
Abstract
Importance Persistent symptoms are reported in patients who survive the initial stage of COVID-19, often referred to as “long COVID” or “post-acute sequelae of SARS-CoV-2 infection” (PASC); however, evidence on incidence is still lacking, and symptoms relevant to pain are yet to be assessed.
Objective To determine long-term symptoms in COVID-19 survivors after infection.
Data Sources A literature search was performed using the electronic databases PubMed, EMBASE, Scopus, and CHINAL and preprint servers MedRχiv and BioRχiv through January 15, 2021.
Study Selection Eligible studies were those reporting patients with a confirmed diagnosis of SARS-CoV-2 and who showed any symptoms persisting beyond the acute phase.
Data Extraction and Synthesis Incidence rate of symptoms were pooled using inverse variance methods with a DerSimonian-Laird random-effects model.
Main Outcomes and Measures The primary outcome was pain-related symptoms such as headache or myalgia. Secondary outcomes were symptoms relevant to pain (depression or muscle weakness) and symptoms frequently reported (anosmia and dyspnea). Heterogeneity among studies and publication bias for each symptom were estimated. The source of heterogeneity was explored using meta-regression, with follow-up period, age and sex as covariates.
Results In total, 35 studies including 18,711 patients were eligible. Eight pain-related symptoms and 26 other symptoms were identified. The highest pooled incidence among pain-related symptoms was chest pain (17%, 95% CI, 12%-25%), followed by headache (16%, 95% CI, 9%-27%), arthralgia (13%, 95% CI, 7%-24%), neuralgia (12%, 95% CI, 3%-38%) and abdominal pain (11%, 95% CI, 7%-16%). The highest pooled incidence among other symptoms was fatigue (45%, 95% CI, 32%-59%), followed by insomnia (26%, 95% CI, 9%-57%), dyspnea (25%, 95% CI, 15%-38%), weakness (25%, 95% CI, 8%-56%) and anosmia (19%, 95% CI, 13%-27%). Substantial heterogeneity was identified (I2, 50-100%). Meta-regression analyses partially accounted for the source of heterogeneity, and yet, 53% of the symptoms remained unexplained.
Conclusions and Relevance The current meta-analysis may provide a complete picture of incidence in PASC. It remains unclear, however, whether post-COVID symptoms progress or regress over time or to what extent PASC are associated with age or sex.
Question What is the incidence rate of long-term post-acute sequelae of SARS-Cov-2 infection related to pain and other symptoms?
Findings In the current meta-analysis of 35 studies with 18,711 patients, the highest estimated incidence among pain-related symptoms was chest pain (17%), followed by headache (16%), arthralgia (13%), neuralgia (12%) and abdominal pain (11%). That among other symptoms was fatigue (45%), followed by insomnia (26%), dyspnea (25%), weakness (25%) and anosmia (19%).
Meaning These findings suggest that long-term post-acute sequelae of SARS-Cov-2 infection must not be overlooked or underestimated especially when vaccination has become the focus.
Introduction
A broad range of symptoms have been reported to persist beyond the acute phase of SARS-CoV-2 virus infection.1-6 These are referred to as “long COVID”,1,3,5,6 “long-hauler”5 or “Post-COVID-19 syndrome”.4,5 The National Institute of Health currently advocates calling it post-acute sequelae of SARS-CoV-2 infection (PASC).7 This syndrome is sometimes covered sensationally by news media or social networks, but little is known about its etiology, natural history, risk factors, or therapeutic interventions. Even more, evidence on its incidence is still lacking.
On a cellular level, the spike protein in the SARS-CoV-2 virus combines with angiotensin-converting enzyme 2 (ACE2) receptor, invades human cells, and injures multiple organs.8 Central and peripheral nerve systems are one of the most susceptible targets for SARS-CoV-2 virus (neurotropism).9 Frequently reported symptoms range from fatigue, muscle weakness and memory loss to anosmia, ageusia, confusion and headache.1-6,10 Some of these symptoms are directly or indirectly related to chronic pain, often worsening quality of life for a long period. As well, a prolonged period of mechanical ventilation in the ICU may cause what is called “post intensive care syndrome” or “ICU-acquired weakness”,9 manifesting as cognitive dysfunction, muscle atrophy, sensory disruption and joint-related pain.8 These patients will be at elevated risk of developing chronic pain. Furthermore, SARS-CoV-2 virus causes “cytokine storm”, which aggravates damage in multiple tissues including joints and muscles that possibly triggers pain-related symptoms.8 A recent study11 has shown that the prevalence of new-onset headache was substantially higher in COVID-19 survivors compared with those in controlled subjects. Nevertheless, pain in COVID-19 survivors has been underestimated or paid little attention. Treatment of pain in such patients is prone to be of low priority, especially due to overburdened healthcare services or difficulty in consulting with a specialist over the course of the pandemic.12
As pain clinicians, we believe that understanding and managing pain-related symptoms along with other symptoms will help to improve the quality of life of SARS-CoV-2 survivors. Therefore, we collected currently available living evidence and conducted rapid systematic reviews and meta-analyses of observational studies to determine the incidence of pain-related and other symptoms in SARS-CoV-2 convalescents.
Methods
We defined long-term complications as symptoms from which patients suffered for more than 1 month after onset of the first COVID-19 symptoms or after discharge from hospital. A meta-analysis was conducted according to the reporting guidelines for the Meta-analysis of Observational Studies in Epidemiology (MOOSE) Statement.13 The protocol was previously registered on PROSPERO (CRD42021228393).
Search Strategy
Three reviewers (HH, SH and TS) searched the electronic databases PubMed, EMBASE, Scopus, CHINAL and preprint servers MedRχiv and BioRχiv. No language restriction was applied. The last search was done on January 15, 2021. The full search strategy is described in eAppendix 1 in the Supplement. Reference lists of all identified articles on “long-covid” were manually searched. All relevant references obtained in the RIS (Research Information Systems) formats were transferred to EndNote X8.2 (USACO Corporation, Tokyo, Japan) and web-platform manager Covidence (Melbourne, Australia).
Eligibility Criteria
Studies involving adults (>18 years old) with a confirmed diagnosis of SARS-CoV-2 were included, as were studies that followed up patients for a minimum of 2 weeks after discharge. Studies only focusing on acute symptoms from admission without any mention of long-term symptoms were excluded. Prospective or retrospective cohort studies were also included. Reviews, editorials, meta-analyses, case reports, case series and case-control studies were excluded. Regardless of whether a reported symptom was pain-related or not, studies reporting any relevant “long-covid” symptoms were included. Studies reporting only radiological findings of lung or brain were excluded.
Screening and Data Extraction
Two reviewers (HH and TS) independently screened titles and abstracts of obtained references by using Covidence. Disagreements were resolved by discussion with a third reviewer (SH). Data extraction was performed by five reviewers (HH, TM, HS, SH and TS), and the extracted data was saved in an Excel spreadsheet. Extracted data included study setting, country where study was performed, patient setting, diagnostic criteria of SARS-CoV-2, respiratory support, mean age, percentage of males, follow-up period and information for evaluating study quality. The primary outcome was defined as pain-related symptoms such as headache or myalgia. The secondary outcome was defined as symptoms other than but relevant to pain such as depression or fatigue, or frequently reported symptoms such as anosmia or dyspnea. When data were reported as a graph only, we reproduced numerical data using Plot Digitizer (http://plotdigitizer.sourceforge.net).
Assessment of Study Quality
The Newcastle-Ottawa scale for cohort studies14 was used to assess the methodological quality of the studies by the five reviewers. Briefly, the scale consists of three subcategories: selection, comparability and outcome and 9 items. However, we focused on pooled incidence of long-covid symptoms rather than any treatment effects and all patients exposed to SARS-Cov-2 virus (excluding the non-exposed cohort); therefore, some of the items were impossible to evaluate such as selection of the non-exposed cohort and comparability. Thus, these two items were excluded from the checklist and study quality was assessed by the rest of the items. One point was given for each item, for a maximum score of 6 and a minimum score of 0.
Statistical Analysis
At least 3 studies were required per one symptom, due to constraints in performing data synthesis. The proportions of symptoms in an individual study were pooled using inverse variance methods following logit transformation.15 Between-study variances were quantified using the DerSimonian-Laird estimator.16 To calculate 95% confidence intervals in an individual study, the Clopper-Pearson interval was used. The I2 statistic was used as a measure of heterogeneity (I2 >60%: high heterogeneity; 40-60%: moderate heterogeneity; <40%: low heterogeneity). Sensitivity analysis and subgroup analysis were not performed because our aim in this meta-analysis was to exploratorily collect currently available evidence of overall incidence.
We explored the source of heterogeneity by meta-regression using a mixed-effects model.17 We incorporated three covariates (follow-up period, mean age and percentage of males) with fixed effects, and each study as a random effect. R2 was used as a measure of the amount of heterogeneity that could be accounted for by the covariate. Briefly, an index R2 value is defined as the ratio of explained heterogeneity to total heterogeneity, with a range of 0% to 100%. We plotted the logit transformed incidence of each symptom on the Y axis and the covariate on the X axis, along with predicted regression line (bubble plot).
Statistical significance was set at a 2-tailed α = .05. To evaluate small-study effects (publication bias), a funnel plot was depicted and Egger test was performed,18 with significance applied at P <.010. All statistical analyses were conducted using the meta package of R version 4.0.3 (The R Foundation for Statistical Computing) and RStudio 1.4 (Boston, MA).
Results
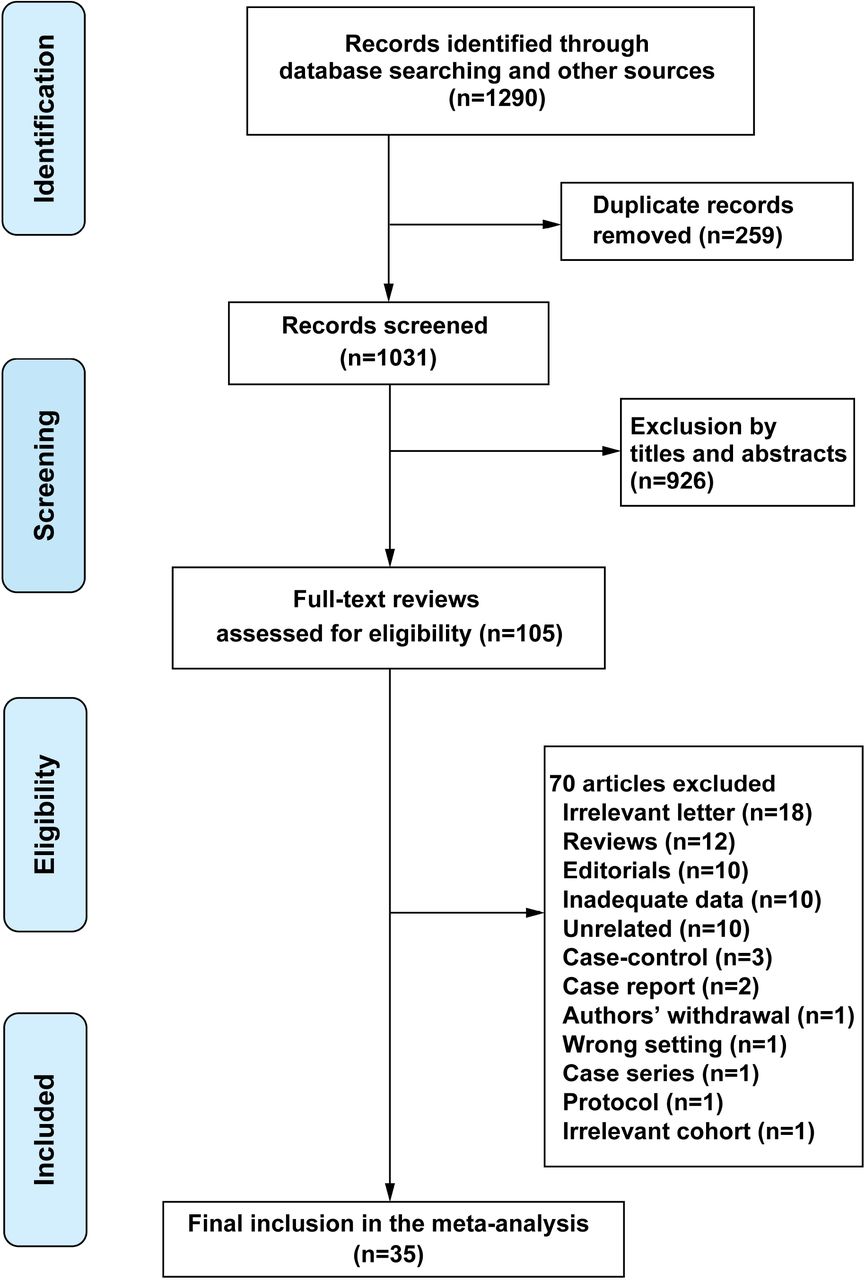
The initial search yielded 1290 citations, of which 105 potentially relevant studies were assessed in full text, and finally, 35 studies19-53 comprising 18,711 patients were included in the meta-analysis (Figure 1). All studies were written in English. A summary of the included studies is presented in eTable 1. Studies were reported mainly from Europe, followed by the USA and China. Follow-up duration ranged from 0.5 to 7 months.
The results of the Newcastle-Ottawa scale are shown in eTable 2. Most of the studies (30/35, 86%) scored 5 or 6, and the median score of the 35 studies was 5 (range: 3-6).
The results of each symptom on the forest plot are shown in eFigure 1-. The pooled incidence of each primary and secondary outcome is shown in order of frequency in Figures 2 and 3, respectively.

I2 represents the degree of heterogeneity, and Egger’s P represents publication bias.

{kind=link}
{kind=link}
{kind=link}
I2 represents the degree of heterogeneity, and Egger’s P represents publication bias.
The most frequent symptom among pain-related symptoms was chest pain (17%, 95% CI, 12%-25%), followed by headache (16%, 95% CI, 9%-27%), arthralgia (13%, 95% CI, 7%-24%), neuralgia (12%, 95% CI, 3%-38%) and abdominal pain (11%, 95% CI, 7%-16%). The most frequent symptom in the secondary outcomes was fatigue (45%, 95% CI, 32%-59%), followed by insomnia (26%, 95% CI, 9%-57%), dyspnea (25%, 95% CI, 15%-38%), weakness (25%, 95% CI, 8%-56%) and anosmia (19%, 95% CI, 13%-27%).
The results of R2 obtained by meta-regression are shown in the Table, and those of the statistical analyses and bubble plots are detailed in eFigures 1-. Among pain-related symptoms, significant correlations were identified only for neuralgia: however, only three studies with this symptom were included. For instance, the regression coefficient for follow-up period was 0.39 (logit transformed), which means that every one month of follow-up corresponds to an increase of 1.45 units (45% increase) in prevalence in patients who developed neuralgia after acute COVID-19 infection. For the other symptoms, significant correlations were found for insomnia, dyspnea, weakness, anosmia, cough, ageusia, memory impairment, depression, anxiety, nasal blockage, weight loss, sputum, chills and nausea. Among the symptoms overall, 53% remained unexplained when using the three covariates in the model.
The results of the funnel plot are shown in eFigure 1-. For pain-related symptoms, small-study effects as assessed by Egger test were observed for 4 of 8 symptoms. For other symptoms, small-study effects were observed for 15 of 26 symptoms. In total, small-study effects were identified for 56% of the symptoms.
Discussion
The current meta-analysis suggested three main findings. First, pain-related symptoms in COVID-19 survivors were multifarious with a incidence of 5-17%. Second, other symptoms were more multifaceted with incidences ranging from 2% to 45%. Third, every symptom varied extensively in its incidence, and the three major covariates (follow-up, age and sex) could not explain the heterogeneity.
Among pain-related symptoms, the highest pooled incidence was chest pain (17%), followed by headache (16%), arthralgia (13%), neuralgia (12%) and abdominal pain (11%). Chest pain is also referred to as “lung burn”, which is considered to be a result of lung injury by SARS-CoV-2 infection.6 Alternatively, other researchers pointed out that chest pain may result from pericarditis caused by infection.29 Headache is one of the most common CNS symptoms in patients with SARS-CoV-2 infection.54,55 It can persist over the period of the initial infection,56 or it can develop as a new-onset form during healing.11 Proposed mechanisms include direct invasion of trigeminal nerve endings by SARS-CoV-2 via disruption of the brain-blood barrier, trigeminovascular activation via involvement of endothelial cells with ACE2 expression, or triggering of perivascular trigeminal nerve endings by release of cytokines and pro-inflammatory mediators.56
Among other symptoms, almost half of the patients developed fatigue. Generally, fatigue is considered to be closely related to chronic pain. Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS)57 or fibromyalgia58 are good examples. A recent report suggested that there are similarities and overlap in pathology between long COVID symptoms and ME/CFS.4,57 As fatigue is often refractory to a single approach, holistic management such as rehabilitation or cognitive behavioral therapy is required.6 Weakness, often accompanied by myalgia and arthralgia, is a musculoskeletal manifestation of SARS-CoV-2 infection.59 Muscle fiber atrophy, extensive use of corticosteroids, prolonged mechanical ventilation or systematic inflammation may be the causes of weakness.59
From the results of the meta-regression, the incidence of neuralgia was significantly associated with follow-up period, age or sex to some extent; however, only 3 studies were included with this symptom. Therefore, it is difficult to consider this result to be valid. As another example, an inverse association was found between the incidence of weakness and age, but we could not explain this well. In any case, we are aware that these statistical models are preliminary and exploratory, and 53% of symptoms were not explainable despite three typical covariates being incorporated into the model. Symptoms of long COVID are reported to be on-and-off, cyclic or multiphasic,5 which is why the linear regression model did not fit well.
To our knowledge, two similar systematic reviews with or without meta-analysis on long COVID still exist in preprint form.60,61 The strength of our study is that it highlights various symptoms from the perspective of pain, which might provide physicians with new insight into the management of patients who suffer from long-term sequelae of SARS-CoV-2 infection.
Limitations
This study has several limitations. First, considerable heterogeneity was found in most of the symptoms, and meta-regression could not explain it in just over half of symptoms. Possible reasons may be the following: in the light of the nature of observational studies, the subjects are not homogenous. The current study includes reports from a wide range of countries; thus, the definition and diagnostic criteria of symptoms might vary from study to study. The majority of data were collected via telephone interview or online survey. A face-to-face visit was not always possible during the COVID-19 pandemic, and therefore, recall bias might possibly have occurred. Second, the current study did not include “brain fog”, “covid toe” or “post-exertional malaise”, which are widely known as post-COVID symptoms,2,6,26,59 because these symptoms did not fulfill our inclusion criteria of at least three studies being required for data synthesis. However, we will be able to update this review if more reports are published on these symptoms in the future. Third, publication bias was identified for 56% of all symptoms. This suggested that the point estimates of the incidence of symptoms in our study might have been overestimated or underestimated. Lastly, the current study is a rapid, living meta-analysis. More robust evidence will be collected in the near future.
Conclusions
The present meta-analysis highlighted the incidence in pain-related and other typical symptoms in patients with PASC. It remains uncertain whether post-COVID symptoms progress or regress over time and to what extent PASC are associated with age or sex.
Data Availability
All data are available from authors.
References



