pattern was not seen in adults where increased humoral responses were modest, even to the most closely-related beta-coronavirus 23, 24. Of note, increased antibody titres against HoCV have also been observed after SARS-CoV-1 infection 25. Using protein domain pre-absorption, we identified that a proportion of this response represented a SARS-CoV-2-specific humoral response that was cross-reactive with the S2 domain of the two more closely related betacoronaviruses. The S2 domain is more highly conserved than S1 between CoV and this pattern is compatible with preferential targeting of structurally-conserved epitopes by HCoV-specific antibodies in children 26. Some studies have shown these to have neutralising activity against SARS-CoV-2 (Shrock et al 2020, Ng et al 2020). Paediatric SARS-CoV-2 infection, however, also boosts HCoV-specific antibody responses that are not directly cross-reactive, as demonstrated by increased titres against alphacoronaviruses that could not be pre-absorbed. This may potentially reflect weakly cross-reactive B cell clones, potentially activated through T cell cross recognition, and is reminiscent of antibody boosting against H3 haemagglutinin after H1N1 infection in children who have had previous H3N2 infection 27. As such, there may be a lower affinity threshold for boosting of related but heterologous immune responses in children which might potentially represent an evolutionary adaptation to expand the memory pool early in life. It is interesting to speculate whether the observation that SARS-CoV-2 infection triggers a broadly reactive humoral response in children and might provide insight into the pathophysiology of PIMS-TS, where intense B cell activation and auto-antibody production leads to a hyper-inflammatory syndrome. Notably, lack of pre-existing immunity to HCoV is a risk factor for development of PIMS-TS and may potentially indicate a protective influence from a stronger prior cross-reactive memory B cell pool 7.
There is currently very little information regarding the cellular immune response to SARS-CoV-2 in children. Interestingly, we found that the virus-specific T cell response was stronger in children than in adults. Furthermore, the specificity mirrored that of the humoral response in that responses against the spike protein were markedly increased compared to nucleocapsid and envelope proteins.
Virus-specific T cell responses in children also showed a differential cytokine response with markedly reduced production of IL-2 and evidence of increased IL-10 production. This may suggest a more highly differentiated profile in children compared to adults, in line with the enhanced magnitude of the response. Indeed, IL-2-IFNg+TNF+ CD8 T cell responses represented the majority of the Spike-specific T cell pool observed in three children at more than 6 months after primary infection. As such further characterisation of the T cell response in children is required.
A further noteworthy feature was that virus-specific T cell responses were detectable in more than half the seronegative children. It is possible that these represent HCoV-specific T cell responses that cross react against SARS-CoV-2 peptides 28, 29, as previously observed for antibody responses that are also focussed against spike protein (Ng et al 2020). HCoV infections are more common in young children and might potentially lead to generation of effector cells that were detected in the SARS-CoV-2 ELISpot. As such, this profile of cross-reactive antibody and cellular responses in children may help to explain the excellent clinical outcomes in this group. Alternatively, it is possible that these responses represent genuine SARS-CoV-2-specific T cells that have been generated following virus exposure in the absence of antibody sero-conversion. This pattern has been reported in health care workers with high levels of viral exposure 30 and it is possible that such conditions are also seen in primary schools where enforcement of social distancing is challenging.
Many participants were seropositive 6 months prior to analysis and our data extend previous findings in adults 17, 31 to show sustained immunity over this time period. Moreover, we also found that children maintained stronger antibody and cellular immune responses at this timepoint compared to adults with no loss of humoral response compared to 7% in adults. We also found that children possess enhanced responses to Spike and importantly RBD from there different VOC; RBD titres to variants have been shown to correlate with viral neutralisation 19. Further studies using virus neutralisation assays will be required following natural infection and vaccination of children to address this important point fully.
Assessment of immunity beyond 6 months post-infection is important as these individuals are more likely to encounter future VOC. Our data suggest strongly that natural infection in children provides immunity to not only the antecedent strain but also robust immune responses to future variants. In the light of increasing concerns that SARS-CoV-2 will become an endemic infection 32, these findings provide encouragement that immunity generated in childhood provides robust and sustained protection, including to emerging VOC.
In conclusion, we show that children display a novel and characteristic profile of adaptive immune response against SARS-CoV-2. This is likely to contribute to the strong clinical protection in this age group but may also provide insight into the characteristic immuno-pathology that may develop. Furthermore, they will help to guide the introduction and interpretation of vaccine deployment in the paediatric population.
Data Availability
Data is available following reasonable requests.


Assay cut-offs were tested using plasma samples from nine children (red) and 50 adults (blue) taken prior to COVID-19. Dotted lines indicate the cut-off used.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
PBMC were stimulated for 6hrs in the presence of total-Spike peptide pool and then analysed by flow cytometry to assess intracellular cytokine production. A) Gating strategy for analysis. B) Representative example of ICS staining from one child at six months post SARS-CoV-2 infection showing strong TNF+IFNγ+ CD8+ T cell response representing 0.45% of the global CD8+ T cell repertoire.
Acknowledgement
We would like to express our gratitude to the staff, parents and especially children for their participation in this study, without whom this work would not have been possible.
Footnotes
The revised manuscript contains an additional figure (figure 6) and associated data table,which is an analysis of antibody recognition of SARS-CoV-2 Variants of Concern in Children and Adults. Figure 3 has also been updated to be more consise.
References



