
Abstract
Objective Given the treatment limitations of depression in bipolar disorder, we evaluated the known risks of using psilocybin (and similar substances) in this population, including a systematic assessment of published case histories, to assess the risk of psilocybin as a treatment of depression in bipolar disorder.
Data Sources A comprehensive search of case studies published through December 31, 2020 was conducted using the following electronic databases: PubMed, Web of Science, and PsychInfo, focusing on classic psychedelics and case studies or case histories.
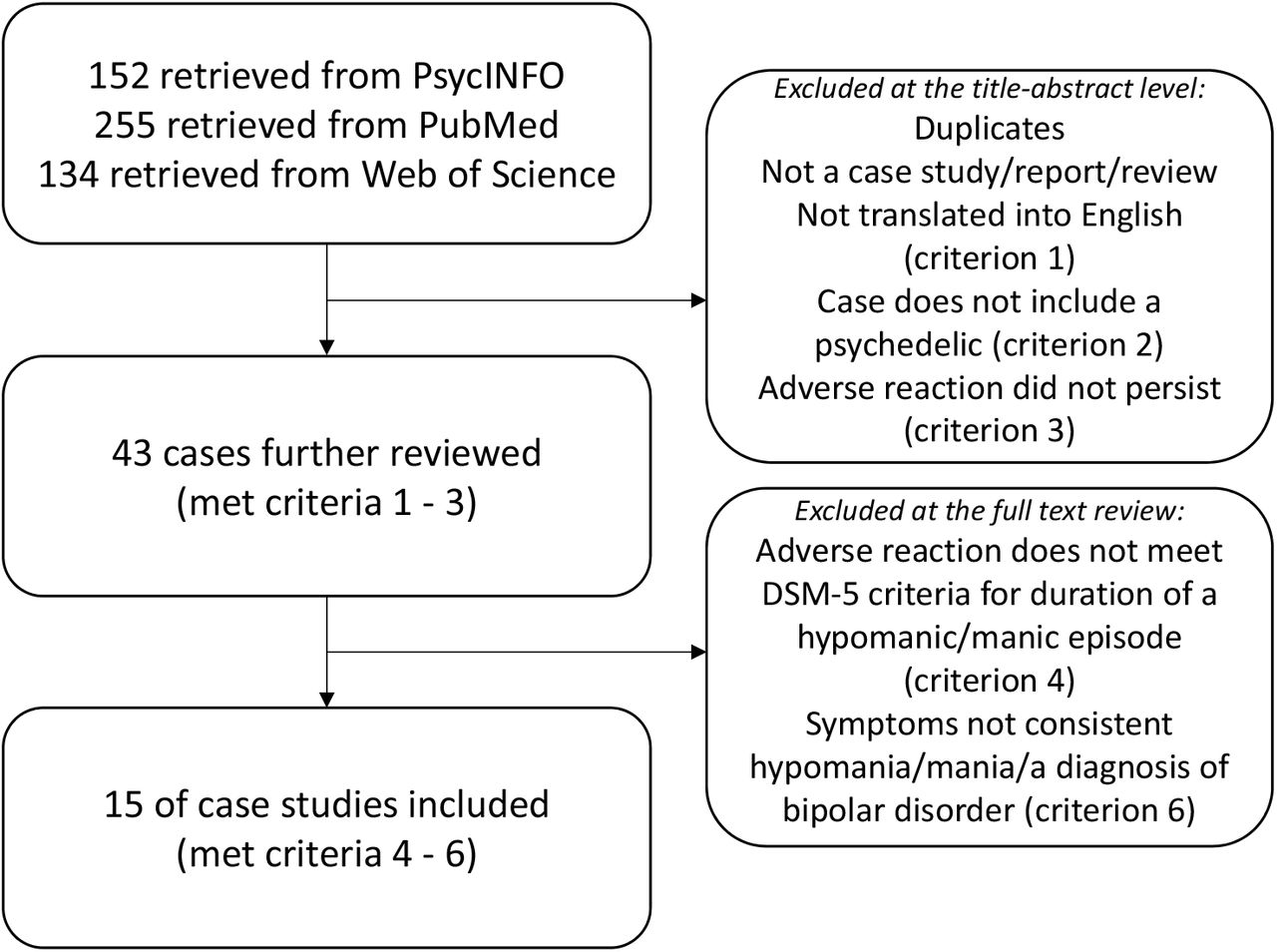
Study Selection Our search terms resulted in 541 hits, of which 43 were non-duplicates of case studies with individuals having an adverse reaction to a psychedelic substance. Of those, 15 case studies indicated some form of adverse event involving mania or manic like behavior that persisted beyond the acute intoxication of the substance.
Data Extraction Two independent evaluators assessed all possible cases, focusing on manic behavior based on DSM criteria. Two separate evaluators convened to evaluate cases where the case information was unclear.
Results Of the 15 cases, four involved psilocybin, two cases involved individuals with a likely pre-existing diagnosis of bipolar disorder, and three involved individuals without a history of polysubstance abuse or concurrent polysubstance use.
Conclusions We conclude that there is some evidence of risk of activating mania with these substances, but that the risk does not appear to be strong or overwhelming. Instead a careful prospective study, such as an open-label treatment protocol with careful controls, appears warranted in this population.
INTRODUCTION
Individuals with bipolar disorder experience high suicide rates, decreased quality of life, and impaired overall functioning relative to people without bipolar disorder, and in many cases, individuals with other psychiatric conditions.1,2 Further, most negative outcomes are related to the depressive phase of the illness.3 Unfortunately, current pharmacological treatment options for depression in bipolar disorder are limited.4 One promising new treatment for depression is psilocybin, a psychedelic compound that has recently received the designation of ‘Breakthrough Therapy for depression’ by the Food and Drug Administration.5 However, little is known about the safety of psilocybin therapy for people with bipolar disorder.
Psilocybin, is a hallucinogenic compound found in several species of mushrooms, and has been used in religious and healing practices by Indigenous peoples for millennia.6 While the evidence for its benefit and safety in humans has been known in research since the 1950’s, in 1970 the Controlled Substances Act essentially ended psychedelic research in humans.5 Following this period general societal views of psychedelic use was quite critical, focusing on recreational use, sometimes bordering on hyperbole and sensationalism.7 This is in contrast to self-report,8,9 observational,10 and epidemiological data11 in contemporary research which suggests that use of these drugs presents a lower risk of harm than other commonly available substances, and may be associated with mental health benefits. In fact, over the past fifteen years, research has indicated that a single dose of psilocybin in a treatment context may dramatically improve symptoms in major depressive disorder and treatment resistant depression,12–14 obsessive-compulsive disorder,15 anxiety,16 and demoralization in long-term AIDS survivors.17 Though acute psychedelic effects of the drug resolve within four to five hours of oral administration, psilocybin’s beneficial effects on mood and well-being may persist for weeks to possibly months.18
Importantly, modern psilocybin trials reflect an appreciation for optimizing the conditions under which the drug is administered, both to reduce risk of adverse events and to increase the likelihood that participants will experience lasting positive effects.19 Specifically, modern trials have emphasized ‘set’ and ‘setting’ or procedures that explicitly address the mindset of participants before psilocybin exposure, and the environmental setting in which dosing and post-dosing psychological processing of the psilocybin experience occurs. Sufficient preparation for the psychedelic experience, including rapport-building with study staff, attention to the physical space to enhance comfort and safety, and post-drug session meetings to discuss the experience, are now considered essential best practices.19,20 Perhaps because of these conditions and careful screening and structure, modern psilocybin trials have not reported any serious adverse events.21
What is known about risks in bipolar disorder and psilocybin and psychedelics?
All modern clinical trials with psychedelics have excluded individuals with bipolar disorder or a family history of bipolar disorder out of a concern for precipitating a manic episode or worsening the course of the condition.22 The scientific evidence for these exclusions, however, is rarely clarified. Nonetheless, there are several rationales for excluding these individuals including: the powerful serotonergic activation from psychedelic substances possibly inducing a Treatment Emergent Affective Switch (TEAS; i.e., the activation of a manic episode through the use of an antidepressant), the potential for adverse events in a population that is at higher risk for impulsive behaviors, as well as clinical consensus drawn from examples in psychiatric and emergency admissions and case reports.
Psilocybin and TEAS
While the phenomenon of mood polarity switching with antidepressants has been extensively studied and correlations are well documented,23 the biologic mechanism of antidepressant-induced TEAS (and for that matter, mood switching in general) remains poorly understood.24 Substantial evidence suggests that any effective antidepressant, including glucocorticoids, dopamine agonists, ketamine, and transcranial magnetic stimulation, can induce TEASs.24–27 However, the risk for TEASs appears to be higher in response to serotonergic antidepressants, such as SSRIs, SNRIs, and most tricyclic antidepressants (TCAs).28–30 Consequently, their use in the treatment of bipolar depression is controversial, leading some to recommend avoiding serotonergic antidepressants whenever possible.31 On the other hand, others have argued that the risk of TEAS may be overstated32 at least partly because TEAS are more common in patients with bipolar treated with older TCA’s (11.2% with a TEAS) compared to SSRI’s (3.7% with a TEAS), which are more commonly used now.28 Further complicating matters is evidence that serotonergic antidepressants in patients with bipolar 2 may be effective for treating depression without inducing enduring switches of mood polarity,33,34 but may cause an increase in short term changes in mood reflecting mixed states or rapid cycling.35 In sum, little is understand about the mechanisms of TEASs and there is active debate about the risk and benefits of using serotonergic agents in bipolar disorder with outstanding issues including characterization of the disorder (e.g., type 1 vs 2), the type of agent (e.g., TCA vs. SSRI), and the concomitant use of mood stabilizers. Given these uncertainties, it is challenging to predict whether a psychedelic such as psilocybin is likely to induce a TEAS.
Though the risk of TEAS after a single psychedelic dose is currently unknown, there are reasons to be concerned. First, psilocybin is a potent antidepressant and all antidepressants carry some risk of inducing TEAS.24–27 Second, psilocin, the active metabolite of psilocybin, is a serotonin transporter inhibitor and 5-HT2A receptor partial agonist that also binds to the 5-HT2C, 5-HT1A, and 5-HT1B receptors.36–38 While different from standard antidepressants in many ways, psilocin has related serotonergic mechanisms of action, which could theoretically promote TEASs.28–30 Third, the relationship between antidepressant drug administration regimen and TEAS is unknown. Psilocybin is typically administered in a distinctly different way from standard antidepressants. Standard antidepressants are dosed daily, with generally imperceptible acute effects on mood. They appear to act gradually, often taking weeks or more to demonstrate clinically significant benefit. Psilocybin treatments, in contrast, usually involve a single high-dose administration of the drug that produces profound subjective effects during the period of intoxication. Antidepressant effects are apparent within hours after dosing, and preliminary evidence suggests that these improvements can persist for weeks to months without further administration of the drug. Whether this dramatically different approach to dosing--and its impact on serotonin signaling--increases or decreases the risk of TEAS relative to standard antidepressants has yet to be determined.
Adverse events and research trials
While all individuals with bipolar disorder or a first degree relative with bipolar disorder have been excluded from recent psychedelic research, given the large and growing literature in this area, it is certainly possible that individuals who did not know that they or a family member had bipolar disorder, or who had yet to meet the criteria for the disorder, have been included in previous studies. However, with the structures of ‘set’ and ‘setting’ in place, and a careful attention to participant well-being, participants have not experienced serious adverse events in these studies. For example, in an analysis of 110 healthy participants who completed a total of 227 laboratory-based psilocybin administration sessions, there were no instances of prolonged psychosis, mania, persisting perceptual changes, or other long-term functional impairment in any participants.22 In a systematic review of psychedelics in modern and pre-prohibition psychedelic studies of psilocybin, lysergic acid diethylamide (LSD), and ayahuasca, no cases of severe adverse events (defined as prolonged psychosis, or Hallucinogen Persisting Perception Disorder; HPPD) were found.41 Early research on LSD and other psychedelics did in fact attempt to treat individuals who likely had bipolar disorder. For example, Busch and Johnson42 described three individuals with “manic depression” who were treated with LSD. While there was no reported follow up on how the patients fared, indications were that while under the influence of LSD, all three patients were more active and agitated, although it was not clear if this was compared to other patients. One 57-year-old woman with “chronic mania” spoke more rapidly and emotionally after a “small” LSD dose, a second 48-year-old woman with “manic depression” was given LSD during a manic phase and was described to be louder and combative, and a third 49-year-old woman with mania was described as more talkative, irritable, and suspicious. Unfortunately, the lack of follow-up (and other methodological problems with pre-prohibition studies) makes it impossible to disentangle the immediate effects of the substance from what might have occurred later, including any worsening of the underlying illness.41
Epidemiology research on psychedelic use
The analysis of recreational hallucinogen use in the general population may provide additional insight into the risk of psilocybin and other psychedelics in people with bipolar disorder, given that the large sample sizes likely include individuals with bipolar disorder or a family history of bipolar disorder. For example, a large-scale survey of more than 130,000 participants indicated that hallucinogen use (in approximately 22,000 individuals) was not a predictor for subsequent mania, psychosis, or mental health treatment.43 In another large-scale survey of over 190,000 participants, individuals who had used psychedelics were at reduced odds of psychological distress and suicidality (while participants who reported other non-psychedelic drug use had increased risk of these factors).11 While these studies focused on drug use broadly, one study specifically focused on community participants who had ‘challenging or difficult experiences’ while on psilocybin and other hallucinogens. Of 1,900 respondents, 2.6% reported behaving in a physically aggressive or violent manner while on the substance, and three respondents reported enduring psychotic symptoms;44 these accounts could potentially reflect activation of a manic episode or the onset of a bipolar illness. However, there were no clear reports of enduring symptoms of mania or activated bipolar illness. Finally, researchers looked at the number of cases of psychotic and bipolar disorders subsequent to over 130,000 doses of ayahuasca given between 1994-2007 at the União do Vegetal (UDV) church in Brazil.45 In total there were 29 cases of psychotic features, of which 4 were labeled ‘bipolar affective disorder; psychotic manic episode.’ These researchers concluded that the number of psychosis and other cases from this sample is slightly less than the expected in the base rate of the population. This is somewhat surprising given that many ayahuasca retreats involve other aspects that might increase the risk of a manic episode (including decreased sleep and repeated dosing). Overall these epidemiological studies do not appear to indicate a clear risk of mania with psychedelic use.
The Present Study - Systematic Review of Published Cases
Given the relative dearth of information on adverse events in bipolar disorder within the broader psychedelic literature, we turned our attention to the case study literature. Our goal was to critically explore these cases for any adverse effects of psilocybin (and related psychedelics) in individuals with bipolar disorder, and the potential for these substances to activate a manic episode. We focused this review on psilocybin as the current evidence suggests that this compound may be effective in treating depression. However, there is limited data on specific risk of psilocybin use in bipolar disorder. Thus we have broadened our question of risk to include all serotonergic psychedelic tryptamines including LSD, ayahuasca, and DMT. Indeed, there is evidence that the classic psychedelics share similar molecular (and experiential) characteristics.46,47 Also, because it can be difficult to clinically differentiate a manic from a psychotic episode, we included case histories and descriptions of what appear to be manic or psychotic behavior with manic behavior that persisted beyond the immediate effects of the substance. However, the focus of this systematic review was on the risk of activating manic episodes in individuals with bipolar spectrum disorder, and not on the risk of activating a psychotic episode leading to a diagnosis of a psychotic spectrum disorder. Therefore, we focus here on the former.
METHOD
Identification and selection of publications
A comprehensive search of case studies published through December 2020 was conducted using the following electronic databases: PubMed, Web of Science, and PsychInfo. Our initial search focused specifically on psilocybin and included the following terms ((“psilocybin”) OR (“hallucinogenic mushrooms”) OR (“magic mushrooms”)) AND ((“case study”) OR (“case report”) OR (“case review”)). This search revealed a small number of publications (Pubmed=66, Web of Science=16, PsychInfo=8) prior to inclusion/exclusion criteria below (which narrowed the case studies down to (Pubmed=4, Web of Science=2, PsychInfo=2, or a total of four non-overlapping cases), and so we expanded the search to include all classic psychedelics (((“psilocybin”) OR (“hallucinogenic mushrooms”) OR (“magic mushrooms”) OR (“LSD”) OR (“ayahuasca”) OR (“DMT”)) AND ((“case study”) OR (“case report”) OR (“case review”)).
Additional inclusion/exclusion criteria
Case studies were included if they met the following criteria: 1) written or translated into English with at least a DOI or abstract to locate the article, 2) described an individual who had clearly taken a psychedelic, 3) included individuals with persistent effects from the substance that was adverse: 3A) For individuals who had a diagnosis of bipolar disorder, or in examples where the authors described a history that indicated a likely diagnosis of bipolar disorder, we included these individuals if there were any adverse events after taking a psychedelic substance, 3B) for individuals who did not have a clear diagnosis or history of bipolar disorder (i.e., the vast majority of cases), we included the case if the problems or symptoms related to the adverse event were described in a way that could be interpreted as mania (e.g., increased goal-directed behavior, decreased need for sleep, etc.) or positive symptoms of psychosis (e.g., hallucinations or delusions) that continued beyond immediate, intoxication effects of the substance, 4) following DSM-5 criteria48 for duration of a manic or hypomanic episode, we included only cases with effects that lasted at least 4 days, or involved hospitalization for the adverse effects, or involved effects that were clearly severe in nature (e.g., resulting in extreme symptoms or problems). 5) We did not exclude polysubstance use, but have noted polysubstance use in the included table (Table 2), 6) while we included psychosis symptoms or adverse events in the initial screening, we excluded cases that resulted in symptoms or problems that did not also ultimately result in mania or hypomania or a diagnosis of a bipolar disorder (e.g., individuals who were subsequently diagnosed with schizophrenia or HPPD).
Process
Two authors (LR and MG) independently reviewed all electronic databases. Four authors (LR, MG, DEG, & JW) conferred to make final decisions when it was unclear whether a case met specific criteria (usually duration of the episode (#4) or whether the ultimate diagnosis would be mania or purely psychosis (#6)). As mentioned above, the initial search was expanded to include other classic psychedelics which resulted in a more substantive case number (Pubmed=255, Web of Science=134, PsycInfo=152). After duplicates were removed and screened using the aforementioned criteria, the references in the remaining cases were examined for additional relevant case studies, but no additional cases were found. In total, 43 cases were initially included based on criteria 1-3 (in English or translated, and clear adverse events with symptoms), and then 28 were excluded based on criteria 4-6 (duration of mania was not met, or the result was clearly psychosis or HPPD only), leaving 15 cases. See Figure 1 for a flow chart of inclusion/exclusion.

{kind=link}
Flow chart for the search and selection of the final cases.
RESULTS
In total, 15 published case studies met all of the selection criteria, four of which involved psilocybin.49–63 Table 1 summarizes the case content (each case is numbered) and Table 2 summarizes the themes in each case. In terms of themes, of the 15, five case studies appeared to involve some history of mania or hypomania before ingestion of the psychedelic, or a family history of bipolar disorder (Cases 7, 9, 11, 13, 15). Five reported some form of additional substance use in the current adverse event (Cases 6, 9, 10, 12, 13), seven had some substance abuse or polysubstance use history prior to the episode (Cases 2, 5, 8, 10, 12, 14, 15), and eight used the substance repeatedly in a relatively short time period (Cases 1, 3, 4, 5, 9, 10, 12, 13). The length of the adverse events varied (often confounded by various treatments) but ranged from a few days to a few months. Most of the case studies noted whether the symptoms had resolved, which was typically within days to weeks, although this, too, was confounded by prescribed treatments. From these cases a number of helpful insights can be gleaned.
The final 15 cases along with brief descriptions of the cases.
Themes from each of the 15 final cases.
First, one of our primary goals was to find clear examples of individuals with a diagnosis of bipolar disorder (or previous history of manic/hypomanic symptoms) who had an adverse outcome after taking a psychedelic substance. Of the 15 cases that met the broader criteria, we found two such cases. In Case 13, a psychiatrist with bipolar disorder type I was hospitalized for mania after self-medicating his depression with 1g of vaporized DMT daily for 6 months and 60mg of phenelzine daily for three months.61 It is unclear if his manic episode was precipitated by factors such as the combination of DMT and an MAOI, time frame, or one of the distinct substances. In Case 11, a 30-year-old man developed symptoms of mania, delusions, and hallucinations two days after participating in a four-day ayahuasca retreat.59 Notably, this individual had symptoms of hypomania (but no depression) two weeks prior to the retreat. The case specifically noted that he was at the retreat to learn about the culture and services, and not as a specific treatment. The presence of hypomania before the retreat raises the possibility that issues related to developing mania (e.g., increasing impulsivity) may have led to his psychedelic use and that he may have developed mania even without using a psychedelic.
Another primary goal was to find cases where an individual without a prior history of bipolar disorder only took a psychedelic substance that appeared to activate a manic episode. We found three cases where an individual with no known bipolar history (although one case had a family history of bipolar) took a single psychedelic substance once (without any other substance or a polysubstance use history), which resulted in sustained manic symptoms. Case 6 was a 31-year-old man who took LSD one time and two weeks later experienced dramatically decreased sleep along with an increased focus on religious themes and an incident of breaking into a neighbor’s house. He was hospitalized and treated successfully with lithium.54 In Case 7, a 21-year-old woman was admitted to a psychiatric hospital with persistent manic and psychotic symptoms one week after taking LSD at a music festival.55 At admission she had decreased need for sleep, paranoia, mood swings, and catatonia. Her mother had a diagnosis of bipolar disorder, and her uncle a diagnosis of schizophrenia. Finally, Case 2 describes a 22-year-old man who took LSD, became paranoid, flew to his home in Israel, took all of his money out of the bank, then flew back and traveled throughout Europe, convinced that he was escaping a Nazi conspiracy.50 This ultimately led him to attack and kill a stranger that he thought was a Nazi soldier. He was hospitalized for four months before his psychosis and manic symptoms remitted. While the overall number of these specific cases is small, these examples highlight that a manic episode can occur when individuals take a psychedelic substance, perhaps especially when one is predisposed to bipolar disorder.
Another important point is that 12 of the 15 cases found involved recreational psychedelic use, leaving three exceptions: Case 13 of the psychiatrist who was self-medicating with DMT,61 Case 11 of the 30-year-old man with a history of hypomania who participated in a four-day ayahuasca retreat,59 and Case 14 of a 40-year-old woman who participated in a two-day ayahuasca retreat.45 In this third case, the patient began to exhibit psychotic symptoms on the second day of the retreat and subsequently had two bouts of sleeplessness (including one 48-hour period), delusional beliefs, and excessive talking. The symptoms remitted after she was hospitalized and treated with haloperidol, and she reported no additional symptoms on follow-up one year later. Notably, these last two cases are the only two cases that we found where the individuals had clear manic episodes after taking a psychedelic substance as a treatment in a guided session. It is unclear whether this low number reflects the fact that those performing unregulated treatments screen individuals with histories that may indicate susceptibility to mania or psychosis, if proper attention to set and setting decreases these outcomes, if these issues are just not well documented, or some combination of these factors. Unfortunately, the ayahuasca ceremony cases identified do not describe the specifics of the set and setting of the ritual retreat, which may be important to understanding the risk of activation of mania in this population.
Finally, it should be noted that in our screening of the literature, we identified a number of published cases that include clear serious adverse outcomes (e.g., severe medical accidents, death, and possible suicides) during the period of active drug effects. However, we did not find any published cases where an individual had a diagnosis of bipolar spectrum disorder, took a psychedelic substance, and then died due to an accident or suicide. While cases such as this may exist, we were not able to find any documented in the extant literature.
DISCUSSION
Overall, the present review focused on the available evidence of risk that psilocybin confers in bipolar disorder. We found several published case studies that implicate psychedelic use as a possible contributor to a manic episode. As described in Table 1, we found 15 cases that describe possible activation of a manic episode (or a psychotic episode that may have had manic elements) after psychedelic use. Of those cases, two (Case 11 and 13) appeared to be people who may have had a bipolar disorder diagnosis prior to taking the substance, and four had a family history of bipolar disorder. Other important themes that our case review indicates is that polysubstance use (5 of 15 cases) and the use of psychedelics multiple times over a short time period (8 of 15 cases) are both risk factors for adverse psychiatric outcomes. Together, this suggests that several factors related to psychedelic use may contribute to the risk of a manic episode in this population.
Though the cases are significant, the small number of published case studies linking psychedelic use to mania induction is not overwhelming. Furthermore, the number of cases in which ingestion of psilocybin led to a possible manic episode is surprisingly small (n=4) and none of the cases that involved someone with or without a history of bipolar disorder developing mania after a clear single ingestion of a psychedelic involved psilocybin or hallucinogenic mushrooms. Given that psychedelic use in general, and ingestion of psilocybin-containing mushrooms in particular, are common recreationally and in unregulated treatment settings, this suggests that the overall rate of inducing mania may be relatively low. Of course, it may be that the small number of published case studies is due to perception (or reality) that examples of mania or worsening of bipolar disorder after psychedelic use are so common that they do not warrant publication as case studies. However, this seems unlikely given the epidemiological research indicating that recreational use of psychedelic substances does not appear to be an independent risk factor for mania or psychosis.43
Between this systematic review of the published case study literature, the exclusion of individuals with bipolar disorder in modern trials, and the epidemiological data on hallucinogen use, perhaps the most striking finding is how little is known about the effects of psilocybin and similar psychedelics in this patient population. It is evident from this review that much more research is needed, including direct evaluations of psychedelic experience and outcomes among individuals with bipolar disorder, in both recreational and unregulated treatment settings. For example, researchers could directly solicit responses from individuals with bipolar disorder on their experiences with psychedelic substances, or from providers or guides in unregulated (or newly regulated) treatment settings.
While this review has focused on the potential risks for individuals with bipolar disorder, it may be that some patients could benefit from psychedelic treatments. In our search there was one case study (not included in the 15 cases) that implicated an accidental LSD overdose in the remission of bipolar disorder for over 20 years.64 A 15-year-old girl (monitored closely by mental health providers following diagnosis of bipolar disorder with psychotic features at age 12), accidentally took 10 times the recreational dosage of LSD and showed essentially no subsequent psychotic, hypomanic, or manic symptoms for 20 years after the event. The adolescent’s parent, psychiatrist, and therapist followed her closely over the subsequent years and attributed her mental health stability to the overdose. We did not find other similar cases in our review, and clearly this case does not provide the kind of evidence needed to evaluate psychedelics in the treatment of bipolar disorder. It is also possible that a psychedelic drug (such as psilocybin) may be specifically challenging for people with bipolar disorder, especially given the feelings of euphoria that often accompany use. Specifically, there is some evidence that people with bipolar disorder can develop a fear of strong positive feelings due to association with a manic episode, leading some researchers to include positive mood exposures into psychosocial treatments.65
There are several reasons that caution around psilocybin use is indicated in this population including: the strong serotonergic activation of psychedelic substances and the possibility of a TEAS, the potential for adverse events in a population known for impulsive behavior, and clinical case reports of negative events. Because all modern clinical psychedelic trials have excluded people with bipolar disorder, we lack critical information about the effects of psilocybin and similar compounds in this clinical population However, people with bipolar disorder carry a significant burden of depression that may respond positively to the antidepressant effects of psilocybin when carefully administered in a controlled setting. Given our findings here that the evidence for the activation of mania is not overwhelming in psychedelic use, this possibility deserves further exploration.
To assess the relative risk of activating a manic episode in bipolar (or worsening the disorder), the gold standard approach would be a prospective study. We, and others (e.g., https://clinicaltrials.gov/ct2/show/NCT04433845), are currently developing such a study, structured to mitigate potential risks in this population. First, we plan to optimize both the ‘set’ and the ‘setting’ in our clinical psilocybin trials. These aspects were missing in nearly every case report we reviewed. Second, we will screen patients for relevant risk factors, such as substance use and history of psychosis. Third, we will use a conservative dose-escalation protocol, administering a low dose of psilocybin followed weeks later with a high dose in order to monitor participants’ responses over time. Fourth, we will initially only include individuals without a history of mania (i.e., individuals with bipolar 2) and individuals who are outside of the age range where a manic episode would likely first occur (i.e., >30 years old). Finally, we will require participants to have both community and psychological support in place to manage any lingering effects of the intervention after the study is completed. Using all of these precautions will likely significantly decrease the risk of adverse events such as those reviewed here.
There are several limitations to the present study. First, it must be noted that we were limited to only those case studies that clinicians and researchers chose to submit for publication. This of course differs from published research that may include null results. Also, as mentioned above, it is certainly possible that there is a perception that experiences of mania brought on by psychedelic use is commonplace and thus not something that treatment providers would think to publish. Indeed, a review of published cases like this can only tell us what can happen, not how often these events occur. There were also several challenges in reviewing the case study literature and we were obviously limited to only the data provided in each individual case. Case details were often sparse, the motivation for the case review was not always on the outcome of the patient or the patient’s background (e.g., some were focused on urine and blood work assessments), timelines were frequently unclear, and most importantly there was often minimal follow-up. Because many of the published cases involved recreational psychedelic use, details leading up to the adverse events were often vague or hard to follow. Furthermore, the dosages (or confirmation of the substance) were frequently unavailable or reliant on patient reports. Additionally, approximately half of the cases involved either concurrent polysubstance use or recent polysubstance use; the role that drug interactions may have played is difficult to determine. Another limitation is that we focused specifically on persistent adverse events. There were a number of cases that did not involve a clear persistent event because the outcome resulted in the death of the patient (either from accident or suicide). It is possible that some of these cases involved individuals with undiagnosed bipolar spectrum disorders, and the psychedelic substance led to impulsive actions resulting in the patient’s death. However, this is purely speculative.
Conclusion
This systematic case review revealed some cases of manic behavior that appeared to be brought on by use of a psychedelic substance. Importantly, though, this type of case was uncommon in the published literature, which suggests that the rate of mania activated by these substances may be relatively low in this population. Given the existing clinical and basic research, epidemiological studies and published case histories, it appears that a cautious approach to conducting trials in bipolar depression with psilocybin therapy, to examine the effects and safety is warranted. In such a prospective trial, it is crucial that attention be given to a carefully regulated environment where researchers can screen participants, emphasize set and setting, and follow patients for an extended period.
Data Availability
Not applicable
Footnotes
Sources of direct funding, support, or sponsorship Dr. Woolley is funded in part via VA CSR&D 1IK4CX002090-01. Grant title: Quantifying and Treating Social Deficits in Veterans with Mental Illness: a Five Year Plan.
Role of the sponsor Not applicable
Potential conflicts of interest Dr. Woolley is a paid consultant for Psilo Scientific Ltd. and Silo Pharma.
References



