
Abstract
Immune response after a single-dose of BNT162b2 vaccine is markedly increased in health care workers with previous SARS-CoV2 exposure, as assessed by positive SARS-CoV2 IgG, particularly after moderate-severe COVID-19. These data may inform the priority of the boosting mRNA second dose in times of vaccine shortage.
Introduction
Vaccination against SARS-Cov2 is proposed by the WHO as the main option, at the present time, to control the COVID-19 pandemic. However, limited vaccine supply reduces the ability to reach a substantial proportion of individuals and delay the expectations of herd immunity[1]. The standard vaccination protocol for mRNA vaccines includes a 2 dose vaccine administration 3-4 weeks apart[2]. In this setting, a strategy to use single-dose of mRNA vaccines for some individuals could accelerate the achievement of this goal. Data on immune responses to single-dose vaccination with BNT162b2 are limited to few observational studies with small number of patients [3–5]. Moreover, impact of previous natural infection on vaccine response is not well known. We thus sought to evaluate the immune responses after a single dose m-RNA vaccination according to different groups of previous SARS-CoV2 exposure and clinical COVID-19 presentation.
Methods
A random sample of 642 health-care workers (HCW) enrolled in a previous hospital-wide seroprevalence study of 2.590 HCW (first survey April 2020 and second survey November 2020[6]) were invited to participate in this study, based on stratification of 3 groups according to their seropositive status in both surveys: 1) Naïve SARS-Cov2 patients: Seronegative in both surveys (SARS-Sero -/-); 2) Transient seropositivity: seropositive in first survey and negative in second survey (SARS-sero +/-) and 3) Persistent seropositivity: seropositive in both surveys (SARS-sero +/+). In addition, seropositive HCW were further classified according to the severity of the previous COVID-19 in 1) asymptomatic COVID: no symptoms and serologic diagnosis of SARS-CoV-2 infection; 2) moderate COVID: mild to moderate declared symptoms attended as out-patients; and 3) severe COVID: HCW that required hospital admission-
A blood sample from HCW who have received the first dose of the mRNA BNT162b2 vaccine (Pfizer/BioNTech) was obtained just before the administration of the second dose of vaccine (21 days after the first dose), once they had signed written informed consent.
Previous COVID-19 disease was defined if any of the following diagnostic test was positive: RT-PCR against SARS-CoV-2, SARS-CoV-2 antigen detection or positive SARS-CoV-2 IgG (regardless of symptoms).
Laboratory procedures
The SARS-cov-2 IgG assay used is a chemiluminescent immunoanalysis of microparticles (CMIA) used for the quantitative detection of IgG antibodies against the Spike protein (RBD domain) of the SARS CoV-2 virus in the Architect system of the Company ABBOTT Diagnostics. The performance of diagnostic accuracy of immunoassay was tested following the manufactures’ instructions, the cut-off point is <50 arbitrary Units/ml (AU/ml).
Statistical analysis
Results are expressed as median and interaquartile range (IQR). Demographics of COVID-19 and no COVID-19 groups were compare by univariate analysis using chi squared test and t Student test (Supplementary Table 1).
Anti-spike IgG values was described using centrality statistics as mean, median and geometric mean and dispersion measures as standard deviation and interquartile range. We used univariate non parametric test, U Mann Whitney and Krusall Wallis test, to compare anti-spike IgG titers between groups. Pairwise comparisons were adjusted by the Bonferroni method.
Data were evaluated with the Statistical Package for Social Sciences (SPSS 17 IBM Armonk, NewYorkM .R 3.4.4 software (https://cran.r-project.org/bin/windows/base/old/3.4.4/.)
The study protocol was approved by the independent ethics research committee of the hospital.
Results
A total of 642 HCW were invited to participate in the study, and 641 accepted (99.8%). They were 77.3% women and mean age was 45.8 (SD 10.7) years. HCW demographics are shown in Supplementary Table 1. There were not significant differences in the demographics variables among the groups except for a lower percentage of tobacco use (14.8 vs 21.5%, p=0.029) and higher percentage of obesity (11.6 vs 6.2%, p=0.014) in patients who developed symptomatic COVID-19.
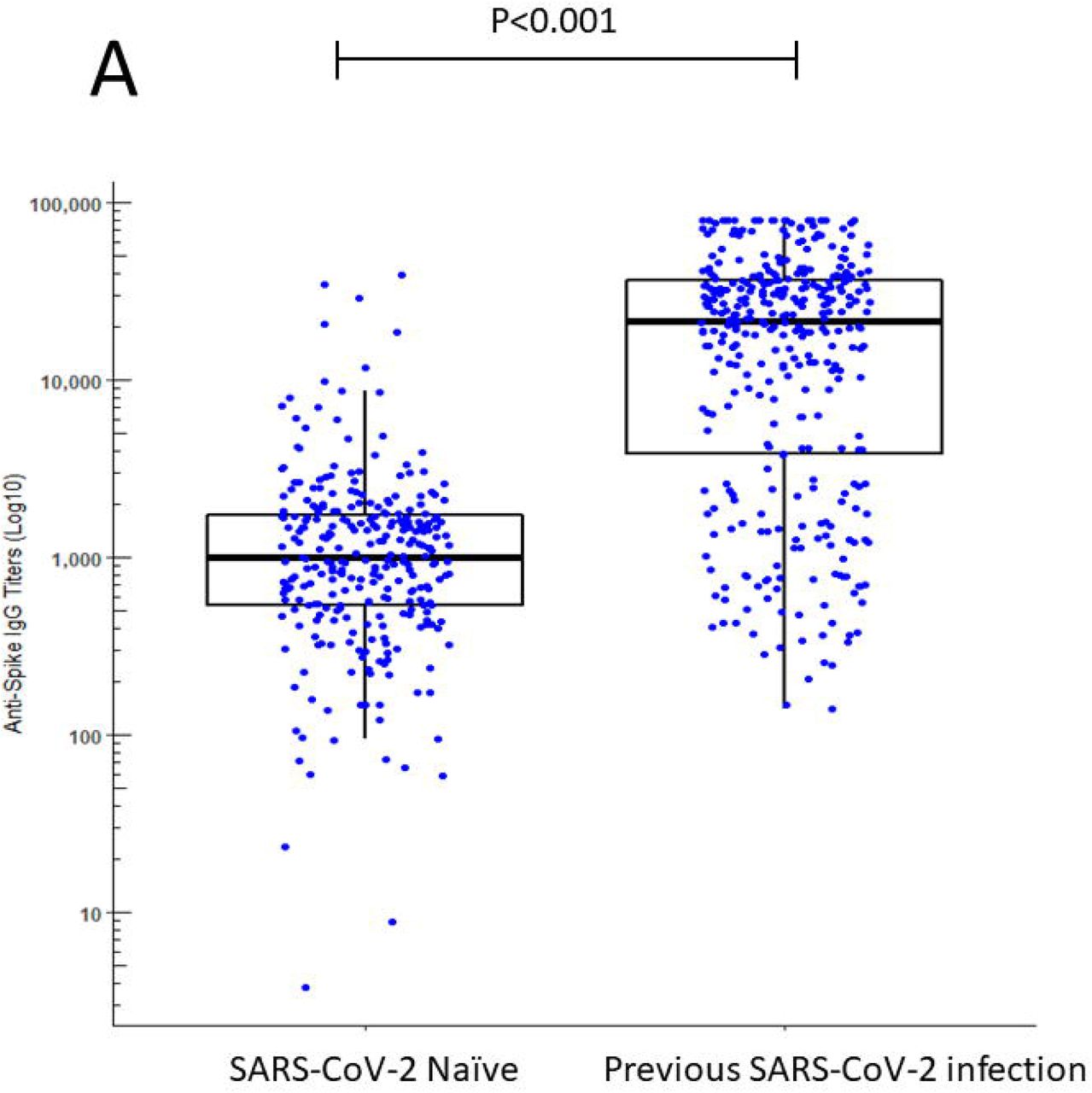
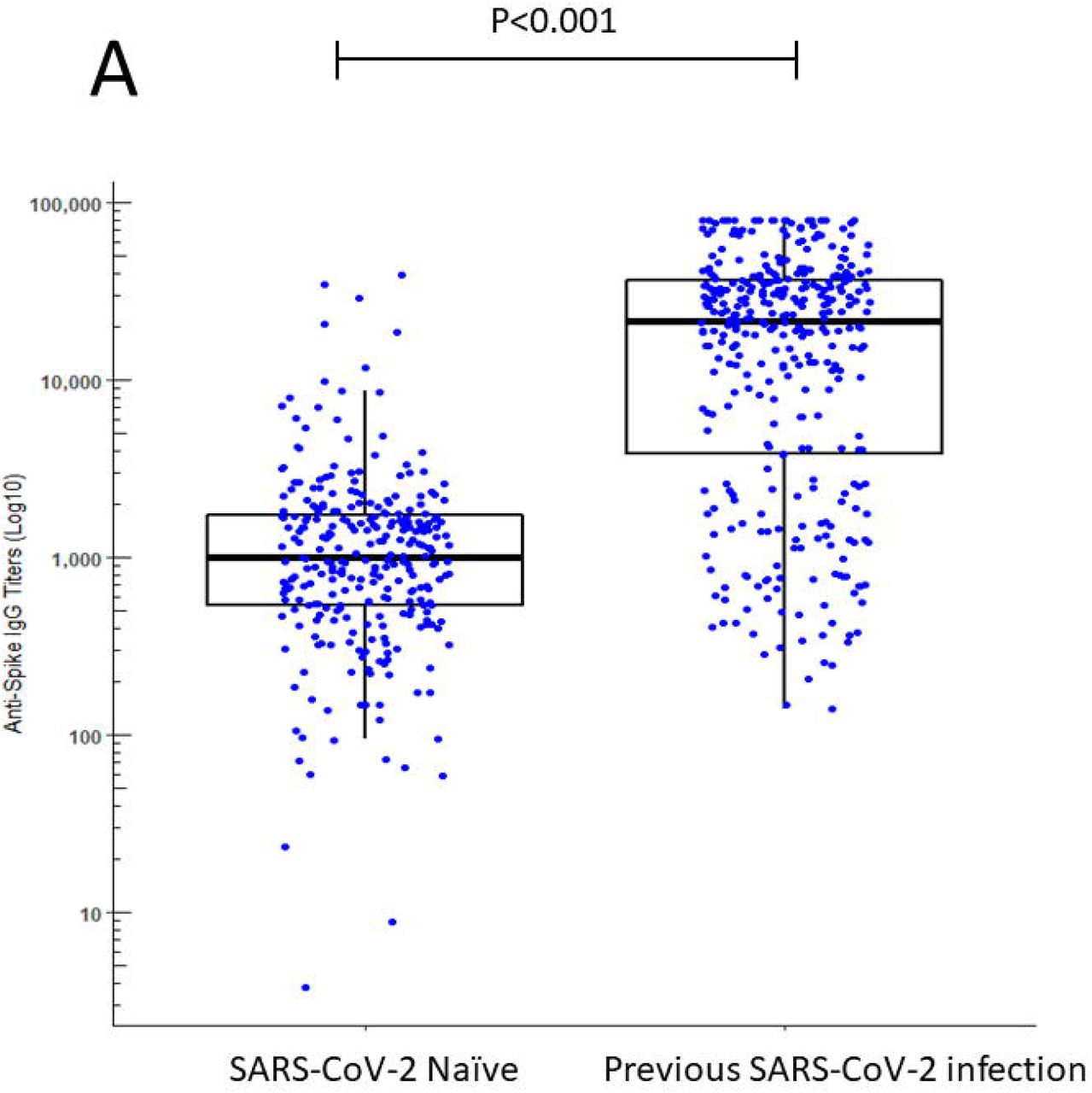
Median Ig G against spike SARS-CoV-2 titers were about 20-fold higher after the first dose of vaccine in HCW with previous SARS-COV2 antibodies (median 22,267.3 AU/ml, IQR 3,972.5 – 3,7091.2) than those SARS-CoV2 naïve (median 1,022.3 AU/ml, IQR 545.7 – 1,760.0, p<0.001), figure 1A, Supplementary Table 2.


{kind=link}
{kind=link}
{kind=link}
Serological response to one dose of the BNT162b2 mRNA COVID-19 vaccine in individuals with and without laboratory-confirmed previous SARS-CoV-2 infection and serological status.
Panel A. SARS-COV2 naïve patients versus patients with previous SARS-COV2 infection. Patients with a previous SARS-COV2 infection had about a 20-fold higher titer than SARS-CoV2 naïve cases 3 weeks after the first dose of BNT162b2 mRNA COVID-19 vaccine
Panel B. SARS-COV2 naïve patients, post vaccine COVID-19 cases, and previous SARS-CoV2 seropositive individuals (transient and persistent).
As compared to naïve SARS-CoV2 subjects, transient seropositive patients showed about a 4 fold, and persistent seropositive patients about a 34 fold higher level of IgG antibodies against SARS-CoV2 Spike protein titres 3 weeks after the first dose of BNT162b2 mRNA COVID-19 vaccine
Panel C. SARS-COV2 naïve patients, and COVID-19 clinical severity (asymptomatic, mild-moderate, and severe COVID-19 cases).
As compared to naïve SARS-CoV2 subjects, asymptomatic, mild-moderate and severe COVID cases exhibited about a 15-, 24- and 44-fold higher of IgG antibodies against SARS-CoV2 Spike protein titres 3 weeks after the first dose of BNT162b2 mRNA COVID-19 vaccine.
Statistical analysis: U Mann Whitney’s test, Bonferroni corrected.
Naïve SARS-CoV2 individuals, transient seropositive and persistent seropositive subjects exhibited progressively higher anti Spike-IgG titers 3 weeks after the first dose of the vaccine (median 1,022.3 AU, IQR 545.7 – 1,760; median 3,860.0 AU; IQR 781.8 – 18,088 and median 34,551.6 AU, IQR 23,432 – 48,597 respectively; p<.001 for all comparisons; figure 1B). In other words, as compared with naïve SARS-CoV-2 subjects, transient seropositive patients showed about a 4-fold, and persistent seropositive patients about a 34-fold higher level of IgG antibodies against SARS-CoV-2 Spike protein.
Previous COVID-19 clinical severity was also associated with increased titers of IgG 3 weeks after the first dose of the vaccine: asymptomatic (median 15,386.4 AU/ml, IQR 1,661.8 – 31,260.9), mild-moderate (median 24,388.8 AU/ml, IQR 7,158.3 – 37,355.5) and severe (median 43,671.7 AU/ml; IQR 20,463.4 – 79,923.7) Figure 1C
A total of 13 subjects developed symptomatic COVID-19 after the first dose of the vaccine, showing a median anti Spike-IgG title of 2,485.8 AU/ml, IQR 1,144.6-9,842.9). Since it is impossible to discern the relative contribution of the vaccine and post-vaccine SARS-CoV2 infection to the IgG titre, no comparison was made between this group and others.
Discussion
Our serological evaluation in HCW shows a dramatic differential response 3 weeks after a single dose of the BNT162b2 mRNA vaccine according to previous exposure to SARS-CoV2 and serological status. So far, this is the large study on immune response after first dose of BNT162b2 vaccine. Of note patients with previous history of COVID-19 exposure reach at least one order of magnitude higher titers of anti Spike-IgG. Although we have not assessed the presences of neutralizing antibodies, our results are strikingly similar to those recently reported by Prendeki [7] and Saadat [8]. This robust serologic response is highly correlated to the presence of neutralizing antibodies. However, we have no data regarding the duration of the serologic response nor the degree of protection against SARS-CoV2 infection.
Our work provides some additional interesting data. First HCW who had lost their SARS-CoV2 antibodies exhibit a lower response, that might be insufficient to provide SARS-CoV2 protection[4,9]. On the other hand, the combination of clinical COVID-19 and the presence of anti Spike-IgG SARS-COV-2 antibodies before vaccination are strong predictors of a robust serologic response to a single dose of BNT162b2 mRNA vaccine that may make less necessary the boost associated with the second dose.
There is current controversy regarding the most efficient strategy regarding the use of available vaccines in order to offer a wider population protection[10–12]. Whether enhanced single dose mRNA vaccine-induced serologic response among previously seropositive individuals will show a lasting response as compared to boosted vaccines is currently unknown. As no trial has evaluated the medium term protective effects of a single-dose mRNA protocol, health policy makers rely on surrogate markers such as SARS-CoV-2 seropositivity prior to vaccination, for this difficult decision. Our results suggest that deferring the second dose of the vaccine to some individuals with a predictable strong serologic response may not a high risk strategy for them, offering the option for vaccination of other individuals at risk until a wider vaccine availability allows for a standard 3-4 week interval between mRNA vaccine doses as this is the protocol that has been tested in clinical trials.
Supplementary tables
Acknowledgments
We thank all workers of the Hospital Universitario Fundación Alcorcón for their everyday work and cooperation in this study.




Subject Area
Reviews and Context
0
Comment
0
TRIP Peer Reviews
0
Community Reviews
0
Automated Services
1
Blogs/Media
Author Videos